
Infection Control for a Carbapenem-Resistant Enterobacteriaceae Outbreak in an Advanced Emergency Medical Services Center

 , ,
, ,
Abstract
:1. Introduction
2. Results
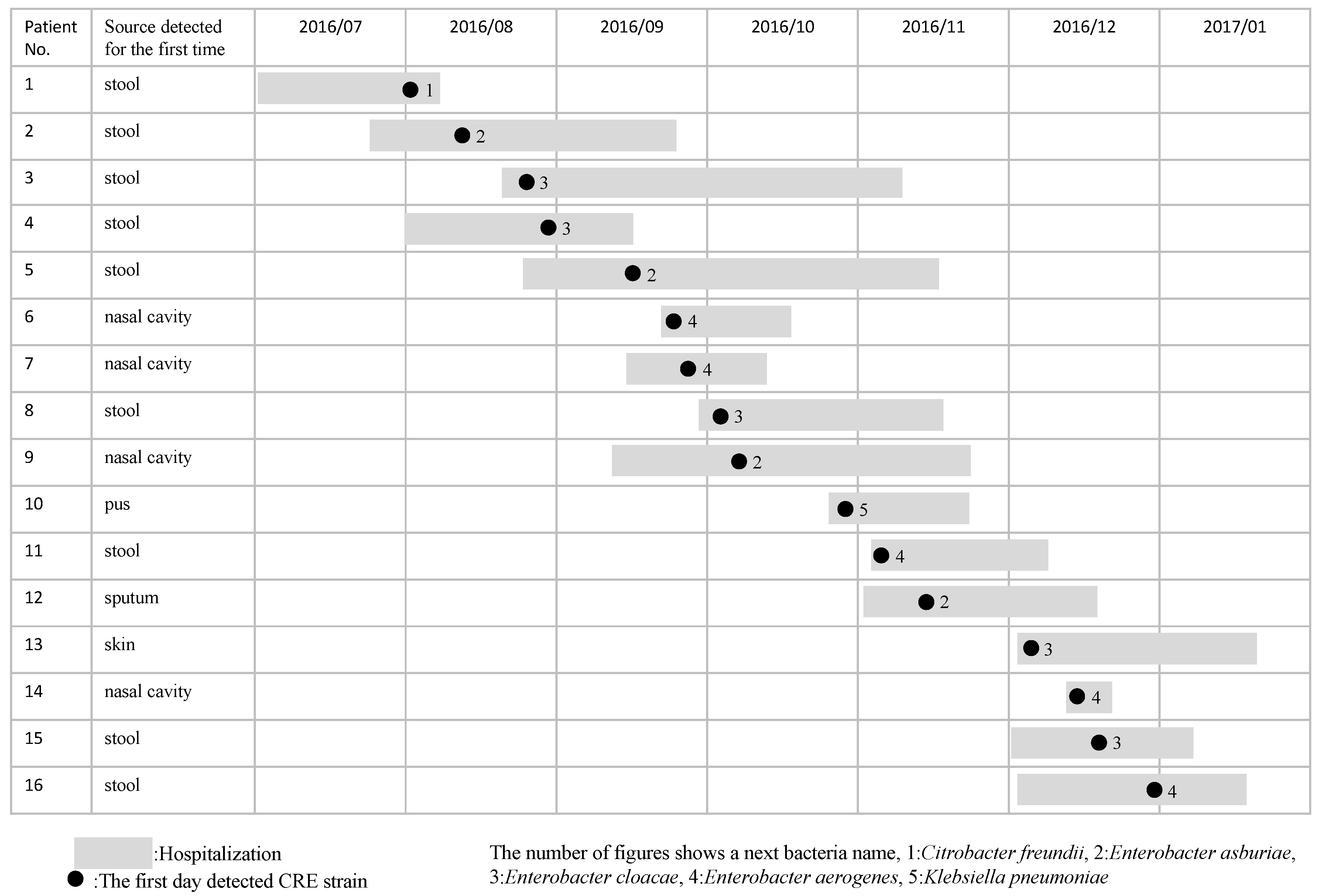
2.1. Bacterial Strains and Patient Characteristics
2.2. MIC
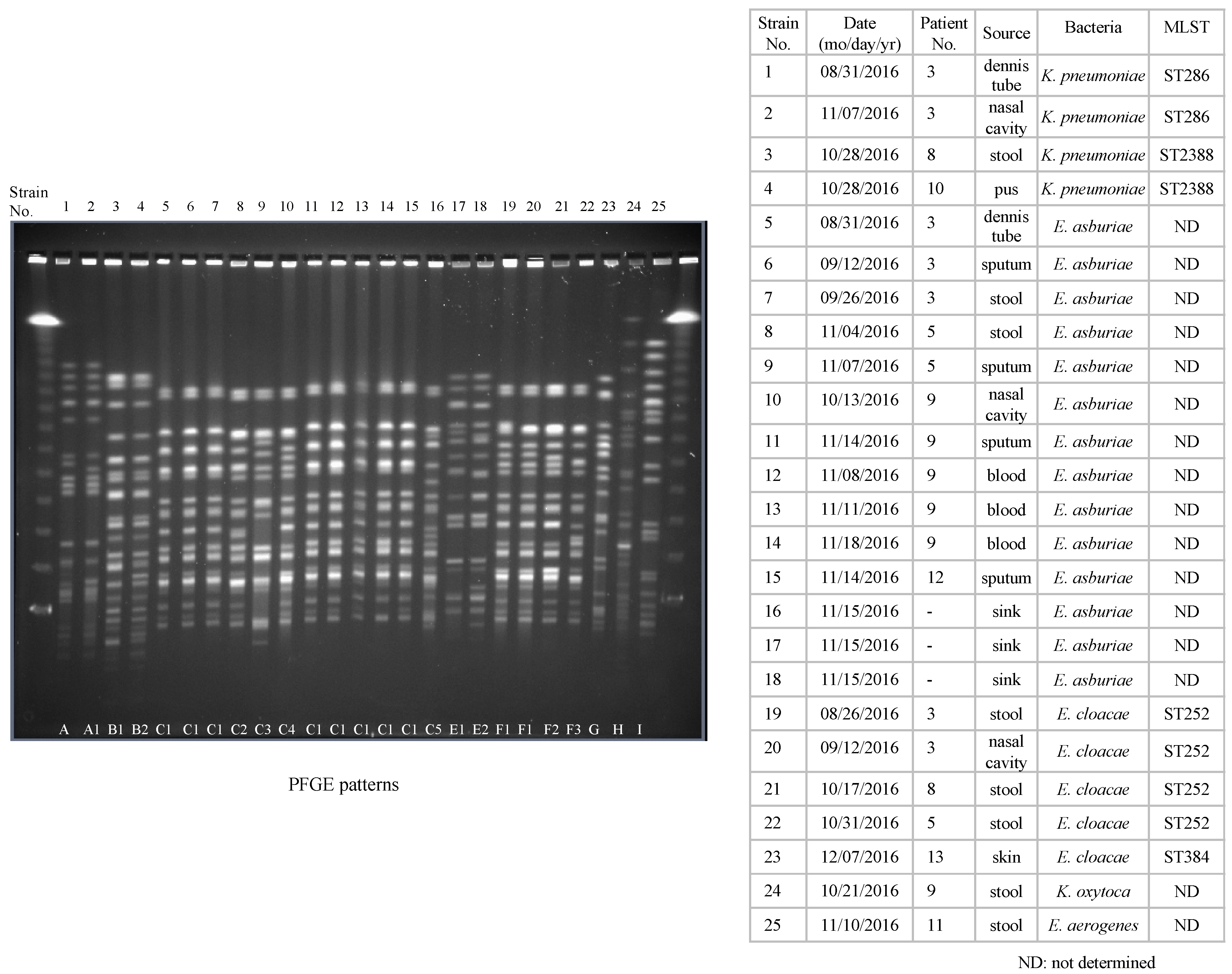
2.3. Interpretation of Molecular Typing by PFGE and MLST Analysis
2.4. Distribution of β-Lactamase Genes
2.5. Intervention by the ICT
3. Discussion
4. Methods
4.1. Ethical Approval
4.2. Setting and Outbreak Description
4.3. Bacterial Strains and Patients
4.4. Identification Test and Minimum Inhibitory Concentration
4.5. Pulsed-Field Gel Electrophoresis
4.6. Multilocus Sequence Typing
4.7. Detection of β-Lactamase Genes
4.8. Plasmid Incompatibility Typing
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Nordmann, P.; Naas, T.; Poirel, L. Global spread of carbapenemase producing Enterobacteriaceae. Emerg. Infect. Dis. 2011, 17, 1791–1798. [Google Scholar] [CrossRef] [PubMed]
- Logan, L.K.; Weinstein, R.A. The epidemiology of carbapenem-resistant Enterobacteriaceae: The impact and evolution of a global menace. J. Infect. Dis. 2017, 215 (Suppl. S1), S28–S36. [Google Scholar] [CrossRef] [Green Version]
- Ishii, Y.; Aoki, K.; Tateda, K.; Kiyota, H. Multicenter collaboration study on the ß-lactam resistant Enterobacteriaceae in Japan—The 65th anniversary public interest purpose project of the Japanese Society of Chemotherapy. J. Infect. Chemother. 2017, 23, 583–586. [Google Scholar] [CrossRef] [Green Version]
- Guh, A.Y.; Bulens, S.N.; Mu, Y.; Jacob, J.T.; Reno, J.; Scott, J.; Wilson, L.E.; Vaeth, E.; Lynfield, R.; Shaw, K.M.; et al. Epidemiology of carbapenem-resistant Enterobacteriaceae in 7 US communities, 2012–2013. JAMA 2015, 314, 1479–1487. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, Q.; Yin, Y.; Chen, H.; Jin, L.; Gu, B.; Xie, L.; Yang, C.; Ma, X.; Li, H.; et al. Epidemiology of carbapenem-resistant Enterobacteriaceae infections: Report from the China CRE network. Antimicrob. Agents Chemother. 