Development of Single-Channel Dual-Element Custom-Made Ultrasound Scanner with Miniature Optical Position Tracker for Freehand Imaging



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
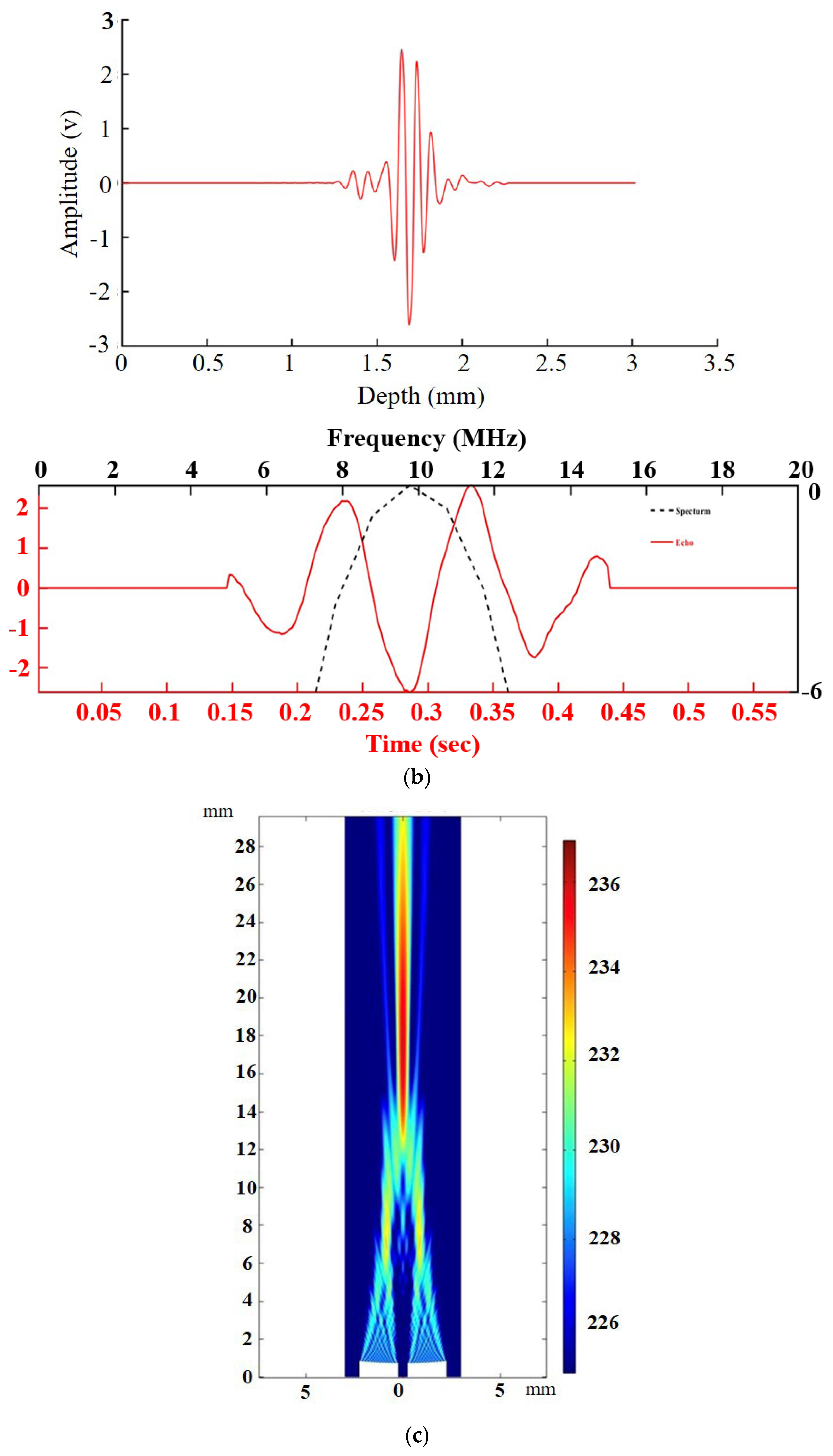
2.1. Dual-Element Ultrasound Transducer
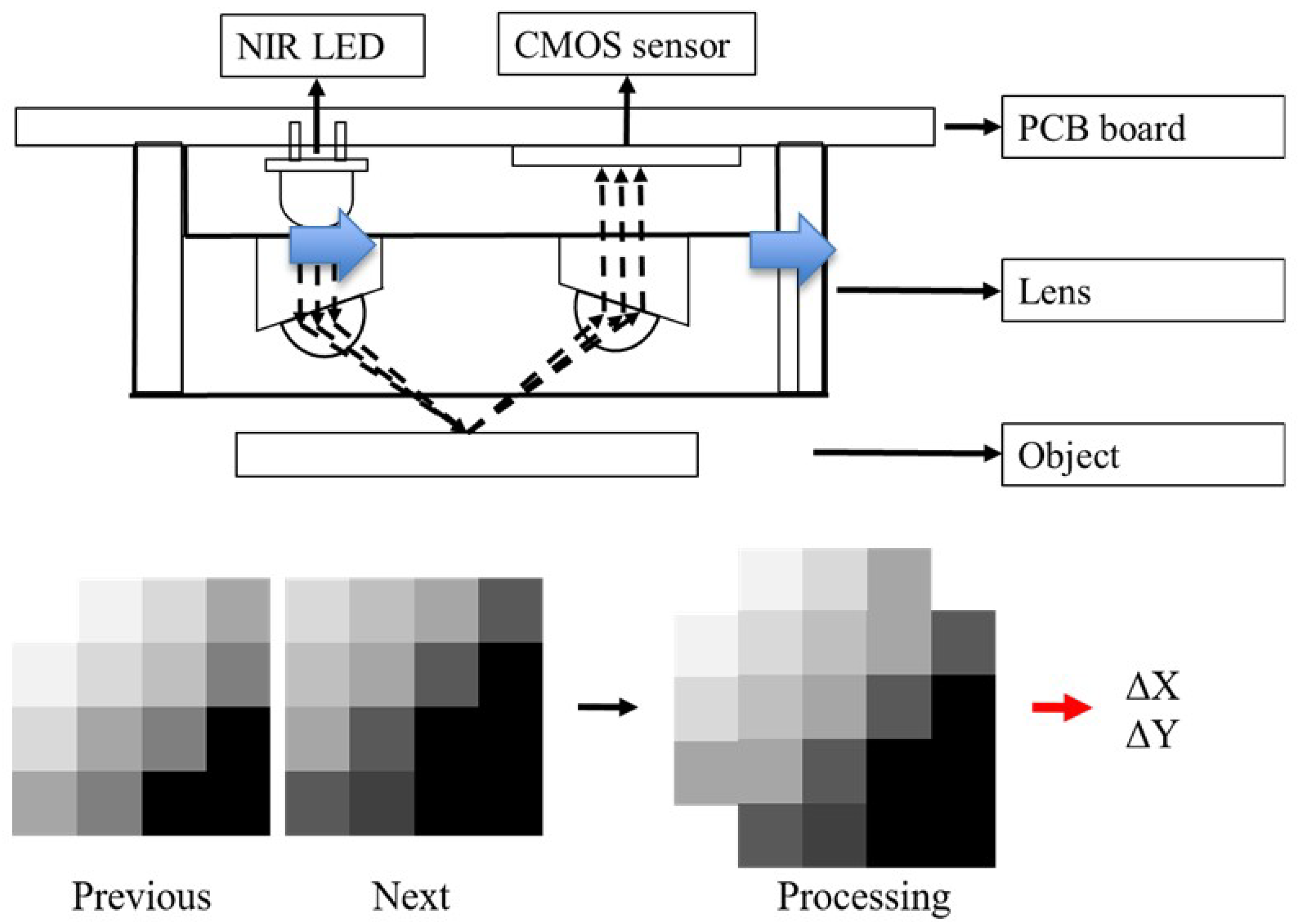
2.2. Optical Tracker
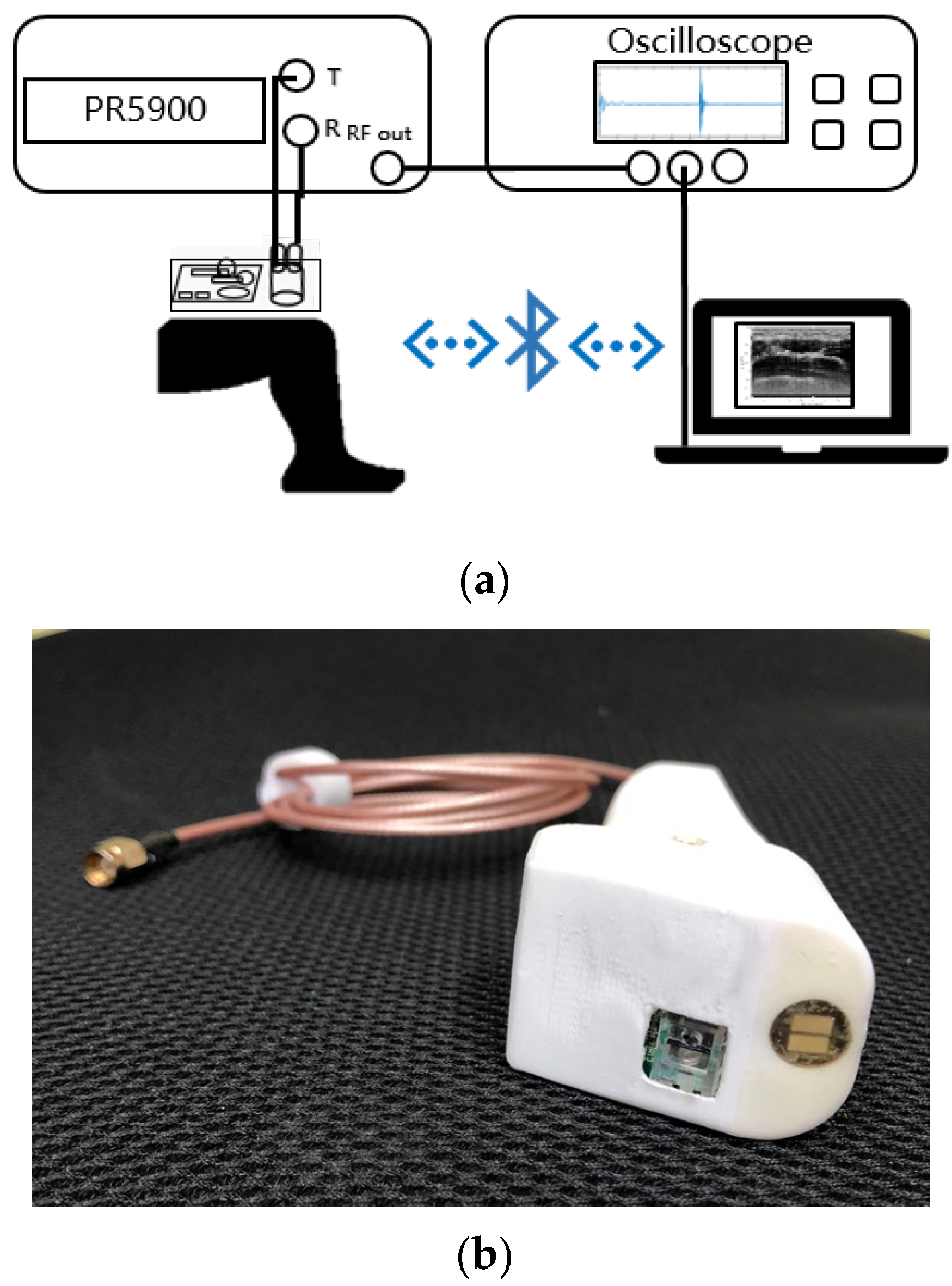
2.3. Measurement System
2.4. Image Processing
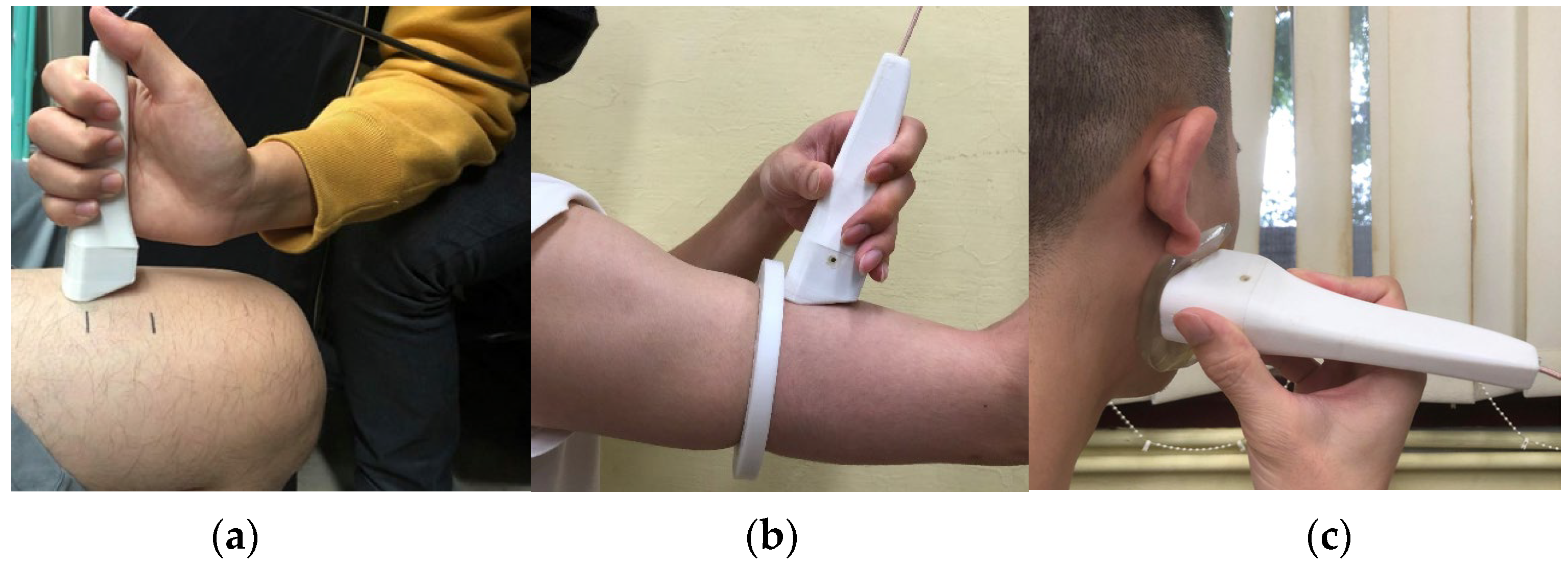
2.5. Ultrasound Scanning
2.6. Comparison of Ultrasound Transducer
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kuhl, C.K.; Schrading, S.; Leutner, C.C.; Morakkabati-Spitz, N.; Wardelmann, E.; Fimmers, R.; Kuhn, W.; Schild, H.H. Mammography, breast ultrasound, and magnetic resonance imaging for surveillance of women at high familial risk for breast cancer. J. Clin. Oncol. 2005, 23, 8469–8476. [Google Scholar] [CrossRef]
- Branney, S.W.; Moore, E.E.; Cantrill, S.V.; Burch, J.M.; Terry, S.J. Ultrasound based key clinical pathway reduces the use of hospital resources for the evaluation of blunt abdominal trauma. J. Trauma Acute Care Surg. 1997, 42, 1086–1090. [Google Scholar] [CrossRef] [PubMed]
- Sengupta, P.P.; Krishnamoorthy, V.K.; Korinek, J.; Narula, J.; Vannan, M.A.; Lester, S.J.; Tajik, J.A.; Seward, J.B.; Khandheria, B.K.; Belohlavek, M. Left ventricular form and function revisited: Applied translational science to cardiovascular ultrasound imaging. J. Am. Soc. Echocardiogr. 2007, 20, 539–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Derchi, L.E.; Serafini, G.; Gandolfo, N.; Gandolfo, N.G.; Martinoli, C. Ultrasound in gynecology. Eur. Radiol. 2001, 11, 2137–2155. [Google Scholar] [CrossRef] [PubMed]
