
The Effect of Superstructures Connected to Implants with Different Surface Properties on the Surrounding Bone

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results and Discussion
2.1. General Characteristics of Implants
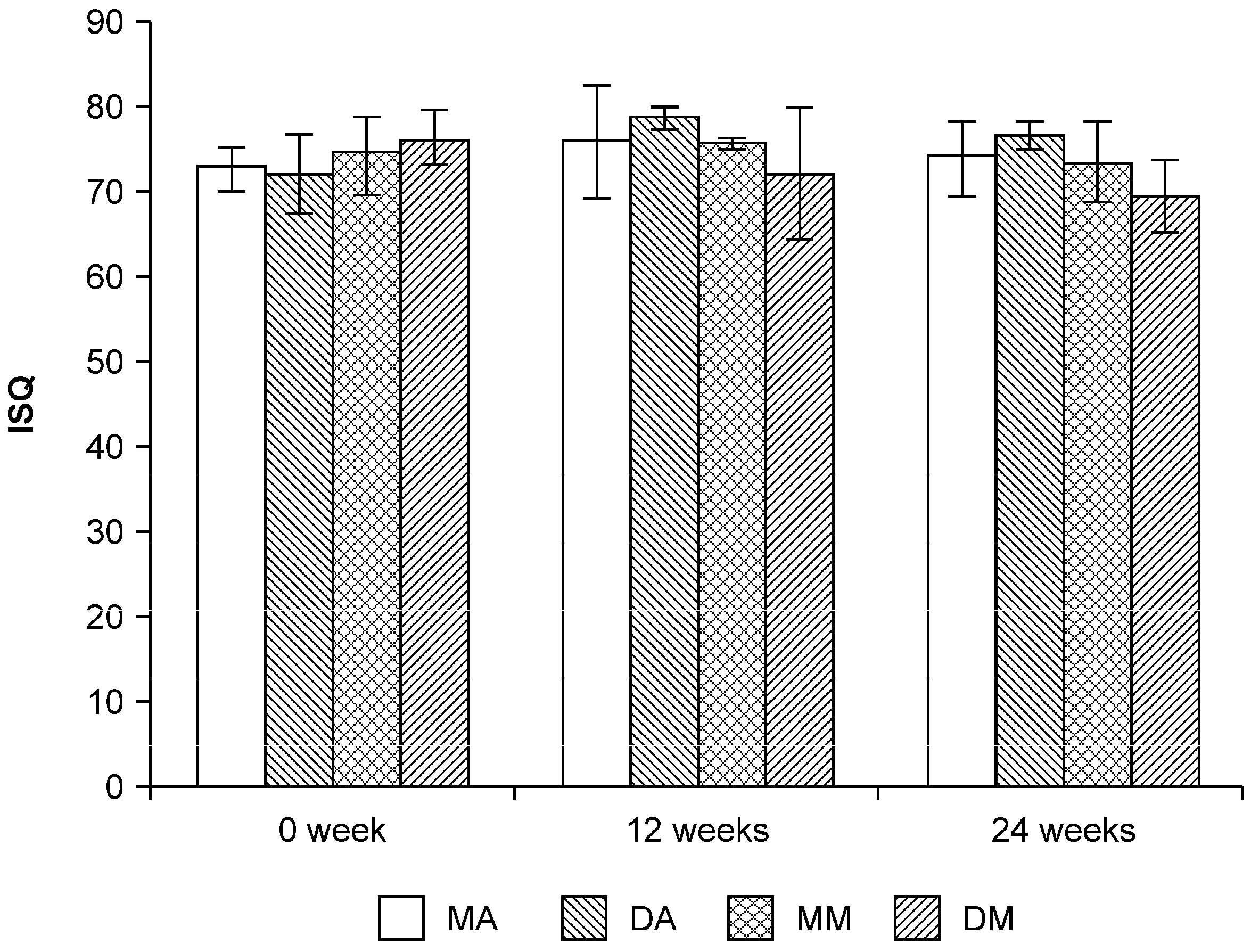
2.2. Implant Stability Quotient (ISQ) Values

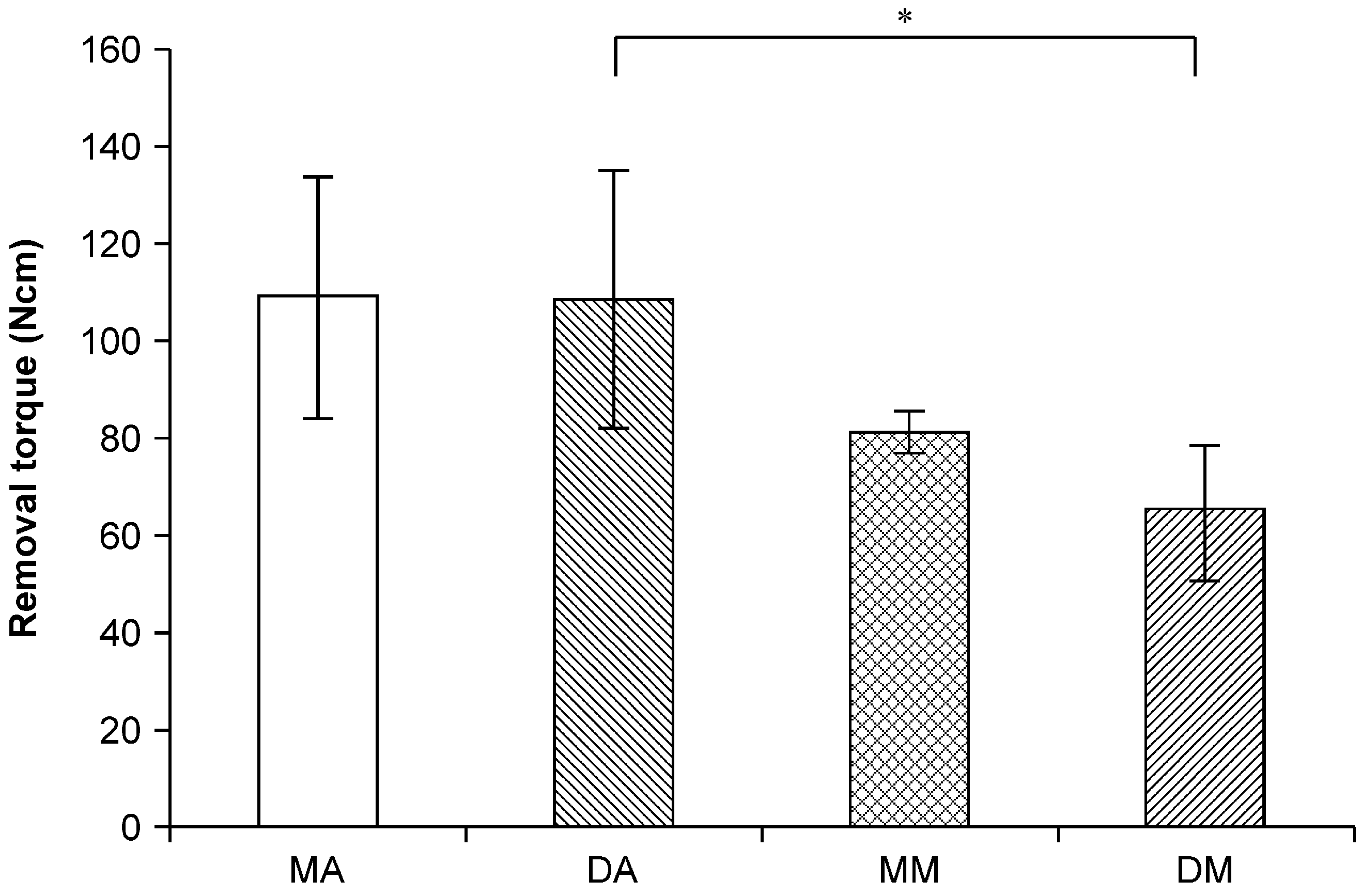
2.3. Removal Torque Values

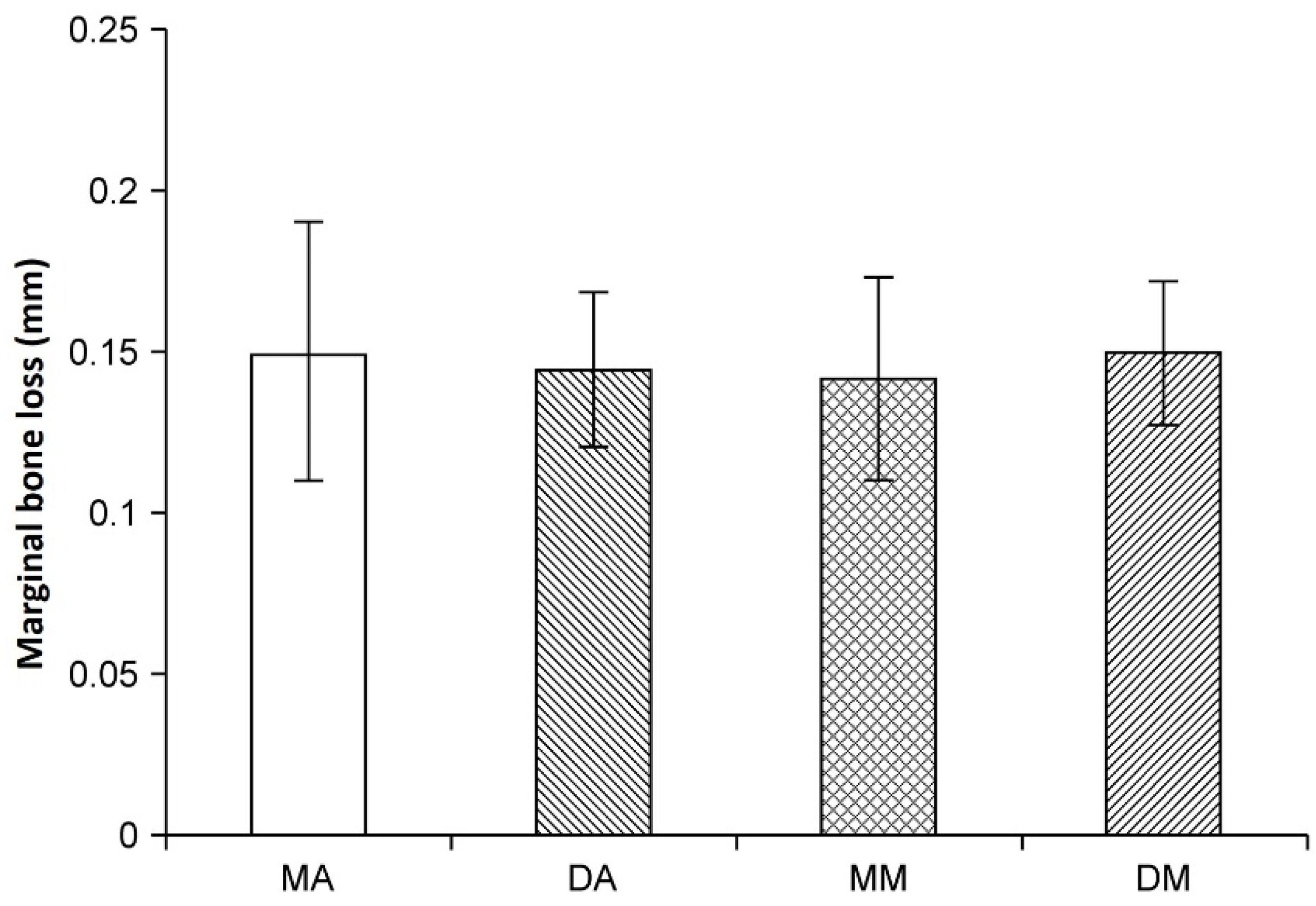
2.4. X-ray Observations

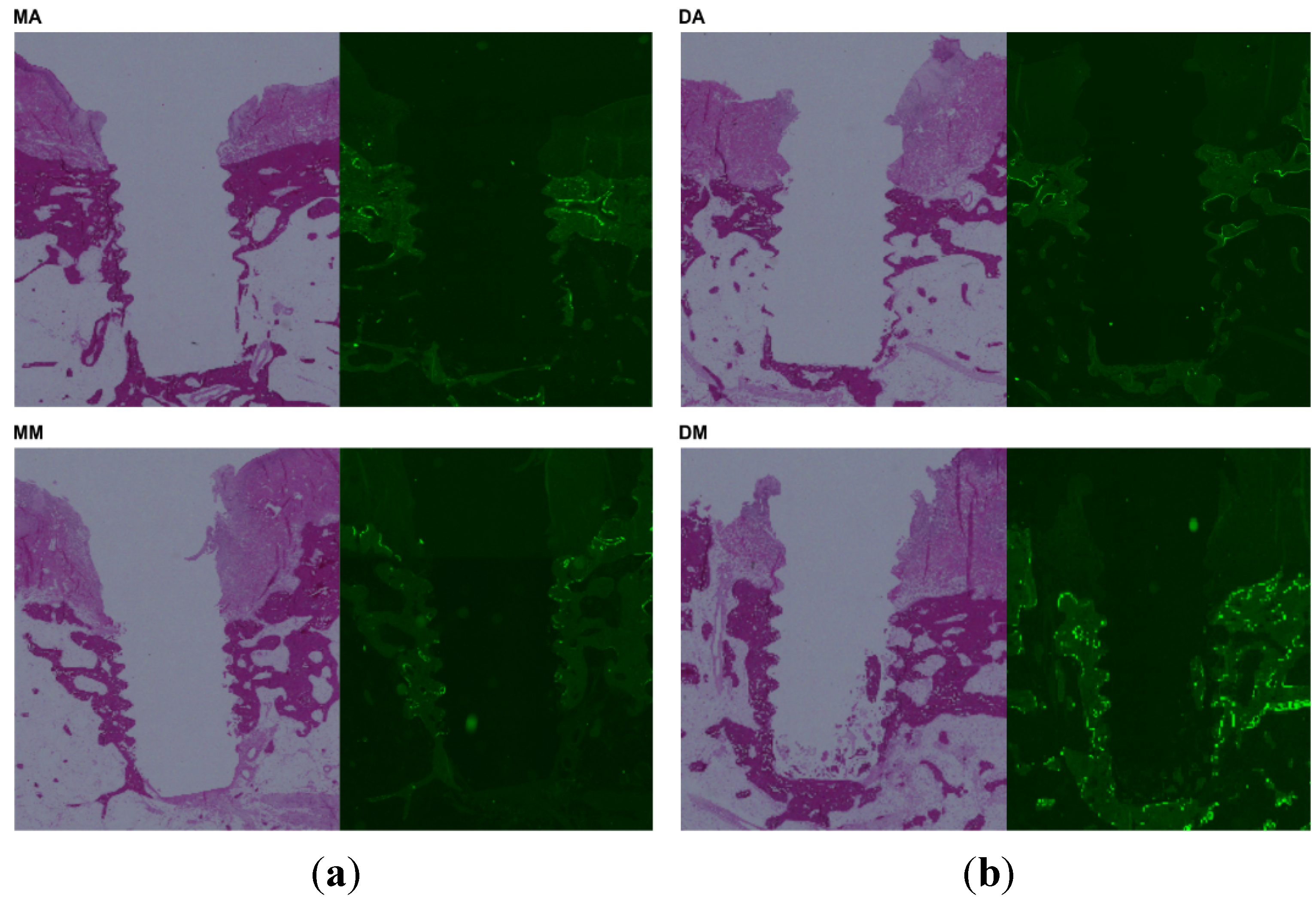
2.5. Histological Observation

2.6. Discussion
3. Experimental Section
3.1. Ethics Statement
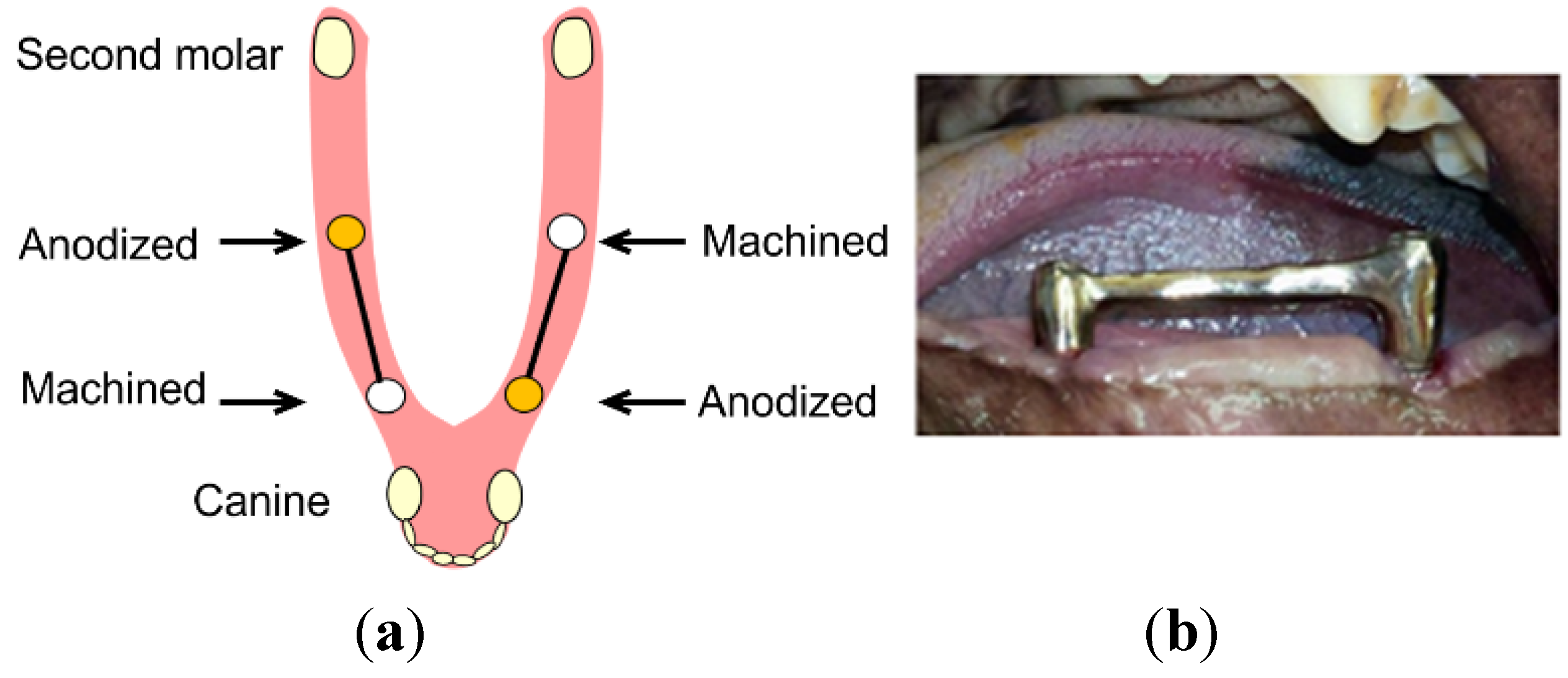
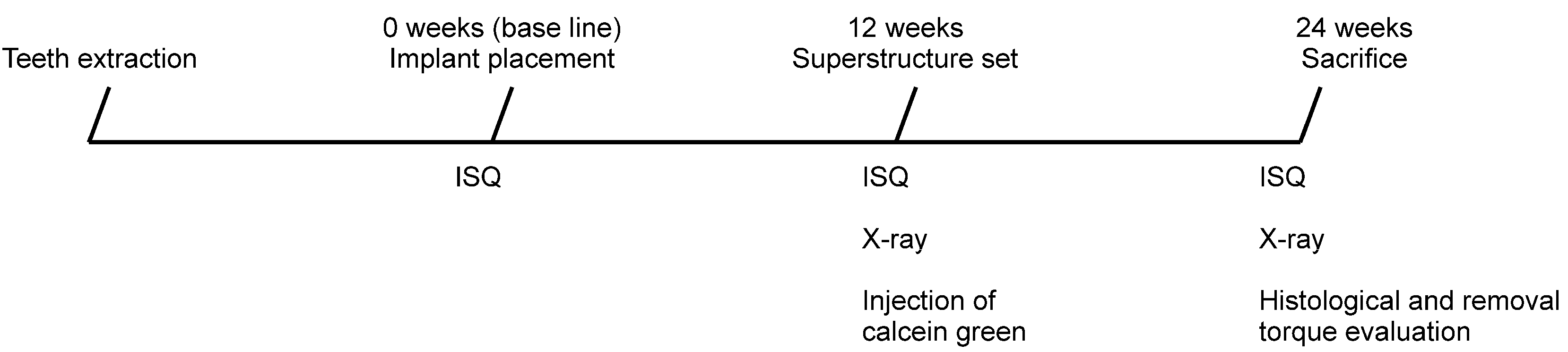
3.2. Study Design


3.3. Implant Stability Evaluation
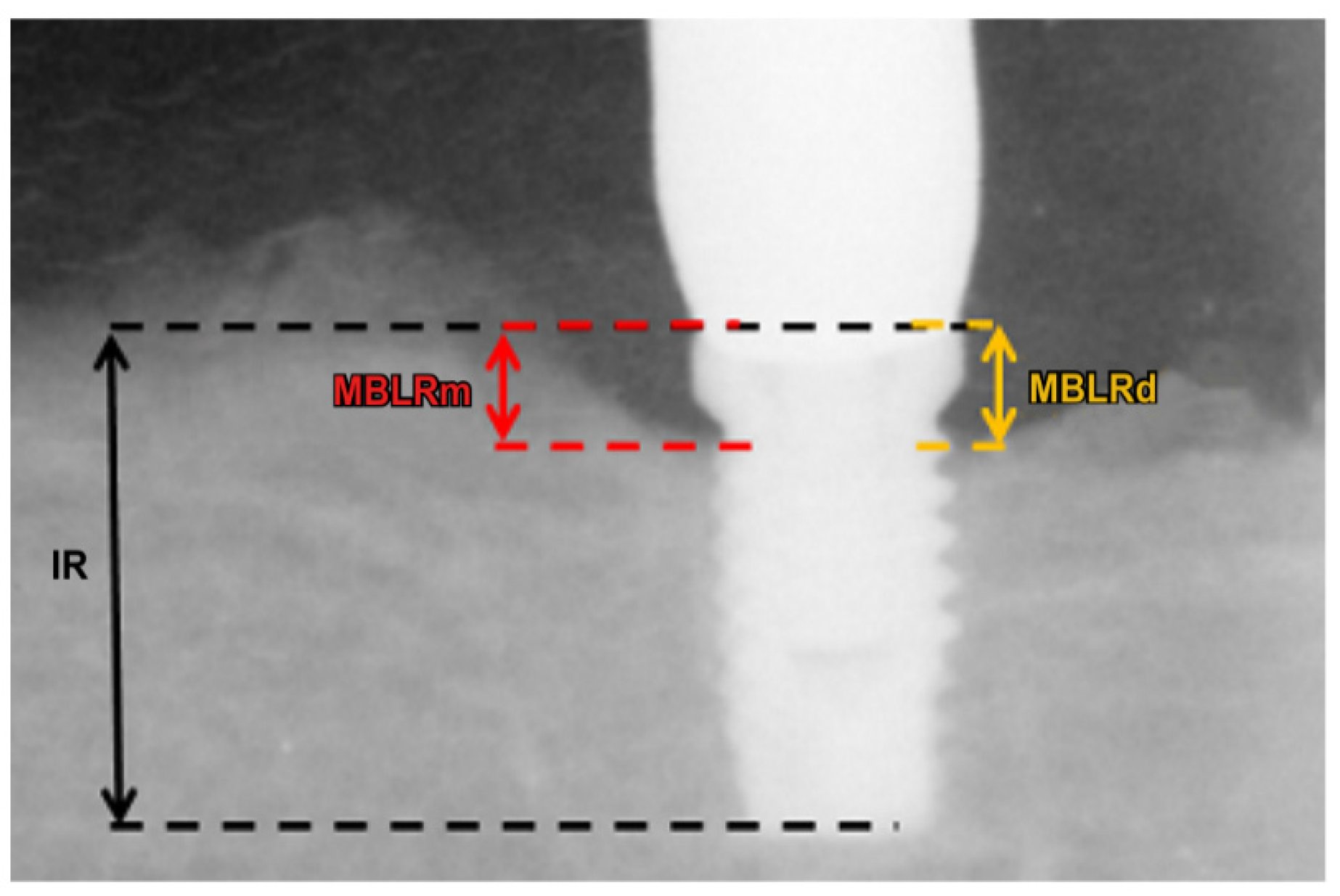
3.4. Radiographic Evaluation

3.5. Removal Torque Evaluation

3.6. Histological Evaluation
