
Time- and Frequency-Domain Analysis of Stroke Volume Variability Using Indoor Cycling to Evaluate Physical Load of Body


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Protocol
2.3. Measurement
2.4. Analysis
2.5. Statistical Analysis
3. Results
3.1. Participant Characteristics
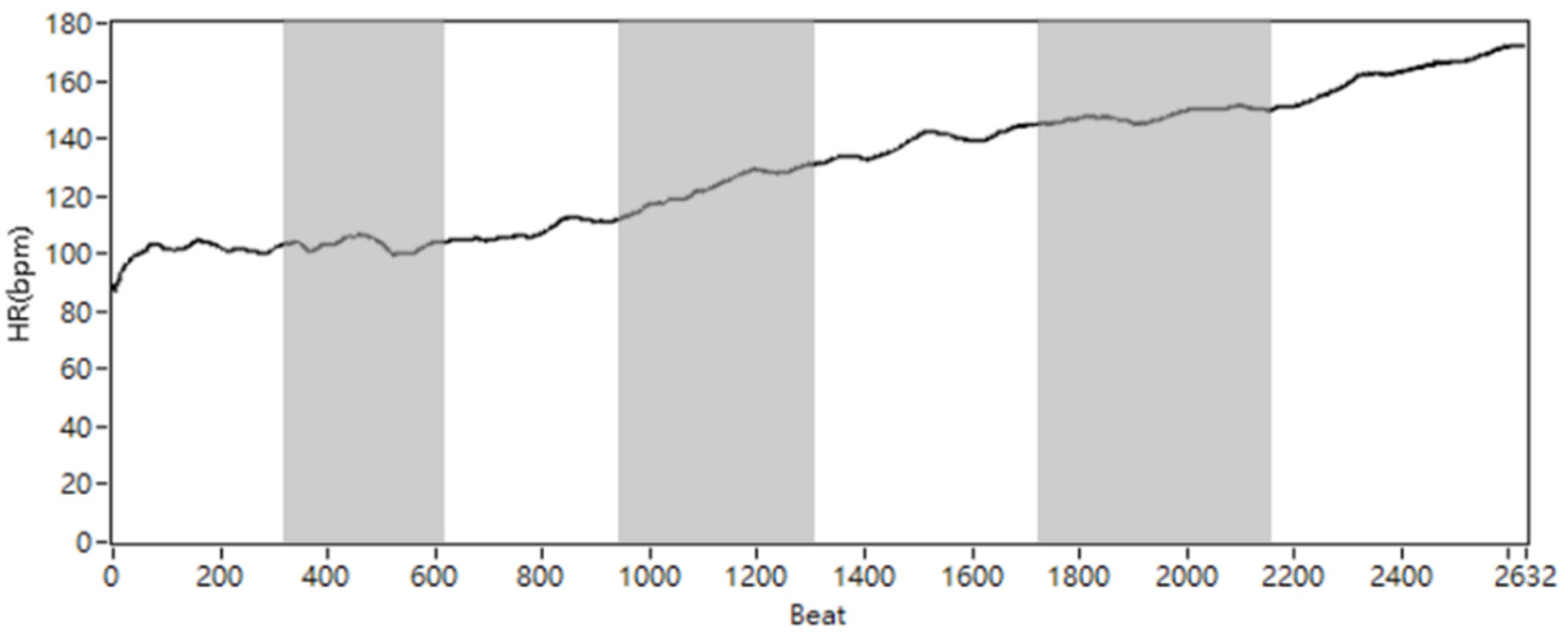
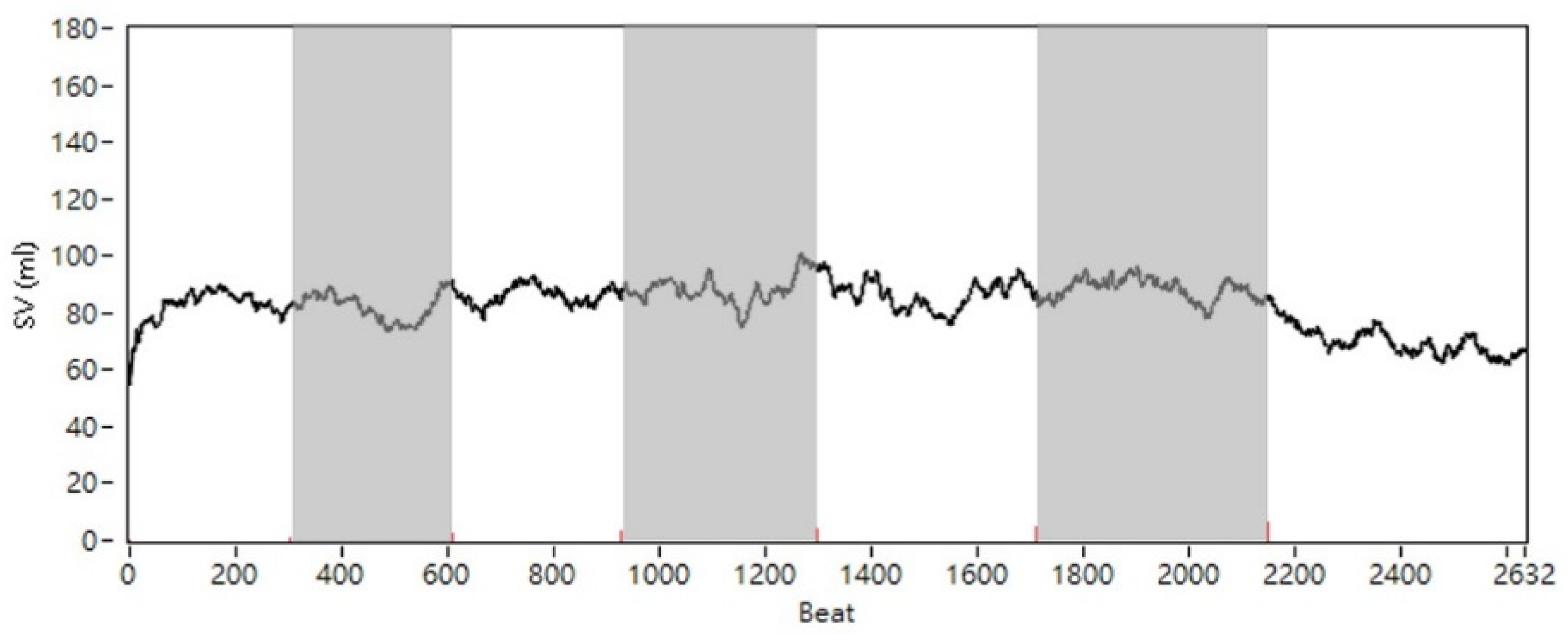
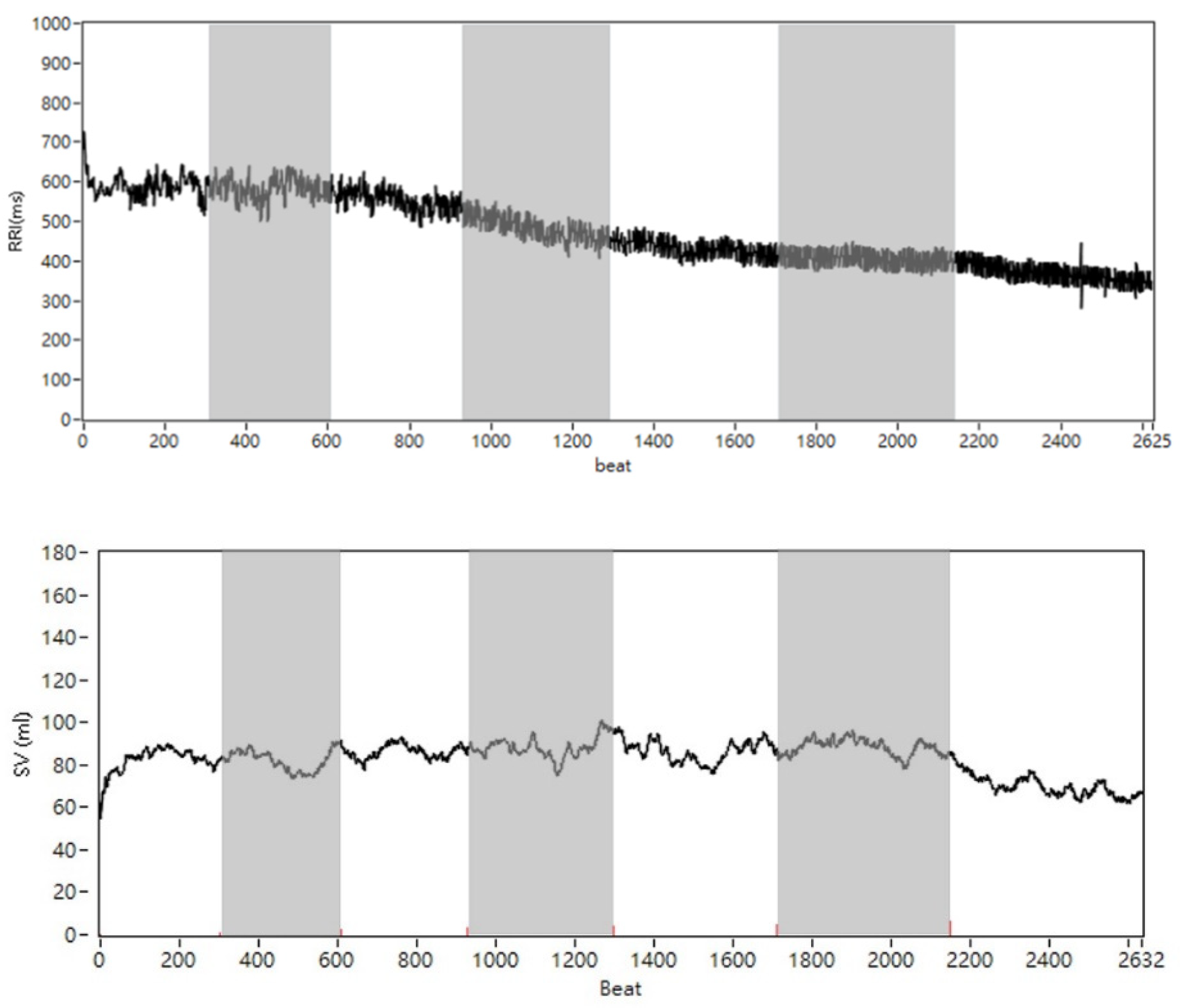
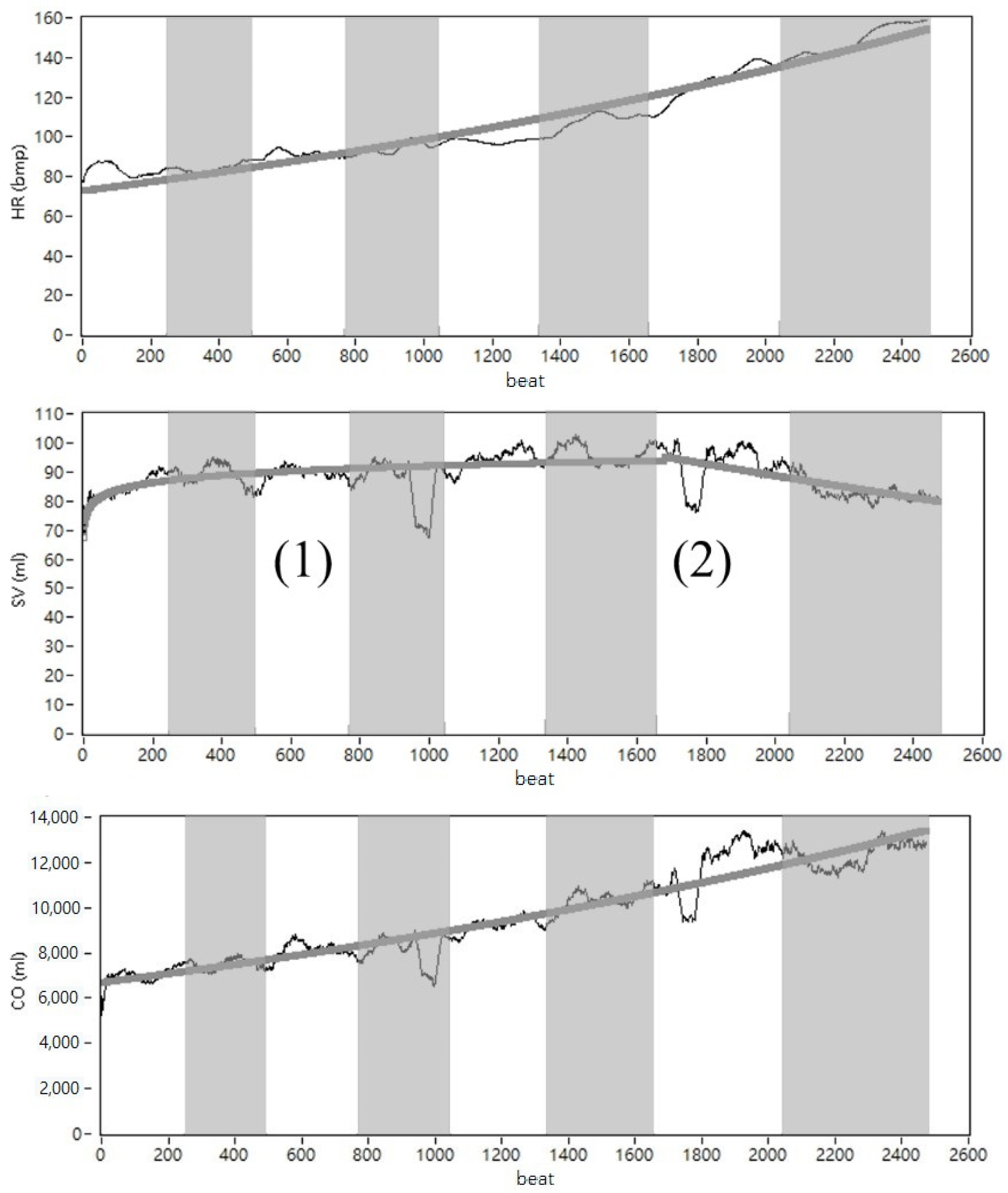
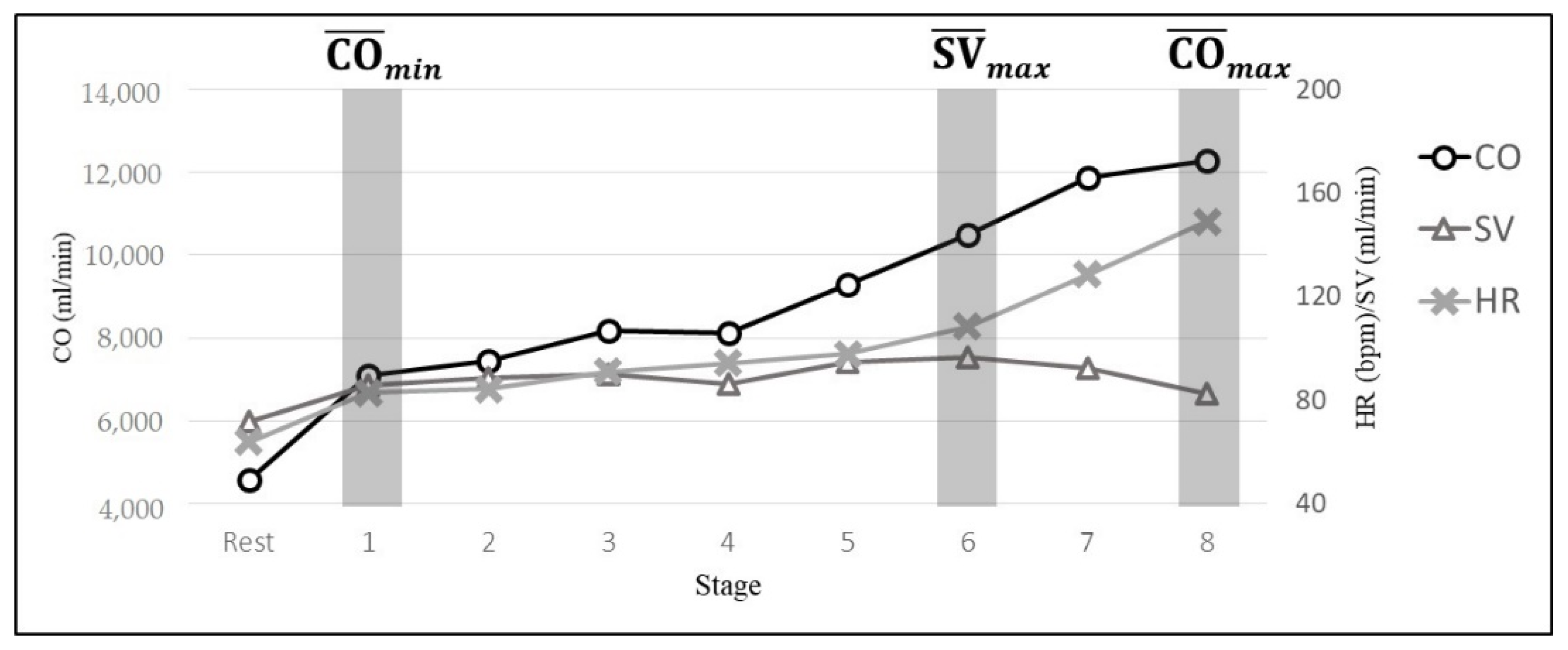
3.2. The Time-Domain Result
3.3. Figures, Tables and Schemes
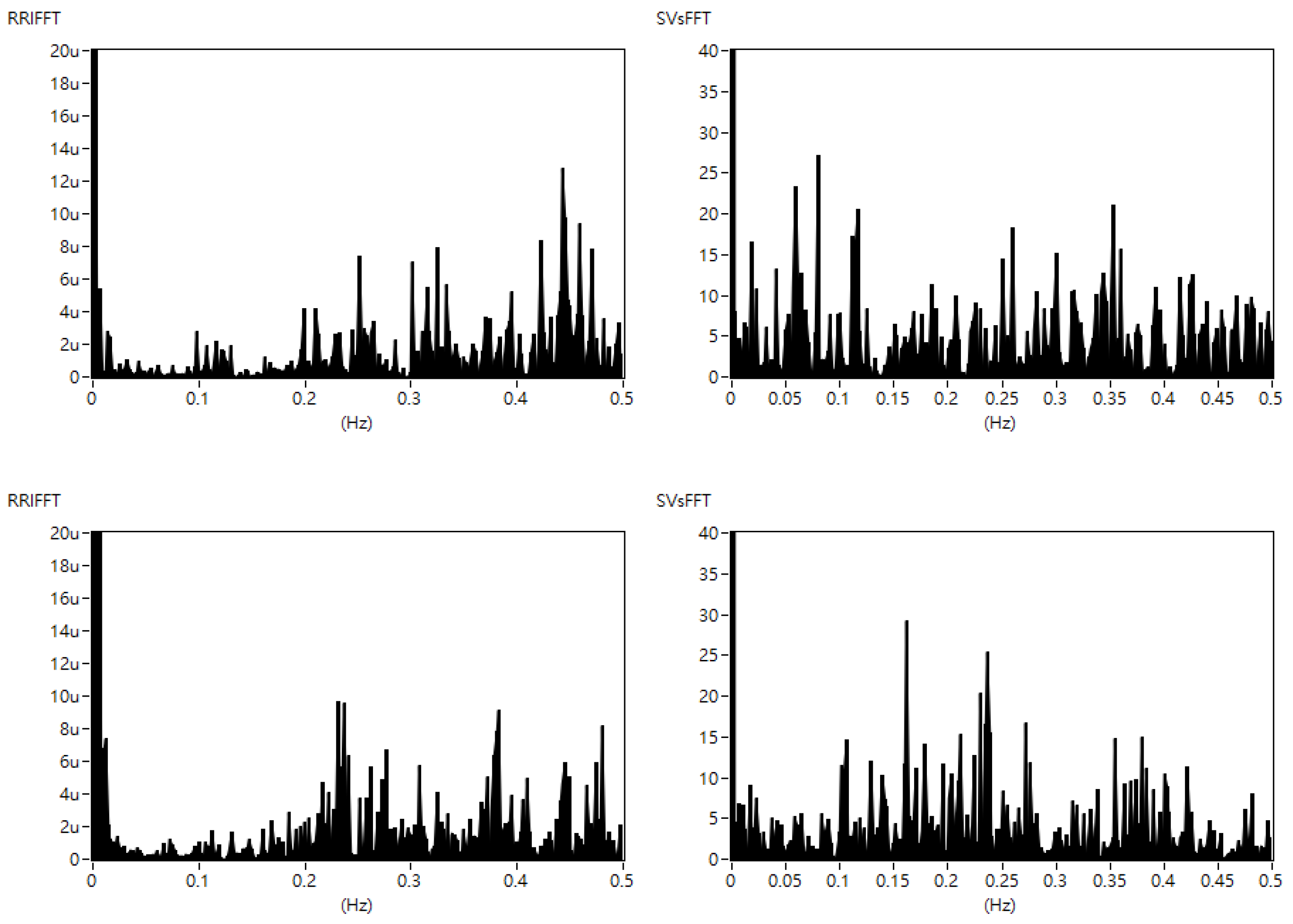
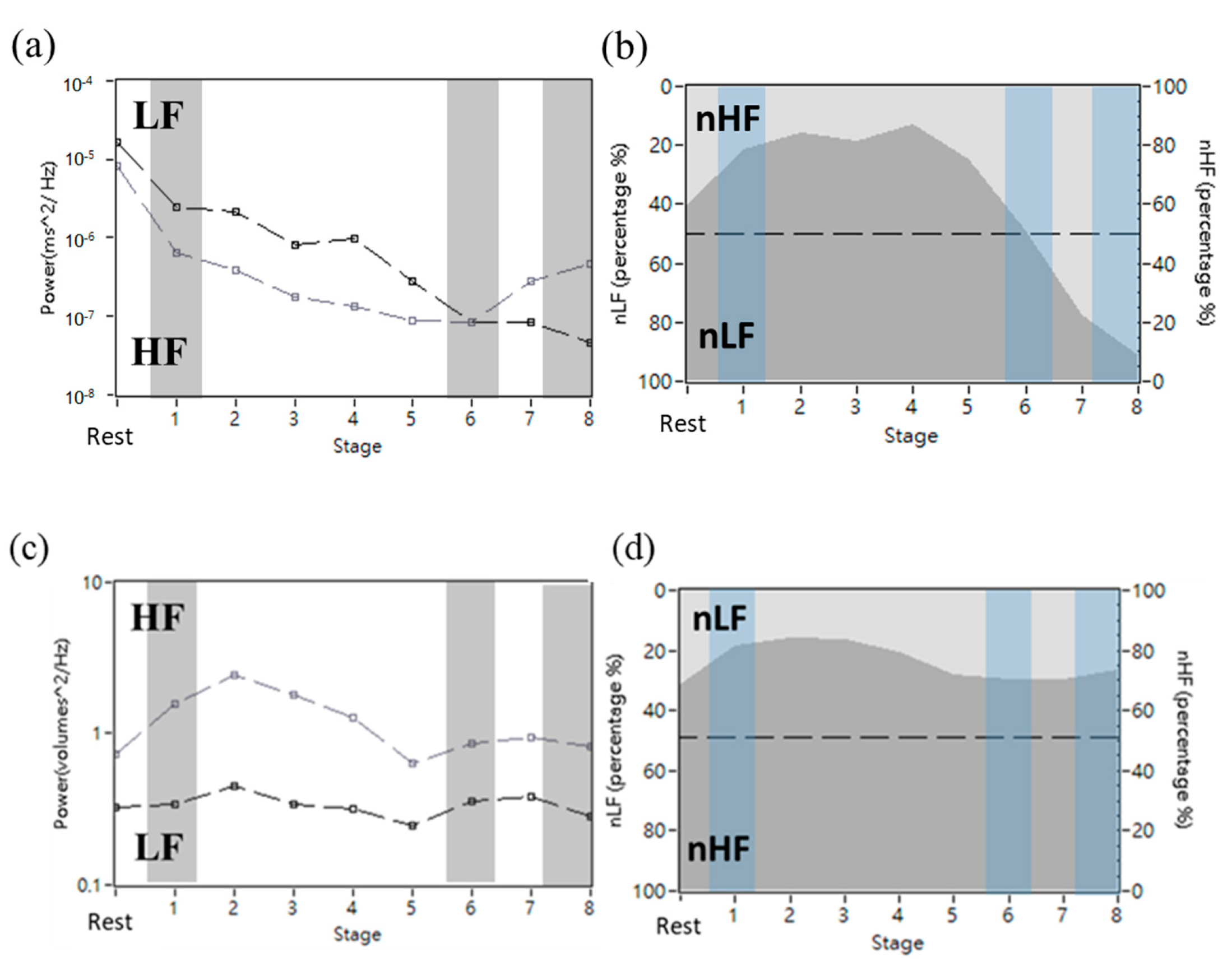
3.4. Results of the Frequency-Domain
3.5. Statistical Result
3.6. Correlation Coefficient Result
4. Discussion
Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Allender, S.; Cowburn, G.; Foster, C. Understanding participation in sport and physical activity among children and adults: A review of qualitative studies. Health Educ. Res. 2006, 21, 826–835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palacios-Ceña, D.; Fernandez-de-las-Peñas, C.; Hernández-Barrera, V.; Jiménez-Garcia, R.; Alonso-Blanco, C.; Carrasco-Garrido, P. Sports participation increased in Spain: A population-based time trend study of 21 381 adults in the years 2000, 2005 and 2010. Br. J. Sports Med. 2012, 46, 1137–1139. [Google Scholar] [CrossRef] [PubMed]
- Fox, S.I. Human Physiology, 12th ed.; McGraw-Hill: New York, NY, USA, 2011. [Google Scholar]
