
Autologous Bone Marrow Mononuclear Cells (BMMC)-Associated Anti-Inflammatory Nanoparticles for Cardiac Repair after Myocardial Infarction

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Experimental Design
2.3. Bone Marrow BMMC Isolation
2.4. Flow Cytometry Analysis
2.5. Preparation of 15d-PGJ2 Loaded PLGA Nanoparticles
2.6. Chronic Myocardial Infarction (MI) and Cell + Nanoparticle Transplantation
2.7. Echocardiography Analysis
2.8. Euthanasia
2.9. Histopathological Analysis
2.10. Statistical Analysis
3. Results
3.1. Characterization of BMMC

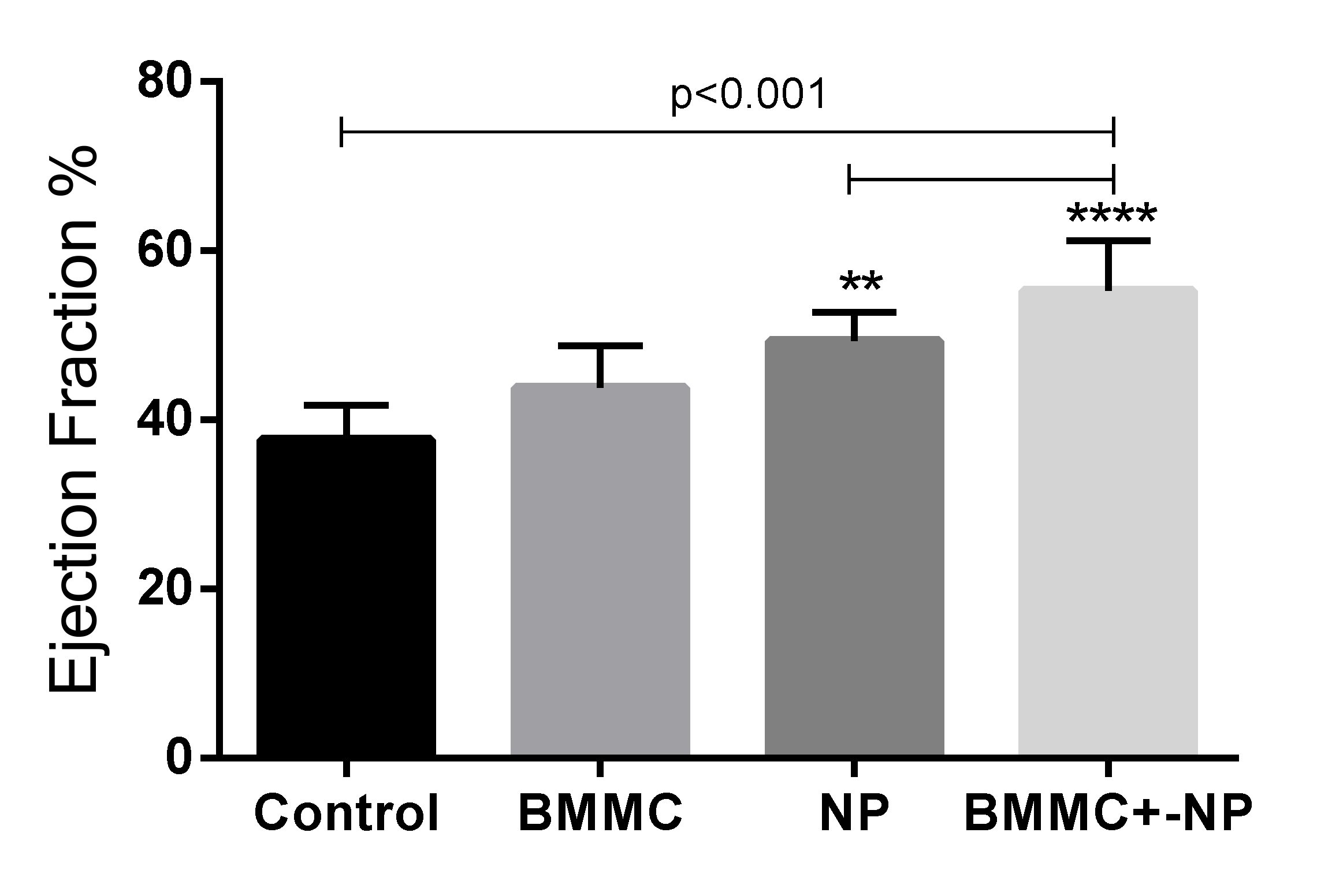
3.2. Echocardiography Findings
Combined Nanoparticle and BMSC Transplantation Improved Post-MI Cardiac Function
Intra-Group Assessment

Inter-Group Evaluation

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Echocardiographic Parameters | Day | n | Control | Nanoparticle (NP) | BMMC | BMMC + NP | p * |
|---|---|---|---|---|---|---|---|
| LVEDV (mL) | 7 | 10 | 0.278 ± 0.062 | 0.267 ± 0.053 | 0.326 ± 0.069 | 0.217 ± 0.040 | 0.248 |
| 30 | 8 | 0.221 ± 0.074 | 0.172 ± 0.034 | 0.229 ± 0.071 | 0.178 ± 0.050 | ||
| LVESV (mL) | 7 | 8 | 0.171 ± 0.053 | 0.176 ± 0.042 | 0.233 ± 0.020 | 0.134 ± 0.031 | 0.248 |
| 30 | 8 | 0.139 ± 0.058 | 0.088 ± 0.036 | 0.130 ± 0.060 | 0.089 ± 0.035 | ||
| LVEF (%) | 7 | 8 | 39.0 ± 7.4 | 34.4 ± 3.9 | 29.2 ± 7.7 | 39.0 ± 6.5 | 0.008 |
| 30 | 8 | 39.6 ± 6.7 | 51.0 ± 10.7 | 46.4 ± 7.0 | 51.4 ± 5.4 |
| LVEF-Pre | LVEF-Post | LVEF-Difference | |
|---|---|---|---|
| Groups Comparison | p | p | p |
| Control × BMMC | 0.005 | 0.054 | 0.054 |
| Control × NP | 0.223 | 0.007 | 0.007 |
| Control × BMMC + NP | 0.985 | 0.004 | 0.004 |
| BMMC × NP | 0.145 | 0.231 | 0.231 |
| BMMC × BMMC + NP | 0.007 | 0.171 | 0.171 |
| NP × BMMC + NP | 0.243 | 0.915 | 0.915 |
3.3. Histological Analyses
| Variable | Group | Mean | Median | SD | p * |
|---|---|---|---|---|---|
| Connexin (%) | Control (n = 10) | 9.51 | 9.39 | 0.73 | 0.034 |
| BMMC (n = 8) | 12.44 | 12.04 | 2.03 | ||
| Nanoparticle (n = 8) | 12.27 | 12.28 | 0.62 | ||
| (BMMC) + NP (n = 8) | 6.63 | 6.48 | 1.04 | ||
| Desmin (%) | Control (n = 10) | 4.41 | 3.61 | 1.98 | 0.015 |
| BMMC (n = 8) | 25.01 | 26.60 | 8.19 | ||
| Nanoparticle (n = 8) | 17.74 | 18.41 | 4.12 | ||
| (BMMC) + NP (n = 8) | 6.63 | 6.48 | 1.04 | ||
| Factor VIII (%) | Control (n = 10) | 3.23 | 3.47 | 0.71 | 0.018 |
| BMMC (n = 8) | 9.95 | 7.23 | 6.04 | ||
| Nanoparticle (n = 8) | 6.63 | 6.48 | 1.04 | ||
| (BMMC) + NP (n = 8) | 6.63 | 6.48 | 1.04 | ||
| TGFβ (%) | Control (n = 10) | 2.81 | 2.55 | 1.11 | <0.0001 |
| BMMC (n = 8) | 6.04 | 5.80 | 2.47 | ||
| Nanoparticle (n = 8) | 16.03 | 4.63 | 4.06 | ||
