Review of HIV Self Testing Technologies and Promising Approaches for the Next Generation

 , , ,
, , ,  , , and
, , and 
Abstract
:1. Introduction
2. Current State of HIV Self-Testing
3. Current State of Self-Sampling
4. HIV and CD4+ T-Cell Separation, Capture, and Detection

5. Self-Testing Technology Advances in Research and Development
5.1. Antigen Tests

5.2. Antibody Tests

5.3. Nucleic Acid Tests

5.4. Intact Virus Detection

6. Virus Self-Testing Technologies Emerging from SARS-CoV-2 Diagnostics

7. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ollevier, A.; Aguiar, G.; Palomino, M.; Simpelaere, I.S. How can technology support ageing in place in healthy older adults? A systematic review. Public Health Rev. 2020, 41, 26. [Google Scholar] [CrossRef] [PubMed]
- Steehler, K.; Siegler, A.J. Bringing HIV self-testing to scale in the United States: A review of challenges, potential solutions, and future opportunities. J. Clin. Microbiol. 2019, 57, e00257-19. [Google Scholar] [CrossRef] [PubMed]
- McGuire, M.; de Waal, A.; Karellis, A.; Janssen, R.; Engel, N.; Sampath, R.; Carmona, S.; Zwerling, A.A.; Suarez, M.F.; Pai, N.P. HIV self-testing with digital supports as the new paradigm: A systematic review of global evidence (2010–2021). EClinicalMedicine 2021, 39, 101059. [Google Scholar] [CrossRef] [PubMed]
- Ender, P.T.; Markson, R.H.; Suri, A.; Ruppert, K.; Padron, N.; Stoltzfus, J.C.; Berges, V.; Reed, R. Rapid Implementation of a Telemedicine Program in a Ryan White-Funded HIV Clinic During a Global Pandemic. J. Acquir. Immune. Defic. Syndr. 2022, 89, e2–e4. [Google Scholar] [CrossRef]
- El-Nahal, W.G.; Shen, N.M.; Keruly, J.C.; Jones, J.L.; Fojo, A.T.; Lau, B.; Manabe, Y.C.; Moore, R.D.; Gebo, K.A.; Lesko, C.R.; et al. Telemedicine and visit completion among people with HIV during the coronavirus disease 2019 pandemic compared with prepandemic. AIDS 2022, 36, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Ochodo, E.A.; Olwanda, E.E.; Deeks, J.J.; Mallett, S. Point-of-care viral load tests to detect high HIV viral load in people living with HIV/AIDS attending health facilities. Cochrane Database Syst. Rev. 2022, 3, CD013208. [Google Scholar] [CrossRef]
- Branson, B.M.; Handsfield, H.H.; Lampe, M.A.; Janssen, R.S.; Taylor, A.W.; Lyss, S.B.; Clark, J.E. Revised recommendations for HIV testing of adults, adolescents, and pregnant women in health-care settings. MMWR Recomm Rep. 2006, 55, 1–17. [Google Scholar]
- UNAIDS. Fast-Track-Ending the AIDS Epidemic by 2030. 2014. Available online: https://www.unaids.org/en/resources/documents/2014/JC2686_WAD2014report (accessed on 6 December 2022).
- Group, I.S.S.; Lundgren, J.D.; Babiker, A.G.; Gordin, F.; Emery, S.; Grund, B.; Sharma, S.; Avihingsanon, A.; Cooper, D.A.; Fatkenheuer, G.; et al. Initiation of Antiretroviral Therapy in Early Asymptomatic HIV Infection. N. Engl. J. Med. 2015, 373, 795–807. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. HIV Testing. Available online: https://www.cdc.gov/hiv/testing/index.html (accessed on 6 December 2022).
- Luo, W.; Sullivan, V.; Smith, T.; Peters, P.J.; Gay, C.; Westheimer, E.; Cohen, S.E.; Owen, S.M.; Masciotra, S. Performance evaluation of the Bio-Rad Geenius HIV 1/2 supplemental assay. J. Clin. Virol. 2019, 111, 24–28. [Google Scholar] [CrossRef]
- Marson, K.G.; Marlin, R.; Pham, P.; Cohen, S.E.; Jones, D.; Roemer, M.; Peters, P.J.; Haller, B.; Pilcher, C.D. Real-world performance of the new US HIV testing algorithm in medical settings. J. Clin. Virol. 2017, 91, 73–78. [Google Scholar] [CrossRef]
- HIV/AIDS. Available online: https://www.mayoclinic.org/diseases-conditions/hiv-aids/diagnosis-treatment/drc-20373531 (accessed on 6 December 2022).
- House, T.W. Fact Sheet: The Biden Administration Announces Americans Can Order Additional Free At-Home, Rapid COVID-19 Tests at COVIDTests.gov. Available online: https://www.whitehouse.gov/briefing-room/statements-releases/2022/05/17/fact-sheet-the-biden-administration-announces-americans-can-order-additional-free-at-home-rapid-covid-19-tests-at-covidtests-gov/ (accessed on 28 November 2022).
- Weissleder, R.; Lee, H.; Ko, J.; Pittet, M.J. COVID-19 diagnostics in context. Sci. Transl. Med. 2020, 12, eabc1931. [Google Scholar] [CrossRef]
- Perez, S.M. Clusters of Rapid HIV Transmission Among Gay, Bisexual, and Other Men Who Have Sex with Men—United States, 2018–2021. MMWR. Morb. Mortal. Wkly. Rep. 2022, 71, 1201–1206. [Google Scholar] [CrossRef]
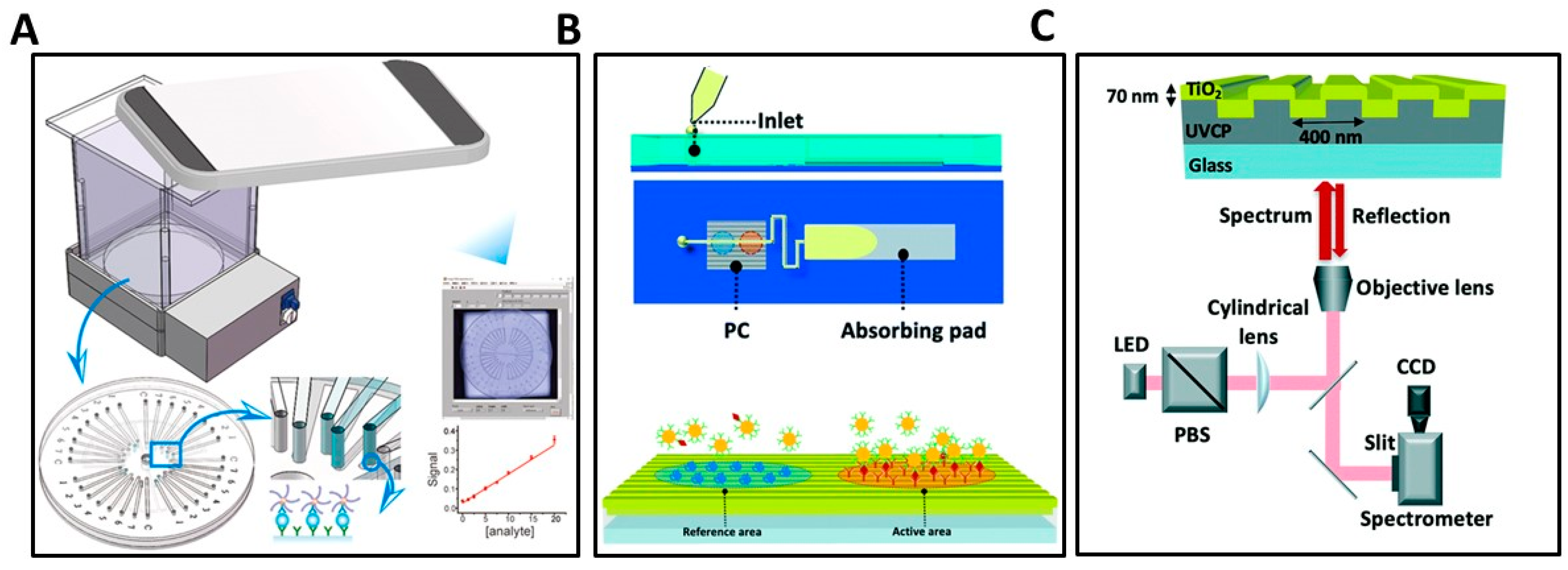
- Ghosh, S.; Li, N.; Xiong, Y.; Ju, Y.G.; Rathslag, M.P.; Onal, E.G.; Falkiewicz, E.; Kohli, M.; Cunningham, B.T. A compact photonic resonator absorption microscope for point of care digital resolution nucleic acid molecular diagnostics. Biomed. Opt. Express 2021, 12, 4637–4650. [Google Scholar] [CrossRef]
- Colasanti, J.A.; Armstrong, W.S. Challenges of reaching 90–90–90 in the Southern United States. Curr. Opin. HIV AIDS 2019, 14, 471–480. [Google Scholar] [CrossRef]
- Deeks, S.G.; Lewin, S.R.; Havlir, D.V. The end of AIDS: HIV infection as a chronic disease. Lancet 2013, 382, 1525–1533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- US Food & Drug Administration. FDA in Brief: FDA Continues to Encourage Ongoing Education about the Benefits and Risks Associated with PrEP, Including Additional Steps to Help Reduce the Risk of Getting HIV. Available online: https://www.fda.gov/news-events/fda-brief/fda-brief-fda-continues-encourage-ongoing-education-about-benefits-and-risks-associated-prep (accessed on 28 November 2022).
- Beyrer, C.; McCormack, S.; Grulich, A. Pre-Exposure Prophylaxis for HIV Infection as a Public Health Tool. J. Law Med. Ethics 2022, 50, 24–28. [Google Scholar] [CrossRef]
- Grispen, J.E.; Ronda, G.; Dinant, G.J.; de Vries, N.K.; van der Weijden, T. To test or not to test: A cross-sectional survey of the psychosocial determinants of self-testing for cholesterol, glucose, and HIV. BMC Public Health 2011, 11, 112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pitasi, M.A.; Beer, L.; Cha, S.; Lyons, S.J.; Hernandez, A.L.; Prejean, J.; Valleroy, L.A.; Crim, S.M.; Trujillo, L.; Hardman, D.; et al. Vital Signs: HIV Infection, Diagnosis, Treatment, and Prevention Among Gay, Bisexual, and Other Men Who Have Sex with Men—United States, 2010–2019. MMWR Morb. Mortal. Wkly Rep. 2021, 70, 1669–1675. [Google Scholar] [CrossRef] [PubMed]
- Peabody, R. Home HIV Testing (Self-Testing and Self-Sampling). Available online: https://www.aidsmap.com/about-hiv/home-hiv-testing-self-testing-and-self-sampling (accessed on 1 December 2022).
- Orasure Technologies. OraQuick® In-Home HIV Test. Available online: https://oraquick.com/oraquick-in-home-hiv-test/ (accessed on 6 December 2022).