3.7. Statistical Analysis
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Brånemark, P.I.; Hansson, B.O.; Adell, R.; Breine, U.; Lindström, J.; Hallén, O.; Ohman, A. Osseointegrated implants in the treatment of edentulous jaw. Experience from a 10-year period. Scand. J. Plast. Reconstr. Surg. Suppl. 1977, 16, 1–132. [Google Scholar] [PubMed]
- Quirynen, M.; Herrera, D.; Teughels, W.; Sanz, M. Implant Therapy: 40 years of experience. Periodontol. 2000 2014, 66, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Wyatt, C.C.; Zarb, G.A. Treatment outcomes of patients with implant-supported fixed partial prostheses. Int. J. Oral Maxillofac. Implants 1998, 13, 204–211. [Google Scholar] [PubMed]
- Romeo, E.; Lops, D.; Margutti, E.; Ghisolfi, M.; Chiapasco, M.; Vogel, G. Long-term survival and success of oral implants in the treatment of full and partial arches: A 7-year prospective study with the ITI dental implant system. Int. J. Oral Maxillofac. Implants 2004, 19, 247–259. [Google Scholar] [PubMed]
- Bavbek, A.B.; Dogan, A.; Cehreli, M.C. Biomechanics of implant-tooth supported prostheses: Effects of mesiodistal implant angulation and mode of prosthesis connection. J. Appl. Biomater. Biomech. 2011, 9, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Zarone, F.; Apicella, A.; Nicolais, L.; Aversa, R.; Sorrentino, R. Mandibular flexure and stress build-up in mandibular full-arch fixed prostheses supported by osseointegrated implants. Clin. Oral Implants Res. 2003, 14, 103–114. [Google Scholar] [CrossRef] [PubMed]
