


Guided Bone Regeneration Using a Novel Magnesium Membrane: A Literature Review and a Report of Two Cases in Humans


 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Literature Search and Review of Current Knowledge on Magnesium Membranes
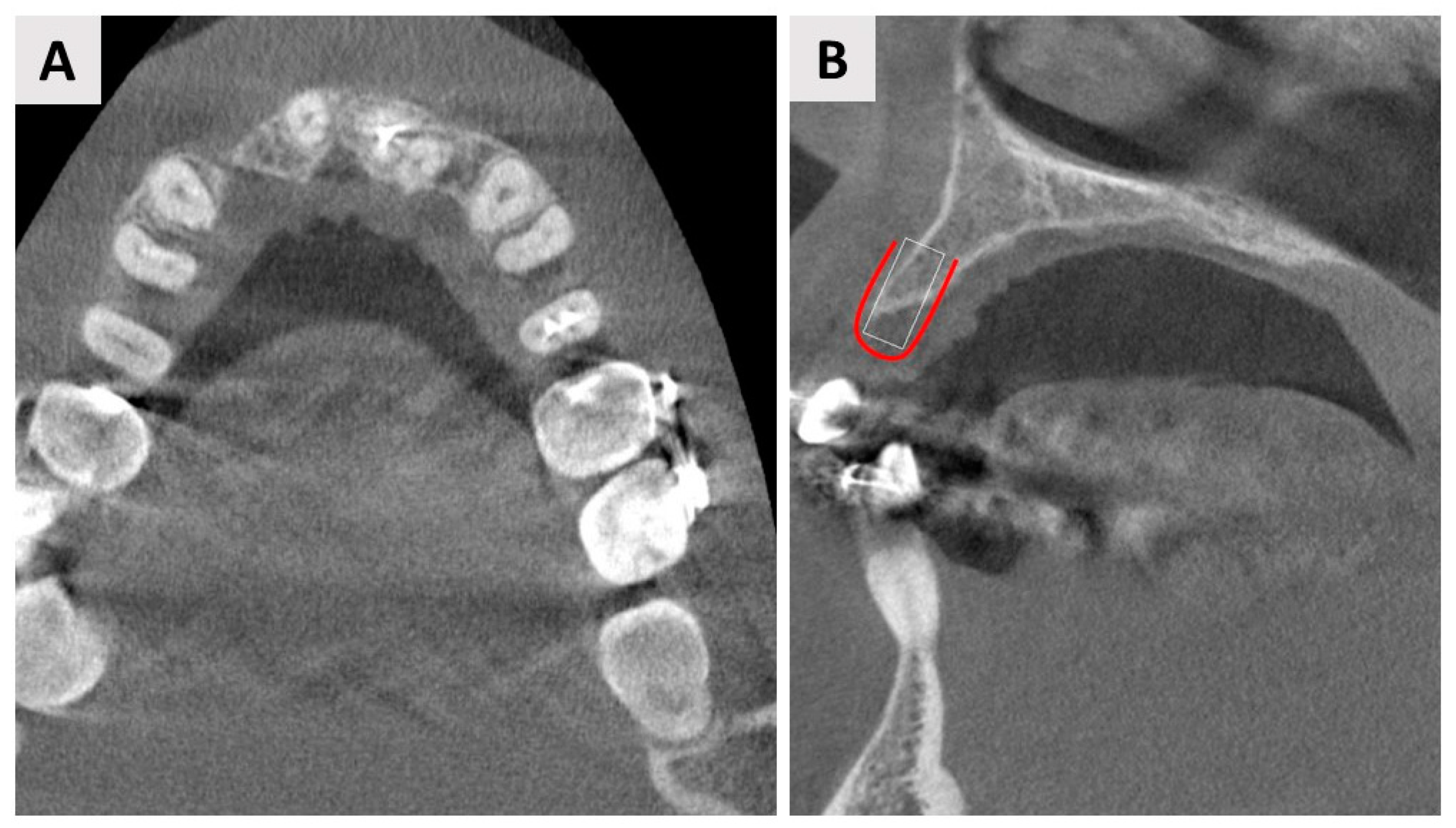
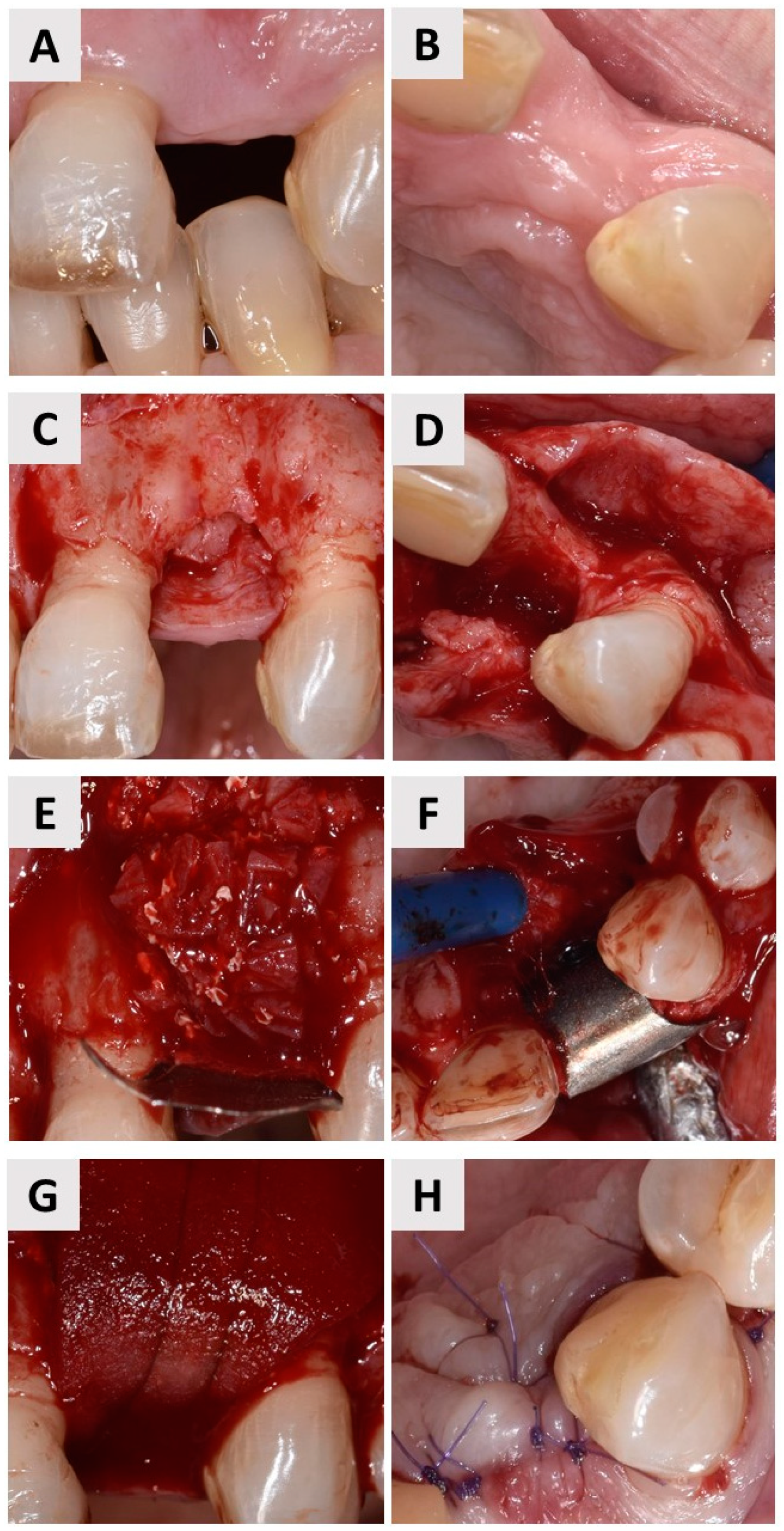
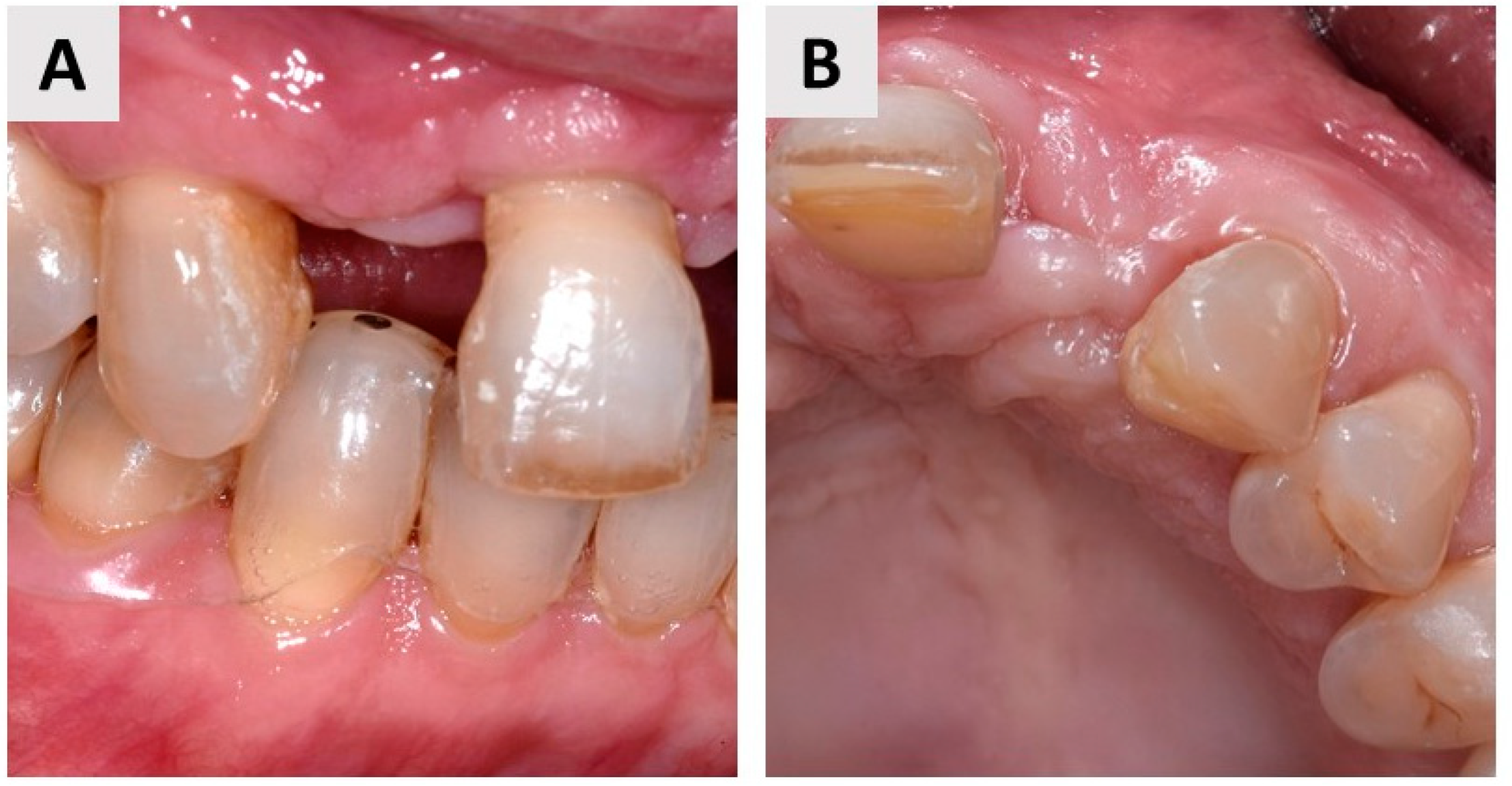
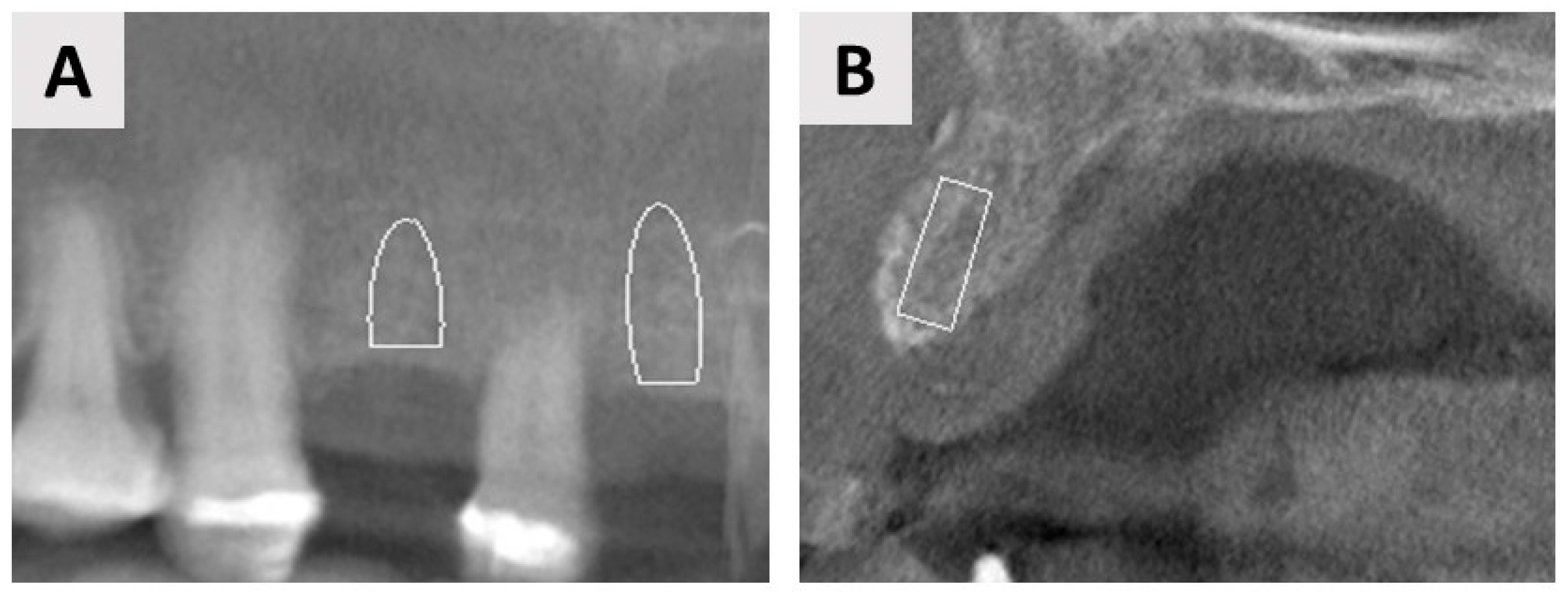
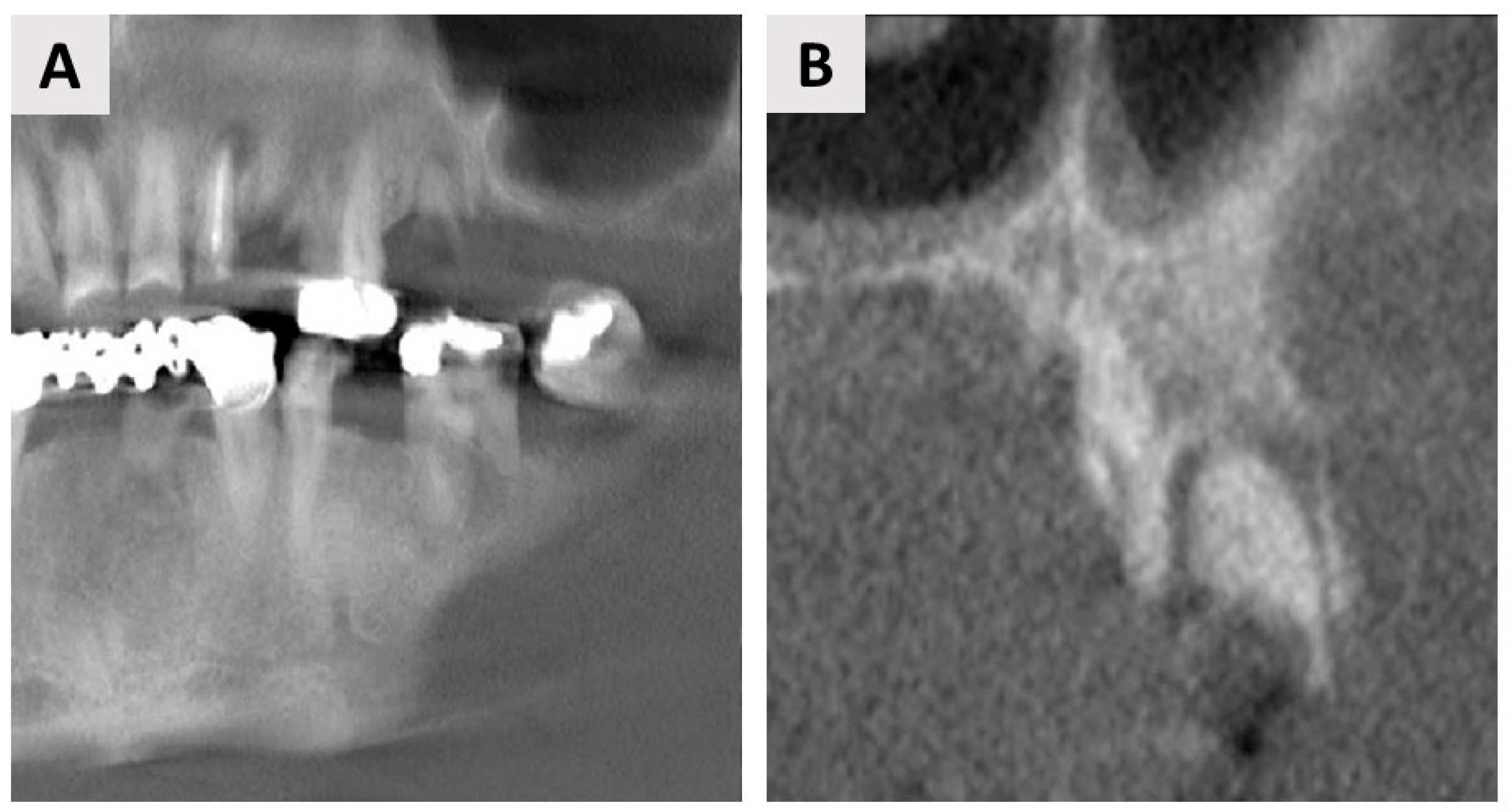
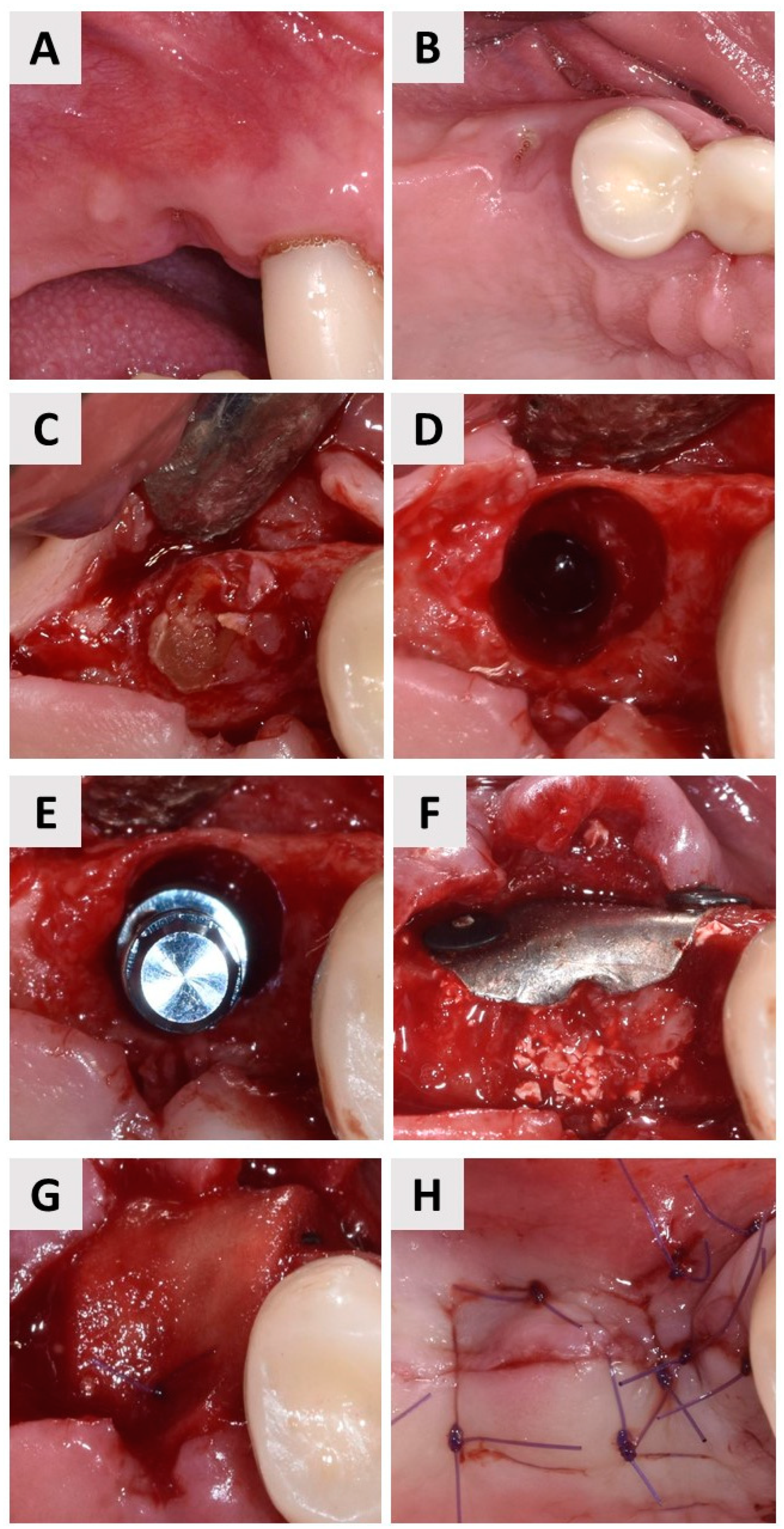
3. Case Report One: GBR with Delayed Implant Placement
4. Case Report Two: GBR with Immediate Implant Placement
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Urban, I.A.; Saleh, M.H.A.; Ravidà, A.; Forster, A.; Wang, H.L.; Barath, Z. Vertical Bone Augmentation Utilizing a Titanium-Reinforced PTFE Mesh: A Multi-Variate Analysis of Influencing Factors. Clin. Oral Implants Res. 2021, 32, 828–839. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, K.; Sailer, I.; Kataoka, Y.; Nogami, S.; Takahashi, T. Sandwich Bone Graft for Vertical Augmentation of the Posterior Maxillary Region: A Case Report with 9-Year Follow-Up. Int. J. Implant Dent. 2017, 3, 20. [Google Scholar] [CrossRef] [PubMed]
- Busenlechner, D.; Fürhauser, R.; Haas, R.; Watzek, G.; Mailath, G.; Pommer, B. Long-Term Implant Success at the Academy for Oral Implantology: 8-Year Follow-up and Risk Factor Analysis. J. Periodontal Implant Sci. 2014, 44, 102. [Google Scholar] [CrossRef]
- Khojasteh, A.; Kheiri, L.; Motamedian, S.; Khoshkam, V. Guided Bone Regeneration for the Reconstruction of Alveolar Bone Defects. Ann. Maxillofac. Surg. 2017, 7, 263. [Google Scholar] [CrossRef] [PubMed]
- Urban, I.A.; Montero, E.; Monje, A.; Sanz-Sánchez, I. Effectiveness of Vertical Ridge Augmentation Interventions: A Systematic Review and Meta-Analysis. J. Clin. Periodontol. 2019, 46, 319–339. [Google Scholar] [CrossRef]
- Elgali, I.; Omar, O.; Dahlin, C.; Thomsen, P. Guided Bone Regeneration: Materials and Biological Mechanisms Revisited. Eur. J. Oral Sci. 2017, 125, 315–337. [Google Scholar] [CrossRef]
- Omar, O.; Elgali, I.; Dahlin, C.; Thomsen, P. Barrier Membranes: More than the Barrier Effect? J. Clin. Periodontol. 2019, 46, 103–123. [Google Scholar] [CrossRef]
- Retzepi, M.; Donos, N. Guided Bone Regeneration: Biological Principle and Therapeutic Applications. Clin. Oral Implants Res. 2010, 21, 567–576. [Google Scholar] [CrossRef]
- Hämmerle, C.H.F.; Araújo, M.G.; Simion, M. Evidence-Based Knowledge on the Biology and Treatment of Extraction Sockets. Clin. Oral Implants Res. 2012, 23, 80–82. [Google Scholar] [CrossRef]
- Caballe-Serrano, J.; Munar-Frau, A.; Ortiz-Puigpelat, O.; Soto-Penaloza, D.; Penarrocha, M.; Hernandez-Alfaro, F. On the Search of the Ideal Barrier Membrane for Guided Bone Regeneration. J. Clin. Exp. Dent. 2018, 10, e477–e483. [Google Scholar] [CrossRef]
- Zitzmann, N.U.; Naef, R.; Scharer, P. Resorbable versus Nonresorbable Membranes in Combination with Bio-Oss for Guided Bone Regeneration—PubMed. Int. J. Oral Maxillofac. Implant. 1997, 12, 844–852. [Google Scholar]