2018, 62, e01882-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kizny Gordon, A.E.; Mathers, A.J.; Cheong, E.Y.; Gottlieb, T.; Kotay, S.; Walker, A.S.; Peto, T.E.; Crook, D.W.; Stoesser, N. The hospital water environment as a reservoir for carbapenem-resistant organisms causing hospital-acquired infections-a systematic review of the literature. Clin. Infect. Dis. 2017, 64, 1435–1444. [Google Scholar] [CrossRef] [PubMed]
- Jacob, J.T.; Klein, E.; Laxminarayan, R.; Beldavs, Z.; Lynfield, R.; Kallen, A.J.; Ricks, P.; Edwards, J.; Srinivasan, A.; Fridkin, S.; et al. Centers for Disease Control and Prevention (CDC). Vital signs: Carbapenem-resistant Enterobacteriaceae. Morb. Mortal. Wkly. Rep. 2013, 62, 165–170. [Google Scholar]
- Friedman, N.D.; Carmeli, Y.; Walton, A.L.; Schwaber, M.J. Carbapenem-resistant Enterobacteriaceae: A strategic roadmap for infection control. Infect. Control Hosp. Epidemiol. 2017, 38, 580–594. [Google Scholar] [CrossRef] [Green Version]
- Sheu, C.C.; Chang, Y.T.; Lin, S.Y.; Chen, Y.H.; Hsueh, P.R. Infections caused by carbapenem-resistant Enterobacteriaceae: An update on therapeutic options. Front. Microbiol. 2019, 10, 80. [Google Scholar] [CrossRef] [Green Version]
- Malchione, M.D.; Torres, L.M.; Hartley, D.M.; Koch, M.; Goodman, J.L. Carbapenem and colistin resistance in Enterobacteriaceae in southeast Asia: Review and mapping of emerging and overlapping challenges. Int. J. Antimicrob. Agents 2019, 54, 381–399. [Google Scholar] [CrossRef] [PubMed]
- Jayol, A.; Poirel, L.; Dortet, L.; Nordmann, P. National survey of colistin resistance among carbapenemase-producing Enterobacteriaceae and outbreak caused by colistin-resistant OXA-48-producing Klebsiella pneumoniae, France, 2014. Eurosurveillance 2016, 21, 30339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peck, K.R.; Kim, M.J.; Choi, J.Y.; Kim, H.S.; Kang, C.-I.; Cho, Y.K.; Park, D.W.; Lee, H.J.; Lee, M.S.; Ko, K.S. In vitro time-kill studies of antimicrobial agents against blood isolates of imipenem-resistant Acinetobacter baumannii, including colistin-or tigecycline-resistant isolates. J. Med. Microbiol. 2012, 61, 353–360. [Google Scholar] [CrossRef]