- World Health Organization. WHO List of Prequalified In Vitro Diagnostic Products. Available online: https://extranet.who.int/pqweb/vitro-diagnostics/vitro-diagnostics-lists (accessed on 1 November 2022).
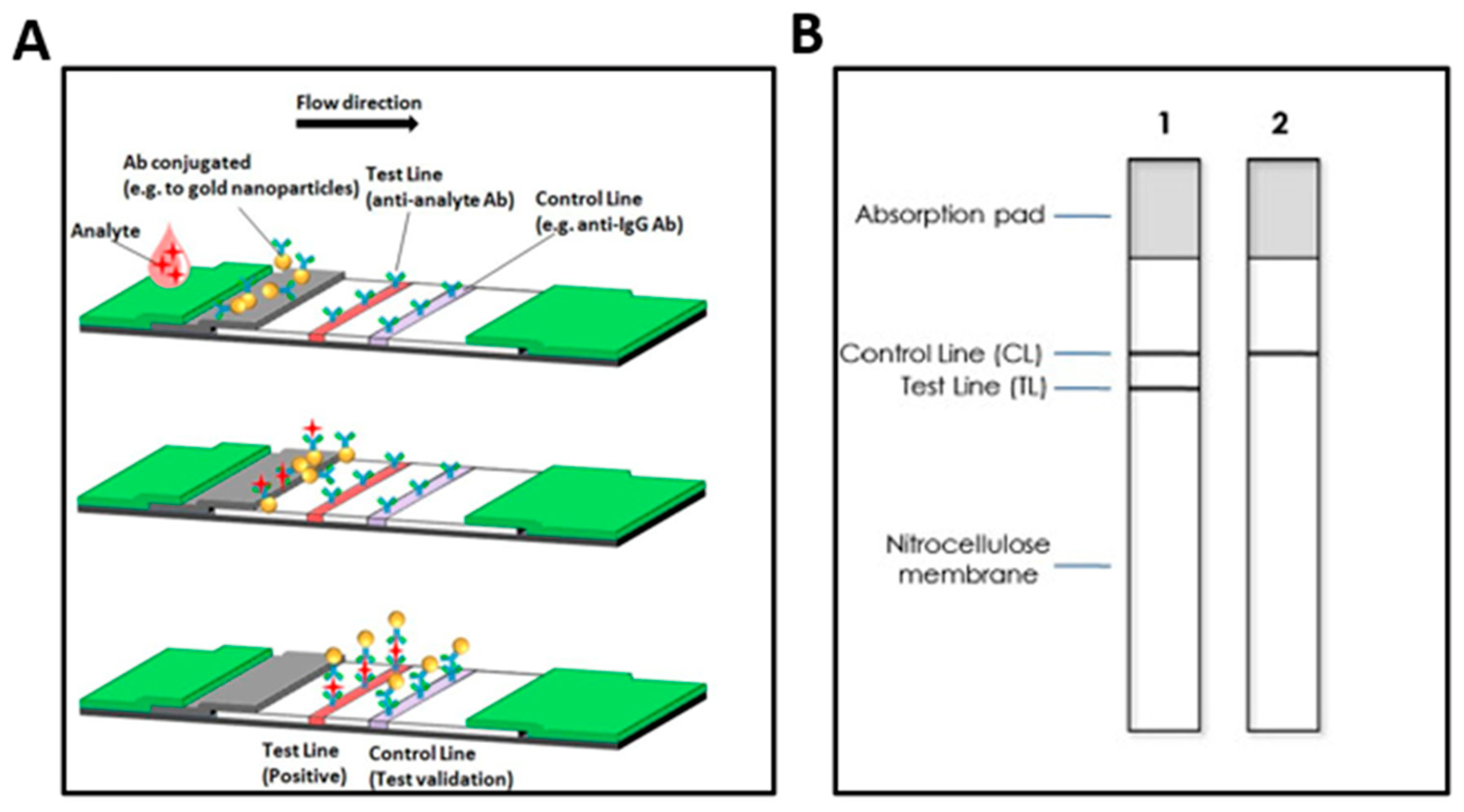
- Banerjee, R.; Jaiswal, A. Recent advances in nanoparticle-based lateral flow immunoassay as a point-of-care diagnostic tool for infectious agents and diseases. Analyst 2018, 143, 1970–1996. [Google Scholar] [CrossRef] [PubMed]
- Koczula, K.M.; Gallotta, A. Lateral flow assays. Essays Biochem. 2016, 60, 111–120. [Google Scholar] [CrossRef] [PubMed]
- Suarez-Pantaleon, C.; Wichers, J.; Abad-Somovilla, A.; van Amerongen, A.; Abad-Fuentes, A. Development of an immunochromatographic assay based on carbon nanoparticles for the determination of the phytoregulator forchlorfenuron. Biosens. Bioelectron. 2013, 42, 170–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bahadir, E.B. Lateral flow assays: Principles, designs and labels. Trends Anal. Chem. 2016, 82, 286–306. [Google Scholar] [CrossRef]
- Yang, W.; Li, X.-B.; Liu, G.-W.; Zhang, B.-B.; Zhang, Y.; Kong, T.; Tang, J.-J.; Li, D.-N.; Wang, Z. A colloidal gold probe-based silver enhancement immunochromatographic assay for the rapid detection of abrin-a. Biosens. Bioelectron. 2011, 26, 3710–3713. [Google Scholar] [CrossRef]
- Panferov, V.G.; Safenkova, I.V.; Zherdev, A.V.; Dzantiev, B.B. Post-assay growth of gold nanoparticles as a tool for highly sensitive lateral flow immunoassay. Application to the detection of potato virus X. Microchim. Acta 2018, 185, 506. [Google Scholar] [CrossRef]
- WHO Prequalification of In Vitro Diagnostics. Product: Determine HIV-1/2. Prequalification of In Vitro Diagnostics Public Report. 2022. Available online: https://extranet.who.int/pqweb/sites/default/files/PQDx_0033-013-00_DetermineHIV-1-2v_7.pdf (accessed on 15 November 2022).
- Wang, Z.; Zhi, D.; Zhao, Y.; Zhang, H.; Wang, X.; Ru, Y.; Li, H. Lateral flow test strip based on colloidal selenium immunoassay for rapid detection of melamine in milk, milk powder, and animal feed. Int. J. Nanomed. 2014, 9, 1699–1707. [Google Scholar] [CrossRef] [Green Version]
- Noguera, P.S.; Posthuma-Trumpie, G.A.; van Tuil, M.; van der Wal, F.J.; Boer, A.d.; Moers, A.P.H.A.; van Amerongen, A. Carbon Nanoparticles as Detection Labels in Antibody Microarrays. Detection of Genes Encoding Virulence Factors in Shiga Toxin-Producing Escherichia coli. Anal. Chem. 2011, 83, 8531–8536. [Google Scholar] [CrossRef]
- Workman, S.; Wells, S.K.; Pau, C.P.; Owen, S.M.; Dong, X.F.; LaBorde, R.; Granade, T.C. Rapid detection of HIV-1 p24 antigen using magnetic immuno-chromatography (MICT). J. Virol. Methods 2009, 160, 14–21. [Google Scholar] [CrossRef]
- Deng, X.; Wang, C.; Gao, Y.; Li, J.; Wen, W.; Zhang, X.; Wang, S. Applying strand displacement amplification to quantum dots-based fluorescent lateral flow assay strips for HIV-DNA detection. Biosens. Bioelectron. 2018, 105, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Fu, X.; Cheng, Z.; Yu, J.; Choo, P.; Chen, L.; Choo, J. A SERS-based lateral flow assay biosensor for highly sensitive detection of HIV-1 DNA. Biosens. Bioelectron. 2016, 78, 530–537. [Google Scholar] [CrossRef]
- Patel, H.K.; Ikpe, S.; Bronson, M.; Birhanu, S.; Abimiku, A.l.; Jahun, I.; Detorio, M.; Lupoli, K.; Yavo, D.; Bassey, O.O.; et al. Performance of HIV rapid testing algorithm in Nigeria: Findings from a household-based Nigeria HIV/AIDS Indicator and Impact Survey (NAIIS). PLoS Glob. Public Health 2022, 2, e0000466. [Google Scholar] [CrossRef]
- Baveewo, S.; Kamya, M.R.; Mayanja-Kizza, H.; Fatch, R.; Bangsberg, D.R.; Coates, T.; Hahn, J.A.; Wanyenze, R.K. Potential for false positive HIV test results with the serial rapid HIV testing algorithm. BMC Res. Notes 2012, 5, 154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO Prequalification of In Vitro Diagnostics. Product: Wondfo HIV Self-Test. Prequalification of In Vitro Diagnostics Public Report. 2022. Available online: https://extranet.who.int/pqweb/sites/default/files/PQDx_0357-004-01_WondfoHIV-Self-test_v1.0.pdf (accessed on 15 November 2022).
- WHO Prequalification of In Vitro Diagnostics. Product: CheckNOW HIV SELF TEST. Prequalification of In Vitro Diagnostics Public Report. 2022. Available online: https://extranet.who.int/pqweb/sites/default/files/PQDx_0481-032-00_CheckNOW_HIV-SelfTest_PR_v2.0.pdf (accessed on 15 November 2022).
- WHO Prequalification of In Vitro Diagnostics. Product: SURE CHECK HIV Self-Test. Prequalification of In Vitro Diagnostics Public Report. 2019. Available online: https://extranet.who.int/pqweb/sites/default/files/191129_pqdx_0054_006_01_sure_check_hiv_self_test.pdf (accessed on 15 November 2022).
- WHO Prequalification of In Vitro Diagnostics. Product: Mylan HIV Self Test. Prequalification of In Vitro Diagnostics Public Report. 2021. Available online: https://extranet.who.int/pqweb/sites/default/files/PQDx_0320-090-00_MylanHIV-SelfTest_V3.0.pdf (accessed on 15 November 2022).
- WHO Prequalification of In Vitro Diagnostics. Product: INSTI HIV Self Test. Prequalification of In Vitro Diagnostics Public Report. 2021. Available online: https://extranet.who.int/pqweb/sites/default/files/PQDx_0002-002-01_INSTI-HIV_SelfTest_v4.0.pdf (accessed on 15 November 2022).
- Mossoro-Kpinde, C.D.; Bobossi, C.; Tonen-Wolyec, S.; Kalla, G.C.M.; Baguida-Bokia, C.; Sombot-Ndicki, S.; Gresenguet, G.; Mbopi-Keou, F.X.; Belec, L. Analytical performances of Exacto((R)) HIV self-test in the Central African Republic. Pan. Afr. Med. J. 2022, 41, 236. [Google Scholar] [CrossRef] [PubMed]
- UNAIDS. Understanding Fast-Track: Accelerating Action to End the Aids Epidemic by 2030. 2020. Available online: https://www.unaids.org/sites/default/files/media_asset/201506_JC2743_Understanding_FastTrack_en.pdf (accessed on 15 November 2022).
