
Photobiomodulation and Inorganic Bovine Bone in Guided Bone Regeneration: Histomorphometric Analysis in Rats

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
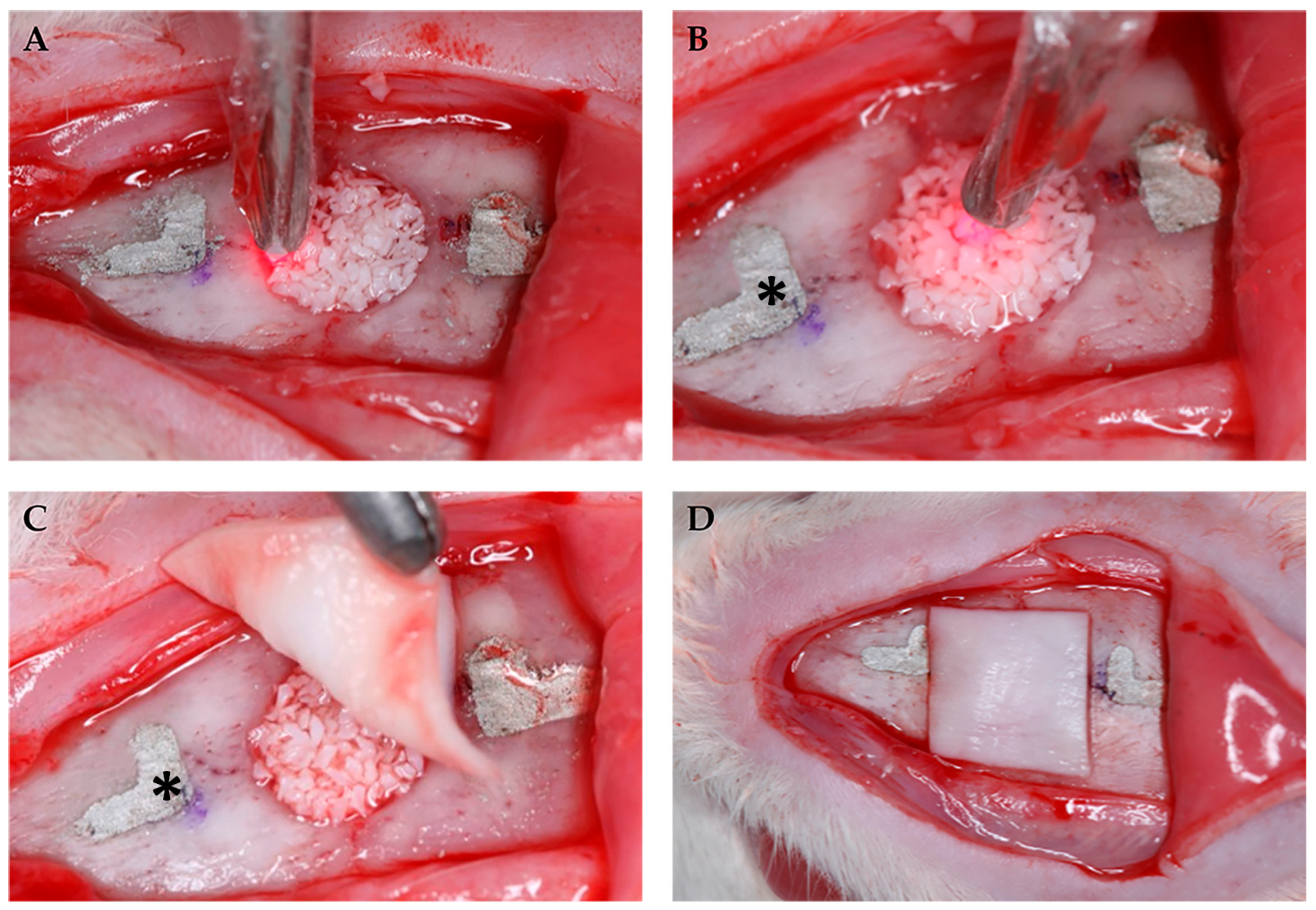
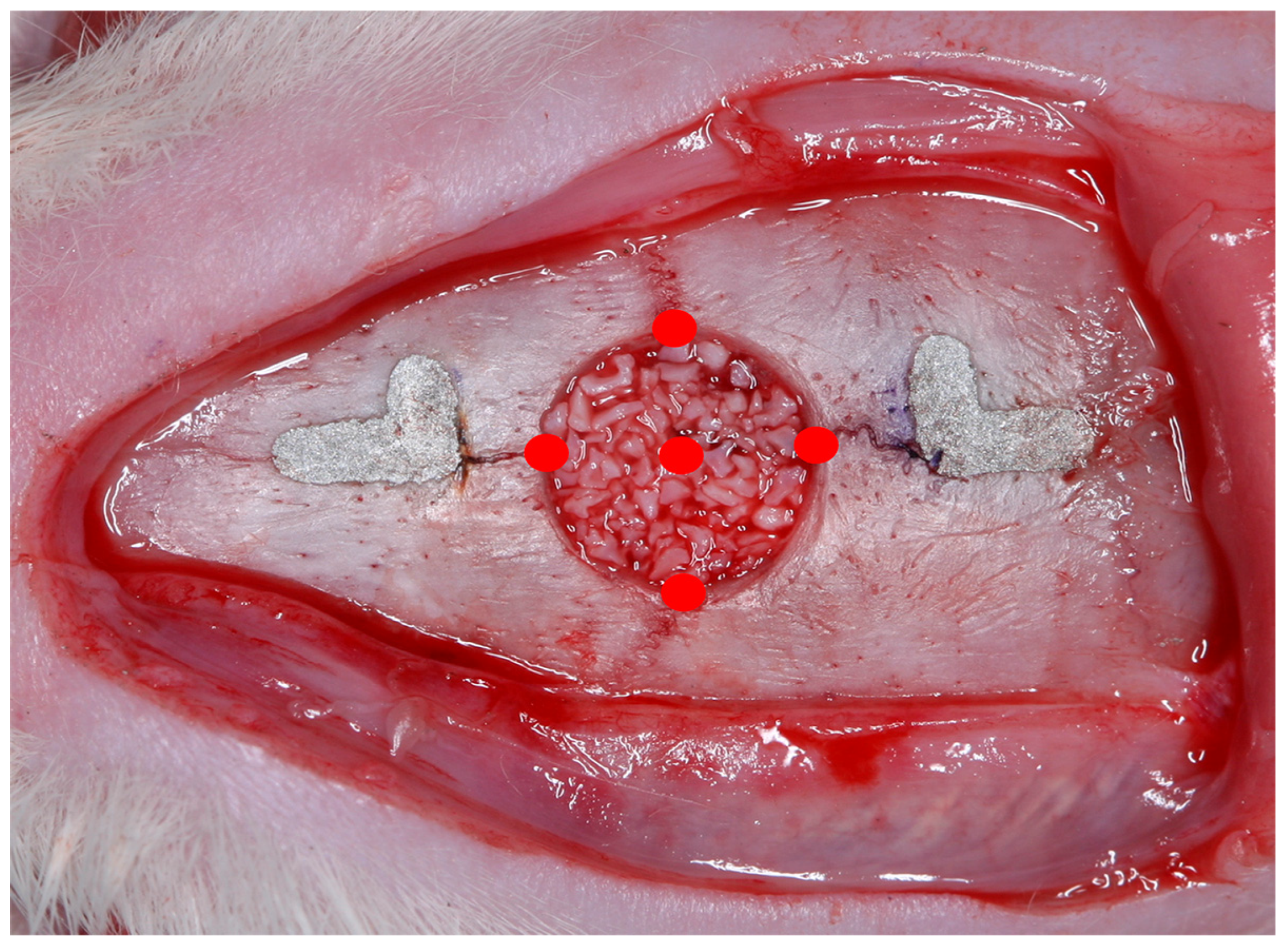
2.1. Experimental Model
2.2. Photobiomodulation
2.3. Tissue Processing
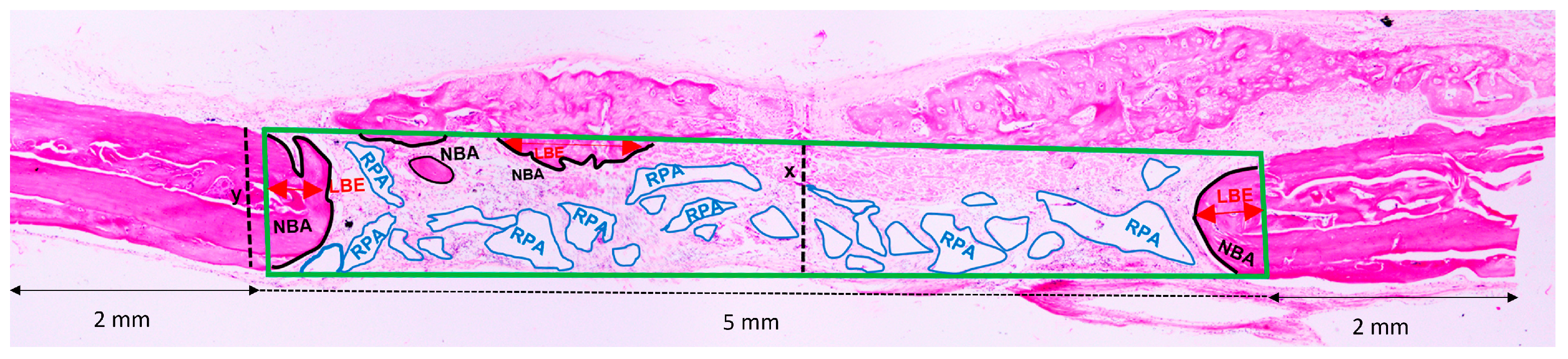
2.4. Histomorphometric Analysis
2.5. Statistical Analysis
3. Results
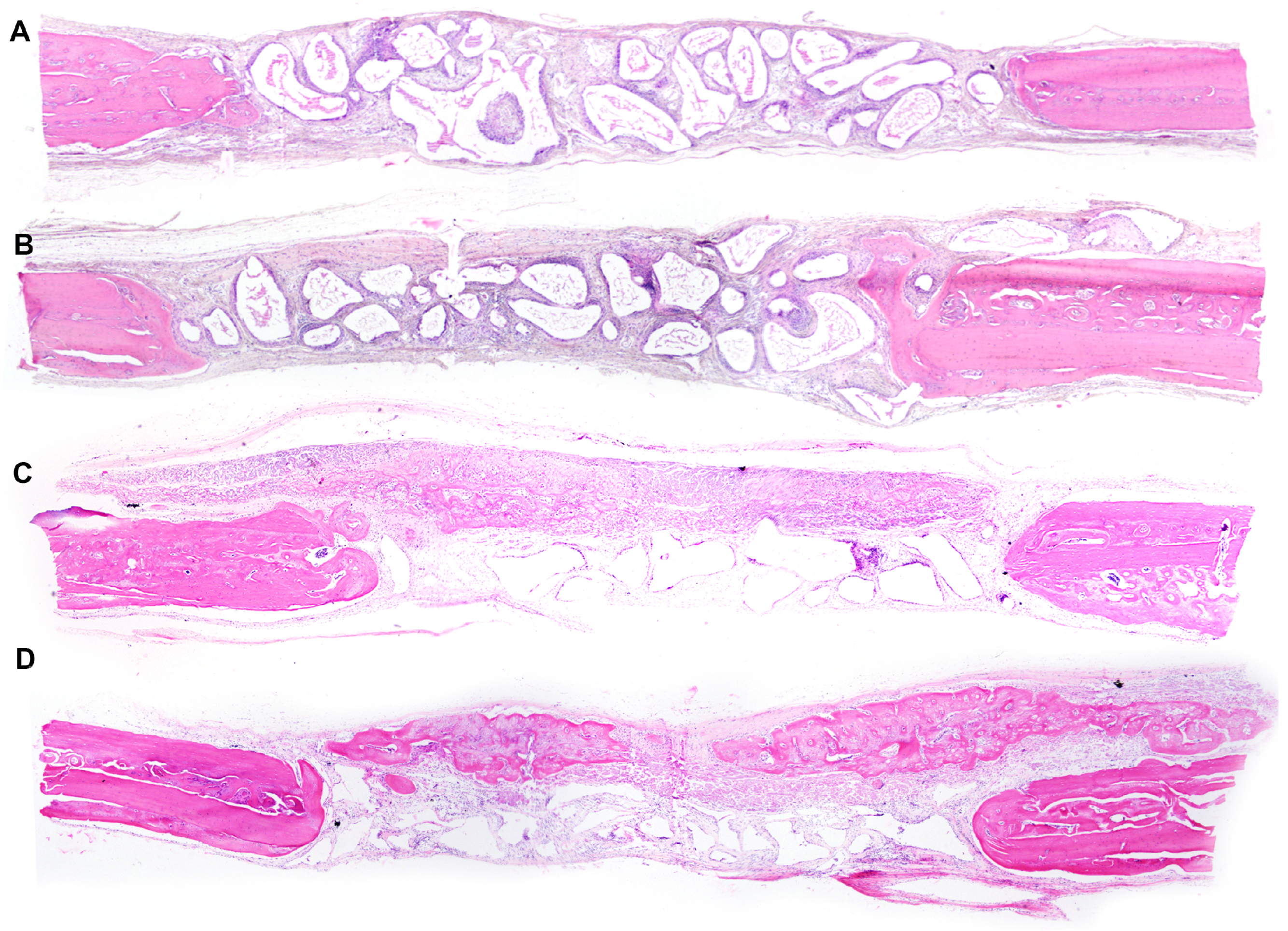
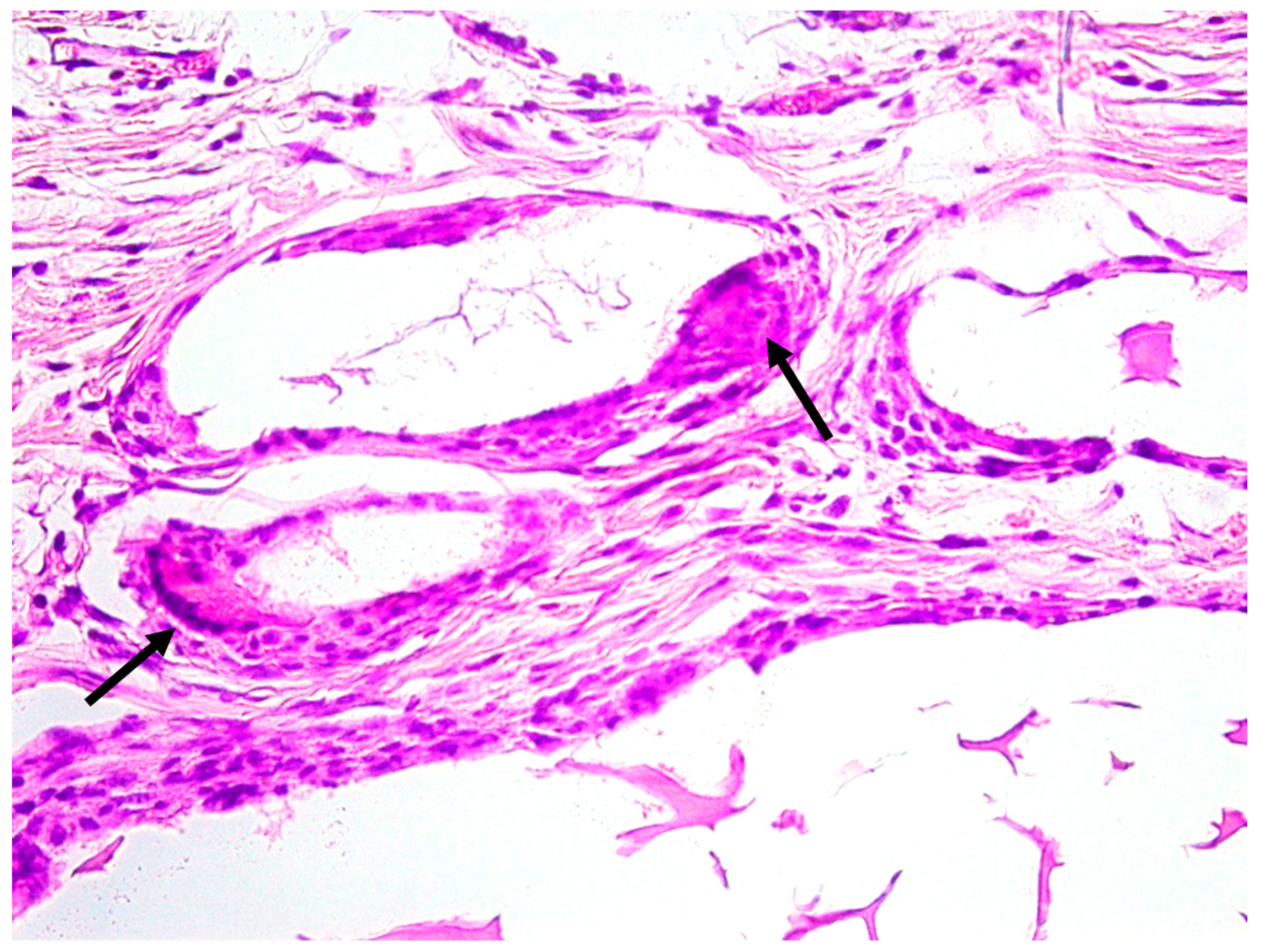
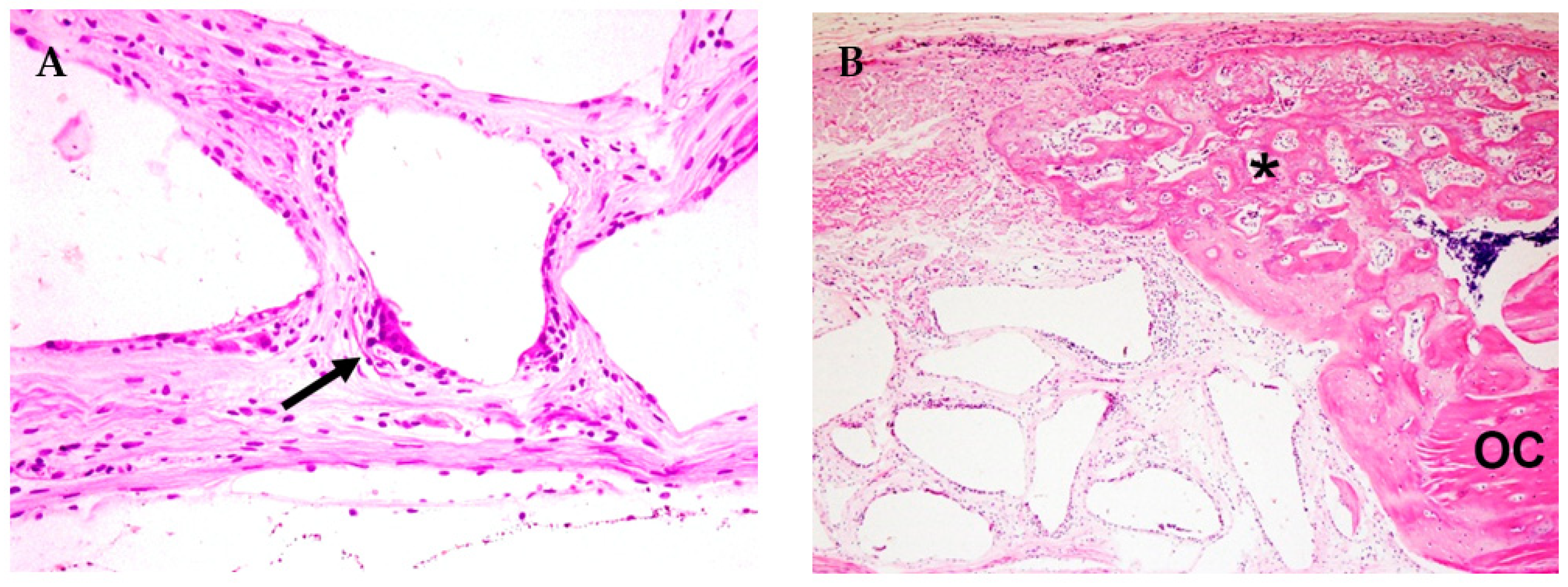
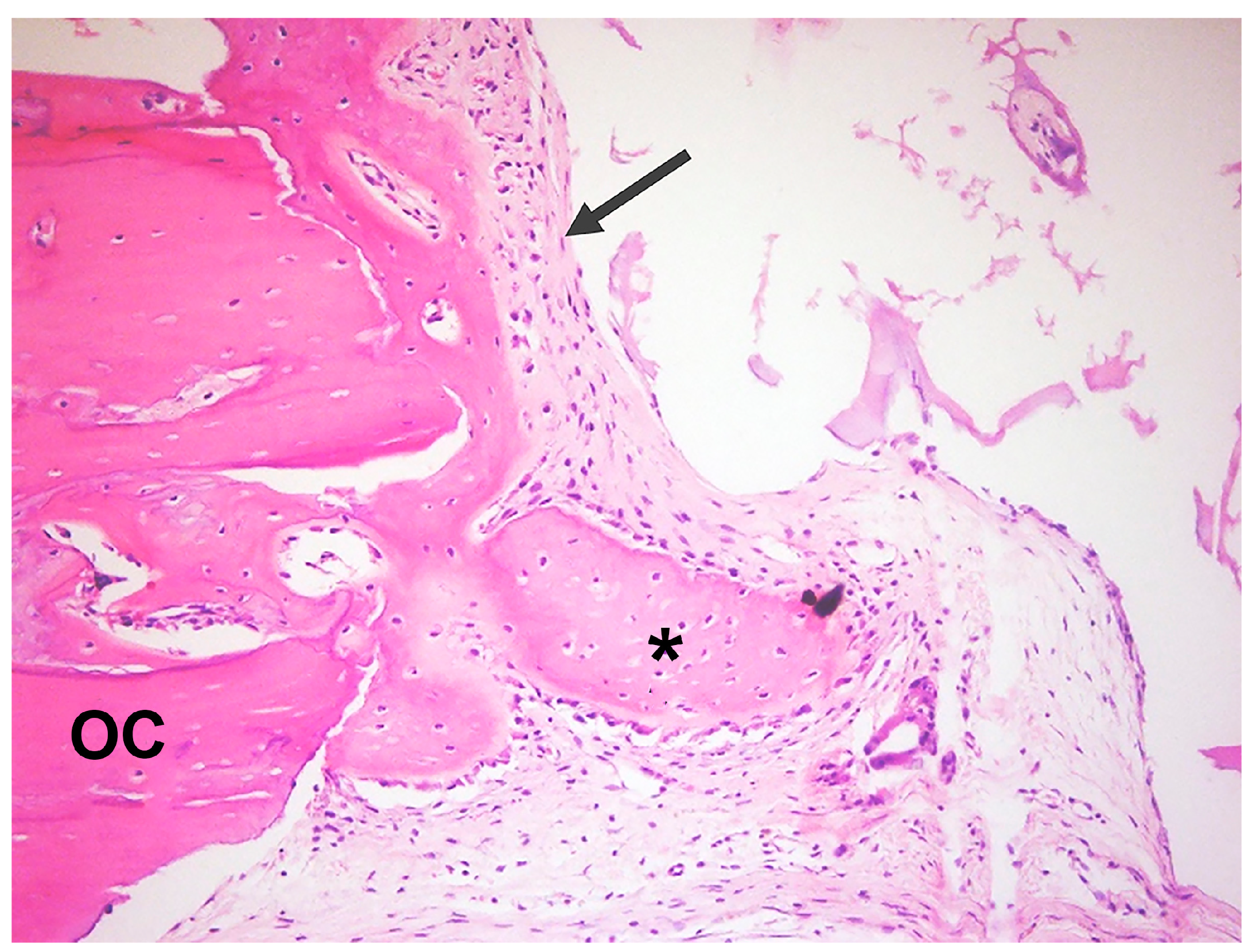
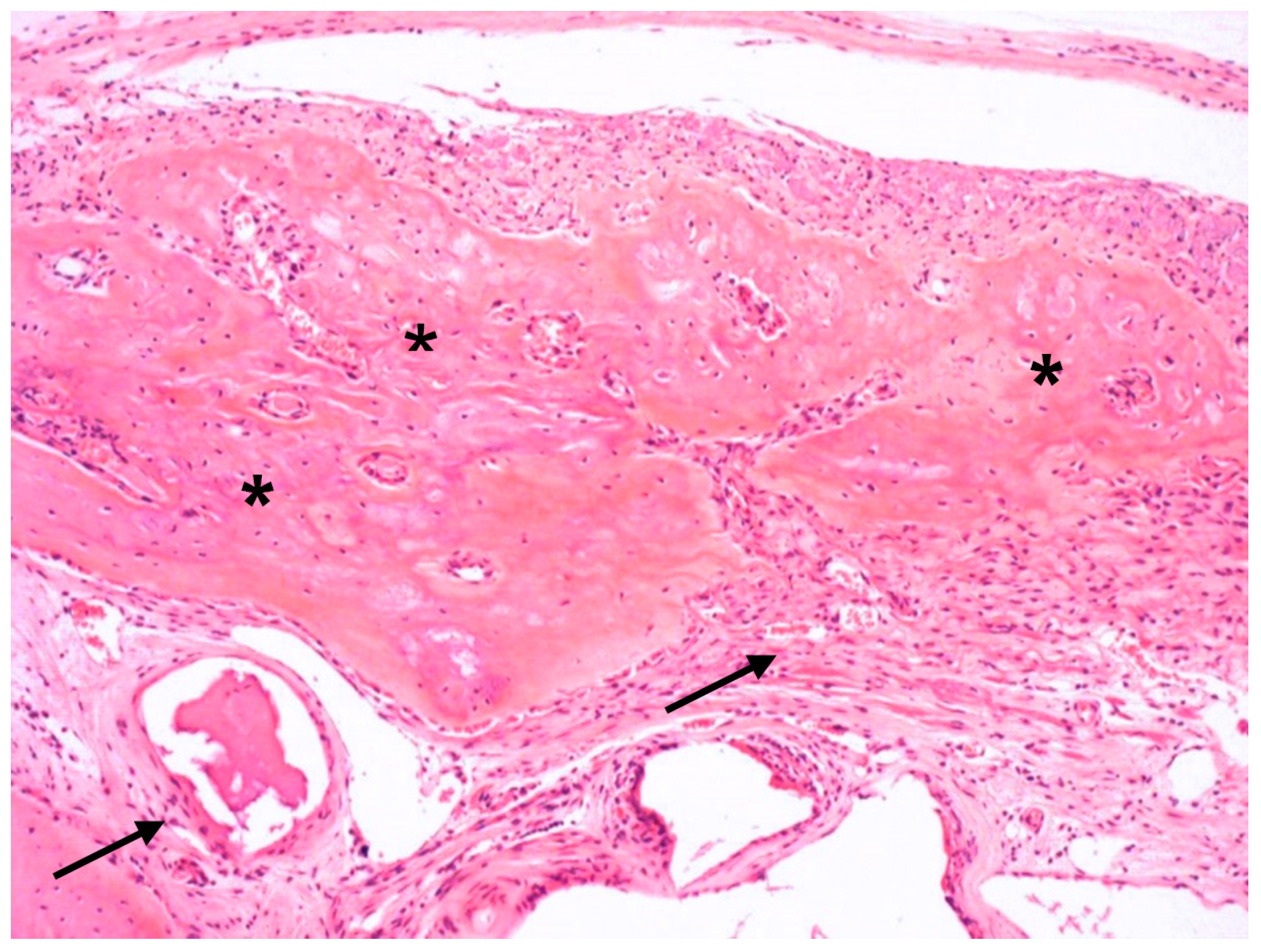
3.1. Qualitative Histological Analysis
3.2. Histometric and Statistical Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brunsvold, M.A.; Mellonig, J.T. Bone grafts and periodontal regeneration. Periodontol. 2000 1993, 1, 80–91. [Google Scholar] [CrossRef] [PubMed]
- Hoexter, D.L. Bone regeneration graft materials. J. Oral. Implantol. 2002, 28, 290–294. [Google Scholar] [CrossRef] [PubMed]
- Hallman, M.; Thor, A. Bone substitutes and growth factors as an alternative/complement to autogenous bone for grafting in implant dentistry. Periodontol. 2000 2008, 47, 172–192. [Google Scholar] [CrossRef] [PubMed]
- Baldini, N.; De Sanctis, M.; Ferrari, M. Deproteinized bovine bone in periodontal and implant surgery. Dent. Mater. 2011, 27, 61–70. [Google Scholar] [CrossRef]
- Shamsoddin, E.; Houshmand, B.; Golabgiran, M. Biomaterial selection for bone augmentation in implant dentistry: A systematic review. J. Adv. Pharm. Technol. Res. 2019, 10, 46–50. [Google Scholar] [CrossRef]