- Garlando, F.; Kohl, J.; Koller, E.A.; Pietsch, P. Effect of coupling the breathing and cycling rhythms on oxygen uptake during bicycle ergometry. Eur. J. Appl. Physiol. Occup. Physiol. 1985, 54, 497–501. [Google Scholar] [CrossRef] [PubMed]
- Daley, M.A.; Bramble, D.M.; Carrier, D.R. Impact loading and locomotor-respiratory coordination significantly influence breathing dynamics in running humans. PLoS ONE 2013, 8, e70752. [Google Scholar] [CrossRef] [Green Version]
- Formosa, D.P.; Sayer, M.G.; Burkett, B. Front crawl stroke-coordination and symmetry: A comparison between timing and net drag force protocols. J. Sports Sci. 2013, 31, 759–766. [Google Scholar] [CrossRef]
- Ganong, W.F. Review of Medical Physiology, 21st ed.; McGraw-Hill: New York, NY, USA, 2003. [Google Scholar]
- Stöhr, E.; González-Alonso, J.; Shave, R. Left ventricular mechanical limitations to stroke volume in healthy humans during incremental exercise. Am. J. Physiol.-Heart Circ. Physiol. 2011, 301, H478–H487. [Google Scholar] [CrossRef] [Green Version]
- Leischik, R.; Spelsberg, N. Endurance sport and “Cardiac Injury”: A prospective study of recreational ironman athletes. Int. J. Environ. Res. Public Health 2014, 11, 9082–9100. [Google Scholar] [CrossRef] [Green Version]
- O’Keefe, J.H.; Patil, H.R.; Lavie, C.J.; Magalski, A.; Vogel, R.A.; McCullough, P.A. Potential adverse cardiovascular effects from excessive endurance exercise. Mayo Clin. Proc. 2012, 87, 587–595. [Google Scholar] [CrossRef] [Green Version]
