An Intelligent ECG-Based Tool for Diagnosing COVID-19 via Ensemble Deep Learning Techniques


Abstract
:1. Introduction
Related Studies
2. Materials and Methods
2.1. ECG Dataset
2.2. Proposed Tool
2.2.1. ECG Image Preprocessing
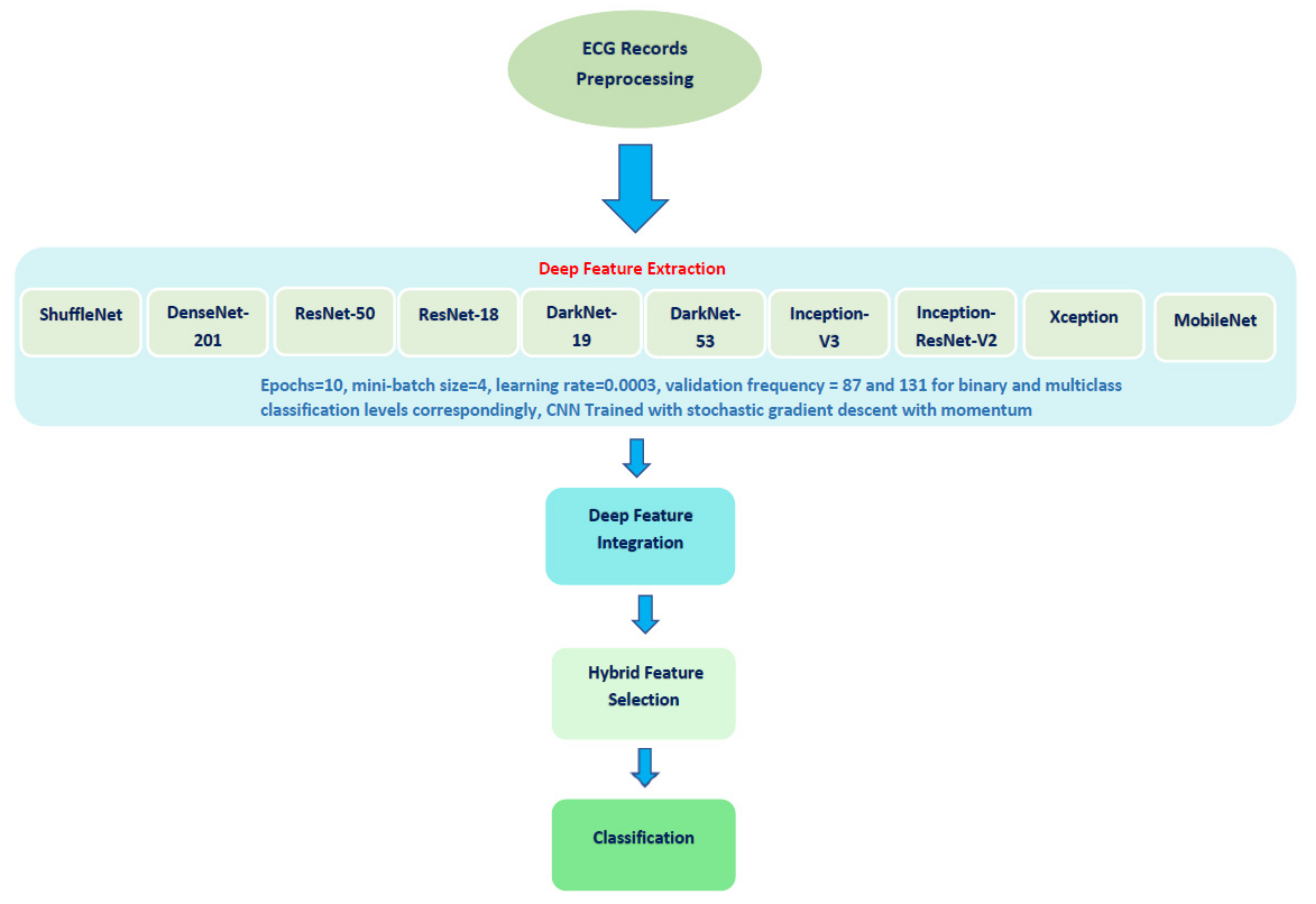
2.2.2. Deep Features Extraction and Feature Incorporation
2.2.3. Hybrid Feature Selection
2.2.4. Classification
2.3. Performance Evaluation
3. Results
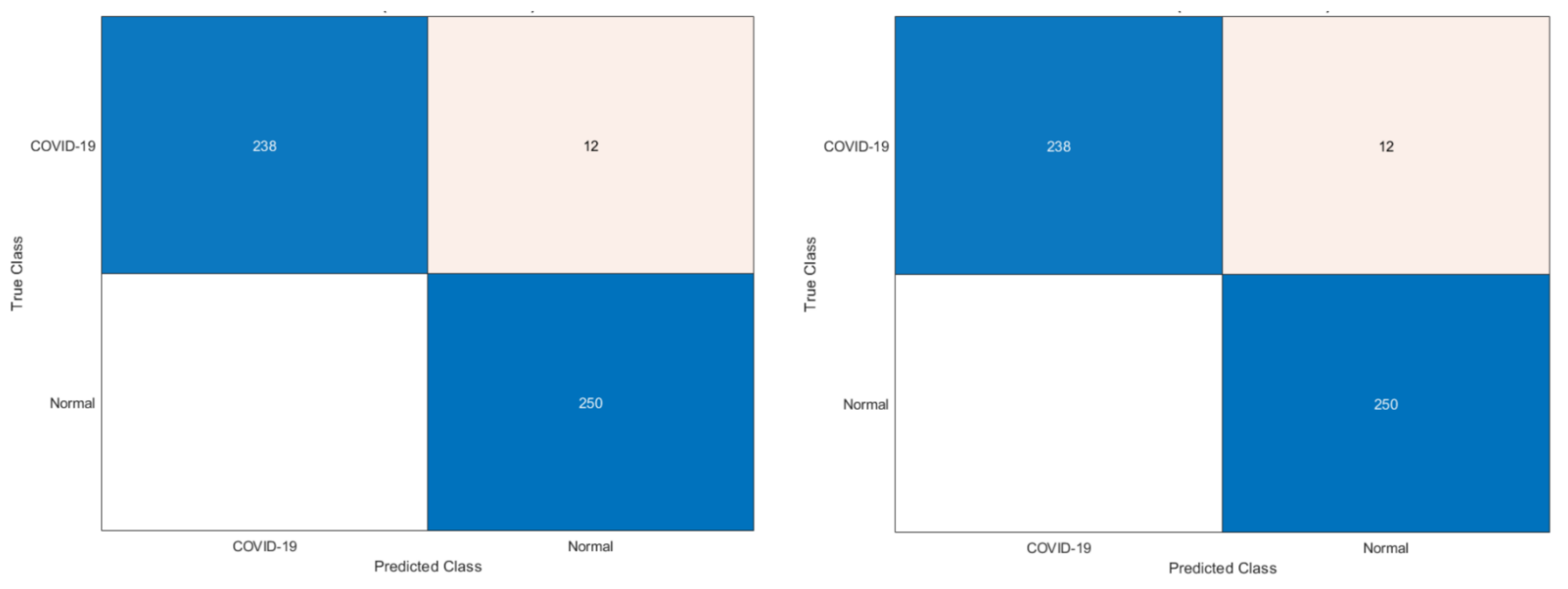
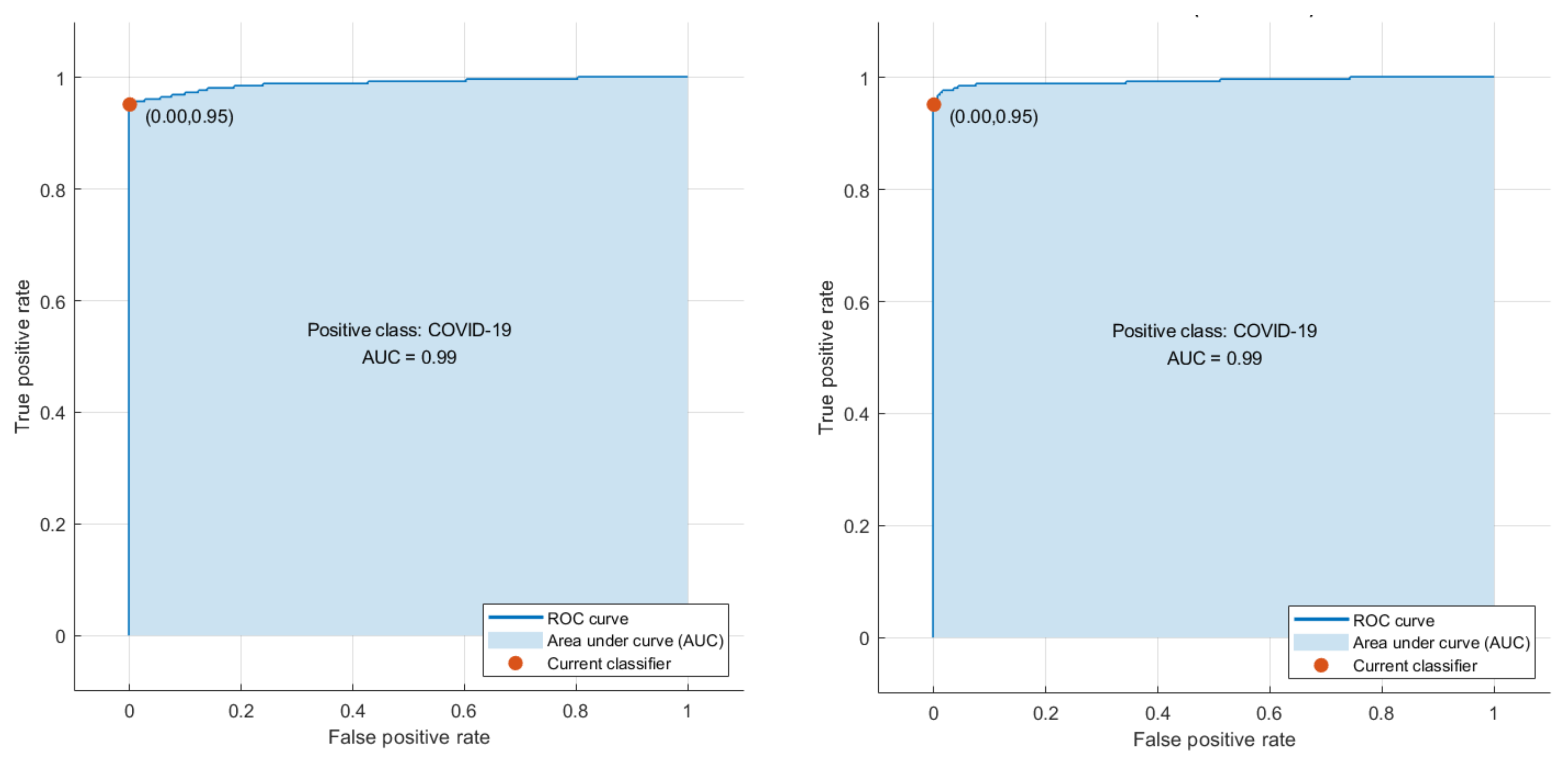
3.1. Phase I Classification Results
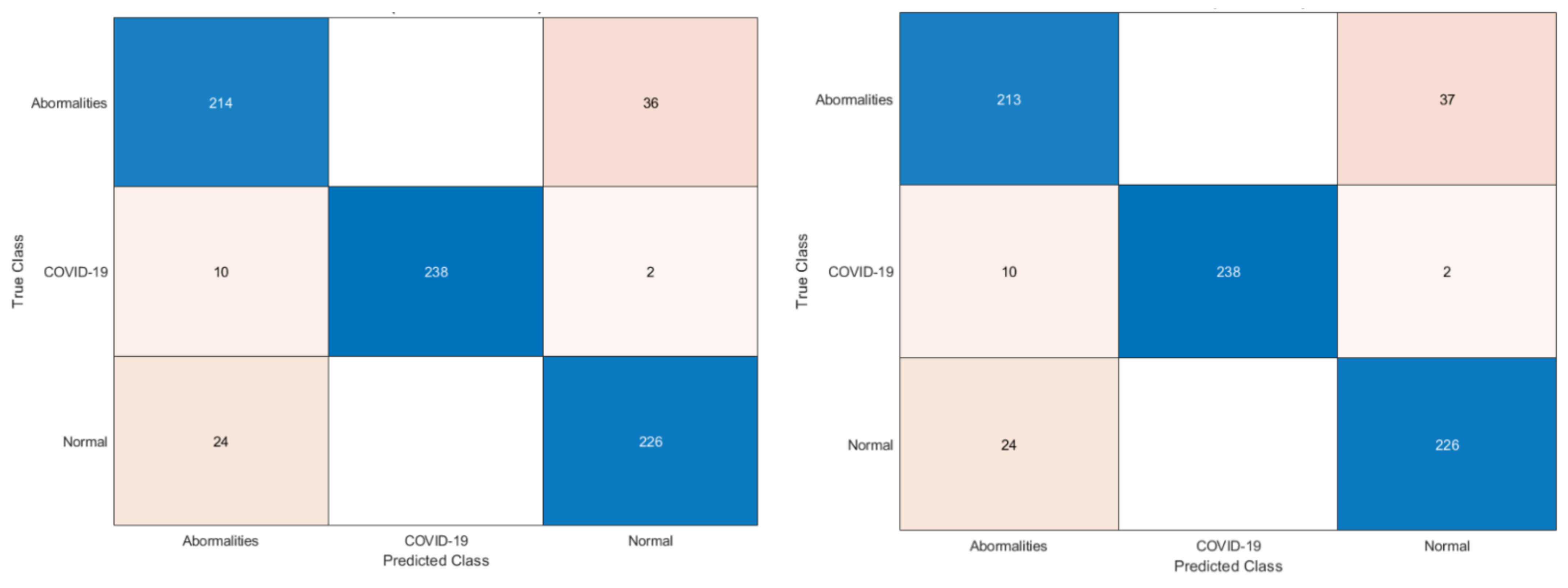
3.2. Phase II Classification Results
4. Discussion
4.1. Comparison with Related Studies
4.2. Limitations
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AI | Artificial intelligence |
| ANOVA | Analysis of variance |
| ANN | Artificial neural networks |
| AVF | Augmented voltage foot |
| AVL | Augmented voltage left |
| AVR | Augmented voltage right |
| CNN | Convolutional Neural Network |
| CT | Computed Temography |
| DL | Deep learning |
| DT | Decision Tree |
| DWT | Discrete wavelet transform |
| ECG | Electrocardiogram |
| FN | False negative |
| FP | False positive |
| FS | Feature Selection |
| GLCM | Gray-Level Co-Occurrence Matrix |
| KNN | K-nearest neighbor |
| LDA | Linear discriminate analysis |
| MI | Myocardial infarction |
| ML | Machine learning |
| QDA | Quadratic discriminate analysis |
| RF | Random Forest |
| RT-PCR | Real-time reverse transcription-polymerase chain reaction |
| SVM | Support vector machine |
| TL | Transfer learning |
| TN | True negative |
| TR | True positive |
| TML | Traditional machine learning techniques |
| WHO | World Health Organization |
Appendix A
References
- Pascarella, G.; Strumia, A.; Piliego, C.; Bruno, F.; Del Buono, R.; Costa, F.; Scarlata, S.; Agrò, F.E. COVID-19 Diagnosis and Management: A Comprehensive Review. J. Intern. Med. 2020, 288, 192–206. [Google Scholar] [CrossRef] [PubMed]
- Attallah, O. A Computer-Aided Diagnostic Framework for Coronavirus Diagnosis Using Texture-Based Radiomics Images. Digital Health 2022, 8, 20552076221092544. [Google Scholar] [CrossRef] [PubMed]
- Alballa, N.; Al-Turaiki, I. Machine Learning Approaches in COVID-19 Diagnosis, Mortality, and Severity Risk Prediction: A Review. Inform. Med. Unlocked 2021, 24, 100564. [Google Scholar] [CrossRef] [PubMed]
- Alsharif, W.; Qurashi, A. Effectiveness of COVID-19 Diagnosis and Management Tools: A Review. Radiography 2021, 27, 682–687. [Google Scholar] [CrossRef] [PubMed]
- Alanagreh, L.; Alzoughool, F.; Atoum, M. The Human Coronavirus Disease COVID-19: Its Origin, Characteristics, and Insights into Potential Drugs and Its Mechanisms. Pathogens 2020, 9, 331. [Google Scholar] [CrossRef] [PubMed]
- Kyosei, Y.; Yamura, S.; Namba, M.; Yoshimura, T.; Watabe, S.; Ito, E. Antigen Tests for COVID-19. Biophys. Phys. 2021, 18, 28–39. [Google Scholar] [CrossRef]
- Scohy, A.; Anantharajah, A.; Bodéus, M.; Kabamba-Mukadi, B.; Verroken, A.; Rodriguez-Villalobos, H. Low Performance of Rapid Antigen Detection Test as Frontline Testing for COVID-19 Diagnosis. J. Clin. Virol. 2020, 129, 104455. [Google Scholar] [CrossRef]
- Raptis, C.A.; Hammer, M.M.; Short, R.G.; Shah, A.; Bhalla, S.; Bierhals, A.J.; Filev, P.D.; Hope, M.D.; Jeudy, J.; Kligerman, S.J. Chest CT and Coronavirus Disease (COVID-19): A Critical Review of the Literature to Date. Am. J. Roentgenol. 2020, 215, 839–842. [Google Scholar] [CrossRef]