- Ozawa, Y.; Shimizu, N.; Kariya, G.; Abiko, Y. Low-energy laser irradiation stimulates bone nodule formation at early stages of cell cultures in rat calvarial cells. Bone 1998, 22, 347–354. [Google Scholar] [CrossRef]
- de Almeida, A.L.P.F.; Medeiros, I.L.; Cunha, M.J.; Sbrana, M.C.; de Oliveira, P.G.; Esper, L.A. The effect of low-level laser on bone healing in critical size defects treated with or without autogenous bone graft. An experimental study in rat calvaria. Clin. Oral. Implant. Res. 2014, 25, 1131–1136. [Google Scholar] [CrossRef]
- Cunha, M.J.; Esper, L.A.; Sbrana, M.C.; de Oliveira, P.G.; do Valle, A.L.; de Almeida, A.L.P.F. Effect of low-level laser on bone defects treated with bovine or autogenous bone grafts: In Vivo study in rat calvaria. BioMed Res. Int. 2014, 2014, 104230. [Google Scholar] [CrossRef]
- de Oliveira, G.J.P.L.; Aroni, M.A.T.; Medeiros, M.C.; Marcantonio, E., Jr.; Marcantonio, R.A.C. Effect of low-level laser therapy on the healing of sites grafted with coagulum, deproteinized bovine bone, and biphasic ceramic made of hydroxyapatite and β-tricalcium phosphate. In vivo study in rats. Lasers Surg. Med. 2018, 50, 651–660. [Google Scholar] [CrossRef]
- Jonasson, T.H.; Zancan, R.; de Oliveira Azevedo, L.; Fonseca, A.C.; Silva, M.C.D.; Giovanini, A.F.; Zielak, J.C.; Araujo, M.R. Effects of low-level laser therapy and platelet concentrate on bone repair: Histological, histomorphometric, immunohistochemical, and radiographic study. J. Craniomaxillofac. Surg. 2017, 45, 1846–1853. [Google Scholar] [CrossRef]