- Pillen, S.; van Alfen, N. Skeletal muscle ultrasound. Neurol. Res. 2011, 33, 1016–1024. [Google Scholar] [CrossRef] [Green Version]
- Bedi, D.G.; Gombos, D.S.; Ng, C.S.; Singh, S. Sonography of the eye. Am. J. Roentgenol. 2006, 187, 1061–1072. [Google Scholar] [CrossRef]
- Garcìa-Garcìa, H.M.; Gogas, B.D.; Serruys, P.W.; Bruining, N. IVUS-based imaging modalities for tissue characterization: Similarities and differences. Int. J. Cardiovasc. Imaging 2011, 27, 215–224. [Google Scholar] [CrossRef] [Green Version]
- Rohr, A.S.; Spector, S.L.; Siegel, S.C.; Katz, R.M.; Rachelefsky, G.S. Correlation between A-mode ultrasound and radiography in the diagnosis of maxillary sinusitis. J. Allergy Clin. Immunol. 1986, 78, 58–61. [Google Scholar] [CrossRef]
- Qiu, W.; Yu, Y.; Tsang, F.K.; Sun, L. An FPGA-based open platform for ultrasound biomicroscopy. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2012, 59, 1432–1442. [Google Scholar]
- Bok, T.-H.; Paeng, D.-G. High Frequency Ultrasound and Its Applications to Animal and Human Imaging Focusing on Vessel and Blood. J. Acoust. Soc. Korea 2010, 29, 73–85. [Google Scholar]
- Vogt, M.; Ermert, H. Limited-angle spatial compound imaging of skin with high-frequency ultrasound (20 MHz). IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2008, 55, 1975–1983. [Google Scholar] [CrossRef]