- Lippman, S.A.; Gilmore, H.J.; Lane, T.; Radebe, O.; Chen, Y.H.; Mlotshwa, N.; Maleke, K.; Manyuchi, A.E.; McIntyre, J. Ability to use oral fluid and fingerstick HIV self-testing (HIVST) among South African MSM. PLoS ONE 2018, 13, e0206849. [Google Scholar] [CrossRef] [Green Version]
- WHO Prequalification of In Vitro Diagnostics. Product: OraQuick HIV Self-Test. Prequalification of In Vitro Diagnostics Public Report. 2022. Available online: https://extranet.who.int/pqweb/sites/default/files/PQDx_0159-055-01_OraQuickHIVSelfTest_v7.0.pdf (accessed on 15 November 2022).
- Kosack, C.S.; Page, A.L.; Beelaert, G.; Benson, T.; Savane, A.; Ng’ang’a, A.; Andre, B.; Zahinda, J.B.; Shanks, L.; Fransen, K. Towards more accurate HIV testing in sub-Saharan Africa: A multi-site evaluation of HIV RDTs and risk factors for false positives. J. Int. AIDS Soc. 2017, 19, 21345. [Google Scholar] [CrossRef] [PubMed]
- Alemnji, G.A.; Ngulefac, G.A.; Ndumbe, P.M.; Asonganyi, T. Field evaluation of Calypte’s AWARE blood serum plasma (BSP) and oral mucosal transudate (OMT) rapid tests for detecting antibodies to HIV-1 and 2 in plasma and oral fluid. Open AIDS J. 2009, 3, 14–18. [Google Scholar] [CrossRef] [Green Version]
- WHO Prequalification of In Vitro Diagnostics. Product: HIV 1/2 STAT-PAK®. Prequalification of In Vitro Diagnostics Public Report. 2012. Available online: https://extranet.who.int/pqweb/sites/default/files/120116_0007_006_00_public_report_final_v1.pdf (accessed on 15 November 2022).
- WHO Prequalification of In Vitro Diagnostics. Product: DPP® HIV 1/2 Assay. Prequalification of In Vitro Diagnostics Public Report. 2018. Available online: https://extranet.who.int/pqweb/sites/default/files/180130_final_amended_pqpr_0053_006_00_v3.pdf (accessed on 15 November 2022).
- Jaspard, M.; Le Moal, G.; Saberan-Roncato, M.; Plainchamp, D.; Langlois, A.; Camps, P.; Guigon, A.; Hocqueloux, L.; Prazuck, T. Finger-stick whole blood HIV-1/-2 home-use tests are more sensitive than oral fluid-based in-home HIV tests. PLoS ONE 2014, 9, e101148. [Google Scholar] [CrossRef]
- WHO Prequalification of In Vitro Diagnostics. Product: SURE CHECK HIV 1/2 Assay. Prequalification of In Vitro Diagnostics Public Report. 2020. Available online: https://extranet.who.int/pqweb/sites/default/files/PQDx_0054-006-00_SURE-CHECK_HIV_1-2_Assay_v3.pdf (accessed on 15 November 2022).
- Mayaphi, S.H.; Martin, D.J.; Quinn, T.C.; Stoltz, A.C. Field performance of the INSTI HIV-1/-2 antibody test in two South African antenatal clinics. J. Med. Virol. 2019, 91, 1355–1359. [Google Scholar] [CrossRef]
- WHO Prequalification of In Vitro Diagnostics. Product: INSTI HIV-1/HIV-2 Antibody Test. Prequalification of In Vitro Diagnostics Public Report. 2019. Available online: https://extranet.who.int/pqweb/sites/default/files/191111_amended_final_pqpr_0002_002_00_v5-rsize.pdf (accessed on 15 November 2022).
- WHO Prequalification of In Vitro Diagnostics. Product: Uni-Gold HIV. Prequalification of In Vitro Diagnostics Public Report. 2021. Available online: https://extranet.who.int/pqweb/sites/default/files/PQDx_0149-052-00-Uni-Gold_HIV_v11.pdf (accessed on 15 November 2022).
- WHO Prequalification of In Vitro Diagnostics. Product: Genie™ Fast HIV 1/2. Prequalification of In Vitro Diagnostics Public Report. 2017. Available online: https://extranet.who.int/pqweb/sites/default/files/171222_final_pq_report_0153_031_00_v3.pdf (accessed on 15 November 2022).
- WHO Prequalification of In Vitro Diagnostics. Product: MERISCREEN HIV 1-2 WB. Prequalification of In Vitro Diagnostics Public Report. 2020. Available online: https://extranet.who.int/pqweb/sites/default/files/PQDx_0464_074_00_meriscreen_hiv_WB.pdf (accessed on 15 November 2022).
- Boadu, R.; Darko, G.; Nortey, P.; Akweongo, P.; Sarfo, B. Assessing the sensitivity and specificity of First Response HIV-1-2 test kit with whole blood and serum samples: A cross-sectional study. AIDS Res. Ther. 2016, 13, 9. [Google Scholar] [CrossRef] [Green Version]
- WHO Prequalification of In Vitro Diagnostics. Product: ONE STEP Anti-HIV (1&2) Test. Prequalification of In Vitro Diagnostics Public Report. 2020. Available online: https://extranet.who.int/pqweb/sites/default/files/200219_amended_pqpr_0372_017_00_one_step_anti_hiv_test_v2.pdf (accessed on 15 November 2022).
- Turbe, V.; Herbst, C.; Mngomezulu, T.; Meshkinfamfard, S.; Dlamini, N.; Mhlongo, T.; Smit, T.; Cherepanova, V.; Shimada, K.; Budd, J.; et al. Deep learning of HIV field-based rapid tests. Nat. Med. 2021, 27, 1165–1170. [Google Scholar] [CrossRef]
- WHO Prequalification of In Vitro Diagnostics. Product: STANDARD Q HIV 1/2 Ab 3-Line Test. Prequalification of In Vitro Diagnostics Public Report. 2020. Available online: https://extranet.who.int/pqweb/sites/default/files/PQDx_0383-117-00_STANDARD-Q-HIV-12-Ab3-LineTest_v1.pdf (accessed on 15 November 2022).
- WHO Prequalification of In Vitro Diagnostics. Product: Bioline HIV 1/2 3.0. Prequalification of In Vitro Diagnostics Public Report. 2020. Available online: https://extranet.who.int/pqweb/sites/default/files/PQDx_0027-012-00_BiolineHIV_1-2-3_v5.pdf (accessed on 15 November 2022).
- WHO Prequalification of In Vitro Diagnostics. Product: Diagnostic kit for HIV (1+2) antibody (colloidal gold) V2. Prequalification of In Vitro Diagnostics Public Report. 2016. Available online: https://extranet.who.int/pqweb/content/public-report-diagnostic-kit-hiv12-antibody-colloidal-gold-v2-pqdx-0267-037-00 (accessed on 15 November 2022).
- Guillon, G.; Yearwood, G.; Snipes, C.; Boschi, D.; Reed, M.R. Human anti-HIV IgM detection by the OraQuick ADVANCE(R) Rapid HIV 1/2 Antibody Test. PeerJ 2018, 6, e4430. [Google Scholar] [CrossRef] [Green Version]
- WHO Prequalification of In Vitro Diagnostics. Product: Rapid Test for Antibody to Human Immunodeficiency Virus (HIV) (Colloidal Gold Device). Prequalification of In Vitro Diagnostics Public Report. 2020. Available online: https://extranet.who.int/pqweb/sites/default/files/PQDx_0005-005-00_ColloidalGoldDevice_v4.pdf (accessed on 15 November 2022).
- WHO Prequalification of In Vitro Diagnostics. Product: ABON HIV 1/2/O Tri-Line Human Immunodeficiency Virus Rapid Test Device. Prequalification of In Vitro Diagnostics Public Report. 2019. Available online: https://extranet.who.int/pqweb/sites/default/files/190301_amended_pqpr_0141_051_00_v7.pdf (accessed on 15 November 2022).
- van den Berk, G.E.; Frissen, P.H.; Regez, R.M.; Rietra, P.J. Evaluation of the rapid immunoassay determine HIV 1/2 for detection of antibodies to human immunodeficiency virus types 1 and 2. J. Clin. Microbiol. 2003, 41, 3868–3869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO Prequalification of In Vitro Diagnostics. Product: TrinScreen HIV. Prequalification of In Vitro Diagnostics Public Report. 2022. Available online: https://extranet.who.int/pqweb/sites/default/files/PQDx_0473-052-00-TrinScreenHIV.pdf (accessed on 15 November 2022).
- da Motta, L.R.; Vanni, A.C.; Kato, S.K.; Borges, L.G.; Sperhacke, R.D.; Ribeiro, R.M.; Inocencio, L.A.; The HIV Rapid Test Evaluation Group. Evaluation of five simple rapid HIV assays for potential use in the Brazilian national HIV testing algorithm. J. Virol. Methods 2013, 194, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Rossetti, R.; Smith, T.; Luo, W.; Masciotra, S. Performance evaluation of the MedMira reveal G4 LAB S/P and POC HIV antibody rapid screening tests using plasma and whole blood specimens. J. Clin. Virol. 2020, 127, 104344. [Google Scholar] [CrossRef] [PubMed]
- Wechsberg, W.M.; van der Horst, C.; Ndirangu, J.; Doherty, I.A.; Kline, T.; Browne, F.A.; Belus, J.M.; Nance, R.; Zule, W.A. Seek, test, treat: Substance-using women in the HIV treatment cascade in South Africa. Addict. Sci. Clin. Pract. 2017, 12, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Majam, M.; Rhagnath, N.; Msolomba, V.; Singh, L.; Urdea, M.S.; Lalla-Edward, S.T. Usability and Clinical Performance Characteristics of the Asante HIV1/2 Test by Trained Users in Two African Sites. Diagnostics 2021, 11, 1727. [Google Scholar] [CrossRef]
- WHO Prequalification of In Vitro Diagnostics. Product: STANDARD Q HIV/Syphilis Combo Test. Prequalification of In Vitro Diagnostics Public Report. 2020. Available online: https://extranet.who.int/pqweb/sites/default/files/PQDx_0382-117-00_Standard_Q-HIV-SyphilisComboTest_0.pdf (accessed on 15 November 2022).
- WHO Prequalification of In Vitro Diagnostics. Product: First Response HIV1+2/Syphilis Combo Card Test. Prequalification of In Vitro Diagnostics Public Report. 2020. Available online: https://extranet.who.int/pqweb/sites/default/files/200219_amended_pqpr_0364_010_00_first_response_hiv_1_2_syphilis_combo_v2.pdf (accessed on 15 November 2022).
- WHO Prequalification of In Vitro Diagnostics. Product: Bioline HIV/Syphilis Duo. Prequalification of In Vitro Diagnostics Public Report. 2022. Available online: https://extranet.who.int/pqweb/sites/default/files/PQDx_0179-012-00_BiolineHIVSyphilisDuo_PublicReport_v7.0.pdf (accessed on 15 November 2022).