| (BMMC) + NP (n = 8) | 12.72 | 12.71 | 3.74 |

3.4. Collagen Level Analysis and Infarct Area

| Variable | Group | Mean | SD | p * |
|---|---|---|---|---|
| Type I | Control (n = 10) | 82.50 | ±10.74 | <0.0001 |
| Collagen (%) | BMMC (n = 8) | 50.50 | ±6.61 | |
| Nanoparticle (n = 8) | 44.74 | ±9.69 | ||
| (BMMC) +NP (n = 8) | 46.50 | ±9.81 | ||
| Type III | Control (n = 10) | 35.81 | ±8.45 | <0.0001 |
| Collagen (%) | BMMC (n = 8) | 100.5 | ±8.07 | |
| Nanoparticle (n = 8) | 115.7 | ±23.45 | ||
| (BMMC) +NP (n = 8) | 112.2± | ±22.19 | ||
| Infarct area (%) | Control (n = 10) | 273.2 | ±1.87 | 0.979 |
| BMMC (n = 8) | 306.6 | ±2.41 | ||
| Nanoparticle (n = 8) | 367.8 | ±3.57 | ||
| (BMMC) +NP (n = 8) | 309.2 | ±2.79 |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aydin, S.; Ugur, K.; Aydin, S.; Sahin, I.; Yardim, M. Biomarkers in acute myocardial infarction: Current perspectives. Vasc. Health Risk Manag. 2019, 15, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, P.; Wang, L.; Li, Q.; Xu, J.; Xu, J.; Xiong, Y.; Chen, G.; Qian, H.; Jin, C.; Yu, Y.; et al. Combinatorial treatment of acute myocardial infarction using stem cells and their derived exosomes resulted in improved heart performance. Stem Cell Res. Ther. 2019, 10, 300. [Google Scholar] [CrossRef] [Green Version]
- Sürder, D.; Manka, R.; Lo Cicero, V.; Moccetti, T.; Rufibach, K.; Soncin, S.; Turchetto, L.; Radrizzani, M.; Astori, G.; Schwitter, J.; et al. Intracoronary injection of bone marrow-derived mononuclear cells early or late after chronic myocardial infarction: Effects on global left ventricular function. Circulation 2013, 127, 1968–1979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delewi, R.; Hirsch, A.; Tijssen, J.G.; Schächinger, V.; Wojakowski, W.; Roncalli, J.; Aakhus, S.; Erbs, S.; Assmus, B.; Tendera, M.; et al. Impact of intracoronary bone marrow cell therapy on left ventricular function in the setting of ST-segment elevation myocardial infarction: A collaborative meta-analysis. Eur. Heart J. 2014, 35, 989–998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ambesh, P.; Campia, U.; Obiagwu, C.; Bansal, R.; Shetty, V.; Hollander, G.; Shani, J. Nanomedicine in coronary artery disease. Indian Heart J. 2017, 69, 244–251. [Google Scholar] [CrossRef]
- Peng, H.; Chen, F.-E. Recent advances in asymmetric total synthesis of prostaglandins. Org. Biomol. Chem. 2017, 15, 6281–6301. [Google Scholar] [CrossRef]
- Ruiz-Miyazawa, K.W.; Staurengo-Ferrari, L.; Pinho-Ribeiro, F.A.; Fattori, V.; Zaninelli, T.H.; Badaro-Garcia, S.; Borghi, S.M.; Andrade, K.C.; Clemente-Napimoga, J.T.; Alves-Filho, J.C.; et al. 15d-PGJ2-loaded nanocapsules ameliorate experimental gout arthritis by reducing pain and inflammation in a PPAR-gamma-sensitive manner in mice. Sci. Rep. 2018, 8, 13979. [Google Scholar] [CrossRef]