- Tiouririne, M.; Nguyen, S.; Hossack, J.A.; Owen, K.; William Mauldin, F., Jr. Handheld real-time volumetric imaging of the spine: Technology development. J. Med. Eng. Technol. 2014, 38, 100–103. [Google Scholar] [CrossRef] [Green Version]
- Choi, S.; Kim, J.Y.; Lim, H.G.; Baik, J.W.; Kim, H.H.; Kim, C. Versatile single-element ultrasound imaging platform using a water-proofed MEMS scanner for animals and humans. Sci. Rep. 2020, 10, 6544. [Google Scholar] [CrossRef] [Green Version]
- Falkowski, A.L.; Jacobson, J.A.; Freehill, M.T.; Kalia, V. Hand-held portable versus conventional cart-based ultrasound in musculoskeletal imaging. Orthop. J. Sport. Med. 2020, 8, 2325967119901017. [Google Scholar] [CrossRef] [Green Version]
- Kuniyil Ajith Singh, M.; Steenbergen, W.; Manohar, S. Handheld probe-based dual mode ultrasound/photoacoustics for biomedical imaging. In Frontiers in Biophotonics for Translational Medicine; Springer: Berlin/Heidelberg, Germany, 2016; pp. 209–247. [Google Scholar]
- Daoud, M.I.; Alshalalfah, A.-L.; Awwad, F.; Al-Najar, M. Freehand 3D Ultrasound Imaging System Using Electromagnetic Tracking. IEEE: New York, NY, USA, 2015; pp. 1–5. [Google Scholar]
- Lang, A.; Mousavi, P.; Fichtinger, G.; Abolmaesumi, P. Fusion of electromagnetic tracking with speckle-tracked 3D freehand ultrasound using an unscented Kalman filter. In Medical Imaging 2009: Ultrasonic Imaging and Signal Processing; SPIE: Bellingham, DC, USA, 2009; pp. 399–410. [Google Scholar]