- Gruner, N.; Stambouli, O.; Ross, R.S. Dried blood spots--preparing and processing for use in immunoassays and in molecular techniques. J. Vis. Exp. 2015, 97, e52619. [Google Scholar] [CrossRef] [Green Version]
- Lim, M.D. Dried Blood Spots for Global Health Diagnostics and Surveillance: Opportunities and Challenges. Am. J. Trop Med. Hyg. 2018, 99, 256–265. [Google Scholar] [CrossRef] [Green Version]
- Delahaye, L.; Veenhof, H.; Koch, B.C.P.; Alffenaar, J.C.; Linden, R.; Stove, C. Alternative Sampling Devices to Collect Dried Blood Microsamples: State-of-the-Art. Drug Monit. 2021, 43, 310–321. [Google Scholar] [CrossRef]
- Marchand, A.; Roulland, I.; Semence, F.; Beck, O.; Ericsson, M. Use of Quantitative Dried Blood Spots to Evaluate the Post-Vaccination Level of Neutralizing Antibodies against SARS-CoV-2. Life 2021, 11, 1125. [Google Scholar] [CrossRef]
- Leuthold, L.A.; Heudi, O.; Deglon, J.; Raccuglia, M.; Augsburger, M.; Picard, F.; Kretz, O.; Thomas, A. New microfluidic-based sampling procedure for overcoming the hematocrit problem associated with dried blood spot analysis. Anal. Chem. 2015, 87, 2068–2071. [Google Scholar] [CrossRef] [PubMed]
- Zasada, A.A.; Zacharczuk, K.; Woznica, K.; Glowka, M.; Ziolkowski, R.; Malinowska, E. The influence of a swab type on the results of point-of-care tests. AMB Express 2020, 10, 46. [Google Scholar] [CrossRef] [PubMed]
- Microbiology, R. Flocked Swabs Proven Superior in Sample Uptake and Release. Available online: https://www.rapidmicrobiology.com/news/flocked-swabs-proven-superior-in-sample-uptake-and-release (accessed on 6 December 2022).
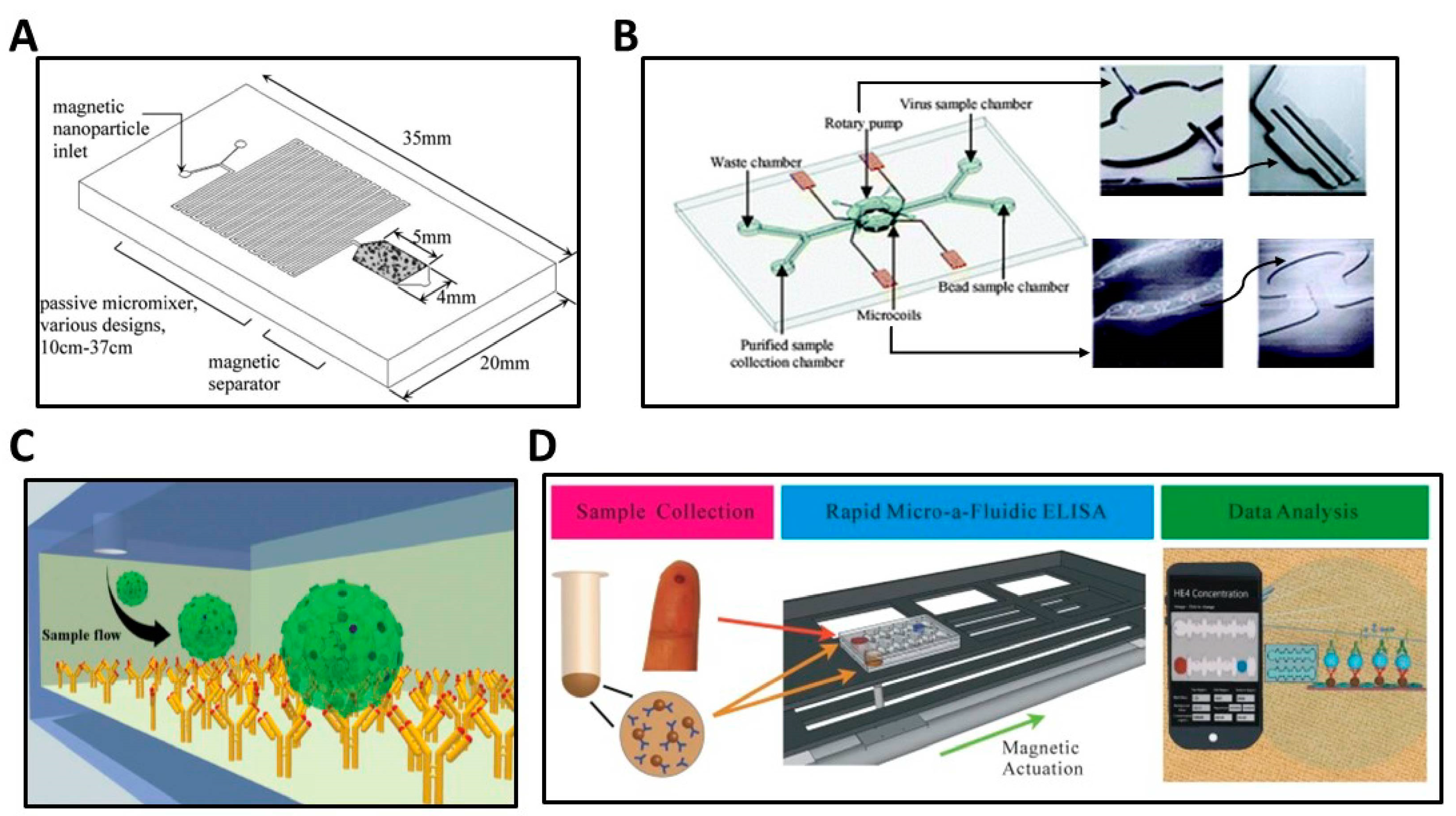
- Chen, G.D.; Alberts, C.J.; Rodriguez, W.; Toner, M. Concentration and Purification of Human Immunodeficiency Virus Type 1 Virions by Microfluidic Separation of Superparamagnetic Nanoparticles. Anal. Chem. 2010, 82, 723–728. [Google Scholar] [CrossRef] [Green Version]
- Lien, K.-Y.; Lin, J.-L.; Liu, C.-Y.; Lei, H.-Y.; Lee, G.-B. Purification and enrichment of virus samples utilizing magnetic beads on a microfluidic system. Lab Chip 2007, 7, 868–875. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Esfahani, M.; Gurkan, U.A.; Inci, F.; Kuritzkes, D.R.; Demirci, U. Efficient on-chip isolation of HIV subtypes. Lab Chip 2012, 12, 1508–1515. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Xu, F.; Demirci, U. Advances in developing HIV-1 viral load assays for resource-limited settings. Biotechnol. Adv. 2010, 28, 770–781. [Google Scholar] [CrossRef] [Green Version]
- Okoye, A.A.; Picker, L.J. CD4(+) T-cell depletion in HIV infection: Mechanisms of immunological failure. Immunol. Rev. 2013, 254, 54–64. [Google Scholar] [CrossRef] [Green Version]
- Thorsen, T.; Maerkl, S.J.; Quake, S.R. Microfluidic large-scale integration. Science 2002, 298, 580–584. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Tasoglu, S.; Chen, P.Z.; Chen, M.; Akbas, R.; Wach, S.; Ozdemir, C.I.; Gurkan, U.A.; Giguel, F.F.; Kuritzkes, D.R.; et al. Micro-a-fluidics ELISA for Rapid CD4 Cell Count at the Point-of-Care. Sci. Rep. 2014, 4, 3796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Orgainzation. Consolidated Guidelines On the Use of Antiretroviral Drugs for Treating and Preventing HIV Infection: Recommendations for a Public Health Approach. Available online: https://www.who.int/publications/i/item/9789241549684 (accessed on 6 December 2022).
- Teeparuksapun, K.; Hedström, M.; Wong, E.Y.; Tang, S.; Hewlett, I.K.; Mattiasson, B. Ultrasensitive Detection of HIV-1 p24 Antigen Using Nanofunctionalized Surfaces in a Capacitive Immunosensor. Anal. Chem. 2010, 82, 8406–8411. [Google Scholar] [CrossRef]
- Bangalee, A.; Bhoora, S.; Punchoo, R. Evaluation of serological assays for the diagnosis of HIV infection in adults. S. Afr. Fam. Pract. (2004) 2021, 63, e1–e5. [Google Scholar] [CrossRef]
- Sickinger, E.; Stieler, M.; Kaufman, B.; Kapprell, H.P.; West, D.; Sandridge, A.; Devare, S.; Schochetman, G.; Hunt, J.C.; Daghfal, D. Multicenter evaluation of a new, automated enzyme-linked immunoassay for detection of human immunodeficiency virus-specific antibodies and antigen. J. Clin. Microbiol. 2004, 42, 21–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, M.; Li, N.; Mao, G.; Liu, Y.; Wang, X.; Tian, S.; Hu, Q.; Ji, X.; Liu, Y.; He, Z. Self-assembled fluorescent Ce(Ⅲ) coordination polymer as ratiometric probe for HIV antigen detection. Anal. Chim. Acta 2019, 1084, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Kurdekar, A.D.; Avinash Chunduri, L.A.; Manohar, C.S.; Haleyurgirisetty, M.K.; Hewlett, I.K.; Venkataramaniah, K. Streptavidin-conjugated gold nanoclusters as ultrasensitive fluorescent sensors for early diagnosis of HIV infection. Sci. Adv. 2018, 4, eaar6280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, F.; Zheng, Y.; Yang, M.; Zhang, Y.; Pu, Q. A triple-layer microchannel array chip with micro through-holes for smartphone based point-of-care testing of biomarker. Sens. Actuators B Chem. 2022, 351, 130963. [Google Scholar] [CrossRef]
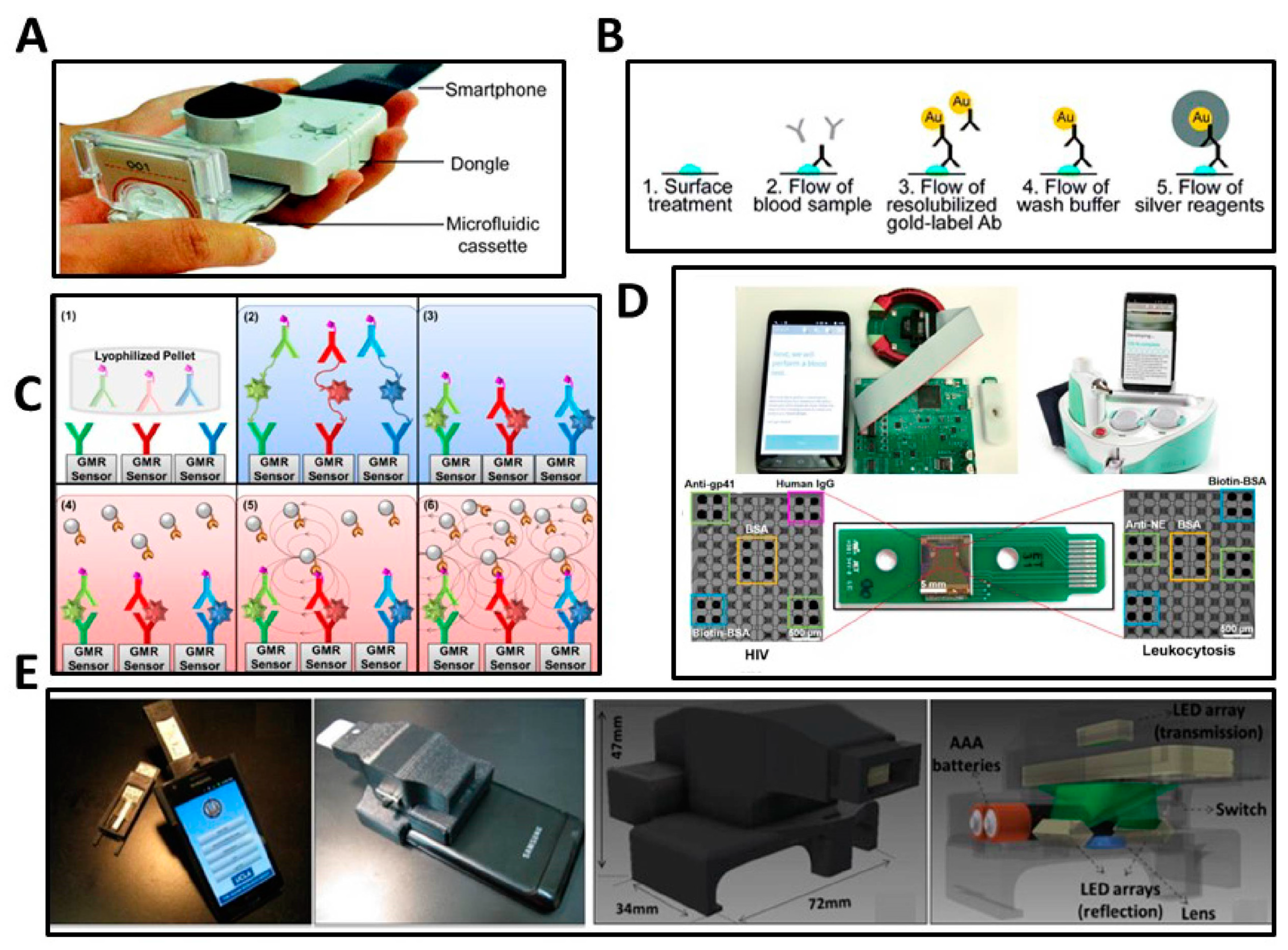
- Ng, E.; Yao, C.; Shultz, T.O.; Ross-Howe, S.; Wang, S.X. Magneto-nanosensor smartphone platform for the detection of HIV and leukocytosis at point-of-care. Nanomedicine 2019, 16, 10–19. [Google Scholar] [CrossRef]
- Choi, J.; Gani, A.W.; Bechstein, D.J.B.; Lee, J.R.; Utz, P.J.; Wang, S.X. Portable, one-step, and rapid GMR biosensor platform with smartphone interface. Biosens. Bioelectron. 2016, 85, 1–7. [Google Scholar] [CrossRef]
- Che, C.; Li, N.; Long, K.D.; Aguirre, M.A.; Canady, T.D.; Huang, Q.; Demirci, U.; Cunningham, B.T. Activate capture and digital counting (AC + DC) assay for protein biomarker detection integrated with a self-powered microfluidic cartridge. Lab Chip 2019, 19, 3943–3953. [Google Scholar] [CrossRef]