- Francisco, J.C.; Uemura, L.; Simeoni, R.B.; da Cunha, R.C.; Mogharbel, B.F.; Simeoni, P.R.B.; Naves, G.; Napimoga, M.H.; Noronha, L.; Carvalho, K.A.T.; et al. Acellular Human Amniotic Membrane Scaffold with 15d-PGJ2 Nanoparticles in Postinfarct Rat Model. Tissue Eng. Part A 2020, 26, 1128–1137. [Google Scholar] [CrossRef]
- Napimoga, M.H.; da Silva, C.A.T.; Carregaro, V.; Farnesi-De-Assunção, T.S.; Duarte, P.M.; de Melo, N.F.S.; Fraceto, L.F. Exogenous Administration of 15d-PGJ2–Loaded Nanocapsules Inhibits Bone Resorption in a Mouse Periodontitis Model. J. Immunol. 2012, 189, 1043–1052. [Google Scholar] [CrossRef] [Green Version]
- Böyum, A. Isolation of mononuclear cells and granulocytes from human blood. Isolation of monuclear cells by one centrifugation, and of granulocytes by combining centrifugation and sedimentation at 1 g. Scand. J. Clin. Lab. Investig. Suppl. 1968, 97, 77–89. [Google Scholar]
- Mogharbel, B.F.; Abdelwahid, E.; Irioda, A.C.; Francisco, J.C.; Simeoni, R.B.; De Souza, D.; De Souza, C.M.C.O.; Beltrame, M.P.; Ferreira, R.J.; Guarita-Souza, L.C.; et al. Bone Marrow-Derived Stem Cell Populations Are Differentially Regulated by Thyroid or/and Ovarian Hormone Loss. Int. J. Mol. Sci. 2017, 18, 2139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guarita-Souza, L.; de Carvalho, K.A.T.; Simeone, B.; Franscisco, J.; Miyague, N.; Olandoski, M. Functional Outcome of Bone Marrow Stem Cells: Mononuclear Versus Mesenchymal Stem Cells After Cellular Therapy in Myocardial Scar in Wistar Rats. Transplant. Proc. 2006, 38, 1953–1954. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Ge, J.; Chen, C.; Shen, Y.; Xie, J.; Zhu, X.; Liu, M.; Hu, J.; Chen, L.; Guo, L.; et al. FAT10 protects against ischemia-induced ventricular arrhythmia by decreasing Nedd4-2/Nav1.5 complex formation. Cell Death Dis. 2021, 12, 25. [Google Scholar] [CrossRef] [PubMed]
- Alves, C.; de Melo, N.; Fraceto, L.; Araújo, D.; Napimoga, M. Effects of 15d-PGJ2-loaded poly(D,L-lactide-co-glycolide) nanocapsules on inflammation. J. Cereb. Blood Flow Metab. 2010, 162, 623–632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerbin, K.A.; Yang, X.; Murry, C.E.; Coulombe, K.L.K. Enhanced Electrical Integration of Engineered Human Myocardium via Intramyocardial versus Epicardial Delivery in Infarcted Rat Hearts. PLoS ONE 2015, 10, e0131446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.; Dong, N.; Niu, Y.; Zhang, Z.; Zhang, C.; Liu, M.; Zhou, T.; Wu, Q.; Cheng, K. Transplantation of human villous trophoblasts preserves cardiac function in mice with acute myocardial infarction. J. Cell. Mol. Med. 2017, 21, 2432–2440. [Google Scholar] [CrossRef] [Green Version]