- Rosso, M.P.d.O.; Buchaim, D.V.; Pomini, K.T.; Della Coletta, B.B.; Reis, C.H.B.; Pilon, J.P.G.; Júnior, G.D.; Buchaim, R.L. Photobiomodulation Therapy (PBMT) Applied in Bone Reconstructive Surgery Using Bovine Bone Grafts: A Systematic Review. Materials 2019, 12, 4051. [Google Scholar] [CrossRef] [PubMed]
- Rufato, F.C.T.; de Sousa, L.G.; Scalize, P.H.; Gimenes, R.; Regalo, I.H.; Rosa, A.L.; Beloti, M.M.; Regalo, S.C.H.; Siéssere, S. Texturized P(VDF-TrFE)/BT membrane enhances bone neoformation in calvaria defects regardless of the association with photobiomodulation therapy in ovariectomized rats. Clin. Oral. Investig. 2022, 26, 1053–1065. [Google Scholar] [CrossRef] [PubMed]
- Torquato, L.C.; Suárez, E.A.C.; Bernardo, D.V.; Pinto, I.L.R.; Mantovani, L.O.; Silva, T.I.L.; Jardini, M.A.N.; Santamaria, M.P.; De Marco, A.C. Bone repair assessment of critical size defects in rats treated with mineralized bovine bone (Bio-Oss®) and photobiomodulation therapy: A histomorphometric and immunohistochemical study. Lasers Med. Sci. 2021, 36, 1515–1525. [Google Scholar] [CrossRef]
- Freitas, N.R.; Guerrini, L.B.; Esper, L.A.; Sbrana, M.C.; Dalben, G.S.; Soares, S.; de Almeida, A.L.P.F. Evaluation of photobiomodulation therapy associated with guided bone regeneration in critical size defects. In Vivo study. J. Appl. Oral. Sci. 2018, 26, e20170244. [Google Scholar] [CrossRef] [PubMed]
- Sbrana, M.C.; Esper, L.A.; de Freitas, N.R.; Guerrini, L.B.; Hernandes, P.H.J.; de Almeida, A.L.P.F. Evaluation of Different Photobiomodulation Therapy Protocols as Adjuncts in the Healing of Bone Defects Grafted with Inorganic Bovine Bone. Int. J. Oral. Maxillofac. Implant. 2022, 37, 1244–1249. [Google Scholar] [CrossRef]