- Gonçalves, I.R.; Ferreira, M.; Araujo, B.; Campos, P.; Royer, S.; Batistão, D.; Souza, L.; Brito, C.; Urzedo, J.; Gontijo-Filho, P.; et al. Outbreaks of colistin-resistant and colistin-susceptible KPC-producing Klebsiella pneumoniae in a Brazilian intensive care unit. J. Hosp. Infect. 2016, 94, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Robert, F.P.; Alaric, W.D.; Gautam, D. The rapid spread of carbapenem-resistant Enterobacteriaceae. Drug Resist. Updat. 2016, 29, 30–46. [Google Scholar]
- Shields, R.K.; Nguyen, M.H.; Chen, L.; Press, E.G.; Kreiswirth, B.N.; Clancy, C.J. Pneumonia and Renal Replacement Therapy Are Risk Factors for Ceftazidime-Avibactam Treatment Failures and Resistance among Patients with Carbapenem-Resistant Enterobacteriaceae Infections. Antimicrob. Agents Chemother. 2018, 62, e02497-17. [Google Scholar] [CrossRef] [Green Version]
- Ackley, R.; Roshdy, D.; Meredith, J.; Minor, S.; Anderson, W.E.; Capraro, G.A.; Polk, C. Meropenem-Vaborbactam versus Ceftazidime-Avibactam for Treatment of Carbapenem-Resistant Enterobacteriaceae Infections. Antimicrob. Agents Chemother. 2020, 64, e02313-19. [Google Scholar] [CrossRef]
- Hidaka, H.; Miura, M.; Masunaga, K.; Qin, L.; Uemura, Y.; Sakai, Y.; Watanabe, H.; Hashimoto, K.; Kawano, S.; Yamashita, N.; et al. Infection control for a methicillin-resistant Staphylococcus aureus outbreak in an advanced emergency medical service center, as monitored by molecular analysis. J. Infect. Chemother. 2013, 19, 884–890. [Google Scholar] [CrossRef]
- Sakai, Y.; Qin, L.; Miura, M.; Masunaga, K.; Tanamachi, C.; Iwahashi, J.; Kida, Y.; Takasu, O.; Sakamoto, T.; Watanabe, H. Successful infection control for a vancomycin-intermediate Staphylococcus aureus outbreak in an advanced emergency medical service centre. J. Hosp. Infect. 2016, 92, 385–391. [Google Scholar] [CrossRef]
- French, C.E.; Coope, C.; Conway, L.; Higgins, J.P.T.; McCulloch, J.; Okoli, G.; Patel, B.C.; Oliver, I. Control of carbapenemase-producing Enterobacteriaceae outbreaks in acute settings: An evidence review. J. Hosp. Infect. 2017, 95, 3–45. [Google Scholar] [CrossRef] [Green Version]