- Lee, C.; Choi, W.; Kim, J.; Kim, C. Three-dimensional clinical handheld photoacoustic/ultrasound scanner. Photoacoustics 2020, 18, 100173. [Google Scholar] [CrossRef]
- Huang, Q.; Lan, J.; Li, X. Robotic arm based automatic ultrasound scanning for three-dimensional imaging. IEEE Trans. Ind. Inform. 2018, 15, 1173–1182. [Google Scholar] [CrossRef]
- Swerdlow, D.R.; Cleary, K.; Wilson, E.; Azizi-Koutenaei, B.; Monfaredi, R. Robotic arm–assisted sonography: Review of technical developments and potential clinical applications. Am. J. Roentgenol. 2017, 208, 733–738. [Google Scholar] [CrossRef]
- Zhang, W.-T.; Lin, Y.-C.; Chen, W.-H.; Yang, C.-W.; Chiang, H.-H.K. A Free-Hand System of the High-Frequency Single Element Ultrasound Transducer for Skin Imaging; Springer: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- Blackall, J.M.; Rueckert, D.; Maurer, C.R.; Penney, G.P.; Hill, D.L.G.; Hawkes, D.J. An Image Registration Approach to Automated Calibration for Freehand 3D Ultrasound; Springer: Berlin/Heidelberg, Germany, 2000. [Google Scholar]
- Fry, N.R.; Gough, M.; Shortland, A.P. Three-dimensional realisation of muscle morphology and architecture using ultrasound. Gait Posture 2004, 20, 177–182. [Google Scholar] [CrossRef]
- Sato, Y.; Nakamoto, M.; Tamaki, Y.; Sasama, T.; Sakita, I.; Nakajima, Y.; Monden, M.; Tamura, S. Image guidance of breast cancer surgery using 3-D ultrasound images and augmented reality visualization. IEEE Trans. Med. Imaging 1998, 17, 681–693. [Google Scholar] [CrossRef]