- Thomaidis, V.; Kazakos, K.; Lyras, D.N.; Dimitrakopoulos, I.; Lazaridis, N.; Karakasis, D.; Botaitis, S.; Agrogiannis, G. Comparative Study of 5 Different Membranes for Guided Bone Regeneration of Rabbit Mandibular Defects beyond Critical Size. Med. Sci. Monit. 2008, 14, BR67–BR73. [Google Scholar] [PubMed]
- Barbeck, M.; Lorenz, J.; Holthaus, M.G.; Raetscho, N.; Kubesch, A.; Booms, P.; Sader, R.; Kirkpatrick, C.J.; Ghanaati, S. Porcine Dermis and Pericardium-Based, Non Cross-Linked Materials Induce Multinucleated Giant Cells after Their in Vivo Implantation: A Physiological Reaction? J. Oral Implantol. 2015, 41, e267–e280. [Google Scholar] [CrossRef] [PubMed]
- Sahin, A.; Gulabi, D.; Buyukdogan, H.; Agar, A.; Kilic, B.; Mutlu, I.; Erturk, C. Is the Magnesium Screw as Stable as the Titanium Screw in the Fixation of First Metatarsal Distal Chevron Osteotomy? A Comparative Biomechanical Study on Sawbones Models. J. Orthop. Surg. 2021, 23094990211056439. [Google Scholar] [CrossRef]
- Sezer, N.; Evis, Z.; Kayhan, S.M.; Tahmasebifar, A.; Koç, M. Review of Magnesium-Based Biomaterials and Their Applications. J. Magnes. Alloys 2018, 6, 23–43. [Google Scholar] [CrossRef]
- Atrens, A.; Song, G.-L.; Liu, M.; Shi, Z.; Cao, F.; Dargusch, M.S. Review of Recent Developments in the Field of Magnesium Corrosion. Adv. Eng. Mater. 2015, 17, 400–453. [Google Scholar] [CrossRef]
- Witte, F.; Hort, N.; Vogt, C.; Cohen, S.; Kainer, K.U.; Willumeit, R.; Feyerabend, F. Degradable Biomaterials Based on Magnesium Corrosion. Curr. Opin. Solid State Mater. Sci. 2008, 12, 63–72. [Google Scholar] [CrossRef]
- Kačarević, Ž.P.; Rider, P.; Elad, A.; Tadic, D.; Rothamel, D.; Sauer, G.; Bornert, F.; Windisch, P.; Hangyási, D.B.; Molnar, B.; et al. Biodegradable Magnesium Fixation Screw for Barrier Membranes Used in Guided Bone Regeneration. Bioact. Mater. 2022, 14, 15–30. [Google Scholar] [CrossRef]
- Rider, P.; Kačarević, Ž.P.; Elad, A.; Tadic, D.; Rothamel, D.; Sauer, G.; Bornert, F.; Windisch, P.; Hangyási, D.B.; Molnar, B.; et al. Biodegradable Magnesium Barrier Membrane Used for Guided Bone Regeneration in Dental Surgery. Bioact. Mater. 2022, 14, 152–168. [Google Scholar] [CrossRef]
- Elad, A.; Rider, P.; Rogge, S.; Witte, F.; Tadić, D.; Kačarević, Ž.P.; Steigmann, L. Application of Biodegradable Magnesium Membrane Shield Technique for Immediate Dentoalveolar Bone Regeneration. Biomedicines 2023, 11, 744. [Google Scholar] [CrossRef]
- Guo, Y.; Liu, W.; Ma, S.; Wang, J.; Zou, J.; Liu, Z.; Zhao, J.; Zhou, Y. A Preliminary Study for Novel Use of Two Mg Alloys (WE43 and Mg3Gd). J. Mater. Sci. Mater. Med. 2016, 27, 82. [Google Scholar] [CrossRef] [PubMed]
- Byun, S.H.; Lim, H.K.; Kim, S.M.; Lee, S.M.; Kim, H.E.; Lee, J.H. The Bioresorption and Guided Bone Regeneration of Absorbable Hydroxyapatite-Coated Magnesium Mesh. J. Craniofac. Surg. 2017, 28, 518–523. [Google Scholar] [CrossRef] [PubMed]
- Amberg, R.; Elad, A.; Rothamel, D.; Fienitz, T.; Szakacs, G.; Heilmann, S.; Witte, F. Design of a Migration Assay for Human Gingival Fibroblasts on Biodegradable Magnesium Surfaces. Acta Biomater. 2018, 79, 158–167. [Google Scholar] [CrossRef] [PubMed]