- Munoz-Price, L.S.; Hayden, M.K.; Lolans, K.; Won, S.; Calvert, K.; Lin, M.; Sterner, A.; Weinstein, R.A. Successful control of an outbreak of Klebsiella pneumoniae carbapenemase-producing K. pneumoniae at a long-term acute care hospital. Infect. Control Hosp. Epidemiol. 2010, 31, 341–347. [Google Scholar] [CrossRef] [Green Version]
- Hussein, K.; Rabino, G.; Eluk, O.; Warman, S.; Reisner, S.; Geffen, Y.; Halif, L.; Paul, M. The association between infection control interventions and carbapenem-resistant Enterobacteriaceae incidence in an endemic hospital. J. Hosp. Infect. 2017, 97, 218–225. [Google Scholar] [CrossRef]
- Friedrich, A.W. Control of hospital acquired infections and antimicrobial resistance in Europe: The way to go. Wien. Med. Wochenschr 2019, 169 (Suppl. S1), 25–30. [Google Scholar] [CrossRef] [Green Version]
- Hopman, J.; Tostmann, A.; Wertheim, H.; Bos, M.; Kolwijck, E.; Akkermans, R.; Sturm, P.; Voss, A.; Pickkers, P. Reduced rate of intensive care unit acquired gram-negative bacilli after removal of sinks and introduction of ‘water-free’ patient care. Antimicrob. Resist. Infect. Control. 2017, 6, 59. [Google Scholar] [CrossRef]
- Shaw, E.; Gavaldà, L.; Càmara, J.; Gasull, R.; Gallego, S.; Tubau, F.; Granada, R.; Ciercoles, P.; Domínguez, M.A.; Manez, R.; et al. Control of endemic multidrug-resistant Gram-negative bacteria after removal of sinks and implementing a new water-safe policy in an intensive care unit. J. Hosp. Infect. 2018, 98, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, N.; Asada, R.; Kawahara, R.; Hagiya, H.; Akeda, Y.; Shanmugakani, R.K.; Yoshida, H.; Yukawa, S.; Yamamoto, K.; Takayama, Y.; et al. Prevalence of, and risk factors for, carriage of carbapenem-resistant Enterobacteriaceae among hospitalized patients in Japan. J. Hosp. Infect. 2017, 97, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Mori, N.; Kagawa, N.; Aoki, K.; Ishi, Y.; Tateda, K.; Aoki, Y. Clinical and molecular analyses of bloodstream infections caused by IMP metallo-β-lactamase-producing Enterobacteriaceae in a tertiary hospital in Japan. J. Infect. Chemother. 2020, 26, 144–147. [Google Scholar] [CrossRef]