- Canady, T.D.; Li, N.; Smith, L.D.; Lu, Y.; Kohli, M.; Smith, A.M.; Cunningham, B.T. Digital-resolution detection of microRNA with single-base selectivity by photonic resonator absorption microscopy. Proc. Natl. Acad. Sci. USA 2019, 116, 19362–19367. [Google Scholar] [CrossRef] [Green Version]
- Zhao, B.; Che, C.; Wang, W.; Li, N.; Cunningham, B.T. Single-step, wash-free digital immunoassay for rapid quantitative analysis of serological antibody against SARS-CoV-2 by photonic resonator absorption microscopy. Talanta 2021, 225, 122004. [Google Scholar] [CrossRef]
- Zhao, B.; Wang, W.; Li, N.; Garcia-Lezana, T.; Che, C.; Wang, X.; Losic, B.; Villanueva, A.; Cunningham, B.T. Digital-resolution and highly sensitive detection of multiple exosomal small RNAs by DNA toehold probe-based photonic resonator absorption microscopy. Talanta 2022, 241, 123256. [Google Scholar] [CrossRef]
- Xiong, Y.; Li, N.; Che, C.; Wang, W.; Barya, P.; Liu, W.; Liu, L.; Wang, X.; Wu, S.; Hu, H.; et al. Microscopies Enabled by Photonic Metamaterials. Sensors 2022, 22, 1086. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. HIV Testing: Understanding the HIV Window Period. Available online: https://www.cdc.gov/hiv/basics/hiv-testing/hiv-window-period.html (accessed on 6 December 2022).
- Dobaño, C.; Vidal, M.; Santano, R.; Jiménez, A.; Chi, J.; Barrios, D.; Ruiz-Olalla, G.; Melero, N.R.; Carolis, C.; Parras, D.; et al. Highly sensitive and specific multiplex antibody assays to quantify immunoglobulins M, A and G against SARS-CoV-2 antigens. bioRxiv 2020, 2020.2006.2011.147363. [Google Scholar] [CrossRef] [PubMed]
- Alexander, T.S. Human Immunodeficiency Virus Diagnostic Testing: 30 Years of Evolution. Clin. Vaccine Immunol. 2016, 23, 249–253. [Google Scholar] [CrossRef]
- Daskalakis, D. HIV diagnostic testing: Evolving technology and testing strategies. Top Antivir. Med. 2011, 19, 18–22. [Google Scholar] [PubMed]
- Liu, J.; Geng, Z.; Fan, Z.; Liu, J.; Chen, H. Point-of-care testing based on smartphone: The current state-of-the-art (2017-2018). Biosens. Bioelectron. 2019, 132, 17–37. [Google Scholar] [CrossRef]
- Cunningham, B.; Canady, T.; Zhao, B.; Ghosh, S.; Li, N.; Huang, Q.; Xiong, Y.; Fried, G.; Kohli, M.; Demirci, U.; et al. Photonic Metamaterial Surfaces for Digital Resolution Biosensor Microscopies Using Enhanced Absorption, Scattering, and Emission; SPIE: Washington, DC, USA, 2021; Volume 11663. [Google Scholar]
- Guo, T.; Patnaik, R.; Kuhlmann, K.; Rai, A.J.; Sia, S.K. Smartphone dongle for simultaneous measurement of hemoglobin concentration and detection of HIV antibodies. Lab Chip 2015, 15, 3514–3520. [Google Scholar] [CrossRef] [PubMed]
- Laksanasopin, T.; Guo, T.W.; Nayak, S.; Sridhara, A.A.; Xie, S.; Olowookere, O.O.; Cadinu, P.; Meng, F.; Chee, N.H.; Kim, J.; et al. A smartphone dongle for diagnosis of infectious diseases at the point of care. Sci. Transl. Med. 2015, 7, 273re271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mudanyali, O.; Dimitrov, S.; Sikora, U.; Padmanabhan, S.; Navruz, I.; Ozcan, A. Integrated rapid-diagnostic-test reader platform on a cellphone. Lab Chip 2012, 12, 2678–2686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garg, N.; Boyle, D.; Randall, A.; Teng, A.; Pablo, J.; Liang, X.; Camerini, D.; Lee, A.P. Rapid immunodiagnostics of multiple viral infections in an acoustic microstreaming device with serum and saliva samples. Lab Chip 2019, 19, 1524–1533. [Google Scholar] [CrossRef]
- Oliveira, B.B.; Veigas, B.; Baptista, P.V. Isothermal Amplification of Nucleic Acids: The Race for the Next “Gold Standard”. Front. Sens. 2021, 2, 752600. [Google Scholar] [CrossRef]
- Liang, Y.; Li, L.; Shui, J.; Hu, F.; Wang, H.; Xia, Y.; Cai, W.; Tang, S. Reduction of anti-HIV antibody responses in subjects receiving antiretroviral therapy during chronic HIV-1 infection. J. Clin. Virol. 2020, 128, 104414. [Google Scholar] [CrossRef] [PubMed]
- Weld, E.D. Limits of Detection and Limits of Infection: Quantitative HIV Measurement in the Era of U = U. J. Appl. Lab. Med. 2020, 6, 324–326. [Google Scholar] [CrossRef]
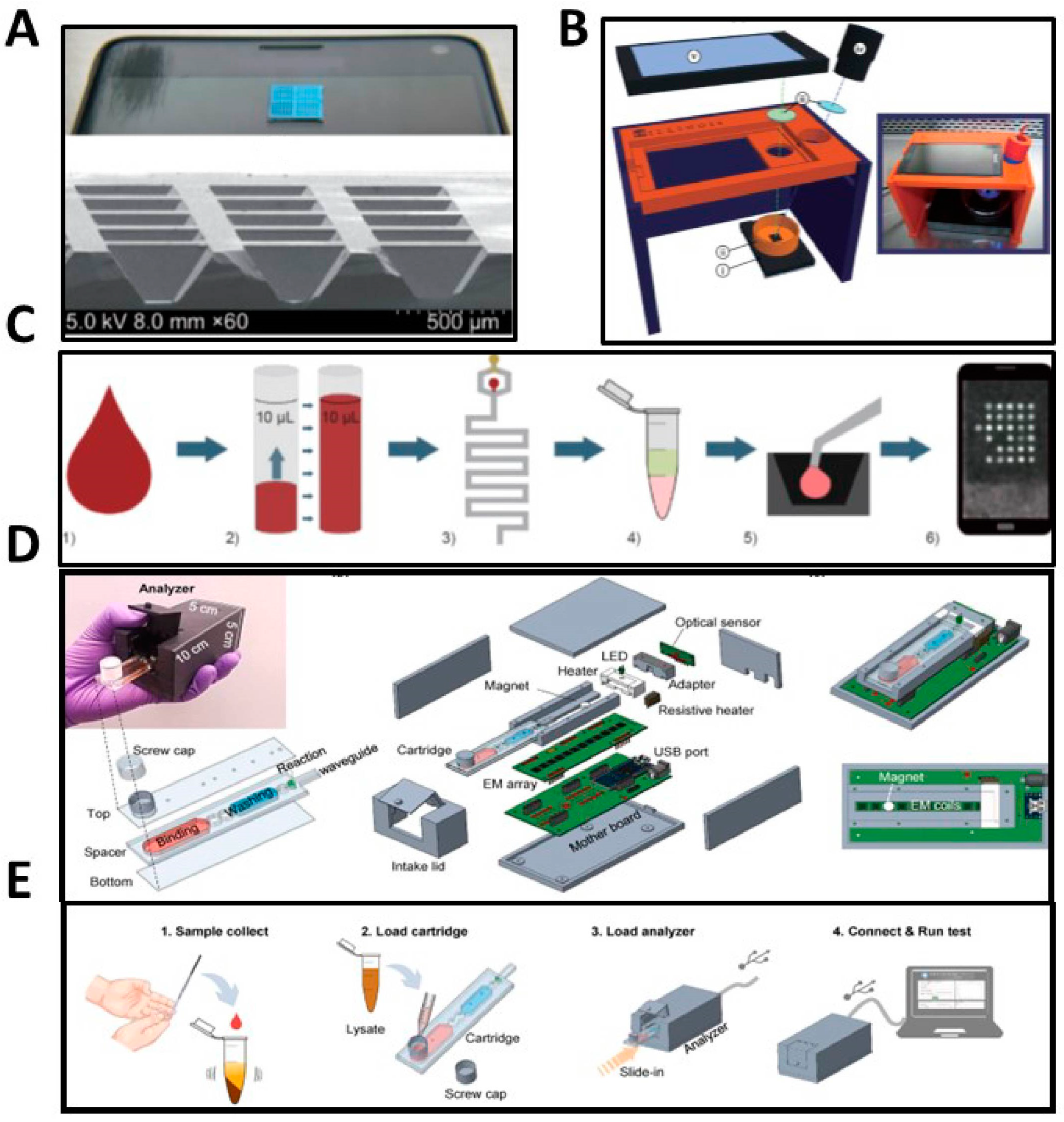
- Damhorst, G.L.; Duarte-Guevara, C.; Chen, W.; Ghonge, T.; Cunningham, B.T.; Bashir, R. Smartphone-Imaged HIV-1 Reverse-Transcription Loop-Mediated Isothermal Amplification (RT-LAMP) on a Chip from Whole Blood. Engineering 2015, 1, 324–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jankelow, A.M.; Lee, H.; Wang, W.; Hoang, T.-H.; Bacon, A.; Sun, F.; Chae, S.; Kindratenko, V.; Koprowski, K.; Stavins, R.A.; et al. Smartphone clip-on instrument and microfluidic processor for rapid sample-to-answer detection of Zika virus in whole blood using spatial RT-LAMP. Analyst 2022, 147, 3838–3853. [Google Scholar] [CrossRef] [PubMed]
- Mauk, M.; Song, J.; Bau, H.H.; Gross, R.; Bushman, F.D.; Collman, R.G.; Liu, C. Miniaturized devices for point of care molecular detection of HIV. Lab Chip 2017, 17, 382–394. [Google Scholar] [CrossRef] [Green Version]
- Das, D.; Lin, C.-W.; Chuang, H.-S. LAMP-Based Point-of-Care Biosensors for Rapid Pathogen Detection. Biosensors 2022, 12, 1068. [Google Scholar] [CrossRef] [PubMed]
- Hosaka, N.; Ndembi, N.; Ishizaki, A.; Kageyama, S.; Numazaki, K.; Ichimura, H. Rapid detection of human immunodeficiency virus type 1 group M by a reverse transcription-loop-mediated isothermal amplification assay. J. Virol. Methods 2009, 157, 195–199. [Google Scholar] [CrossRef]
- Liu, T.; Choi, G.; Tang, Z.; Kshirsagar, A.; Politza, A.J.; Guan, W. Fingerpick Blood-Based Nucleic Acid Testing on A USB Interfaced Device towards HIV self-testing. Biosens. Bioelectron. 2022, 209, 114255. [Google Scholar] [CrossRef]
- Myers, F.B.; Henrikson, R.H.; Bone, J.; Lee, L.P. A Handheld Point-of-Care Genomic Diagnostic System. PLoS ONE 2013, 8, e70266. [Google Scholar] [CrossRef]