- Rousan, L.A.; Elobeid, E.; Karrar, M.; Khader, Y. Chest X-Ray Findings and Temporal Lung Changes in Patients with COVID-19 Pneumonia. BMC Pulm. Med. 2020, 20, 245. [Google Scholar] [CrossRef]
- Xie, X.; Zhong, Z.; Zhao, W.; Zheng, C.; Wang, F.; Liu, J. Chest CT for Typical 2019-NCoV Pneumonia: Relationship to Negative RT-PCR Testing. Radiology 2020, 296, E41–E45. [Google Scholar] [CrossRef] [Green Version]
- Attallah, O.; Anwar, F.; Ghanem, N.M.; Ismail, M.A. Histo-CADx: Duo Cascaded Fusion Stages for Breast Cancer Diagnosis from Histopathological Images. PeerJ Comput. Sci. 2021, 7, e493. [Google Scholar] [CrossRef] [PubMed]
- Attallah, O. DIAROP: Automated Deep Learning-Based Diagnostic Tool for Retinopathy of Prematurity. Diagnostics 2021, 11, 2034. [Google Scholar] [CrossRef] [PubMed]
- Attallah, O.; Sharkas, M. GASTRO-CADx: A Three Stages Framework for Diagnosing Gastrointestinal Diseases. PeerJ Comput. Sci. 2021, 7, e423. [Google Scholar] [CrossRef]
- Karthikesalingam, A.; Attallah, O.; Ma, X.; Bahia, S.S.; Thompson, L.; Vidal-Diez, A.; Choke, E.C.; Bown, M.J.; Sayers, R.D.; Thompson, M.M. An Artificial Neural Network Stratifies the Risks of Reintervention and Mortality after Endovascular Aneurysm Repair; a Retrospective Observational Study. PLoS ONE 2015, 10, e0129024. [Google Scholar] [CrossRef]
- Attallah, O. An Effective Mental Stress State Detection and Evaluation System Using Minimum Number of Frontal Brain Electrodes. Diagnostics 2020, 10, 292. [Google Scholar] [CrossRef] [PubMed]
- Attallah, O.; Karthikesalingam, A.; Holt, P.J.; Thompson, M.M.; Sayers, R.; Bown, M.J.; Choke, E.C.; Ma, X. Using Multiple Classifiers for Predicting the Risk of Endovascular Aortic Aneurysm Repair Re-Intervention through Hybrid Feature Selection. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2017, 231, 1048–1063. [Google Scholar] [CrossRef] [PubMed]
- Ragab, D.A.; Sharkas, M.; Attallah, O. Breast Cancer Diagnosis Using an Efficient CAD System Based on Multiple Classifiers. Diagnostics 2019, 9, 165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Attallah, O. MB-AI-His: Histopathological Diagnosis of Pediatric Medulloblastoma and Its Subtypes via AI. Diagnostics 2021, 11, 359–384. [Google Scholar] [CrossRef]
- Attallah, O. CoMB-Deep: Composite Deep Learning-Based Pipeline for Classifying Childhood Medulloblastoma and Its Classes. Front. Neuroinform. 2021, 15, 663592. [Google Scholar] [CrossRef]
- Attallah, O.; Zaghlool, S. AI-Based Pipeline for Classifying Pediatric Medulloblastoma Using Histopathological and Textural Images. Life 2022, 12, 232. [Google Scholar] [CrossRef]
- Alyasseri, Z.A.A.; Al-Betar, M.A.; Doush, I.A.; Awadallah, M.A.; Abasi, A.K.; Makhadmeh, S.N.; Alomari, O.A.; Abdulkareem, K.H.; Adam, A.; Damasevicius, R. Review on COVID-19 Diagnosis Models Based on Machine Learning and Deep Learning Approaches. Expert syst. 2021, 39, e12759. [Google Scholar] [CrossRef] [PubMed]
- Attallah, O.; Ragab, D.A.; Sharkas, M. MULTI-DEEP: A Novel CAD System for Coronavirus (COVID-19) Diagnosis from CT Images Using Multiple Convolution Neural Networks. PeerJ 2020, 8, e10086. [Google Scholar] [CrossRef] [PubMed]
- Ragab, D.A.; Attallah, O. FUSI-CAD: Coronavirus (COVID-19) Diagnosis Based on the Fusion of CNNs and Handcrafted Features. PeerJ Comput. Sci. 2020, 6, e306. [Google Scholar] [CrossRef] [PubMed]