- Amberg, R.; Elad, A.; Beuer, F.; Vogt, C.; Bode, J.; Witte, F. Effect of Physical Cues of Altered Extract Media from Biodegradable Magnesium Implants on Human Gingival Fibroblasts. Acta Biomater. 2019, 98, 186–195. [Google Scholar] [CrossRef]
- Guo, Y.; Yu, Y.; Han, L.; Ma, S.; Zhao, J.; Chen, H.; Yang, Z.; Zhang, F.; Xia, Y.; Zhou, Y. Biocompatibility and Osteogenic Activity of Guided Bone Regeneration Membrane Based on Chitosan-Coated Magnesium Alloy. Mater. Sci. Eng. C. Mater. Biol. Appl. 2019, 100, 226–235. [Google Scholar] [CrossRef]
- Peng, W.; Chen, J.X.; Shan, X.F.; Wang, Y.C.; He, F.; Wang, X.J.; Tan, L.L.; Yang, K. Mg-Based Absorbable Membrane for Guided Bone Regeneration (GBR): A Pilot Study. Rare Met. 2019, 38, 577–587. [Google Scholar] [CrossRef]
- Wu, S.; Jang, Y.S.; Kim, Y.K.; Kim, S.Y.; Ko, S.O.; Lee, M.H. Surface Modification of Pure Magnesium Mesh for Guided Bone Regeneration: In Vivo Evaluation of Rat Calvarial Defect. Materials 2019, 12, 2684. [Google Scholar] [CrossRef]
- Barbeck, M.; Kühnel, L.; Witte, F.; Pissarek, J.; Precht, C.; Xiong, X.; Krastev, R.; Wegner, N.; Walther, F.; Jung, O. Degradation, Bone Regeneration and Tissue Response of an Innovative Volume Stable Magnesium-Supported GBR/GTR Barrier Membrane. Int. J. Mol. Sci. 2020, 21, 3098. [Google Scholar] [CrossRef]
- Steigmann, L.; Jung, O.; Kieferle, W.; Stojanovic, S.; Proehl, A.; Görke, O.; Emmert, S.; Najman, S.; Barbeck, M.; Rothamel, D. Biocompatibility and Immune Response of a Newly Developed Volume-Stable Magnesium-Based Barrier Membrane in Combination with a PVD Coating for Guided Bone Regeneration (GBR). Biomedicines 2020, 8, 636. [Google Scholar] [CrossRef]
- Dong, Y.; Yao, L.; Cai, L.; Jin, M.; Forouzanfar, T.; Wu, L.; Liu, J.; Wu, G. Antimicrobial and Pro-Osteogenic Coaxially Electrospun Magnesium Oxide Nanoparticles-Polycaprolactone /Parathyroid Hormone-Polycaprolactone Composite Barrier Membrane for Guided Bone Regeneration. Int. J. Nanomed. 2023, 18, 369–383. [Google Scholar] [CrossRef]
- Rider, P.; Kačarević, Ž.P.; Elad, A.; Rothamel, D.; Sauer, G.; Bornert, F.; Windisch, P.; Hangyási, D.; Molnar, B.; Hesse, B.; et al. Analysis of a Pure Magnesium Membrane Degradation Process and Its Functionality When Used in a Guided Bone Regeneration Model in Beagle Dogs. Materials 2022, 15, 3106. [Google Scholar] [CrossRef] [PubMed]
- Shan, X.; Xu, Y.; Kolawole, S.K.; Wen, L.; Qi, Z.; Xu, W.; Chen, J. Degradable Pure Magnesium Used as a Barrier Film for Oral Bone Regeneration. J. Funct. Biomater. 2022, 13, 298. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Xia, D.; Wang, S.; Gu, R.; Yang, F.; Zhao, X.; Liu, X.; Zhu, Y.; Liu, H.; Xu, Y.; et al. Photocrosslinkable Col/PCL/Mg Composite Membrane Providing Spatiotemporal Maintenance and Positive Osteogenetic Effects during Guided Bone Regeneration. Bioact. Mater. 2022, 13, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Yan, Z.Y.; Zhu, J.H.; Liu, G.Q.; Liu, Z.C.; Guo, C.B.; Cui, N.H.; Han, J.M. Feasibility and Efficacy of a Degradable Magnesium-Alloy GBR Membrane for Bone Augmentation in a Distal Bone-Defect Model in Beagle Dogs. Bioinorg. Chem. Appl. 2022, 2022, 4941635. [Google Scholar] [CrossRef] [PubMed]
