First Results of a New Vacuum Plasma Sprayed (VPS) Titanium-Coated Carbon/PEEK Composite Cage for Lumbar Interbody Fusion

 ,
,
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Inclusion/Exclusion Criteria
4.2. Implant
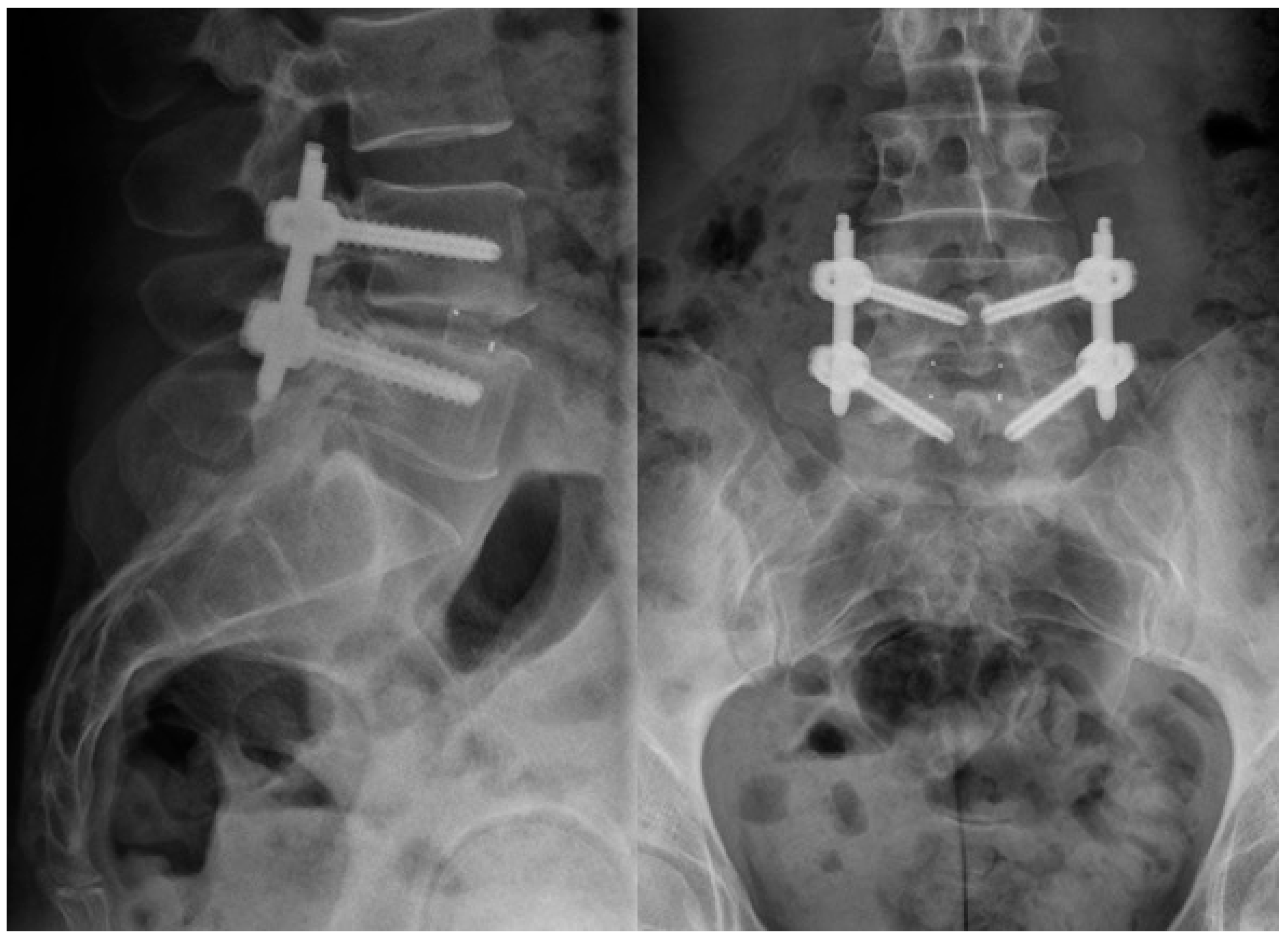
4.3. Surgical Technique
4.4. Clinical Evaluation
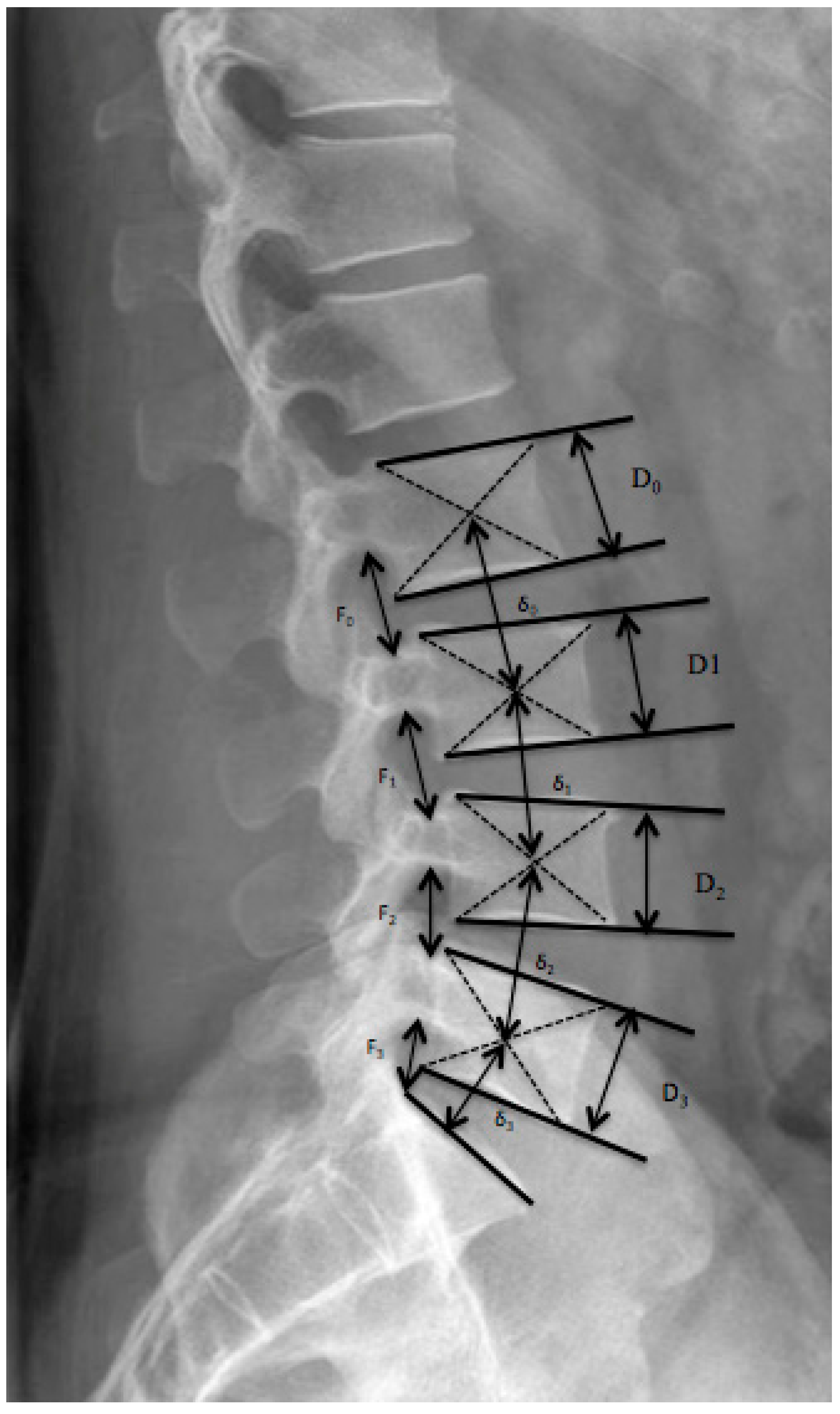
4.5. Radiological Evaluation
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Gödde, S.; Fritsch, E.; Dienst, M.; Kohn, D. Influence of cage geometry on sagittal alignment in instrumented posterior lumbar interbody fusion. Spine 2003, 28, 1693–1699. [Google Scholar] [CrossRef] [PubMed]
- Ramakrishna, S.M.J.; Wintermantel, E.; Leong, K.W. Biomedical applications of polymer-composite materials: A review. Compos. Sci. Technol. 2001, 61, 1189–1224. [Google Scholar] [CrossRef]
- Cuppone, M.; Seedhom, B.B.; Berry, E.; Ostell, A.E. The longitudinal Young’s modulus of cortical bone in the midshaft of human femur and its correlation with CT scanning data. Calcif. Tissue Int. 2004, 74, 302–309. [Google Scholar] [PubMed]
- Odgaard, A.; Linde, F. The underestimation of Young’s modulus in compressive testing of cancellous bone specimens. J. Biomech. 1991, 24, 691–698. [Google Scholar] [CrossRef]
- Han, C.M.; Lee, E.J.; Kim, H.E.; Koh, Y.H.; Kim, K.N.; Ha, Y.; Kuh, S.U. The electron beam deposition of titanium on polyetheretherketone (PEEK) and the resulting enhanced biological properties. Biomaterials 2010, 31, 3465–3470. [Google Scholar] [CrossRef] [PubMed]
- Devine, D.M.; Hahn, J.; Richards, R.G.; Gruner, H.; Wieling, R.; Pearce, S.G. Coating of carbon fiber-reinforced polyetheretherketone implants with titanium to improve bone apposition. J. Biomed. Mater. Res. B Appl. Biomater. 2013, 101, 591–598. [Google Scholar] [CrossRef] [PubMed]
- Takemoto, M.; Fujibayashi, S.; Neo, M.; So, K.; Akiyama, N.; Matsushita, T.; Kokubo, T.; Nakamura, T. A porous bioactive titanium implant for spinal interbody fusion: An experimental study using a canine model. J. Neurosurg. Spine 2007, 7, 435–443. [Google Scholar] [CrossRef] [PubMed]