- Bernardo, M.E.; Fibbe, W.E. Mesenchymal stromal cells and hematopoietic stem cell transplantation. Immunol. Lett. 2015, 168, 215–221. [Google Scholar] [CrossRef]
- Guarita-Souza, L.C.; Atahyde, K.; De Carvalho, T.; Rebelatto, C.; Hansen, P.; Furuta, M.; Miyague, N.; Francisco, J.C.; Olandoski, M.; Woitowiczet, V.; et al. Comparison of mononu-clear and mesenchymal stem cell transplantation in myocardium infarction. Braz. J. Cardiovasc. Surg. 2005, 20, 270–278. [Google Scholar] [CrossRef]
- Azhar, M.; Schultz, J.E.J.; Grupp, I.; Dorn, G.W.; Meneton, P.; Molin, D.G.M.; Gittenberger-de Groot, A.C.; Doetschman, T. Transforming growth factor beta in cardiovascular development and function. Cytokine Growth Factor Rev. 2003, 14, 391–407. [Google Scholar] [CrossRef] [Green Version]
- Khan, I.; Ali, A.; Akhter, M.A.; Naeem, N.; Chotani, M.A.; Mustafa, T.; Salim, A. Preconditioning of mesenchymal stem cells with 2,4-dinitrophenol improves cardiac function in infarcted rats. Life Sci. 2016, 162, 60–69. [Google Scholar] [CrossRef]
- Cosmo, S.; Francisco, J.C.; Da Cunha, R.C.; De Macedo, R.M.; Faria-Neto, J.R.; Simeoni, R.; de Carvalho, K.A.T.; Olandoski, M.; Miyague, N.I.; Amaral, V.F.D.; et al. Effect of exercise associated with stem cell transplantation on ventricular function in rats after acute myocardial infarction. Rev. Bras. Cir. Cardiovasc. 2012, 27, 542–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayıroğlu, M.; Keskin, M.; Uzun, A.O.; Yıldırım, D.I.; Kaya, A.; Çinier, G.; Bozbeyoğlu, E.; Yıldırımtürk, Ö.; Kozan, Ö.; Pehlivanoğlu, S. Predictors of In-Hospital Mortality in Patients With ST-Segment Elevation Myocardial Infarction Complicated with Cardiogenic Shock. Heart Lung Circ. 2019, 28, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Passino, C.; Barison, A.; Vergaro, G.; Gabutti, A.; Borrelli, C.; Emdin, M.; Clerico, A. Markers of fibrosis, inflammation, and remodeling pathways in heart failure. Clin. Chim. Acta 2015, 443, 29–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boarescu, P.-M.; Chirilă, I.; Bulboacă, A.E.; Bocșan, I.C.; Pop, R.M.; Gheban, D.; Bolboacă, S.D. Effects of Curcumin Nanoparticles in Isoproterenol-Induced Myocardial Infarction. Oxid. Med. Cell. Longev. 2019, 2019, 7847142. [Google Scholar] [CrossRef]