- Buser, D.; Brägger, U.; Lang, N.P.; Nyman, S. Regeneration and enlargement of jaw bone using guided tissue regeneration. Clin. Oral. Implant. Res. 1990, 1, 22–32. [Google Scholar] [CrossRef]
- Kitayama, S.; Wong, L.O.; Ma, L.; Hao, J.; Kasugai, S.; Lang, N.P.; Mattheos, N. Regeneration of rabbit calvarial defects using biphasic calcium phosphate and a strontium hydroxyapatite-containing collagen membrane. Clin. Oral. Implant. Res. 2016, 27, 206–214. [Google Scholar] [CrossRef] [PubMed]
- Dimitriou, R.; Mataliotakis, G.I.; Calori, G.M.; Giannoudis, P.V. The role of barrier membranes for guided bone regeneration and restoration of large bone defects: Current experimental and clinical evidence. BMC Med. 2012, 10, 81. [Google Scholar] [CrossRef]
- Gerbi, M.E.; Pinheiro, A.L.; Marzola, C.; Limeira Júnior, F.A.; Ramalho, L.M.; Ponzi, E.A.; Soares, A.O.; Carvalho, L.C.; Lima, H.V.; Gonçalves, T.O. Assessment of bone repair associated with the use of organic bovine bone and membrane irradiated at 830 nm. Photomed. Laser Surg. 2005, 23, 382–388. [Google Scholar] [CrossRef]
- Sella, V.R.; do Bomfim, F.R.; Machado, P.C.; da Silva Morsoleto, M.J.; Chohfi, M.; Plapler, H. Effect of low-level laser therapy on bone repair: A randomized controlled experimental study. Lasers Med. Sci. 2015, 30, 1061–1068. [Google Scholar] [CrossRef]
- de Oliveira Gonçalves, J.B.; Buchaim, D.V.; de Souza Bueno, C.R.; Pomini, K.T.; Barraviera, B.; Júnior, R.S.F.; Andreo, J.C.; de Castro Rodrigues, A.; Cestari, T.M.; Buchaim, R.L. Effects of low-level laser therapy on autogenous bone graft stabilized with a new heterologous fibrin sealant. J. Photochem. Photobiol. B 2016, 162, 663–668. [Google Scholar] [CrossRef]