- Ponsonnet, L.; Reybier, K.; Jaffrezic, N.; Comte, V.; Lagneau, C.; Lissac, M.; Martelet, C. Relationship between surface properties (roughness, wettability) of titanium and titanium alloys and cell behaviour. Mater. Sci. Eng. C 2003, 23, 551–560. [Google Scholar] [CrossRef]
- Schwartz, Z.; Raz, P.; Zhao, G.; Barak, Y.; Tauber, M.; Yao, H.; Boyan, B.D. Effect of micrometer-scale roughness of the surface of Ti6Al4V pedicle screws in vitro and in vivo. J. Bone Jt. Surg. Am. 2008, 90, 2485–2498. [Google Scholar] [CrossRef] [PubMed]
- Upasani, V.V.; Farnsworth, C.L.; Tomlinson, T.; Chambers, R.C.; Tsutsui, S.; Slivka, M.A.; Mahar, A.T.; Newton, P.O. Pedicle screw surface coatings improve fixation in nonfusion spinal constructs. Spine 2009, 34, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.F.; Yang, H.L.; Wang, J.W.; Tang, T.S. Two-year follow-up results after treatment of lumbar instability with titanium-coated fusion system. Orthop. Surg. 2009, 1, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Kokubo, T.; Kim, H.M.; Kawashita, M. Novel bioactive materials with different mechanical properties. Biomaterials 2003, 24, 2161–2175. [Google Scholar] [CrossRef]
- Ma, R.; Tang, T. Current strategies to improve the bioactivity of PEEK. Int. J. Mol. Sci. 2014, 15, 5426–5445. [Google Scholar] [CrossRef] [PubMed]
- Borsari, V.; Giavaresi, G.; Fini, M.; Torricelli, P.; Tschon, M.; Chiesa, R.; Chiusoli, L.; Salito, A.; Volpert, A.; Giardino, R. Comparative in vitro study on a ultra-high roughness and dense titanium coating. Biomaterials 2005, 26, 4948–4955. [Google Scholar] [CrossRef] [PubMed]
- Hayes, J.S.; Seidenglanz, U.; Pearce, A.I.; Pearce, S.G.; Archer, C.W.; Richards, R.G. Surface polishing positively influences ease of plate and screw removal. Eur. Cells Mater. 2010, 19, 117–126. [Google Scholar] [CrossRef]
- Aebli, N.; Krebs, J.; Stich, H.; Schawalder, P.; Walton, M.; Schwenke, D.; Gruner, H.; Gasser, B.; Theis, J.C. In vivo comparison of the osseointegration of vacuum plasma sprayed titanium- and hydroxyapatite-coated implants. J. Biomed. Mater. Res. A 2003, 66, 356–363. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.H.; Yue, W.M.; Yeo, W.; Soeharno, H.; Tan, S.B. Clinical and radiological outcomes of open versus minimally invasive transforaminal lumbar interbody fusion. Eur. Spine J. 2012, 21, 2265–2270. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhou, Y.; Zhang, Z.F.; Li, C.Q.; Zheng, W.J.; Liu, J. Comparison of one-level minimally invasive and open transforaminal lumbar interbody fusion in degenerative and isthmic spondylolisthesis grades 1 and 2. Eur. Spine J. 2010, 19, 1780–1784. [Google Scholar] [CrossRef] [PubMed]
- Wu, R.H.; Fraser, J.F.; Härtl, R. Minimal access versus open transforaminal lumbar interbody fusion: Meta-analysis of fusion rates. Spine 2010, 35, 2273–2281. [Google Scholar] [CrossRef] [PubMed]
- Galimberti, F.; Lubelski, D.; Healy, A.T.; Wang, T.; Abdullah, K.G.; Nowacki, A.S.; Benzel, E.C.; Mroz, T.E. A Systematic Review of Lumbar Fusion Rates with and Without the Use of rhBMP-2. Spine 2015, 40, 1132–1139. [Google Scholar] [CrossRef] [PubMed]
- Villavicencio, A.T.; Burneikiene, S.; Nelson, E.L.; Bulsara, K.R.; Favors, M.; Thramann, J. Safety of transforaminal lumbar interbody fusion and intervertebral recombinanthuman bone morphogenetic protein-2. J. Neurosurg. Spine 2005, 3, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Mummaneni, P.V.; Pan, J.; Haid, R.W.; Rodts, G.E. Contribution of recombinant human bone morphogenetic protein-2 to the rapid creation of interbody fusion when used in transforaminal lumbar interbody fusion: A preliminary report. Invited submission from the Joint Section Meeting on Disorders of the Spine and Peripheral Nerves, March 2004. J. Neurosurg. Spine 2004, 1, 19–23. [Google Scholar] [PubMed]
- Singh, K.; Nandyala, S.V.; Marquez-Lara, A.; Cha, T.D.; Khan, S.N.; Fineberg, S.J.; Pelton, M.A. Clinical sequelae after rhBMP-2 use in a minimally invasive transforaminal lumbar interbody fusion. Spine J. 2013, 13, 1118–1125. [Google Scholar] [CrossRef] [PubMed]
- Vaidya, R.; Sethi, A.; Bartol, S.; Jacobson, M.; Coe, C.; Craig, J.G. Complications in the use of rhBMP-2 in PEEK cages for interbody spinal fusions. J. Spinal Disord. Tech. 2008, 21, 557–562. [Google Scholar] [CrossRef] [PubMed]
- Hayes, J.S.; Richards, R.G. Surfaces to control tissue adhesion for osteosynthesis with metal implants: In vitro and in vivo studies to bring solutions to the patient. Expert Rev. Med. Devices 2010, 7, 131–142. [Google Scholar] [CrossRef] [PubMed]