- George, K.P.; Wolfe, L.A.; Burggraf, G.W. The ‘athletic heart syndrome’. A critical review. Sports Med. 1991, 11, 300–331. [Google Scholar] [CrossRef]
- Leischik, R. Endurance Sport and Cardiac Injury. Kardiol. Pol. (Pol. Heart J.) 2014, 72, 587–597. [Google Scholar] [CrossRef]
- Kubicek, W.G.; Patterson, R.P.; Witsoe, D.A. Impedance cardiography as a noninvasive method of monitoring cardiac function and other parameters of the cardiovascular system. Ann. N. Y. Acad. Sci. 1970, 170, 724–732. [Google Scholar] [CrossRef]
- Kubicek, W.G. On the source of peak first time derivative (dZ/dt) during impedance cardiography. Ann. Biomed. Eng. 1989, 17, 459–462. [Google Scholar]
- Denniston, J.C.; Maher, J.T.; Reeves, J.T.; Cruz, J.C.; Cymerman, A.; Gover, R.F. Measurement of cardiac output by electrical impedance at rest and during exercise. J. Appl. Physiol. 1976, 40, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Northridge, D.B.; Findlay, I.N.; Wilson, J.; Henderson, E.; Dargie, H.J. Non-invasie determination of cardiac output by Doppler echocardiography and electrical bioimpedance. Br. Heart J. 1990, 63, 93–97. [Google Scholar] [CrossRef] [Green Version]
- Naidu, S.M.M.; Bagal, U.R.; Pandey, P.C.; Hardas, S.; Khambete, N.D. Detection of characteristic points of impedance cardiogram and validation using Doppler echocardiography. In Proceedings of the 2014 Annual IEEE India Conference, Pune, India, 11–13 December 2014. [Google Scholar]