- Hirata, I.; Yoshida, Y.; Nagaoka, N.; Hiasa, K.; Abe, Y.; Maekawa, K.; Kuboki, T.; Akagawa, Y.; Suzuki, K.; Meerbeek, B.V.; et al. Real time assessment of surface interactions with a titanium passivation layer by surface plasmon resonance. Acta Biomater. 2012, 8, 1260–1266. [Google Scholar] [CrossRef] [PubMed]
- Okada, S.; Koretake, K.; Miyamoto, Y.; Oue, H.; Akagawa, Y. Increased crown-to-implant ratio may not be a risk factor for dental implant failure under appropriate plaque control. PLoS One 2013, 8, e63992. [Google Scholar] [CrossRef] [PubMed]
- Glauser, R.; Portmann, M.; Ruhstaller, P.; Lundgren, A.K.; Hämmerle, C.; Gottlow, J. Stability measurements of immediately loaded machined and oxidized implants in the posterior maxilla. A comparative clinical study using resonance frequency analysis. Appl. Osseonteg. Res. 2001, 2, 27–29. [Google Scholar]
- Barewal, R.M.; Oates, T.W.; Meredith, N.; Cochran, D.L. Resonance frequency measurement of implant stability in vivo on implants with a sandblasted and acid-etched surface. Int. J. Oral Maxillofac. Implants 2003, 18, 641–651. [Google Scholar] [PubMed]
- Gehrke, S.A.; Marin, G.W. Biomechanical evaluation of dental implants with three different designs: Removal torque and resonance frequency analysis in rabbits. Ann. Anat. 2014, 199, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Degidi, M.; Perrotti, V.; Piattelli, A.; Iezzi, G. Mineralized bone-implant contact and implant stability quotient in 16 human implants retrieved after early healing periods: A histologic and histomorphometric evaluation. Int. J. Oral Maxillofac. Implants 2010, 25, 45–48. [Google Scholar] [PubMed]
- Cordioli, G.; Majzoub, Z.; Piattelli, A.; Scarano, A. Removal torque and histomorphometric investigation of 4 different titanium surfaces: An experimental study in the rabbit tibia. Int. J. Oral Maxillofac. Implants 2000, 15, 668–674. [Google Scholar] [PubMed]