- Pawlak, A.; Ręka, G.; Olszewska, A.; Warchulińska, J.; Piecewicz-Szczęsna, H. Methods of Assessing Body Composition and Anthropometric Measurements–a Review of the Literature. J. Educ. Health Sport 2021, 11, 18–27. [Google Scholar] [CrossRef]
- Khawaja, S.A.; Mohan, P.; Jabbour, R.; Bampouri, T.; Bowsher, G.; Hassan, A.M.; Huq, F.; Baghdasaryan, L.; Wang, B.; Sethi, A. COVID-19 and Its Impact on the Cardiovascular System. Open Heart 2021, 8, e001472. [Google Scholar] [CrossRef] [PubMed]
- Buja, L.M.; Stone, J.R. A Novel Coronavirus Meets the Cardiovascular System: Society for Cardiovascular Pathology Symposium 2021. Cardiovasc. Pathol. 2021, 53, 107336. [Google Scholar] [CrossRef]
- Barman, H.A.; Atici, A.; Alici, G.; Sit, O.; Tugrul, S.; Gungor, B.; Okuyan, E.; Sahin, I. The Effect of the Severity COVID-19 Infection on Electrocardiography. Am. J. Emerg. Med. 2021, 46, 317–322. [Google Scholar] [CrossRef]
- Babapoor-Farrokhran, S.; Rasekhi, R.T.; Gill, D.; Babapoor, S.; Amanullah, A. Arrhythmia in COVID-19. SN Compr. Clin. Med. 2020, 2, 1430–1435. [Google Scholar] [CrossRef]
- Predabon, B.; Souza, A.Z.M.; Bertoldi, G.H.S.; Sales, R.L.; Luciano, K.S.; de March Ronsoni, R. The Electrocardiogram in the Differential Diagnosis of Cardiologic Conditions Related to the Covid-19 Pandemic. J. Card. Arrhythm. 2020, 33, 133–141. [Google Scholar] [CrossRef]
- Andrysiak, T. Machine Learning Techniques Applied to Data Analysis and Anomaly Detection in ECG Signals. Appl. Artif. Intell. 2016, 30, 610–634. [Google Scholar] [CrossRef]
- Tuncer, T.; Dogan, S.; Pławiak, P.; Acharya, U.R. Automated Arrhythmia Detection Using Novel Hexadecimal Local Pattern and Multilevel Wavelet Transform with ECG Signals. Knowl.-Based Syst. 2019, 186, 104923. [Google Scholar] [CrossRef]
- Hernandez-Matamoros, A.; Fujita, H.; Escamilla-Hernandez, E.; Perez-Meana, H.; Nakano-Miyatake, M. Recognition of ECG Signals Using Wavelet Based on Atomic Functions. Biocybern. Biomed. Eng. 2020, 40, 803–814. [Google Scholar] [CrossRef]
- Pandey, S.K.; Janghel, R.R.; Vani, V. Patient Specific Machine Learning Models for ECG Signal Classification. Procedia Comput. Sci. 2020, 167, 2181–2190. [Google Scholar] [CrossRef]
- Rouhi, R.; Clausel, M.; Oster, J.; Lauer, F. An Interpretable Hand-Crafted Feature-Based Model for Atrial Fibrillation Detection. Front. Physiol. 2021, 12, 581. [Google Scholar] [CrossRef] [PubMed]
- Nanni, L.; Ghidoni, S.; Brahnam, S. Handcrafted vs. Non-Handcrafted Features for Computer Vision Classification. Pattern Recognit. 2017, 71, 158–172. [Google Scholar] [CrossRef]
- Huang, J.; Chen, B.; Yao, B.; He, W. ECG Arrhythmia Classification Using STFT-Based Spectrogram and Convolutional Neural Network. IEEE Access 2019, 7, 92871–92880. [Google Scholar] [CrossRef]
- Zhai, X.; Tin, C. Automated ECG Classification Using Dual Heartbeat Coupling Based on Convolutional Neural Network. IEEE Access 2018, 6, 27465–27472. [Google Scholar] [CrossRef]
- Kiranyaz, S.; Ince, T.; Gabbouj, M. Real-Time Patient-Specific ECG Classification by 1-D Convolutional Neural Networks. IEEE Trans. Biomed. Eng. 2015, 63, 664–675. [Google Scholar] [CrossRef]
- Attallah, O.; Sharkas, M.A.; Gadelkarim, H. Deep Learning Techniques for Automatic Detection of Embryonic Neurodevelopmental Disorders. Diagnostics 2020, 10, 27. [Google Scholar] [CrossRef] [Green Version]