- Leahy, S.; Toomey, C.; McCreesh, K.; O’Neill, C.; Jakeman, P. Ultrasound measurement of subcutaneous adipose tissue thickness accurately predicts total and segmental body fat of young adults. Ultrasound Med. Biol. 2012, 38, 28–34. [Google Scholar] [CrossRef]
- Hida, T.; Ando, K.; Kobayashi, K.; Ito, K.; Tsushima, M.; Kobayakawa, T.; Morozumi, M.; Tanaka, S.; Machino, M.; Ota, K. Ultrasound measurement of thigh muscle thickness for assessment of sarcopenia. Nagoya J. Med. Sci. 2018, 80, 519. [Google Scholar] [PubMed]
- Abe, T.; Fujita, E.; Thiebaud, R.S.; Loenneke, J.P.; Akamine, T. Ultrasound-derived forearm muscle thickness is a powerful predictor for estimating DXA-derived appendicular lean mass in Japanese older adults. Ultrasound Med. Biol. 2016, 42, 2341–2344. [Google Scholar] [CrossRef]
- Souza, V.A.D.; Oliveira, D.; Cupolilo, E.N.; Miranda, C.S.; Colugnati, F.A.B.; Mansur, H.N.; Fernandes, N.M.D.S.; Bastos, M.G. Rectus femoris muscle mass evaluation by ultrasound: Facilitating sarcopenia diagnosis in pre-dialysis chronic kidney disease stages. Clinics 2018, 73, e392. [Google Scholar] [CrossRef] [PubMed]
- Strasser, E.M.; Draskovits, T.; Praschak, M.; Quittan, M.; Graf, A. Association between ultrasound measurements of muscle thickness, pennation angle, echogenicity and skeletal muscle strength in the elderly. Age 2013, 35, 2377–2388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, G.; Bonmati, E.; Thompson, S.; Evans, J.; Hipwell, J.; Nikitichev, D.; Gurusamy, K.; Ourselin, S.; Hawkes, D.J.; Davidson, B. Electromagnetic tracking in image-guided laparoscopic surgery: Comparison with optical tracking and feasibility study of a combined laparoscope and laparoscopic ultrasound system. Med. Phys. 2018, 45, 5094–5104. [Google Scholar] [CrossRef]