- Curtis, K.A.; Rudolph, D.L.; Nejad, I.; Singleton, J.; Beddoe, A.; Weigl, B.; LaBarre, P.; Owen, S.M. Isothermal amplification using a chemical heating device for point-of-care detection of HIV-1. PLoS ONE 2012, 7, e31432. [Google Scholar] [CrossRef]
- Kim, D.; Wei, Q.; Kim, D.H.; Tseng, D.; Zhang, J.; Pan, E.; Garner, O.; Ozcan, A.; Di Carlo, D. Enzyme-Free Nucleic Acid Amplification Assay Using a Cellphone-Based Well Plate Fluorescence Reader. Anal. Chem. 2018, 90, 690–695. [Google Scholar] [CrossRef]
- Huang, C.-H.; Park, Y.I.; Lin, H.-Y.; Pathania, D.; Park, K.S.; Avila-Wallace, M.; Castro, C.M.; Weissleder, R.; Lee, H. Compact and Filter-Free Luminescence Biosensor for Mobile In Vitro Diagnoses. ACS Nano 2019, 13, 11698–11706. [Google Scholar] [CrossRef] [PubMed]
- Tarim, E.A.; Karakuzu, B.; Oksuz, C.; Sarigil, O.; Kizilkaya, M.; Al-Ruweidi, M.; Yalcin, H.C.; Ozcivici, E.; Tekin, H.C. Microfluidic-based virus detection methods for respiratory diseases. Emergent Mater. 2021, 4, 143–168. [Google Scholar] [CrossRef]
- Poghossian, A.; Jablonski, M.; Molinnus, D.; Wege, C.; Schöning, M.J. Field-Effect Sensors for Virus Detection: From Ebola to SARS-CoV-2 and Plant Viral Enhancers. Front. Plant Sci. 2020, 11, 598103. [Google Scholar] [CrossRef]
- Syahir, A.; Usui, K.; Tomizaki, K.Y.; Kajikawa, K.; Mihara, H. Label and Label-Free Detection Techniques for Protein Microarrays. Microarrays 2015, 4, 228–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cunningham, B.T.; Laing, L.G. Advantages and application of label-free detection assays in drug screening. Expert Opin. Drug Discov. 2008, 3, 891–901. [Google Scholar] [CrossRef]
- Rapp, B.E.; Gruhl, F.J.; Länge, K. Biosensors with label-free detection designed for diagnostic applications. Anal. Bioanal. Chem. 2010, 398, 2403–2412. [Google Scholar] [CrossRef]
- Li, N.; Wang, X.; Tibbs, J.; Che, C.; Peinetti, A.S.; Zhao, B.; Liu, L.; Barya, P.; Cooper, L.; Rong, L.; et al. Label-Free Digital Detection of Intact Virions by Enhanced Scattering Microscopy. J. Am. Chem. Soc. 2022, 144, 1498–1502. [Google Scholar] [CrossRef]
- Inci, F.; Tokel, O.; Wang, S.; Gurkan, U.A.; Tasoglu, S.; Kuritzkes, D.R.; Demirci, U. Nanoplasmonic Quantitative Detection of Intact Viruses from Unprocessed Whole Blood. ACS Nano 2013, 7, 4733–4745. [Google Scholar] [CrossRef]
- Chauhan, N.; Xiong, Y.; Ren, S.; Dwivedy, A.; Magazine, N.; Zhou, L.; Jin, X.; Zhang, T.; Cunningham, B.T.; Yao, S.; et al. Net-Shaped DNA Nanostructures Designed for Rapid/Sensitive Detection and Potential Inhibition of the SARS-CoV-2 Virus. J. Am. Chem. Soc. 2022, jacs.2c04835. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Canady, T.D.; Huang, Q.; Wang, X.; Fried, G.A.; Cunningham, B.T. Photonic resonator interferometric scattering microscopy. Nat. Commun. 2021, 12, 1744. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, X.; Mauk, M.G.; Yin, K.; Kadimisetty, K.; Liu, C. Interfacing Pathogen Detection with Smartphones for Point-of-Care Applications. Anal. Chem. 2019, 91, 655–672. [Google Scholar] [CrossRef] [PubMed]
- Malekjahani, A.; Sindhwani, S.; Syed, A.M.; Chan, W.C.W. Engineering Steps for Mobile Point-of-Care Diagnostic Devices. Acc. Chem. Res. 2019, 52, 2406–2414. [Google Scholar] [CrossRef]
- Xiao, M.; Tian, F.; Liu, X.; Zhou, Q.; Pan, J.; Luo, Z.; Yang, M.; Yi, C. Virus Detection: From State-of-the-Art Laboratories to Smartphone-Based Point-of-Care Testing. Adv. Sci. 2022, 9, 2105904. [Google Scholar] [CrossRef]
- Zhang, Z.; Ma, P.; Ahmed, R.; Wang, J.; Akin, D.; Soto, F.; Liu, B.-F.; Li, P.; Demirci, U. Advanced Point-of-Care Testing Technologies for Human Acute Respiratory Virus Detection. Adv. Mater. 2022, 34, 2103646. [Google Scholar] [CrossRef]
- Eissa, S. Diagnostic biosensors for coronaviruses and recent developments. Adv. Biosens. Virus Detect. 2022, 261–278. [Google Scholar] [CrossRef]
- Renzoni, A.; Perez, F.; Ngo Nsoga, M.T.; Yerly, S.; Boehm, E.; Gayet-Ageron, A.; Kaiser, L.; Schibler, M. Analytical Evaluation of Visby Medical RT-PCR Portable Device for Rapid Detection of SARS-CoV-2. Diagnostics 2021, 11, 813. [Google Scholar] [CrossRef]
- Donato, L.J.; Trivedi, V.A.; Stransky, A.M.; Misra, A.; Pritt, B.S.; Binnicker, M.J.; Karon, B.S. Evaluation of the Cue Health point-of-care COVID-19 (SARS-CoV-2 nucleic acid amplification) test at a community drive through collection center. Diagn Microbiol. Infect. Dis. 2021, 100, 115307. [Google Scholar] [CrossRef]
- Iwamoto, T.; Sonobe, T.; Hayashi, K. Loop-mediated isothermal amplification for direct detection of Mycobacterium tuberculosis complex, M. avium, and M. intracellulare in sputum samples. J. Clin. Microbiol. 2003, 41, 2616–2622. [Google Scholar] [CrossRef] [Green Version]
- Compton, J. Nucleic acid sequence-based amplification. Nature 1991, 350, 91–92. [Google Scholar] [CrossRef] [PubMed]
- Lillis, L.; Lehman, D.A.; Siverson, J.B.; Weis, J.; Cantera, J.; Parker, M.; Piepenburg, O.; Overbaugh, J.; Boyle, D.S. Cross-subtype detection of HIV-1 using reverse transcription and recombinase polymerase amplification. J. Virol. Methods 2016, 230, 28–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mota, D.S.; Guimarães, J.M.; Gandarilla, A.M.D.; Filho, J.C.B.S.; Brito, W.R.; Mariúba, L.A.M. Recombinase polymerase amplification in the molecular diagnosis of microbiological targets and its applications. Can. J. Microbiol. 2022, 68, 383–402. [Google Scholar] [CrossRef]
- Sun, B.; Shen, F.; McCalla, S.E.; Kreutz, J.E.; Karymov, M.A.; Ismagilov, R.F. Mechanistic evaluation of the pros and cons of digital RT-LAMP for HIV-1 viral load quantification on a microfluidic device and improved efficiency via a two-step digital protocol. Anal. Chem. 2013, 85, 1540–1546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez-Manzano, J.; Karymov, M.A.; Begolo, S.; Selck, D.A.; Zhukov, D.V.; Jue, E.; Ismagilov, R.F. Reading Out Single-Molecule Digital RNA and DNA Isothermal Amplification in Nanoliter Volumes with Unmodified Camera Phones. ACS Nano 2016, 10, 3102–3113. [Google Scholar] [CrossRef] [Green Version]