- Witte, F. The History of Biodegradable Magnesium Implants: A Review. Acta Biomater. 2010, 6, 1680–1692. [Google Scholar] [CrossRef]
- Naenni, N.; Sapata, V.; Bienz, S.P.; Leventis, M.; Jung, R.E.; Hämmerle, C.H.F.; Thoma, D.S. Effect of Flapless Ridge Preservation with Two Different Alloplastic Materials in Sockets with Buccal Dehiscence Defects—Volumetric and Linear Changes. Clin. Oral Investig. 2018, 22, 2187–2197. [Google Scholar] [CrossRef]
- Mir-Mari, J.; Wui, H.; Jung, R.E.; Hämmerle, C.H.F.; Benic, G.I. Influence of Blinded Wound Closure on the Volume Stability of Different GBR Materials: An In Vitro Cone-Beam Computed Tomographic Examination. Clin. Oral Implants Res. 2016, 27, 258–265. [Google Scholar] [CrossRef]
- Naenni, N.; Schneider, D.; Jung, R.E.; Hüsler, J.; Hämmerle, C.H.F.; Thoma, D.S. Randomized Clinical Study Assessing Two Membranes for Guided Bone Regeneration of Peri-Implant Bone Defects: Clinical and Histological Outcomes at 6 Months. Clin. Oral Implants Res. 2017, 28, 1309–1317. [Google Scholar] [CrossRef]
- Rakhmatia, Y.D.; Ayukawa, Y.; Furuhashi, A.; Koyano, K. Current Barrier Membranes: Titanium Mesh and Other Membranes for Guided Bone Regeneration in Dental Applications. J. Prosthodont. Res. 2013, 57, 3–14. [Google Scholar] [CrossRef]
- Poinern, G.E.J.; Brundavanam, S.; Fawcett, D. Biomedical Magnesium Alloys: A Review of Material Properties, Surface Modifications and Potential as a Biodegradable Orthopaedic Implant. Am. J. Biomed. Eng. 2013, 2, 218–240. [Google Scholar] [CrossRef]
- Oshibe, N.; Marukawa, E.; Yoda, T.; Harada, H. Degradation and Interaction with Bone of Magnesium Alloy WE43 Implants: A Long-Term Follow-up in Vivo Rat Tibia Study. J. Biomater. Appl. 2019, 33, 1157–1167. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.; Shadanbaz, S.; Woodfield, T.B.F.; Staiger, M.P.; Dias, G.J. Magnesium Biomaterials for Orthopedic Application: A Review from a Biological Perspective. J. Biomed. Mater. Res. Part B Appl. Biomater. 2014, 102, 1316–1331. [Google Scholar] [CrossRef]
- Kay, S.A.; Wisner-Lynch, L.; Marxer, M.; Lynch, S.E. Guided Bone Regeneration: Integration of a Resorbable Membrane and a Bone Graft Material. Pract. Periodontics Aesthet. Dent. 1997, 9, 185–194. [Google Scholar] [PubMed]
- Rider, P.; Kačarević, Ž.P.; Elad, A.; Rothamel, D.; Sauer, G.; Bornert, F.; Windisch, P.; Hangyási, D.; Molnar, B.; Hesse, B.; et al. Biodegradation of a Magnesium Alloy Fixation Screw Used in a Guided Bone Regeneration Model in Beagle Dogs. Materials 2022, 15, 4111. [Google Scholar] [CrossRef]
- Banerjee, P.C.; Al-Saadi, S.; Choudhary, L.; Harandi, S.E.; Singh, R. Magnesium Implants: Prospects and Challenges. Materials 2019, 12, 136. [Google Scholar] [CrossRef]
- Jung, O.; Hesse, B.; Stojanovic, S.; Seim, C.; Weitkamp, T.; Batinic, M.; Goerke, O.; Kačarević, Ž.P.; Rider, P.; Najman, S.; et al. Biocompatibility Analyses of HF-Passivated Magnesium Screws for Guided Bone Regeneration (GBR). Int. J. Mol. Sci. 2021, 22, 12567. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Title | Year | Study Type | Aim | Tested Biomaterial | Outcomes | Reference |