- Izci, E.; Ozdemir, M.A.; Degirmenci, M.; Akan, A. Cardiac Arrhythmia Detection from 2d Ecg Images by Using Deep Learning Technique. In Proceedings of the 2019 Medical Technologies Congress (TIPTEKNO), Izmir, Turkey, 3–5 October 2019; pp. 1–4. [Google Scholar]
- Huang, J.-S.; Chen, B.-Q.; Zeng, N.-Y.; Cao, X.-C.; Li, Y. Accurate Classification of ECG Arrhythmia Using MOWPT Enhanced Fast Compression Deep Learning Networks. J. Ambient Intell. Humaniz. Comput. 2020, 1–18. [Google Scholar] [CrossRef]
- Singh, S.A.; Majumder, S. A Novel Approach Osa Detection Using Single-Lead ECG Scalogram Based on Deep Neural Network. J. Mech. Med. Biol. 2019, 19, 1950026. [Google Scholar] [CrossRef]
- Bortolan, G.; Christov, I.; Simova, I. Potential of Rule-Based Methods and Deep Learning Architectures for ECG Diagnostics. Diagnostics 2021, 11, 1678. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.; Lan, X.; Zhao, T.; Guo, Y.; Kojodjojo, P.; Xu, Z.; Liu, Z.; Liu, S.; Wang, H.; Sun, X. Identification of 27 Abnormalities from Multi-Lead ECG Signals: An Ensembled SE_ResNet Framework with Sign Loss Function. Physiol. Meas. 2021, 42, 065008. [Google Scholar] [CrossRef] [PubMed]
- Jo, Y.-Y.; Kwon, J.; Jeon, K.-H.; Cho, Y.-H.; Shin, J.-H.; Lee, Y.-J.; Jung, M.-S.; Ban, J.-H.; Kim, K.-H.; Lee, S.Y. Detection and Classification of Arrhythmia Using an Explainable Deep Learning Model. J. Electrocardiol. 2021, 67, 124–132. [Google Scholar] [CrossRef]
- Yang, X.; Zhang, X.; Yang, M.; Zhang, L. 12-Lead ECG Arrhythmia Classification Using Cascaded Convolutional Neural Network and Expert Feature. J. Electrocardiol. 2021, 67, 56–62. [Google Scholar] [CrossRef]
- Zhang, H.; Liu, C.; Zhang, Z.; Xing, Y.; Liu, X.; Dong, R.; He, Y.; Xia, L.; Liu, F. Recurrence Plot-Based Approach for Cardiac Arrhythmia Classification Using Inception-ResNet-V2. Front. Physiol. 2021, 12, 648950. [Google Scholar] [CrossRef]
- Krasteva, V.; Christov, I.; Naydenov, S.; Stoyanov, T.; Jekova, I. Application of Dense Neural Networks for Detection of Atrial Fibrillation and Ranking of Augmented ECG Feature Set. Sensors 2021, 21, 6848. [Google Scholar] [CrossRef]
- Dai, H.; Hwang, H.-G.; Tseng, V.S. Convolutional Neural Network Based Automatic Screening Tool for Cardiovascular Diseases Using Different Intervals of ECG Signals. Comput. Methods Programs Biomed. 2021, 203, 106035. [Google Scholar] [CrossRef]
- Alday, E.A.P.; Gu, A.; Robichaux, C.; Ian Wong, A.K.; Liu, C.; Liu, F.; Elola, A.; Seyedi, S.; Li, Q.; Sharma, A. Classification of 12-Lead ECGs: The PhysioNet/Computing in Cardiology Challenge 2020. Physiol. Meas. 2021, 41, 124003. [Google Scholar] [CrossRef]
- Reyna, M.A.; Sadr, N.; Alday, E.A.P.; Gu, A.; Shah, A.J.; Robichaux, C.; Rad, A.B.; Elola, A.; Seyedi, S.; Ansari, S. Issues in the Automated Classification of Multilead ECGs Using Heterogeneous Labels and Populations. Personnel 2021, 4, 5. [Google Scholar]
- Badilini, F.; Erdem, T.; Zareba, W.; Moss, A.J. ECGscan: A Method for Digitizing Paper ECG Printouts. J. Electrocardiol. 2003, 36, 39. [Google Scholar] [CrossRef]
- Mishra, S.; Khatwani, G.; Patil, R.; Sapariya, D.; Shah, V.; Parmar, D.; Dinesh, S.; Daphal, P.; Mehendale, N. ECG Paper Record Digitization and Diagnosis Using Deep Learning. J. Med. Biol. Eng. 2021, 41, 422–432. [Google Scholar] [CrossRef] [PubMed]