- Goh, J.C.H.; Wong, H.K.; Thambyah, A.; Yu, C.S. Influence of PLIF cage size on lumbar spine stability. Spine 2000, 25, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Rao, P.J.; Pelletier, M.H.; Walsh, W.R.; Mobbs, R.J. Spine interbody implants: Material selection and modification, functionalization and bioactivation of surfaces to improve osseointegration. Orthop. Surg. 2014, 6, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Ha, S.W.; Gisep, A.; Mayer, J.; Wintermantel, E.; Gruner, H.; Wieland, M. Topographical characterization and microstructural interface analysis of vacuum-plasma-sprayed titanium and hydroxyapatite coatings on carbon fibre-reinforced poly(etheretherketone). J. Mater. Sci. Mater. Med. 1997, 8, 891–896. [Google Scholar] [CrossRef] [PubMed]
- Bridwell, K.H.; Lenke, L.G.; McEnery, K.W.; Baldus, C.; Blanke, K. Anterior structural allografts in the thoracic and lumbar spine. Spine 1995, 20, 1410–1418. [Google Scholar] [CrossRef] [PubMed]
- Benneker, L.M.; Heini, P.F.; Anderson, S.E.; Alini, M.; Ito, K. Correlation of radiographic and MRI parameters to morphological and biochemical assessment of intervertebral disc degeneration. Eur. Spine J. 2005, 14, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Frobin, W.; Brinckmann, P.; Biggemann, M. Objective measurement of the height of lumbar intervertebral discs from lateral roentgen views of the spine. Z. Orthop. Ihre Grenzgeb. 1997, 135, 394–402. [Google Scholar] [CrossRef] [PubMed]
- Kroppenstedt, S.; Gulde, M.; Schönmayr, R. Radiological comparison of instrumented posterior lumbar interbody fusion with one or two closed-box plasmapore coated titanium cages: Follow-up study over more than seven years. Spine 2008, 33, 2083–2088. [Google Scholar] [CrossRef] [PubMed]
- Mochida, J.; Nishimura, K.; Nomura, T.; Toh, E.; Chiba, M. The importance of preserving disc structure in surgical approaches to lumbar disc herniation. Spine 1996, 21, 1556–1563. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Pre-OP | Six Months Post-OP | Latest FU | |
|---|---|---|---|
| Lordosis | |||