|---|---|---|---|---|---|---|---|
| Guo et al. | A preliminary study for novel use of two Mg alloys (WE43 and Mg3Gd) | 2016 | In vitro/in vivo | The aim of this research was to investigate two types of magnesium alloys (WE43 and Mg3Gd) compared with the Heal-All® (Yantai Zhenghai Biotechnology Co., Shandong, China) membrane to determine whether the alloys can be used as biodegradable membranes | Magnesium alloy sheet (WE43 and Mg3Gd) | Degradation rate results for WE43 and Mg3Gd alloys showed no significant difference, but both Mg alloys corroded faster than Heal-All® membrane. All three types of materials showed good biocompatibility | [21] |
| Byun et al. | The bioresorption and guided bone regeneration of absorbable hydroxyapatite-coated magnesium mesh | 2017 | In vivo (the rat calvarium) | The purpose of this study was to evaluate the absorption capacity of magnesium mesh coated with hydroxyapatite | Magnesium mesh coated with hydroxyapatite | A magnesium mesh coated with hydroxyapatite was shown to provide a reasonable process of bioresorption and bone reaction | [22] |
| Amberg et al. | Design of a migration assay for human gingival fibroblasts on biodegradable magnesium surfaces | 2018 | In vivo | The aim of this study was to investigate the migration behavior of human gingival fibroblasts on the surface of magnesium | The pure magnesium membrane | The results of this study showed that human gingiva fibroblasts adhered to and formed confluent layers on a precorroded magnesium membrane surface; however, the cells migrated more slowly over the surface compared to plastic and titanium | [23] |
| Amberg et al. | Effect of physical cues of altered extract media from biodegradable magnesium implants on human gingival fibroblasts | 2019 | In vivo | The aim of the study was to investigate the effects of minerals such as Mg2+, Ca2+, H2 and increased osmolality, as well as the effects of magnesium extracts, on human gingival fibroblasts (HGFs) in terms of their migration, proliferation, and viability | Pure magnesium membrane (NovaMag® membrane, botiss biomaterials, Zossen, Germany, Mg purity: 99.95%) | The migration rate of HGFs tends to slow down when the ratio of Mg2+ and Ca2+ changes because the concentration of Mg2+ increases and the concentration of Ca2+ decreases near the corroding magnesium implant | [24] |
| Guo et al. | Biocompatibility and osteogenic activity of guided bone regeneration membrane based on chitosan-coated magnesium alloy | 2019 | In vitro and in vivo (rabbit calvaria) | The objective was to evaluate the performance of chitosan–magnesium membrane prepared with a specific protocol for the needs of the study and to compare the results with the commercially available membrane Heal-All® (Yantai Zhenghai Biotechnology Co., Shandong, China) | Composite chitosan–magnesium (CS-Mg) membrane fabricated by dip-coating Mg alloy into chitosan solution | In vitro: CS-Mg had a suitable degradation rate and similar cell adhesion and cytocompatibility as commercially available membrane In vivo: new bone formation was good in both groups compared to the blank control. There were no significant differences between the CS-Mg and Heal-All® groups (p > 0.1) | [25] |