- Sebastian, T.; Pandey, P.C.; Naidu, S.M.M.; Pandey, V.K. Wavelet based denoising for suppression of respiratory and motion artifacts in impedance cardiography. In Proceedings of the Computing in Cardiology 2011, Hangzhou, China, 18–21 September 2011. [Google Scholar]
- Trinkmann, F.; Schneider, C.; Michels, J.; Stach, K.; Doesch, C.; Schoenberg, S.O.; Borggrefe, M.; Saur, J.; Papavassiliu, T. Comparison of bioreactance non-invasive cardiac output measurements with cardiac magnetic resonance imaging. Anaesth. Intensive Care 2016, 44, 769–776. [Google Scholar] [CrossRef] [Green Version]
- Charloux, A.; Lonsdorfer-Wolf, E.; Richard, R.; Lampert, E.; Oseald-Mammosser, M.; Mettauer, B.; Geny, B.; Lonsdorfer, J. A new impedance cardiograph device for the non-invasive evaluation of cardiac output at rest and during exercise: Comparison with the “direct” Fick method. Eur. J. Appl. Physiol. 2000, 82, 313–320. [Google Scholar] [CrossRef]
- Schmidt, C.; Theilmeier, G.; van Aken, H.; Korsmeier, P.; Wirtz, S.P.; Berendes, E.; Hoffmeier, A.; Meissner, A. Comparison of electrical velocimetry and transesophageal Doppler Echocardiography for measuring stroke volume and cardiac output. Br. J. Anaesth. 2005, 95, 603–610. [Google Scholar] [CrossRef] [Green Version]