- Rismanchian, M.; Movahedian, B.; Khalighinejad, N.; Badrian, H.; Mohammad Razavi, S.; Nekouie, A. Comparative evaluation of two types of immediately loaded implants using biomechanical and histomorphometric tests: An animal case study. ISRN Dent. 2012, 2012. [Google Scholar] [CrossRef] [PubMed]
- Al-Sukhun, J.; Helenius, M.; Lindqvist, C.; Kelleway, J. Biomechanics of the mandible. Part 1: Measurement of mandibular functional deformation using custom-fabricated displacement transducers. J. Oral Maxillofac. Surg. 2006, 64, 1015–1022. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Latif, H.; Hobkirk, J.; Kelleway, J. Functional mandibular deformation in edentulous subjects treated with dental implants. Int. J. Prosthodont. 2000, 13, 513–519. [Google Scholar] [PubMed]
- Law, C.; Bennani, V.; Lyons, K.; Swain, M. Mandibular flexure and its significance on implant fixed prostheses: A review. J. Prosthodont. 2012, 21, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, Y.; Koretake, K.; Hirata, M.; Kubo, T.; Akagawa, Y. Influence of static overload on the bony interface around implants in dogs. Int. J. Prosthodont. 2008, 21, 437–444. [Google Scholar] [PubMed]
© 2015 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koretake, K.; Oue, H.; Okada, S.; Takeda, Y.; Doi, K.; Akagawa, Y.; Tsuga, K. The Effect of Superstructures Connected to Implants with Different Surface Properties on the Surrounding Bone. J. Funct. Biomater. 2015, 6, 623-633. https://doi.org/10.3390/jfb6030623
Koretake K, Oue H, Okada S, Takeda Y, Doi K, Akagawa Y, Tsuga K. The Effect of Superstructures Connected to Implants with Different Surface Properties on the Surrounding Bone. Journal of Functional Biomaterials. 2015; 6(3):623-633. https://doi.org/10.3390/jfb6030623
Chicago/Turabian StyleKoretake, Katsunori, Hiroshi Oue, Shinsuke Okada, Yosuke Takeda, Kazuya Doi, Yasumasa Akagawa, and Kazuhiro Tsuga. 2015. "The Effect of Superstructures Connected to Implants with Different Surface Properties on the Surrounding Bone" Journal of Functional Biomaterials 6, no. 3: 623-633. https://doi.org/10.3390/jfb6030623
APA StyleKoretake, K., Oue, H., Okada, S., Takeda, Y., Doi, K., Akagawa, Y., & Tsuga, K. (2015). The Effect of Superstructures Connected to Implants with Different Surface Properties on the Surrounding Bone. Journal of Functional Biomaterials, 6(3), 623-633. https://doi.org/10.3390/jfb6030623