| Peng et al. | Mg-based absorbable membrane for guided bone regeneration (GBR): A pilot study | 2019 | In vitro/in vivo | The aim of this study is to investigate microstructural characteristics and perform electrochemical testing, immersion testing, fluorescent labeling analysis, and histopathological evaluation of magnesium membrane coated with calcium phosphate | Calcium phosphate-coated Mg membrane | The Ca–P coating increased the corrosion resistance of the Mg membrane in vitro and in vivo and achieved better results than pure Ti membranes in terms of membrane duration | [26] |
| Wu et al. | Surface modification of pure magnesium mesh for guided bone regeneration: In vivo evaluation of rat calvarial defect | 2019 | In vivo (rat calvaria defect) | The aim of this research was the surface modification of pure magnesium mesh using plasma electrolytic oxidation and hydrothermal treatment | Magnesium mesh with a protective layer that mainly consisted of Mg (OH)2 with amorphous calcium phosphate | Biodegradation of the magnesium mesh was found to be significantly retarded, and surface modification of Mg could also improve volume and bone density of the calvarial defect compared to that of pure Mg mesh | [27] |
| Barbeck et al. | Degradation, bone regeneration and tissue response of an innovative volume stable magnesium-supported GBR/GTR barrier membrane | 2020 | In vitro/in vivo | The aim of this research was to investigate a new bioresorbable hydrofluoric acid (HF)-treated magnesium (Mg) mesh in native collagen membrane for stable-volume situations | Hydrofluoric acid (HF)-treated magnesium (Mg) mesh | In vitro: Mg treated with HF showed higher cytocompatibility. Histopathologically, HF-Mg prevented gas voids while untreated Mg showed partially significantly more gas voids and fibrotic tissue reaction. In vivo: bone regeneration was not significantly different between all groups | [28] |
| Steigmann et al. | Biocompatibility and immune response of a newly developed volume-stable magnesium-based barrier membrane in combination with a PVD coating for guided bone regeneration (GBR) | 2020 | In vitro and in vivo (the subscapular region of BALB/c mice) | The aim of the study was to analyze a new approach based on ion implantation (II) with a PVD coating for passivation of newly developed Mg membranes for GBR/GTR procedures | Mg membranes were passivated by ion implantation in an argon atmosphere followed by PVD treatment using a specially designed coating system | In vitro: untreated and PVD-coated membranes were not cytocompatible as static conditions could not be used for magnesium in vitro tests. Both types of membranes showed good biocompatibility in in vivo studies | [29] |