- Bosco, A.F.; Faleiros, P.L.; Carmona, L.R.; Garcia, V.G.; Theodoro, L.H.; de Araujo, N.J.; Nagata, M.J.H.; de Almeida, J.M. Effects of low-level laser therapy on bone healing of critical-size defects treated with bovine bone graft. J. Photochem. Photobiol. B 2016, 163, 303–310. [Google Scholar] [CrossRef]
- Pinheiro, A.L.; Gerbi, M.E. Photoengineering of bone repair processes. Photomed. Laser Surg. 2006, 24, 169–178. [Google Scholar] [CrossRef]
- da Silva, J.P.; da Silva, M.A.; Almeida, A.P.; Lombardi Junior, I.; Matos, A.P. Laser therapy in the tissue repair process: A literature review. Photomed. Laser Surg. 2010, 28, 17–21. [Google Scholar] [CrossRef]
- Scalize, P.H.; Sousa, L.G.; Regalo, S.C.H.; Semprini, M.; Pitol, D.L.; Da Silva, G.A.; Coelho, J.A.; Coppi, A.A.; Laad, A.A.B.L.; Prado, K.F.B.; et al. Low-level laser therapy improves bone formation: Stereology findings for osteoporosis in rat model. Lasers Med. Sci. 2015, 30, 1599–1607. [Google Scholar] [CrossRef]
- Khalil, N.M.; Noureldin, M.G. Comparison of Single Versus Multiple Low-Level Laser Applications on Bone Formation in Extraction Socket Healing in Rabbits (Histologic and Histomorphometric Study). J. Oral. Maxillofac. Surg. 2019, 77, 1760–1768. [Google Scholar] [CrossRef]
- Weber, J.B.; Pinheiro, A.L.; de Oliveira, M.G.; Oliveira, F.A.; Ramalho, L.M. Laser therapy improves healing of bone defects submitted to autologous bone graft. Photomed. Laser Surg. 2006, 24, 38–44. [Google Scholar] [CrossRef]