- Shaffer, F.; Ginsberg, J.P. An overview of heart rate variability metrics and norms. Front. Public Health 2017, 5, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Siebert, J.; Wtorek, J.; Rogowski, J. Stroke volume variabilityCardiovascular—to orthostatic maneuver in patients with coronary artery diseases. Ann. N. Y. Acad. Sci. 1999, 873, 182–190. [Google Scholar] [CrossRef]
- Liu, H.; Yambe, T.; Sasada, H.; Nanka, S.; Tanaka, A.; Nagatomi, R.; Nitta, S.I. Comparison of heart rate variability and stroke volume variability. Auton. Neurosci. 2004, 116, 69–75. [Google Scholar] [CrossRef]
- Bernstein, D.P.; Fe, R.S.; Osypka, M.J. Apparatus and Method for Determining an Approximation of the Stroke Volume and the Cardiac Output of the Heart. U.S. Patent Application No. 6,511,438, 3 April 2001. [Google Scholar]
- Åstrand, P.O.; Cuddy, T.E.; Saltin, B.; Stenberg, J. Cardiac output during submaximal and maximal work. J. Appl. Physiol. 1964, 19, 268–374. [Google Scholar] [CrossRef] [PubMed]
- Robison, B.F.; Epstein, S.E.; Beiser, G.D.; Braunwald, E. Control of heart rate by the autonomic nervous system: Studies in man on the interrelation between baroreceptor mechanisms and exercise. Circ. Res. 1966, 19, 400–411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perini, R.; Veicsteinas, A. Heart rate variability and autonomic activity at rest and during exercise in various physiological conditions. Eur. J. Appl. Physiol. 2003, 90, 317–325. [Google Scholar] [CrossRef]
- Sarmiento, S.; Garcia-Manso, J.M.; Martin-Gonzalz, J.M.; Vaamonde, D.; Calderon, J.; da Silva-Grigoletto, M.E. Heart rate variability during high-intensity exercise. J. Syst. Sci. Complex. 2013, 26, 104–116. [Google Scholar] [CrossRef]