| Segmental lordosis (range) | 9° (0–14°) | 12° (7–16°) * | 10° (2–15°) |
| Caudal adjacent lordosis | 10° (8–15°) | 10° (7–15°) | 10° (7–15°) |
| Cranial adjacent lordosis | 11° (7–14°) | 11°(7–14°) | 11° (7–15°) |
| Lumbar lordosis L1–S1 | 52° (41–63°) | 53° (41–63°) | 53° (41–63°) |
| Degeneration at adjacent segments (n = 74) | |||
| G0 (n) | 15 | 14 | 13 |
| G1 (n) | 38 | 39 | 36 |
| G2 (n) | 15 | 15 | 14 |
| G3 (n) | 4 | 4 | 11 * |
| Patient | Age (Years) | Operation Level | Post-Operative Interval (Days) | Complications | Treatment | Results |
|---|---|---|---|---|---|---|
| 1 | 55 | L4–5 | 5 | Seroma | Clinical Observation | Resolved without intervention |
| 2 | 29 | L5–S1 | 4 | Hyposensibility | Steroid | 2 months later resolved |
| 3 | 65 | L3–4 | 11 | Hematoma | Clinical Observation | Resolved without intervention |
| 4 | 54 | L3–4 | 3 | Deep infection | 5 times debridement + antibitherapy | Fully recovered |
| 5 | 69 | L4–5 | 5 | L5 right partial motor deficit | Steroid | Resolved without intervention |
| 6. | 67 | L4–5 | 4 | L5 right partial motor deficit | Steroid | Resolved without intervention |
| 7 | 78 | L5–S1 | 8 | Wound disorder | Clinical Observation | Resolved without intervention |
| 8 | 63 | L3–4 | 4 | L5 right paraesthisia | Steroid | Resolved without intervention |
| 9 | 41 | L5–S1 | 9 | L4–5 partial motor deficit + paraesthisia | Steroid | Persisting L4–5 hyposensibility + decreased force (M4) |
| 10 | 63 | L3–4 | 9 | Lung embolia | Medical treatment | Fully recovered |
| 11 | 28 | L4–S1 | 4 | L5 right paraesthisia | Steroid | Paraesthisia |
| 12 | 62 | L3–4 | 8 | L2–3 partial motor deficit + L5 paraesthisia | Steroid | L2–3 M4 |
| Parameter | Value |
|---|---|
| Number of patients (levels) | 42 (47) |
| Patients lost to follow-up (%) | 27 |
| Multiple level fusion (%) | 5 (12) |
| Mean age (range) | 59.6 (28–82) |
| Male (%) | 23 (55) |
| Mean BMI (± SD, range; kg) | 28.3 ± 5 (19–40) |
| Mean time of follow-up (± SD, range; months) | 29.1 ± 9 (24–39) |
| Diagnosis | |
| Spinal stenosis (%) | 26 (62) |
| Degenerative spondylolisthesis (%) | 11 (26) |
| - Meyerding I (%) | 7 (63) |
| - Meyerding II (%) | 4 (37) |
| - Meyerding III (%) | - |
| - Meyerding IV (%) | - |