| Rider et al. | Biodegradable magnesium barrier membrane used for guided bone regeneration in dental surgery | 2021 | In vitro and in vivo (Yucatan minipigs) | The aim of this study was to analyze chemical and mechanical properties, in vitro corrosion, and in vivo corrosion in Yucatan minipigs | NOVAMag® membrane (botiss biomaterials, Zossen, Germany) | The magnesium membrane exhibited mechanical stability that allowed satisfactory shielding of the augmentation site. The magnesium membrane was completely resorbed, and bone healing was completed before current standards for treating patients with a second surgical procedure | [19] |
| Dong et al. | Antimicrobial and pro-osteogenic coaxially electrospun magnesium oxide nanoparticles-polycaprolactone/parathyroid hormone-polycaprolactone composite barrier membrane for guided bone regeneration | 2022 | In vitro/in vivo | The goal was to produce an antibacterial and pro-osteogenic coaxial electrospun membrane for guided bone regeneration (GBR) from nanofibers to meet the complicated phasic requirements of the GBR process | GBR membrane of coaxially electrospun nanofibers with parathyroid hormone (PTH) encapsulation in the central layer and magnesium oxide nanoparticles (MgONP) in the shell layer (MgONP-PCL/PTH-PCL) | MgONP-PCL/PTH-PCL showed remarkable antibacterial potential through the release of MgONPs. It was also found that the incorporation of MgONP significantly prolonged the release of PTH. High-dose PTH promotes membrane pro-osteogenicity to improve the efficiency of bone regeneration in the presence of MgONP | [30] |
| Rider et al. | Analysis of a pure magnesium membrane degradation process and its functionality when used in a guided bone regeneration model in beagle dogs | 2022 | In vivo (beagle dogs) | The aim was to evaluate the degradation process and the potential for tissue regeneration of a pure magnesium membrane and to compare it with the commonly used collagen membrane | NOVAMag® membrane (botiss biomaterials, Zossen, Germany) | The greatest rate of magnesium membrane degradation was seen between 1 and 8 weeks after implantation and continued until week 16. New bone formation was similar in both groups, suggesting that magnesium membrane may be an alternative to collagen membrane | [31] |
| Shan et al. | Degradable pure magnesium used as a barrier film for oral bone regeneration | 2022 | In vitro and in vivo (cranial parietal bone of experimental rabbits) | The aim was to conduct electrochemical tests, immersion tests, and in vivo tests to investigate the potential of the magnesium membrane as a barrier membrane | Pure Mg membrane surface treated with micro-arc oxidation (MAO) | In vitro: experimental results showed that the corrosion resistance of MAO-treated pure Mg membrane was better than that of uncoated pure Mg, and cell experiments showed no cytotoxicity. In vivo: MAO-Mg membrane showed better biological activity than pure Ti membrane in the early stage of implantation and good bone regeneration ability | [32] |