- Lin, X.; Huang, X.; Urmann, K.; Xie, X.; Hoffmann, M.R. Digital Loop-Mediated Isothermal Amplification on a Commercial Membrane. ACS Sens 2019, 4, 242–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlappi, T.S.; McCalla, S.E.; Schoepp, N.G.; Ismagilov, R.F. Flow-through Capture and in Situ Amplification Can Enable Rapid Detection of a Few Single Molecules of Nucleic Acids from Several Milliliters of Solution. Anal. Chem. 2016, 88, 7647–7653. [Google Scholar] [CrossRef] [PubMed]
- Amouzadeh Tabrizi, M.; Fernández-Blázquez, J.P.; Medina, D.M.; Acedo, P. An ultrasensitive molecularly imprinted polymer-based electrochemical sensor for the determination of SARS-CoV-2-RBD by using macroporous gold screen-printed electrode. Biosens. Bioelectron. 2022, 196, 113729. [Google Scholar] [CrossRef] [PubMed]
- Ayankojo, A.G.; Boroznjak, R.; Reut, J.; Öpik, A.; Syritski, V. Molecularly imprinted polymer based electrochemical sensor for quantitative detection of SARS-CoV-2 spike protein. Sens. Actuators B Chem. 2022, 353, 131160. [Google Scholar] [CrossRef]
- Ratautaite, V.; Boguzaite, R.; Brazys, E.; Ramanaviciene, A.; Ciplys, E.; Juozapaitis, M.; Slibinskas, R.; Bechelany, M.; Ramanavicius, A. Molecularly imprinted polypyrrole based sensor for the detection of SARS-CoV-2 spike glycoprotein. Electrochim. Acta 2022, 403, 139581. [Google Scholar] [CrossRef]
- Singhal, A.; Parihar, A.; Kumar, N.; Khan, R. High throughput molecularly imprinted polymers based electrochemical nanosensors for point-of-care diagnostics of COVID-19. Mater. Lett. 2022, 306, 130898. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Shen, X.L.; Zeng, Q.; Wang, H.S.; Wang, L.S. A multi-walled carbon nanotubes based molecularly imprinted polymers electrochemical sensor for the sensitive determination of HIV-p24. Talanta 2017, 164, 121–127. [Google Scholar] [CrossRef]
- Liu, Z.; Meng, T.; Tang, X.; Tian, R.; Guan, W. The Promise of Aggregation-Induced Emission Luminogens for Detecting COVID-19. Front. Immunol. 2021, 12, 635558. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Fan, Y.-Y.; Wen, J.; Zhang, J.; Zhang, Z.-Q. Metal-Enhanced Aggregation-Induced Emission Strategy for the HIV-I RNA-Binding Ligand Assay. Anal. Chem. 2022, 94, 4695–4702. [Google Scholar] [CrossRef] [PubMed]
- Thanihaichelvan, M.; Surendran, S.N.; Kumanan, T.; Sutharsini, U.; Ravirajan, P.; Valluvan, R.; Tharsika, T. Selective and electronic detection of COVID-19 (Coronavirus) using carbon nanotube field effect transistor-based biosensor: A proof-of-concept study. Mater. Today Proc. 2022, 49, 2546–2549. [Google Scholar] [CrossRef]
- Shao, W.; Shurin, M.R.; Wheeler, S.E.; He, X.; Star, A. Rapid Detection of SARS-CoV-2 Antigens Using High-Purity Semiconducting Single-Walled Carbon Nanotube-Based Field-Effect Transistors. ACS Appl. Mater. Interfaces 2021, 13, 10321–10327. [Google Scholar] [CrossRef] [PubMed]
- Seo, G.; Lee, G.; Kim, M.J.; Baek, S.-H.; Choi, M.; Ku, K.B.; Lee, C.-S.; Jun, S.; Park, D.; Kim, H.G.; et al. Rapid Detection of COVID-19 Causative Virus (SARS-CoV-2) in Human Nasopharyngeal Swab Specimens Using Field-Effect Transistor-Based Biosensor. ACS Nano 2020, 14, 5135–5142. [Google Scholar] [CrossRef] [Green Version]
- Ali, M.A.; Hu, C.; Jahan, S.; Yuan, B.; Saleh, M.S.; Ju, E.; Gao, S.-J.; Panat, R. Sensing of COVID-19 Antibodies in Seconds via Aerosol Jet Nanoprinted Reduced-Graphene-Oxide-Coated 3D Electrodes. Adv. Mater. 2021, 33, e2006647. [Google Scholar] [CrossRef]
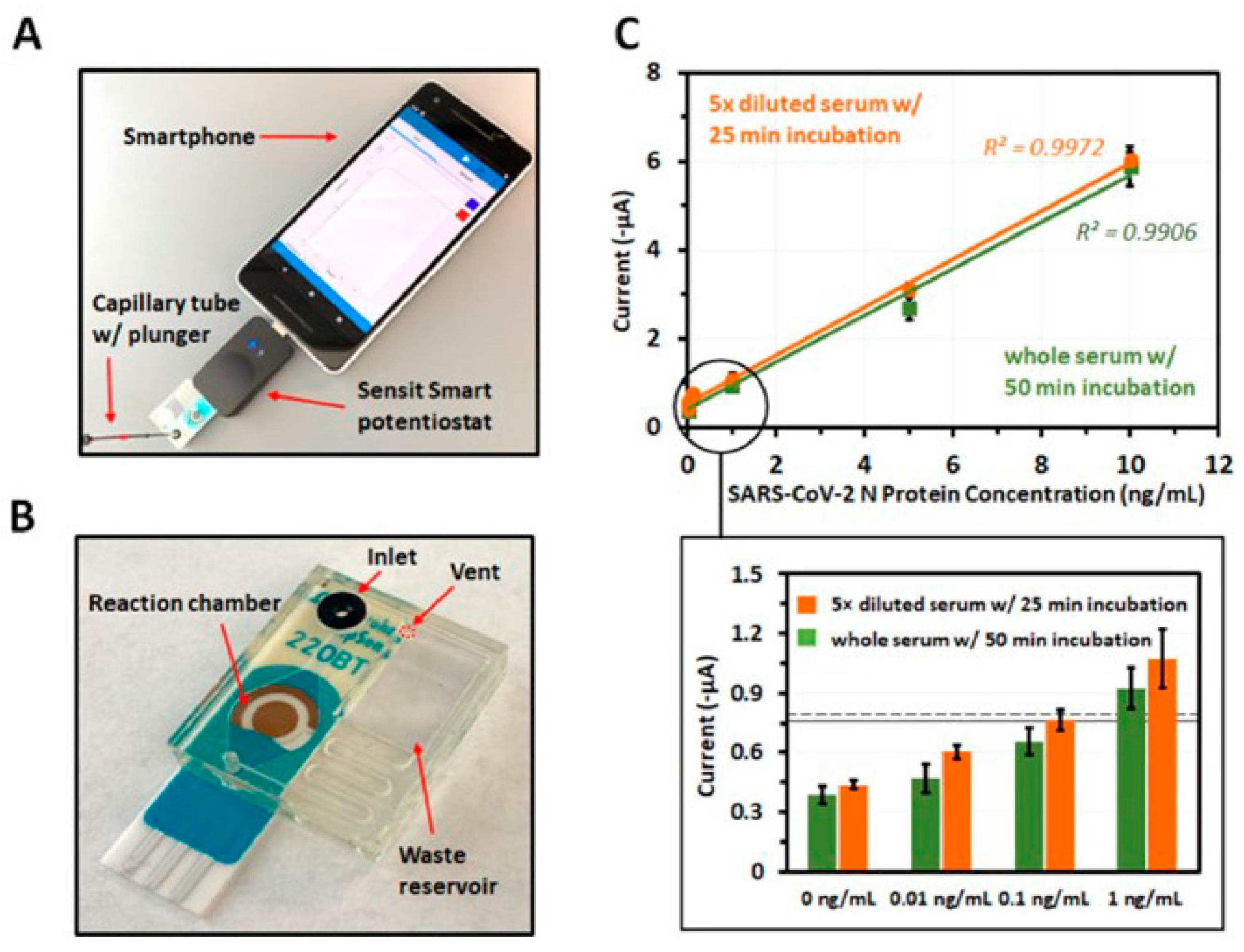
- Li, J.; Lillehoj, P.B. Microfluidic Magneto Immunosensor for Rapid, High Sensitivity Measurements of SARS-CoV-2 Nucleocapsid Protein in Serum. ACS Sens. 2021, 6, 1270–1278. [Google Scholar] [CrossRef]
- Boppart, S.A.; Richards-Kortum, R. Point-of-care and point-of-procedure optical imaging technologies for primary care and global health. Sci. Transl. Med. 2014, 6, 253rv252. [Google Scholar] [CrossRef] [Green Version]
- RADx Programs. Available online: https://www.nibib.nih.gov/covid-19/radx-tech-program (accessed on 6 December 2020).
- Robinson, M.; Gaydos, C.; Van Der Pol, B.; McFall, S.; Hsieh, Y.-H.; Clarke, W.; Murphy, R.L.; Widdice, L.E.; Hirschhorn, L.R.; Rothman, R.; et al. The Clinical Review Committee: Impact of the Development of In Vitro Diagnostic Tests for SARS-CoV-2 Within RADx Tech. IEEE Open J. Eng. Med. Biol. 2021, 2, 138–141. [Google Scholar] [CrossRef] [PubMed]
- Land, K.J.; Boeras, D.I.; Chen, X.-S.; Ramsay, A.R.; Peeling, R.W. REASSURED diagnostics to inform disease control strategies, strengthen health systems and improve patient outcomes. Nat Microbiol 2019, 4, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.S.; Chen, Y.Q.; McCauley, M.; Gamble, T.; Hosseinipour, M.C.; Kumarasamy, N.; Hakim, J.G.; Kumwenda, J.; Grinsztejn, B.; Pilotto, J.H.; et al. Prevention of HIV-1 infection with early antiretroviral therapy. N. Engl. J. Med. 2011, 365, 493–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okoli, C.; Van de Velde, N.; Richman, B.; Allan, B.; Castellanos, E.; Young, B.; Brough, G.; Eremin, A.; Corbelli, G.M.; Mc Britton, M.; et al. Undetectable equals untransmittable (U = U): Awareness and associations with health outcomes among people living with HIV in 25 countries. Sex. Transm. Infect. 2021, 97, 18–26. [Google Scholar] [CrossRef]
- Center for Disease Control and Protection. HIV and Gay and Bisexual Men: HIV Diagnoses. Available online: https://www.cdc.gov/hiv/group/msm/msm-content/diagnoses.html (accessed on 6 December 2022).