- Widman, L.E.; Freeman, G.L. A-to-D Conversion from Paper Records with a Desktop Scanner and a Microcomputer. Comput. Biomed. Res. 1989, 22, 393–404. [Google Scholar] [CrossRef]
- Hao, P.; Gao, X.; Li, Z.; Zhang, J.; Wu, F.; Bai, C. Multi-Branch Fusion Network for Myocardial Infarction Screening from 12-Lead ECG Images. Comput. Methods Programs Biomed. 2020, 184, 105286. [Google Scholar] [CrossRef]
- Mohamed, B.; Issam, A.; Mohamed, A.; Abdellatif, B. ECG Image Classification in Real Time Based on the Haar-like Features and Artificial Neural Networks. Procedia Comput. Sci. 2015, 73, 32–39. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, M.A.A.; Gurgel, M.V.; Marinho, L.B.; Nascimento, N.M.M.; da Silva, S.P.P.; Alves, S.S.A.; Ramalho, G.L.B.; Rebouças Filho, P.P. Evaluation of Heart Disease Diagnosis Approach Using ECG Images. In Proceedings of the 2019 International Joint Conference on Neural Networks (IJCNN), Budapest, Hungary, 14–19 July 2019; pp. 1–7. [Google Scholar]
- Du, N.; Cao, Q.; Yu, L.; Liu, N.; Zhong, E.; Liu, Z.; Shen, Y.; Chen, K. FM-ECG: A Fine-Grained Multi-Label Framework for ECG Image Classification. Inf. Sci. 2021, 549, 164–177. [Google Scholar] [CrossRef]
- Khan, A.H.; Hussain, M.; Malik, M.K. Cardiac Disorder Classification by Electrocardiogram Sensing Using Deep Neural Network. Complexity 2021, 2021, 5512243. [Google Scholar] [CrossRef]
- Xie, Y.; Yang, H.; Yuan, X.; He, Q.; Zhang, R.; Zhu, Q.; Chu, Z.; Yang, C.; Qin, P.; Yan, C. Stroke Prediction from Electrocardiograms by Deep Neural Network. Multimed. Tools Appl. 2021, 80, 17291–17297. [Google Scholar] [CrossRef]
- Khan, A.H.; Hussain, M.; Malik, M.K. ECG Images Dataset of Cardiac and COVID-19 Patients. Data Brief 2021, 34, 106762. [Google Scholar] [CrossRef]
- Anwar, T.; Zakir, S. Effect of Image Augmentation on ECG Image Classification Using Deep Learning. In Proceedings of the 2021 International Conference on Artificial Intelligence (ICAI), Islamabad, Pakistan, 5–7 April 2021; pp. 182–186. [Google Scholar]
- Rahman, T.; Akinbi, A.; Chowdhury, M.E.; Rashid, T.A.; Şengür, A.; Khandakar, A.; Islam, K.R.; Ismael, A.M. COV-ECGNET: COVID-19 Detection Using ECG Trace Images with Deep Convolutional Neural Network. arXiv 2021, arXiv:2106.00436. [Google Scholar] [CrossRef]
- Ozdemir, M.A.; Ozdemir, G.D.; Guren, O. Classification of COVID-19 Electrocardiograms by Using Hexaxial Feature Mapping and Deep Learning. BMC Med. Inform. Decis. Mak. 2021, 21, 170. [Google Scholar] [CrossRef] [PubMed]
- Attallah, O. ECG-BiCoNet: An ECG-Based Pipeline for COVID-19 Diagnosis Using Bi-Layers of Deep Features Integration. Comput. Biol. Med. 2022, 142, 105210. [Google Scholar] [CrossRef] [PubMed]
- Shorten, C.; Khoshgoftaar, T.M. A Survey on Image Data Augmentation for Deep Learning. J. Big Data 2019, 6, 60. [Google Scholar] [CrossRef]
- Amin, S.U.; Alsulaiman, M.; Muhammad, G.; Mekhtiche, M.A.; Hossain, M.S. Deep Learning for EEG Motor Imagery Classification Based on Multi-Layer CNNs Feature Fusion. Future Gener. Comput. Syst. 2019, 101, 542–554. [Google Scholar] [CrossRef]
- Xu, Q.; Wang, Z.; Wang, F.; Gong, Y. Multi-Feature Fusion CNNs for Drosophila Embryo of Interest Detection. Phys. A Stat. Mech. Its Appl. 2019, 531, 121808. [Google Scholar] [CrossRef]