- Lai, W.-C.; Huang, P.-H.; Hsiao, T.-C. Relationship between breath regulation and stroke volume with exercise intensity: A pilot study. In Proceedings of the 12th International Conference on eHealth, Telemedicine, and Social Medicine (eTELEMED 2020), Valencia, Spain, 21–25 November 2020. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Male n = 17 | Female n = 13 | Total n = 30 | |
|---|---|---|---|---|
| Age (year) | mean ± SD | 24.29 ±1.72 | 27.38 ± 4.07 | 25.63 ± 3.30 |
| median | 24 | 26 | 25 | |
| Height (cm) | mean ± SD | 176.14 ± 6.04 | 159.65 ± 4.25 | 169.00 ± 9.83 |
| median | 178 | 159 | 168 | |
| Weight (kg) | mean ± SD | 72.00 ± 10.00 | 56.69 ± 6.50 | 65.37 ± 0.50 |
| median | 70 | 57 | 62.5 | |
| BMI | mean ± SD | 23.18 ± 2.72 | 22.30 ± 3.30 | 22.80 ± 2.84 |
| median | 23.38 | 21.76 | 22.83 | |
| Final stage | median | 7 | 6 | 6 |
| Stage | Median Stage | |||
|---|---|---|---|---|
| Rest | 0 | 41.52 ± 6.72 (81.33 ± 12.33) | 95.23 ± 20.62 (71.70 ± 0.65) | 57.99 ± 16.59 (5827.31 ± 855.61) |
| min | 1 | 55.58 ± 11.15 * (103.69 ± 14.27) | 85.15 ± 13.63 * (72.54 ± 13.97) | 71.38 ± 10.36 * (7446.10 ± 1447.64) |
| max | 2 | 59.14 ± 10.12 (116.57 ± 19.29) | 100.00 # (78.26 ± 14.88) | 86.38 ± 12.25 # (9137.12 ± 2505.62) |
| max | 6 | 76.28 ± 7.94 † (150.49 ± 19.28) | 89.86 ± 7.90 † (70.01 ± 16.13) | 100.00 † (10,575.43 ± 2305.81) |