- Hirshfield, S.; Downing, M.J.; Chiasson, M.A.; Houang, S.T.; Yoon, I.S.; Teran, R. Would HIV-positive MSM use a home viral load test? In Proceedings of the International Association of Providers of AIDS Care, Fort Lauderdale, FL, USA, 11 May 2016. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Product Name | Manufacturer | Specimen | Time to Result | Analyte | Sensitivity/Specificity (95% CI) | Regulatory Approval | |
|---|---|---|---|---|---|---|---|
| * | Wondfo HIV Self-Test [41] | Guangzhou Wondfo Biotech Co | WB | 15–30 min | HIV-1/2 Ab | 95.8%/99.6% | WHO PQ, |
| * | CheckNOW HIV SELF TEST [42] | Abbott Rapid Diagnostics | WB | 15–20 min | HIV-1/2 Ab | 99.5%/98.5% | WHO PQ, CE marked |
| * | SURE CHECK® HIV Self-Test [43] | Chembio Diagnostic Systems | WB | 15–20 min | HIV-1/2 Ab | 97%/100% | WHO PQ, FDA |
| * | Mylan HIV Self Test [44] | Atomo Diagnostics | WB | 15–20 min | HIV-1/2 Ab | 99.8%/99.8% | WHO PQ |
| * | INSTI® HIV Self Test [45] | bioLytical Laboratories | WB | 5 min | HIV-1/2 Ab | 99.8%/99.5% | WHO PQ, CE marked |
| * | Exacto HIV self-test [46] | Biosynex | WB | 10–20 min | HIV-1/2 Ab | 100%/99.9% | CE marked |
| * | Autotest VIH® [7] | AAZ | WB | 15–20 min | HIV-1/2 Ab | 99.86%/99.95% | WHO PQ, CE marked |
| * | Action! HIV Self-Test [47] | Chembio Diagnostic Systems | WB | 10–20 min | HIV-1/2 Ab & p24 Ag | 99.9%/99.9% | CE marked |
| * | AtomoRapid HIV Self-Test (3rd) [48] | Atomo Diagnostics | WB | 15–20 min | HIV-1/2 Ab | 99.6%/99.6% | CE marked |
| * | OraQuick® HIV Self-Test [49] | OraSure Technologies | Oral fluid | 20–40 min | HIV-1/2 Ab | 99.4%/99.0% | WHO PQ, CE Marked |
| * | Saliteste HIV [50] | Ebram Product | WB | – | HIV-1/2 Ab | -/99.8% | |
| * | AWARETM HIV-1/2 OMT Oral HIV Self Test [51] | Calyple | Oral fluid | 20–40 min | HIV-1/2 Ab | 99.2%/99.9% | |
| ** | HIV 1/2 STAT-PAK [52] | Chembio Diagnostic Systems | WB | 15–20 min | HIV-1/2 Ab | 99.52%/100% | WHO PQ, FDA |
| ** | DPP HIV 1/2 Assay [53,54] | Chembio Diagnostic Systems | WB or oral fluid | 30–45 min | HIV-1/2 Ab | 100%/99.9% | WHO PQ, FDA CE marked |
| ** | SURE CHECK® HIV 1/2 Assay [54,55] | Chembio Diagnostic Systems | WB | 15–20 min | HIV-1/2 Ab | 99.8%/99.9% | WHO PQ, FDA |
| ** | INSTI HIV-1/HIV-2 Antibody Test [56,57] | BioLytical Laboratories | WB | 5 min | HIV-1/2 Ab | 99.6%/99.3% | WHO PQ, FDA, CE Marked |
| ** | Uni-Gold HIV [58] | Trinity Biotech Manufacturing | WB | 10–12 min | HIV-1/2 Ab | 99.76%/99.85% | WHO PQ |
| ** | Genie Fast HIV 1/2 [50,59] | Bio-Rad | WB | 10–30 min | HIV-1/2 Ab | 100%/98.5% | WHO PQ, CE marked |
| ** | MERISCREEN HIV 1-2 WB [60] | Meril Diagnostics | WB | 20–30 min | HIV-1/2 Ab | 99.4%/99.9% | WHO PQ, CE Marked |
| ** | First Response HIV 1-2.O Card test (Version 2.0) [61] | Premier Medical Corporation Private Limited | WB | 15–25 min | HIV-1/2 Ab | 100%/100% | WHO PQ, CE Marked |
| ** | ONE STEP Anti-HIV (1&2) Test [62,63] | InTec PRODUCTS | WB | 15–20 min | HIV-1/2 Ab | 100%/100% | WHO PQ, CE Marked |
| ** | STANDARD Q HIV 1/2 Ab 3-Line Test [64] | SD Biosensor | WB | 10–20 min | HIV-1/2 Ab | 100%/99.3% | WHO PQ, |
| ** | Bioline HIV-1/2 3.0 [65] | Abbott Diagnostics Korea | WB | 10–20 min | HIV-1/2 Ab | 100%/99.9% | WHO PQ, |
| ** | Diagnostic kit for HIV (1 + 2) antibody (colloidal gold) V2 [66] | Shanghai Kehua Bioengineering | WB | 15–25 min | HIV-1/2 Ab | 100%/100% | WHO PQ, |
| ** | OraQuick® HIV 1/2 Advance Rapid Antibody Test [67] | OraSure Technologies | WB | 20 min | HIV-1/2 Ab | 99.1%/99.8% | WHO PQ, FDA |
| ** | Rapid Test for Antibody to HIV (Colloidal Gold Device) [68] | Beijing Wantai Biological Pharmacy Enterprise | WB | 15–20 min | HIV-1/2 Ab | 100%/98.48% | WHO PQ, |
| ** | ABON HIV 1/2/O Tri-Line Human Immunodeficiency Virus Rapid Test Device [69] | ABON Biopharm | WB | 10–20 min | HIV-1/2 Ab | 100%/99.7% | WHO PQ, |
| ** | Determine HIV-1/2 [70] | Abbott Diagnostics Medical Co | WB | 15–60 min | HIV-1/2 Ab | 100%/98.93% | WHO PQ, |
| ** | TrinScreen HIV [71] | Trinity Biotech Manufacturing | WB | 10–12 min | HIV-1/2 Ab | 100%/100% | WHO PQ, |
| ** | Vikia HIV-1/2 [72] | bioMérieux | WB | 30 min | HIV-1/2 Ab | 99.86%/99.95% | CE marked |
| ** | Reveal Rapid HIV-1 Antibody Test [73] | MedMira | WB | Immediate | HIV-1 Ab | 99.8%/99.1% | FDA |
| ** | iCARE One-Step HIV1&2 Whole Blood/Serum/Plasma Test [74] | JAL Innovation | WB | 10 min | HIV-1/2 Ab | ||
| - | Asanté™ HIV-1/2 Oral Fluid Rapid Test [75] | Sedia | Oral fluid | 20 min | HIV1/2 Ab | ||
| ** | STANDARD Q HIV/Syphilis Combo Test [76] | SD Biosensor | WB | 10–20 min | HIV-1/2 Ab, and syphilis | 100%/99.9% (HIV) 98.8%/100% (Syphilis) | WHO PQ |
| ** | First Response HIV1 + 2/Syphilis Combo Card Test [77] | Premier Medical Corporation Private Limited | WB | 15–25 min | HIV-1/2 Ab, and syphilis | 100%/99.5% (HIV-1/2) 99%/100% (Syphilis) | WHO PQ |
| ** | Bioline HIV/Syphilis Duo [78] | Abbott Diagnostics Korea | WB | 15–20 min | HIV-1/2 Ab, and syphilis | 100%/99.5% (HIV-1/2) 87%/99.5% (Syphilis) | WHO PQ |
| Product Name | Manufacturer | Specimen | Anolyte | Format | Regulatory Approval | |
|---|---|---|---|---|---|---|
| * | Home Access HIV-1 Test System | Home Access Health Corp | WB | HIV-1 Ab | Dried blood spot | FDA |
| * | OraQuick In-Home HIV Test | OraSure Technologies | Oral fluid | HIV-1/2 Ab | Oral fluid | FDA |
| * | TASSO-M20 | Tasso | WB | Dried blood spot | FDA, CE mark | |
| * | OneDraw | DrawBridge Health | WB | Wet | FDA, CE marked | |
| * | Capitainer qDBS | Capitainer | WB | Dried blood spot | FDA (Filed) | |
| * | HemaPEN | Trajan Scientific and Medical | WB | Dried blood spot | ||
| * | HemaSpot HF/SE/HD | Spot on Science | WB | Dried blood spot | ||
| * | Mitra Blood Collection Device | Neoteryx | WB | Dried blood spot | ||
| ** | OraSure HIV-1 Oral Specimen Collection Device | OraSure Technologies | Oral fluid | HIV-1 Ab | Oral fluid | FDA |
| ** | Haiim | Winnoz | WB | Wet | CE mark | |
| - | HemaXis DB10 | DBS System | WB | Dried blood spot | ||
| - | Touch Activated Phlebotomy (TAP) 20CTM | Seventh Sense Biosystems | WB | Dried blood spot | ||
| - | TASSO-SST | Tasso | WB | Wet | ||
| - | PBS-1000 | PreciHealth | WB | Wet | ||
| - | Noviplex Cards | Shimadzu | WB | Dried plasma spot | ||
| - | Book-Type Dried Plasma Spot Card | WB | Dried plasma spot |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bacon, A.; Wang, W.; Lee, H.; Umrao, S.; Sinawang, P.D.; Akin, D.; Khemtonglang, K.; Tan, A.; Hirshfield, S.; Demirci, U.; et al. Review of HIV Self Testing Technologies and Promising Approaches for the Next Generation. Biosensors 2023, 13, 298. https://doi.org/10.3390/bios13020298
Bacon A, Wang W, Lee H, Umrao S, Sinawang PD, Akin D, Khemtonglang K, Tan A, Hirshfield S, Demirci U, et al. Review of HIV Self Testing Technologies and Promising Approaches for the Next Generation. Biosensors. 2023; 13(2):298. https://doi.org/10.3390/bios13020298
Chicago/Turabian StyleBacon, Amanda, Weijing Wang, Hankeun Lee, Saurabh Umrao, Prima Dewi Sinawang, Demir Akin, Kodchakorn Khemtonglang, Anqi Tan, Sabina Hirshfield, Utkan Demirci, and et al. 2023. "Review of HIV Self Testing Technologies and Promising Approaches for the Next Generation" Biosensors 13, no. 2: 298. https://doi.org/10.3390/bios13020298
APA StyleBacon, A., Wang, W., Lee, H., Umrao, S., Sinawang, P. D., Akin, D., Khemtonglang, K., Tan, A., Hirshfield, S., Demirci, U., Wang, X., & Cunningham, B. T. (2023). Review of HIV Self Testing Technologies and Promising Approaches for the Next Generation. Biosensors, 13(2), 298. https://doi.org/10.3390/bios13020298