- Ravì, D.; Wong, C.; Deligianni, F.; Berthelot, M.; Andreu-Perez, J.; Lo, B.; Yang, G.-Z. Deep Learning for Health Informatics. IEEE J. Biomed. Health Inform. 2016, 21, 4–21. [Google Scholar] [CrossRef] [Green Version]
- Szegedy, C.; Vanhoucke, V.; Ioffe, S.; Shlens, J.; Wojna, Z. Rethinking the Inception Architecture for Computer Vision. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 2818–2826. [Google Scholar]
- Szegedy, C.; Liu, W.; Jia, Y.; Sermanet, P.; Reed, S.; Anguelov, D.; Erhan, D.; Vanhoucke, V.; Rabinovich, A. Going Deeper with Convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Boston, Ma, USA, 7–12 June 2015; pp. 1–9. [Google Scholar]
- Radhika, K.; Devika, K.; Aswathi, T.; Sreevidya, P.; Sowmya, V.; Soman, K.P. Performance Analysis of NASNet on Unconstrained Ear Recognition. In Nature Inspired Computing for Data Science; Springer: Berlin/Heidelberg, Germany, 2020; pp. 57–82. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016. [Google Scholar]
- Chollet, F. Xception: Deep Learning with Depthwise Separable Convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 1251–1258. [Google Scholar]
- Jinsakul, N.; Tsai, C.-F.; Tsai, C.-E.; Wu, P. Enhancement of Deep Learning in Image Classification Performance Using Xception with the Swish Activation Function for Colorectal Polyp Preliminary Screening. Mathematics 2019, 7, 1170. [Google Scholar] [CrossRef] [Green Version]
- Szegedy, C.; Ioffe, S.; Vanhoucke, V.; Alemi, A. Inception-v4, Inception-Resnet and the Impact of Residual Connections on Learning. arXiv 2016, arXiv:1602.07261. [Google Scholar]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely Connected Convolutional Networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]
- Zhang, X.; Zhou, X.; Lin, M.; Sun, J. Shufflenet: An Extremely Efficient Convolutional Neural Network for Mobile Devices. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–23 June 2018; pp. 6848–6856. [Google Scholar]
- Redmon, J.; Farhadi, A. YOLO9000: Better, Faster, Stronger. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 7263–7271. [Google Scholar]
- Howard, A.G.; Zhu, M.; Chen, B.; Kalenichenko, D.; Wang, W.; Weyand, T.; Andreetto, M.; Adam, H. Mobilenets: Efficient Convolutional Neural Networks for Mobile Vision Applications. arXiv 2017, arXiv:1704.04861. [Google Scholar]
- Tan, C.; Sun, F.; Kong, T.; Zhang, W.; Yang, C.; Liu, C. A Survey on Deep Transfer Learning. In International Conference on Artificial Neural Networks; Springer: Berlin/Heidelberg, Germany, 2018; pp. 270–279. [Google Scholar]
- Hancer, E.; Xue, B.; Zhang, M. A Survey on Feature Selection Approaches for Clustering. Artif. Intell. Rev. 2020, 53, 4519–4545. [Google Scholar] [CrossRef]
- Chizi, B.; Rokach, L.; Maimon, O. A Survey of Feature Selection Techniques. In Encyclopedia of Data Warehousing and Mining, Second Edition; IGI Global: Hershey, PA, USA, 2009; pp. 1888–1895. [Google Scholar]
- Attallah, O.; Karthikesalingam, A.; Holt, P.J.; Thompson, M.M.; Sayers, R.; Bown, M.J.; Choke, E.C.; Ma, X. Feature Selection through Validation and Un-Censoring of Endovascular Repair Survival Data for Predicting the Risk of Re-Intervention. BMC Med. Inform. Decis. Mak. 2017, 17, 115–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bahassine, S.; Madani, A.; Al-Sarem, M.; Kissi, M. Feature Selection Using an Improved Chi-Square for Arabic Text Classification. J. King Saud Univ.-Comput. Inf. Sci. 2020, 32, 225–231. [Google Scholar] [CrossRef]