| Wang et al. | Photocrosslinkable Col/PCL/Mg composite membrane providing spatiotemporal maintenance and positive osteogenetic effects during guided bone regeneration | 2022 | In vitro/in vivo | The aim was to design a photocrosslinkable collagen/polycaprolactone methacryloyl/magnesium (Col/PCLMA/Mg) composite membrane that provides a spatiotemporal support effect after photocrosslinking | A photocrosslinkable collagen/polycaprolactone methacryloyl/magnesium (Col/PCLMA/Mg) composite membrane | Col/PCL and Col/PCL/Mg membranes showed a much higher elastic modulus and lower swelling rate than Col membranes, and there were no differences in cell biocompatibility between groups. Col/PCL and Col/PCL/Mg membranes had lower degradation rates than Col membranes. Col/PCL/Mg groups showed improved osteogenic ability compared to Col groups | [33] |
| Yan et al. | Feasibility and efficacy of a degradable magnesium-alloy GBR membrane for bone augmentation in a distal bone-defect model in beagle dogs | 2022 | In vivo (beagle dogs) | The aim of the study was to investigate the effectiveness and feasibility of guided bone regeneration using a degradable magnesium alloy for the healing of bone defects after tooth extraction | Degradable Mg alloy regeneration membrane (MAR-Gide (MG)) | Mg alloy membrane regeneration did not increase the prevalence of infection, dehiscence, or subcutaneous emphysema compared to those who used Bio-Gide. It also showed good biocompatibility and clinical applicability | [34] |
| Elad et al. | Application of biodegradable magnesium membrane shield technique for immediate dentoalveolar bone regeneration | 2023 | Clinical case series (humans) | The aim was to demonstrate the first clinical usage of a magnesium metal membrane in a shield technique | NOVAMag® membrane (botiss biomaterials, Zossen, Germany) | In all presented clinical cases, there was good regeneration of bone tissue and healing of soft tissue | [20] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blašković, M.; Butorac Prpić, I.; Blašković, D.; Rider, P.; Tomas, M.; Čandrlić, S.; Botond Hangyasi, D.; Čandrlić, M.; Perić Kačarević, Ž. Guided Bone Regeneration Using a Novel Magnesium Membrane: A Literature Review and a Report of Two Cases in Humans. J. Funct. Biomater. 2023, 14, 307. https://doi.org/10.3390/jfb14060307
Blašković M, Butorac Prpić I, Blašković D, Rider P, Tomas M, Čandrlić S, Botond Hangyasi D, Čandrlić M, Perić Kačarević Ž. Guided Bone Regeneration Using a Novel Magnesium Membrane: A Literature Review and a Report of Two Cases in Humans. Journal of Functional Biomaterials. 2023; 14(6):307. https://doi.org/10.3390/jfb14060307
Chicago/Turabian StyleBlašković, Marko, Ivana Butorac Prpić, Dorotea Blašković, Patrick Rider, Matej Tomas, Slavko Čandrlić, David Botond Hangyasi, Marija Čandrlić, and Željka Perić Kačarević. 2023. "Guided Bone Regeneration Using a Novel Magnesium Membrane: A Literature Review and a Report of Two Cases in Humans" Journal of Functional Biomaterials 14, no. 6: 307. https://doi.org/10.3390/jfb14060307
APA StyleBlašković, M., Butorac Prpić, I., Blašković, D., Rider, P., Tomas, M., Čandrlić, S., Botond Hangyasi, D., Čandrlić, M., & Perić Kačarević, Ž. (2023). Guided Bone Regeneration Using a Novel Magnesium Membrane: A Literature Review and a Report of Two Cases in Humans. Journal of Functional Biomaterials, 14(6), 307. https://doi.org/10.3390/jfb14060307