- Meme’, L.; Gallusi, G.; Coli, G.; Strappa, E.; Bambini, F.; Sampalmieri, F. Photobiomodulation to Reduce Orthodontic Treatment Time in Adults: A Historical Prospective Study. Appl. Sci. 2022, 12, 11532. [Google Scholar] [CrossRef]
- Nunes, C.M.M.; Ferreira, C.L.; Bernardo, D.V.; Oblack, G.B.; Longo, M.; Santamaria, M.P.; Jardini, M.A.N. The influence of LLLT applied on applied on calvarial defect in rats under effect of cigarette smoke. J. Appl. Oral. Sci. 2019, 27, e20180621. [Google Scholar] [CrossRef]
- Tunér, J. Photobiomodulation: How Many Sessions and How Often? Photomed. Laser Surg. 2018, 36, 59–60. [Google Scholar] [CrossRef]
- Nicola, R.A.; Jorgetti, V.; Rigau, J.; Pacheco, M.T.; dos Reis, L.M.; Zângaro, R.A. Effect of low-power GaAlAs laser (660 nm) on bone structure and cell activity: An experimental animal study. Lasers Med. Sci. 2003, 18, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Tetè, S.; Zara, S.; Vinci, R.; Zizzari, V.; Di Tore, U.; Mastrangelo, F.; Cataldi, A.; Gherlone, E. Vascular endothelial growth factor and e-nitric oxide synthase-mediated regenerative response occurring upon autologous and heterologous bone grafts. Int. J. Immunopathol. Pharmacol. 2009, 22, 1105–1116. [Google Scholar] [CrossRef] [PubMed]
- Zizzari, V.L.; Zara, S.; Tetè, G.; Vinci, R.; Gherlone, E.; Cataldi, A. Biological and clinical aspects of integration of diferente bone substitutes in oral surgery: A literature review. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. 2016, 122, 392–402. [Google Scholar] [CrossRef] [PubMed]
- Tamimi, F.M.; Torres, J.; Tresguerres, I.; Clemente, C.; Lopez-Cabarcos, E.; Blanco, L.J. Bone augmentation in rabbit calvariae: Comparative study between bio-oss and a novel betatcp/dcpd granulate. J. Clin. Periodontol. 2006, 33, 922–928. [Google Scholar] [CrossRef]