- Hall, M.; Frank, E.; Holmes, G.; Pfahringer, B.; Reutemann, P.; Witten, I.H. The WEKA Data Mining Software: An Update. ACM SIGKDD Explor. Newsl. 2009, 11, 10–18. [Google Scholar] [CrossRef]
- Haseeb, S.; Gul, E.E.; Çinier, G.; Bazoukis, G.; Alvarez-Garcia, J.; Garcia-Zamora, S.; Lee, S.; Yeung, C.; Liu, T.; Tse, G. Value of Electrocardiography in Coronavirus Disease 2019 (COVID-19). J. Electrocardiol. 2020, 62, 39–45. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Class | Number of Available Images | Images Used in the Proposed Study | Images Used in Training | Images Used in Validation |
|---|---|---|---|---|
| COVID-19 | 250 | 250 | 175 | 75 |
| Normal | 859 | 250 | 175 | 75 |
| Cardiac Abnormalities include: | 848 | 250 | 175 | 75 |
| 548 | 125 | 88 | 37 |
| 300 | 125 | 88 | 37 |
| CNN Construction | Dimension of Input | Length of the Extracted Deep Features |
|---|---|---|
| ResNet-50 ResNet-18 DenseNet-201 ShuffleNet MobileNet | 224 × 224 × 3 | Binary Classification Level |
| 2 | ||
| Multiclass Classification Level | ||
| 3 | ||
| Inception-V3 Inception-ResNet Xception | 229 × 229 × 3 | Binary Classification Level |
| 2 | ||
| Multiclass Classification Level | ||
| 3 | ||
| DarkNet-19 DarkNet-53 | 226 × 226 × 3 | Binary Classification Level |
| 2 | ||
| Multiclass | ||
| 3 |
| Binary Classification Level | |||||
|---|---|---|---|---|---|
| DT | RF | QDA | LDA | SVM | KNN |
| 97.62 (0.14) | 97.78 (0.06) | 97.6 (0) | 97.6 (0) | 97.6 (0) | 97.36 (0.23) |
| Multiclass classification Level | |||||
| DT | RF | QDA | LDA | SVM | KNN |
| 86.56 (0.8) | 90.88 (0.19) | 85.6 (0.06) | 90.35 (0.21) | 90.43 (0.28) | 89.39 (0.30) |
| Source of Variation | SS | df | MS | F | p Value |
|---|---|---|---|---|---|
| Columns | 0.901 | 5 | 0.180 | 12.54 | <0.001 |
| Error | 0.776 | 54 | 0.014 | ||
| Total | 1.677 | 59 |
| Source of Variation | SS | df | MS | F | p Value |
|---|---|---|---|---|---|
| Columns | 252.148 | 5 | 50.429 | 298.07 | <0.001 |
| Error | 9.136 | 54 | 0.1692 | ||
| Total | 261.284 | 59 |
| Rank | Order | Feature Name |
|---|---|---|
| 461.538 | 18 | Feature 2 of MobileNet |
| 461.538 | 5 | Feature 1 of InceptionResNet |
| 460.68 | 6 | Feature 2 of InceptionResNet |
| 457.854 | 17 | Feature 1 of MobileNet |
| 457.854 | 7 | Feature 1 of Xception |
| 457.592 | 13 | Feature 1 of DarkNet-53 |
| 456.608 | 14 | Feature 2 of DarkNet-53 |
| 456.397 | 19 | Feature 1 of Shuffle |
| 454.198 | 3 | Feature 1 of Inception |
| 454.198 | 2 | Feature 2 of ResNet-50 |
| 454.198 | 4 | Feature 2 of Inception |
| 454.198 | 20 | Feature 2 of Shuffle |
| 454.198 | 10 | Feature 2 of DenseNet |
| 454.198 | 8 | Feature 2 of Xception |
| 454.198 | 15 | Feature 1 of DarkNet-19 |
| 454.198 | 16 | Feature 2 of DarkNet-19 |
| 454.198 | 12 | Feature 2 of ResNet-18 |
| 454.198 | 9 | Feature 1 of DenseNet |
| 454.198 | 11 | Feature 1 of ResNet-18 |
| 454.198 | 1 | Feature 1 of ResNet-50 |
| Rank | Order | Feature Name |
| 1021.0997 | 1 | Feature 1 of ResNet-50 |
| 980.0815 | 25 | Feature 1 of MobileNet |
| 938.3733 | 19 | Feature 1 of DarkNet-53 |
| 932.5696 | 12 | Feature 3 of Xception |
| 926.9128 | 28 | Feature 2 of Shuffle |
| 917.393 | 6 | Feature 3 of Inception |
| 916.3032 | 18 | Feature 3 of ResNet-18 |