- Peters, T.; Cleary, K. Image-Guided Interventions: Technology and Applications; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2008. [Google Scholar]
- Zhao, X.; Gang, T.; Xu, C. Prediction of side-drilled hole signals captured by a dual crystal contact probe. J. Nondestruct. Eval. 2010, 29, 105–110. [Google Scholar] [CrossRef]












Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-L.; Chiang, H.K. Development of Single-Channel Dual-Element Custom-Made Ultrasound Scanner with Miniature Optical Position Tracker for Freehand Imaging. Biosensors 2023, 13, 431. https://doi.org/10.3390/bios13040431
Chen Y-L, Chiang HK. Development of Single-Channel Dual-Element Custom-Made Ultrasound Scanner with Miniature Optical Position Tracker for Freehand Imaging. Biosensors. 2023; 13(4):431. https://doi.org/10.3390/bios13040431
Chicago/Turabian StyleChen, Yen-Lung, and Huihua Kenny Chiang. 2023. "Development of Single-Channel Dual-Element Custom-Made Ultrasound Scanner with Miniature Optical Position Tracker for Freehand Imaging" Biosensors 13, no. 4: 431. https://doi.org/10.3390/bios13040431
APA StyleChen, Y. -L., & Chiang, H. K. (2023). Development of Single-Channel Dual-Element Custom-Made Ultrasound Scanner with Miniature Optical Position Tracker for Freehand Imaging. Biosensors, 13(4), 431. https://doi.org/10.3390/bios13040431