
Comparative Effectiveness of Treatments for Bacterial Vaginosis: A Network Meta-Analysis


Abstract
:1. Introduction
2. Results
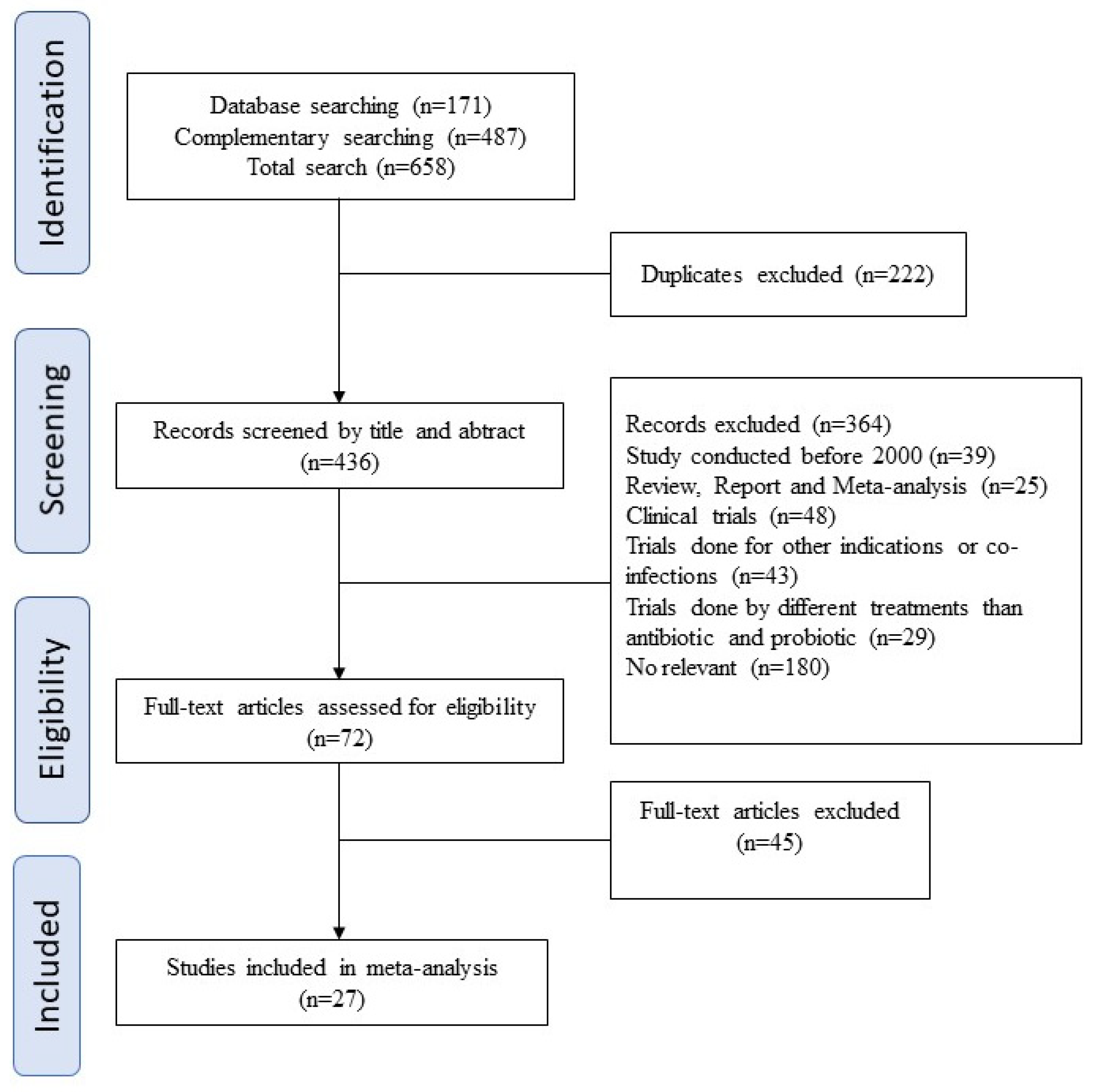