- Ichimura, K.; Matoba, T.; Nakano, K.; Tokutome, M.; Honda, K.; Koga, J.-I.; Egashira, K. A Translational Study of a New Therapeutic Approach for Acute Myocardial Infarction: Nanoparticle-Mediated Delivery of Pitavastatin into Reperfused Myocardium Reduces Ischemia-Reperfusion Injury in a Preclinical Porcine Model. PLoS ONE 2016, 11, e0162425. [Google Scholar] [CrossRef] [Green Version]
- Rikhtegar, R.; Pezeshkian, M.; Dolati, S.; Safaie, N.; Rad, A.A.; Mahdipour, M.; Nouri, M.; Jodati, A.R.; Yousefi, M. Stem cells as therapy for heart disease: iPSCs, ESCs, CSCs, and skeletal myoblasts. Biomed. Pharmacother. 2019, 109, 304–313. [Google Scholar] [CrossRef]
- Guo, R.; Morimatsu, M.; Feng, T.; Lan, F.; Chang, D.; Wan, F.; Ling, Y. Stem cell-derived cell sheet transplantation for heart tissue repair in myocardial infarction. Stem Cell Res. Ther. 2020, 11, 19. [Google Scholar] [CrossRef] [Green Version]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uemura, L.; Baggio Simeoni, R.; Bispo Machado Júnior, P.A.; Gavazzoni Blume, G.; Kremer Gamba, L.; Sgarbossa Tonial, M.; Baggio Simeoni, P.R.; Stadler Tasca Ribeiro, V.; Silvestre, R.; de Carvalho, K.A.T.; et al. Autologous Bone Marrow Mononuclear Cells (BMMC)-Associated Anti-Inflammatory Nanoparticles for Cardiac Repair after Myocardial Infarction. J. Funct. Biomater. 2022, 13, 59. https://doi.org/10.3390/jfb13020059
Uemura L, Baggio Simeoni R, Bispo Machado Júnior PA, Gavazzoni Blume G, Kremer Gamba L, Sgarbossa Tonial M, Baggio Simeoni PR, Stadler Tasca Ribeiro V, Silvestre R, de Carvalho KAT, et al. Autologous Bone Marrow Mononuclear Cells (BMMC)-Associated Anti-Inflammatory Nanoparticles for Cardiac Repair after Myocardial Infarction. Journal of Functional Biomaterials. 2022; 13(2):59. https://doi.org/10.3390/jfb13020059
Chicago/Turabian StyleUemura, Laercio, Rossana Baggio Simeoni, Paulo André Bispo Machado Júnior, Gustavo Gavazzoni Blume, Luize Kremer Gamba, Murilo Sgarbossa Tonial, Paulo Ricardo Baggio Simeoni, Victoria Stadler Tasca Ribeiro, Rodrigo Silvestre, Katherine Athayde Teixeira de Carvalho, and et al. 2022. "Autologous Bone Marrow Mononuclear Cells (BMMC)-Associated Anti-Inflammatory Nanoparticles for Cardiac Repair after Myocardial Infarction" Journal of Functional Biomaterials 13, no. 2: 59. https://doi.org/10.3390/jfb13020059
APA StyleUemura, L., Baggio Simeoni, R., Bispo Machado Júnior, P. A., Gavazzoni Blume, G., Kremer Gamba, L., Sgarbossa Tonial, M., Baggio Simeoni, P. R., Stadler Tasca Ribeiro, V., Silvestre, R., de Carvalho, K. A. T., Napimoga, M. H., Cesar Francisco, J., & Guarita-Souza, L. C. (2022). Autologous Bone Marrow Mononuclear Cells (BMMC)-Associated Anti-Inflammatory Nanoparticles for Cardiac Repair after Myocardial Infarction. Journal of Functional Biomaterials, 13(2), 59. https://doi.org/10.3390/jfb13020059