- Queenan, A.M.; Bush, K. Carbapenemases: The versatile beta-lactamases. Clin. Microbiol. Rev. 2007, 20, 440–458. [Google Scholar] [CrossRef] [Green Version]
- Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing; Twenty-Second Informational Supplement; CLSI document M100-S22; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2012. [Google Scholar]
- Ribot, E.M.; Fair, M.A.; Gautom, R.; Cameron, D.N.; Hunter, S.B.; Swaminathan, B.; Barrett, T.J. Standardization of pulsed-field gel electrophoresis protocols for the subtyping of Escherichia coli O157:H7, Salmonella, and Shigella for PulseNet. Foodborne Pathog. Dis. 2006, 3, 59–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tenover, F.C.; Arbeit, R.D.; Goering, R.V.; Mickelsen, P.A.; Murray, B.; Persing, D.H.E.; Swaminathan, B. Interpreting chromosomal DNA restriction patterns produced by pulsed-field gel electrophoresis: Criteria for bacterial strain typing. J. Clin. Microbiol. 1995, 33, 2233–2239. [Google Scholar] [CrossRef] [Green Version]
- van der Zwaluw, K.; de Haan, A.; Pluister, G.N.; Bootsma, H.J.; de Neeling, A.J.; Schouls, L.M. The carbapenem inactivation method (CIM), a simple and low-cost alternative for the Carba NP test to assess phenotypic carbapenemase activity in gram-negative rods. PLoS ONE 2015, 10, e0123690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poirel, L.; Walsh, T.R.; Cuvillier, V.; Nordmann, P. Multiplex PCR for detection of acquired carbapenemase genes. Diagn. Microbiol. Infect. Dis. 2011, 70, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Dallenne, C.; Da Costa, A.; Decré, D.; Favier, C.; Arlet, G. Development of a set of multiplex PCR assays for the detection of genes encoding important β-lactamases in Enterobacteriaceae. J. Antimicrob. Chemother. 2010, 65, 490–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carattoli, A.; Bertini, A.; Villa, L.; Falbo, V.; Hopkins, K.L.; Threlfall, E.J. Identification of plasmids by PCR-based replicon typing. J. Microbiol. Methods 2005, 63, 219–228. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patient No. | ABPC | PIPC | CTX | CAZ | CFPM | CMZ | IPM | MEPM | AZT | ABPC/SBT | PIPC/TAZ | GM | AMK | MINO | LVFX | ST |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | >16 | <8 | >2 | >8 | 4 | >32 | 2 | >2 | <4 | >16 | <16 | 4 | <4 | 4 | 2 | <2 |
| 2 | >16 | >64 | >2 | >8 | >16 | >32 | >2 | >2 | <4 | >16 | 64 | >8 | <4 | 4 | 1 | <2 |
| 3 | >16 | >64 | >2 | >8 | >16 | >32 | >2 | >2 | <4 | >16 | >64 | >8 | <4 | 4 | 1 | <2 |
| 4 | >16 | <8 | <1 | <4 | <2 | >32 | 2 | <1 | <4 | 16 | <16 | <2 | <4 | 4 | <0.5 | <2 |
| 5 | >16 | >64 | >2 | >8 | >16 | >32 | >2 | >2 | >8 | >16 | >64 | 8 | <4 | <2 | <0.5 | <2 |
| 6 | <8 | <8 | <1 | <4 | <2 | >32 | 2 | <1 | <4 | <8 | <16 | <2 | <4 | <2 | <0.5 | <2 |
| 7 | >16 | <8 | <1 | <4 | <2 | >32 | 2 | <1 | <4 | 16 | <16 | <2 | <4 | <2 | <0.5 | <2 |
| 8 | >16 | >64 | >2 | >8 | >16 | >32 | >2 | >2 | >8 | >16 | >64 | >8 | <4 | >8 | 4 | <2 |
| 9 | >16 | >64 | >2 | >8 | >16 | >32 | >2 | >2 | <4 | >16 | 64 | >8 | <4 | >8 | 4 | >2 |
| 10 | >16 | 16 | >2 | >8 | >16 | >32 | 2 | >2 | <4 | >16 | <16 | 8 | <4 | 4 | 4 | >2 |
| 11 | >16 | <8 | <1 | <4 | <2 | >32 | 2 | <1 | <4 | 16 | <16 | <2 | <4 | <2 | <0.5 | <2 |
| 12 | >16 | <8 | >2 | >8 | 4 | >32 | >2 | >2 | <4 | >16 | <16 | >8 | <4 | <2 | 1 | <2 |
| 13 | >16 | <8 | 2 | <4 | <2 | >32 | 2 | <1 | <4 | >16 | <16 | <2 | <4 | 4 | <0.5 | <2 |
| 14 | >16 | <8 | <1 | <4 | <2 | >32 | 2 | <1 | <4 | 16 | <16 | <2 | <4 | <2 | <0.5 | <2 |
| 15 | >16 | <8 | >2 | <4 | <2 | >32 | 2 | <1 | <4 | >16 | <16 | <2 | <4 | <2 | <0.5 | <2 |
| 16 | >16 | <8 | <1 | <4 | <2 | >32 | 2 | <1 | <4 | 16 | <16 | <2 | <4 | <2 | <0.5 | <2 |
| Strain No. | Carbapenemase | CTX-M | ESBL | CIM | Inc |
|---|---|---|---|---|---|
| 1 | IMP-1 | ND | SHV | + | FIIA |
| 2 | IMP-1 | ND | SHV | + | FIIA |
| 3 | IMP-1 | ND | SHV | + | N |
| 4 | IMP-1 | ND | SHV | + | N |
| 5 | IMP-1 | ND | ND | + | FIIA |
| 6 | IMP-1 | ND | TEM, SHV | + | FIIA |