| Isthmic spondylolisthesis (%) | 2 (5) |
| Recurrent degenerative disc disease (%) | 3 (7) |
| Level with fusion | |
| L2–3 (%) | 9 |
| L3–4 (%) | 17 |
| L4–5 (%) | 23 |
| L5–S1 (%) | 51 |
| I | Fused with remodeling and trabeculae present |
| II | Graft intact, not fully remodeled and incorporated, but no lucency present |
| III | Graft intact, potential lucency present at top and bottom of graft |
| IV | Fusion absent with collapse/resorption of graft |
| Grade | Height Loss | Osteophytes | Schmorl’s Nodes | Intradiscal Calcification | Sclerosis | Endplate Shape |
|---|---|---|---|---|---|---|
| 0 | 0–10% | Margins rounded | Not present | No calcifications | None | Continuous |
| 1 | 10–20% | Margins pointed | Present | Rim calcification | Moderate | Irregular |
| 2 | 20–30% | <2 mm | - | Intranuclear calcification | Severe | Disrupted |
| 3 | >30% | >2 mm | - | - | - | - |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hoppe, S.; Albers, C.E.; Elfiky, T.; Deml, M.C.; Milavec, H.; Bigdon, S.F.; Benneker, L.M. First Results of a New Vacuum Plasma Sprayed (VPS) Titanium-Coated Carbon/PEEK Composite Cage for Lumbar Interbody Fusion. J. Funct. Biomater. 2018, 9, 23. https://doi.org/10.3390/jfb9010023
Hoppe S, Albers CE, Elfiky T, Deml MC, Milavec H, Bigdon SF, Benneker LM. First Results of a New Vacuum Plasma Sprayed (VPS) Titanium-Coated Carbon/PEEK Composite Cage for Lumbar Interbody Fusion. Journal of Functional Biomaterials. 2018; 9(1):23. https://doi.org/10.3390/jfb9010023
Chicago/Turabian StyleHoppe, Sven, Christoph E. Albers, Tarek Elfiky, Moritz C. Deml, Helena Milavec, Sebastian F. Bigdon, and Lorin M. Benneker. 2018. "First Results of a New Vacuum Plasma Sprayed (VPS) Titanium-Coated Carbon/PEEK Composite Cage for Lumbar Interbody Fusion" Journal of Functional Biomaterials 9, no. 1: 23. https://doi.org/10.3390/jfb9010023
APA StyleHoppe, S., Albers, C. E., Elfiky, T., Deml, M. C., Milavec, H., Bigdon, S. F., & Benneker, L. M. (2018). First Results of a New Vacuum Plasma Sprayed (VPS) Titanium-Coated Carbon/PEEK Composite Cage for Lumbar Interbody Fusion. Journal of Functional Biomaterials, 9(1), 23. https://doi.org/10.3390/jfb9010023