- Ezirganli, S.; Polat, S.; Baris, E.; Tatar, I.; Celik, H.H. Comparative investigation of the effects of different materials used with a titanium barrier on new bone formation. Clin. Oral. Implant. Res. 2013, 24, 312–319. [Google Scholar] [CrossRef]
- Carmagnola, D.; Adriaens, P.; Berglundh, T. Healing of human extraction sockets filled with Bio-Oss. Clin. Oral. Implant. Res. 2003, 14, 137–143. [Google Scholar] [CrossRef]
- Elgali, I.; Turri, A.; Xia, W.; Norlindh, B.; Johansson, A.; Dahlin, C.; Thomsen, P.; Omar, O. Guided bone regeneration using resorbable membrane and different bone substitutes: Early histological and molecular events. Acta Biomater. 2016, 29, 409–423. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | NBA | LBE | RPA | |
|---|---|---|---|---|
| N | DBBM | 10 | 10 | 10 |
| DBBM+P | 10 | 10 | 10 | |
| GBR | 9 | 9 | 9 | |
| GBR+P | 10 | 10 | 10 | |
| Mean | DBBM | 11.4 | 27.4 | 38.7 |
| DBBM+P | 48.6 | 76.2 | 16.7 | |
| GBR | 22.0 | 62.9 | 32.3 | |
| GBR+P | 19.0 | 48.9 | 24.2 | |
| Satandard deviation | DBBM | 7.8 | 15.5 | 6.9 |
| DBBM+P | 28.2 | 29.0 | 15.2 | |
| GBR | 10.7 | 21.6 | 6.2 | |
| GBR+P | 13.7 | 21.7 | 6.0 | |
| Median | DBBM | 9.4 | 23.6 | 37.7 |
| DBBM+P | 42.2 | 79.4 | 22.4 | |
| GBR | 19.9 | 71.9 | 32.4 | |
| GBR+P | 13.6 | 57.1 | 26.8 | |
| Q 25 | DBBM | 6.5 | 18.7 | 36.2 |
| DBBM+P | 35.9 | 51.9 | 0 | |
| GBR | 15.8 | 48.6 | 29.9 | |
| GBR+P | 9.6 | 34.1 | 21.2 | |
| Q75 | DBBM | 11.4 | 31.1 | 42.2 |
| DBBM+P | 74.6 | 96.8 | 27.5 | |
| GBR | 24.6 | 77.3 | 37.4 | |
| GBR+P | 28.2 | 62.4 | 28.3 |