| 7 | IMP-1 | ND | TEM, SHV | + | FIIA |
| 8 | IMP-1 | ND | ND | + | FIIA |
| 9 | IMP-1 | ND | SHV | + | ND |
| 10 | IMP-1 | ND | TEM, SHV | + | FIIA |
| 11 | IMP-1 | ND | ND | + | FIIA |
| 12 | IMP-1 | ND | ND | + | FIIA |
| 13 | IMP-1 | ND | ND | + | FIIA |
| 14 | IMP-1 | ND | ND | + | FIIA |
| 15 | IMP-1 | ND | ND | + | FIIA |
| 16 | IMP-1 | ND | ND | + | FIIA |
| 17 | IMP-1 | ND | ND | + | ND |
| 18 | IMP-1 | ND | ND | + | ND |
| 19 | IMP-1 | ND | TEM, SHV | + | ND |
| 20 | IMP-1 | ND | TEM | + | ND |
| 21 | IMP-1 | ND | TEM, SHV | + | FIIA |
| 22 | IMP-1 | ND | TEM, SHV | + | FIIA |
| 23 | ND | ND | ND | - | ND |
| 24 | IMP-1 | ND | TEM | + | ND |
| 25 | ND | ND | ND | - | FIIA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sakai, Y.; Gotoh, K.; Nakano, R.; Iwahashi, J.; Miura, M.; Horita, R.; Miyamoto, N.; Yano, H.; Kannae, M.; Takasu, O.; et al. Infection Control for a Carbapenem-Resistant Enterobacteriaceae Outbreak in an Advanced Emergency Medical Services Center. Antibiotics 2021, 10, 1537. https://doi.org/10.3390/antibiotics10121537
Sakai Y, Gotoh K, Nakano R, Iwahashi J, Miura M, Horita R, Miyamoto N, Yano H, Kannae M, Takasu O, et al. Infection Control for a Carbapenem-Resistant Enterobacteriaceae Outbreak in an Advanced Emergency Medical Services Center. Antibiotics. 2021; 10(12):1537. https://doi.org/10.3390/antibiotics10121537
Chicago/Turabian StyleSakai, Yoshiro, Kenji Gotoh, Ryuichi Nakano, Jun Iwahashi, Miho Miura, Rie Horita, Naoki Miyamoto, Hisakazu Yano, Mikinori Kannae, Osamu Takasu, and et al. 2021. "Infection Control for a Carbapenem-Resistant Enterobacteriaceae Outbreak in an Advanced Emergency Medical Services Center" Antibiotics 10, no. 12: 1537. https://doi.org/10.3390/antibiotics10121537
APA StyleSakai, Y., Gotoh, K., Nakano, R., Iwahashi, J., Miura, M., Horita, R., Miyamoto, N., Yano, H., Kannae, M., Takasu, O., & Watanabe, H. (2021). Infection Control for a Carbapenem-Resistant Enterobacteriaceae Outbreak in an Advanced Emergency Medical Services Center. Antibiotics, 10(12), 1537. https://doi.org/10.3390/antibiotics10121537