| Stage | Median Stage | nLFHRV(%) | nHFHRV(%) | nLFSVV(%) | nHFSVV(%) |
|---|---|---|---|---|---|
| Rest | 0 | 68.24 ± 19.03 | 31.76 ± 19.03 | 28.64 ± 2.02 | 71.36 ± 2.02 |
| min | 1 | 63.96 ± 18.06 | 36.04 ± 18.06 | 29.43 ± 10.07 | 70.57 ± 10.07 |
| max | 2 | 50.30 ± 22.71 # | 49.70 ± 22.71 # | 29.81 ± 8.16 | 70.19 ± 8.16 |
| max | 6 | 25.01 ± 18.47 * | 74.99 ± 18.47 * | 30.12 ± 7.11 | 69.88 ± 7.11 |
| r-Value | Mean ± SD | Median |
|---|---|---|
| Normal stages (S1) | 0.88 ± 0.06 | 0.91 # |
| The last stage before APC (S2) | 0.81 ± 0.13 | 0.87 * |
| The APC stages (S3) | 0.59 ± 0.21 | 0.60 *# |
| LF Lower Band (Hz) | LF Upper Band/ HF Lower Band (Hz) | HF Upper Band (Hz) | |
|---|---|---|---|
| mean ± SD | 0.035 ± 0.01 | 0.084 ± 0.04 | 0.301 ± 0.06 |
| median | 0.035 | 0.11 | 0.290 |
| r-Value | r2 | |||||
|---|---|---|---|---|---|---|
| LF | HF | LF | HF | LF | HF | |
| mean ± SD | 0.60 ± 0.67 | 0.35 ± 0.72 | 0.88 ± 0.16 | 0.77 ± 0.23 | 0.79 ± 0.25 | 0.64 ± 0.31 |
| median | 0.91 | 0.73 | 0.94 | 0.81 | 0.88 | 0.65 |
| r-Value | r2 | ||||||
|---|---|---|---|---|---|---|---|
| LF | HF | LF | HF | LF | HF | ||
| Original | mean ± SD | 0.16 ± 0.45 | 0.13 ± 0.49 | 0.37 ± 0.28 | 0.39 ± 0.31 | 0.22 ± 0.27 | 0.24 ± 0.30 |
| median | 0.12 | 0.10 | 0.37 | 0.30 | 0.14 | 0.29 | |
| New | mean ± SD | 0.38 ± 0.51 | 0.29 ± 0.51 | 0.56 ± 0.28 | 0.51 ± 0.29 | 0.39 ± 0.32 | 0.34 ± 0.30 |
| median | 0.46 * | 0.31 * | 0.53 * | 0.58 * | 0.28 * | 0.34 | |
| r-Value | r2 | ||||||
|---|---|---|---|---|---|---|---|