| NBA | LBE | RPA | |
|---|---|---|---|
| DBBM × DBBM+P | 0.017 * | 0.005 * | 0.008 * |
| DBBM × GBR | 0.068 | 0.013 * | 0.238 |
| DBBM × GBR+P | 0.525 | 0.148 | 0.003 * |
| DBBM+P × GBR | 0.238 | 0.761 | 0.054 |
| DBBM+P × GBR+P | 0.106 | 0.232 | 0.666 |
| GBR × GBR+P | 0.713 | 0.663 | 0.017 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Freitas, N.R.d.; Guerrini, L.B.; Esper, L.A.; Sbrana, M.C.; Santos, C.C.V.d.; Almeida, A.L.P.F.d. Photobiomodulation and Inorganic Bovine Bone in Guided Bone Regeneration: Histomorphometric Analysis in Rats. J. Funct. Biomater. 2023, 14, 281. https://doi.org/10.3390/jfb14050281
Freitas NRd, Guerrini LB, Esper LA, Sbrana MC, Santos CCVd, Almeida ALPFd. Photobiomodulation and Inorganic Bovine Bone in Guided Bone Regeneration: Histomorphometric Analysis in Rats. Journal of Functional Biomaterials. 2023; 14(5):281. https://doi.org/10.3390/jfb14050281
Chicago/Turabian StyleFreitas, Nicole Rosa de, Luísa Belluco Guerrini, Luis Augusto Esper, Michyele Cristhiane Sbrana, Caroline Chepernate Vieira dos Santos, and Ana Lúcia Pompéia Fraga de Almeida. 2023. "Photobiomodulation and Inorganic Bovine Bone in Guided Bone Regeneration: Histomorphometric Analysis in Rats" Journal of Functional Biomaterials 14, no. 5: 281. https://doi.org/10.3390/jfb14050281
APA StyleFreitas, N. R. d., Guerrini, L. B., Esper, L. A., Sbrana, M. C., Santos, C. C. V. d., & Almeida, A. L. P. F. d. (2023). Photobiomodulation and Inorganic Bovine Bone in Guided Bone Regeneration: Histomorphometric Analysis in Rats. Journal of Functional Biomaterials, 14(5), 281. https://doi.org/10.3390/jfb14050281