| 906.3512 | 13 | Feature 1 of DenseNet |
| 898.5766 | 10 | Feature 1 of Xception |
| 894.4025 | 15 | Feature 3 of DenseNet |
| 886.2739 | 3 | Feature 3 of ResNet-50 |
| 883.1262 | 7 | Feature 1 of InceptionResNet |
| 877.7686 | 21 | Feature 3 of DarkNet-53 |
| 865.6989 | 22 | Feature 1 of DarkNet-19 |
| 814.21 | 2 | Feature 2 of ResNet-50 |
| 811.4717 | 24 | Feature 3 of DarkNet-53 |
| 798.1348 | 16 | Feature 1 of ResNet-18 |
| 797.0761 | 27 | Feature 3 of MobileNet |
| 781.2226 | 4 | Feature 1 of Inception |
| 760.9445 | 8 | Feature 2 of InceptionResNet |
| 755.4454 | 29 | Feature 2 of Shuffle |
| 723.6848 | 11 | Feature 2 of Xception |
| 720.4829 | 23 | Feature 1 of DarkNet-19 |
| 703.0506 | 5 | Feature 2 of Inception |
| 697.2656 | 20 | Feature 2 of DarkNet-53 |
| 697.2656 | 26 | Feature 2 of MobileNet |
| 697.2656 | 17 | Feature 2 of ResNet-18 |
| 697.2656 | 14 | Feature 2 of DenseNet |
| 673.7605 | 9 | Feature 3 of InceptionResNet |
| 634.5971 | 30 | Feature 3 of Shuffle |
| Classifier | Before FS | Forward | Backward | Bidirectional |
|---|---|---|---|---|
| DT | 97.62 | 98.2 | 98.2 | 98.2 |
| RF | 97.78 | 98.0 | 98.0 | 98.0 |
| QDA | 97.6 | 97.8 | 97.6 | 97.8 |
| Classifier | Sensitivity | Specificity | Precision | F1-Score | MCC |
|---|---|---|---|---|---|
| DT | 96.8 | 99.6 | 99.6 | 98.2 | 96.4 |
| RF | 96.0 | 100 | 100 | 96.1 | 98.9 |
| QDA | 95.6 | 100 | 100 | 97.8 | 95.7 |
| Classifier | Before FS | Forward | Backward | Bidirectional |
|---|---|---|---|---|
| RF | 90.88 | 91.6 | 91.33 | 90.93 |
| LDA | 90.35 | 91.07 | 91.07 | 91.33 |
| SVM | 90.43 | 90.58 | 90 | 90.53 |
| Classifier | Sensitivity | Specificity | Precision | F1-score | MCC |
|---|---|---|---|---|---|
| RF | 91.6 | 95.8 | 91.8 | 91.7 | 87.5 |
| LDA | 91.1 | 95.5 | 91.8 | 91.7 | 87.5 |
| SVM | 90.5 | 95.3 | 90.8 | 90.6 | 85.9 |
| Binary Classification Level | |||||
|---|---|---|---|---|---|
| Article | Technique | Sensitivity (%) | Precision (%) | Specificity (%) | Accuracy (%) |
| [64] | hexaxial feature mapping + GLCM + CNN | 98.4 | 94.3 | 94 | 96.2 |
| [63] | ResNet-18 | 98.6 | 98.5 | 96 | 98.62 |
| Presented diagnostic tool | Fully connected deep features + hybrid FS (forward search with DT classifier) | 96.8 | 99.6 | 99.6 | 98.2% |
| Multiclass Classification Level | |||||
| Sensitivity (%) | Precision (%) | Specificity (%) | Accuracy (%) | ||
| [62] | EfficientNet | 75.8 | 80.8 | - | 81.8 |
| [63] | MobileNet | 90.8 | 91.3 | 92.8 | 90.79 |
| Presented diagnostic tool | Fully connected deep features + hybrid FS (forward search with RF classifier) | 91.6 | 91.8 | 95.8 | 91.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Attallah, O. An Intelligent ECG-Based Tool for Diagnosing COVID-19 via Ensemble Deep Learning Techniques. Biosensors 2022, 12, 299. https://doi.org/10.3390/bios12050299
Attallah O. An Intelligent ECG-Based Tool for Diagnosing COVID-19 via Ensemble Deep Learning Techniques. Biosensors. 2022; 12(5):299. https://doi.org/10.3390/bios12050299
Chicago/Turabian StyleAttallah, Omneya. 2022. "An Intelligent ECG-Based Tool for Diagnosing COVID-19 via Ensemble Deep Learning Techniques" Biosensors 12, no. 5: 299. https://doi.org/10.3390/bios12050299
APA StyleAttallah, O. (2022). An Intelligent ECG-Based Tool for Diagnosing COVID-19 via Ensemble Deep Learning Techniques. Biosensors, 12(5), 299. https://doi.org/10.3390/bios12050299