| LF | HF | LF | HF | LF | HF | ||
| All stages (S1 + S2 + S3) | mean ±SD | 0.38 ± 0.51 | 0.29 ± 0.51 | 0.56 ± 0.28 | 0.51 ± 0.29 | 0.39 ± 0.32 | 0.34 ± 0.30 |
| median | 0.46 | 0.31 | 0.53 | 0.58 | 0.28 | 0.34 | |
| The stages without ACP (S1 + S2) | mean ± SD | 0.14 ± 0.82 | 0.30 ± 0.72 | 0.78 ± 0.23 | 0.72 ± 0.26 | 0.66 ± 0.33 | 0.59 ± 0.36 |
| median | 0.55 | 0.50 | 0.82 * | 0.80 * | 0.66 * | 0.64 * | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, Y.-H.; Lai, W.-C.; Huang, P.-H.; Hsiao, T.-C. Time- and Frequency-Domain Analysis of Stroke Volume Variability Using Indoor Cycling to Evaluate Physical Load of Body. Information 2022, 13, 148. https://doi.org/10.3390/info13030148
Lai Y-H, Lai W-C, Huang P-H, Hsiao T-C. Time- and Frequency-Domain Analysis of Stroke Volume Variability Using Indoor Cycling to Evaluate Physical Load of Body. Information. 2022; 13(3):148. https://doi.org/10.3390/info13030148
Chicago/Turabian StyleLai, Yu-Han, Wei-Chen Lai, Po-Hsun Huang, and Tzu-Chien Hsiao. 2022. "Time- and Frequency-Domain Analysis of Stroke Volume Variability Using Indoor Cycling to Evaluate Physical Load of Body" Information 13, no. 3: 148. https://doi.org/10.3390/info13030148
APA StyleLai, Y. -H., Lai, W. -C., Huang, P. -H., & Hsiao, T. -C. (2022). Time- and Frequency-Domain Analysis of Stroke Volume Variability Using Indoor Cycling to Evaluate Physical Load of Body. Information, 13(3), 148. https://doi.org/10.3390/info13030148