2.1. Study Inclusion Criteria and Characteristics of the Eligible Studies
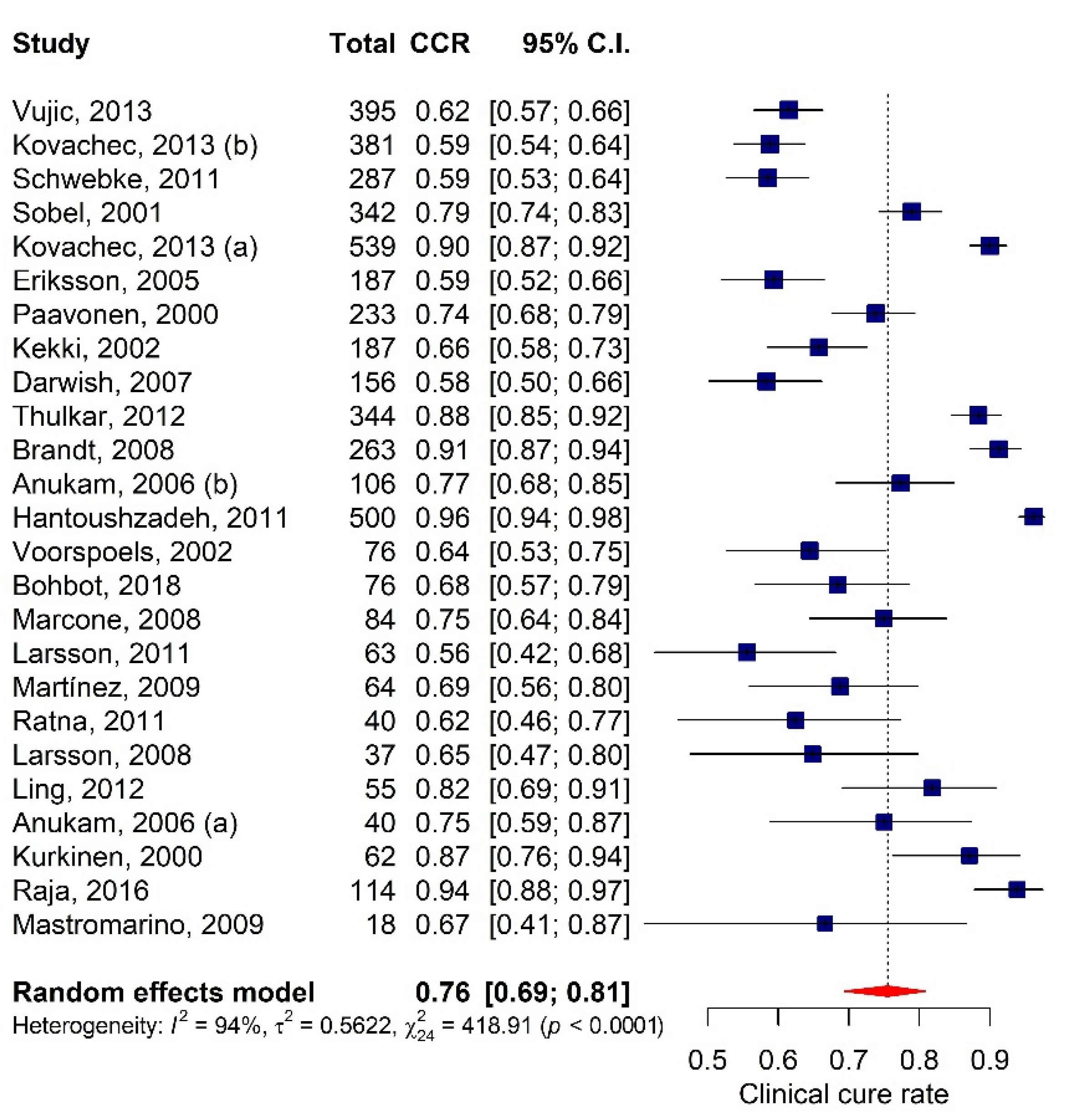
2.2. The Overall Efficiency of Bacterial Vaginosis Treatments
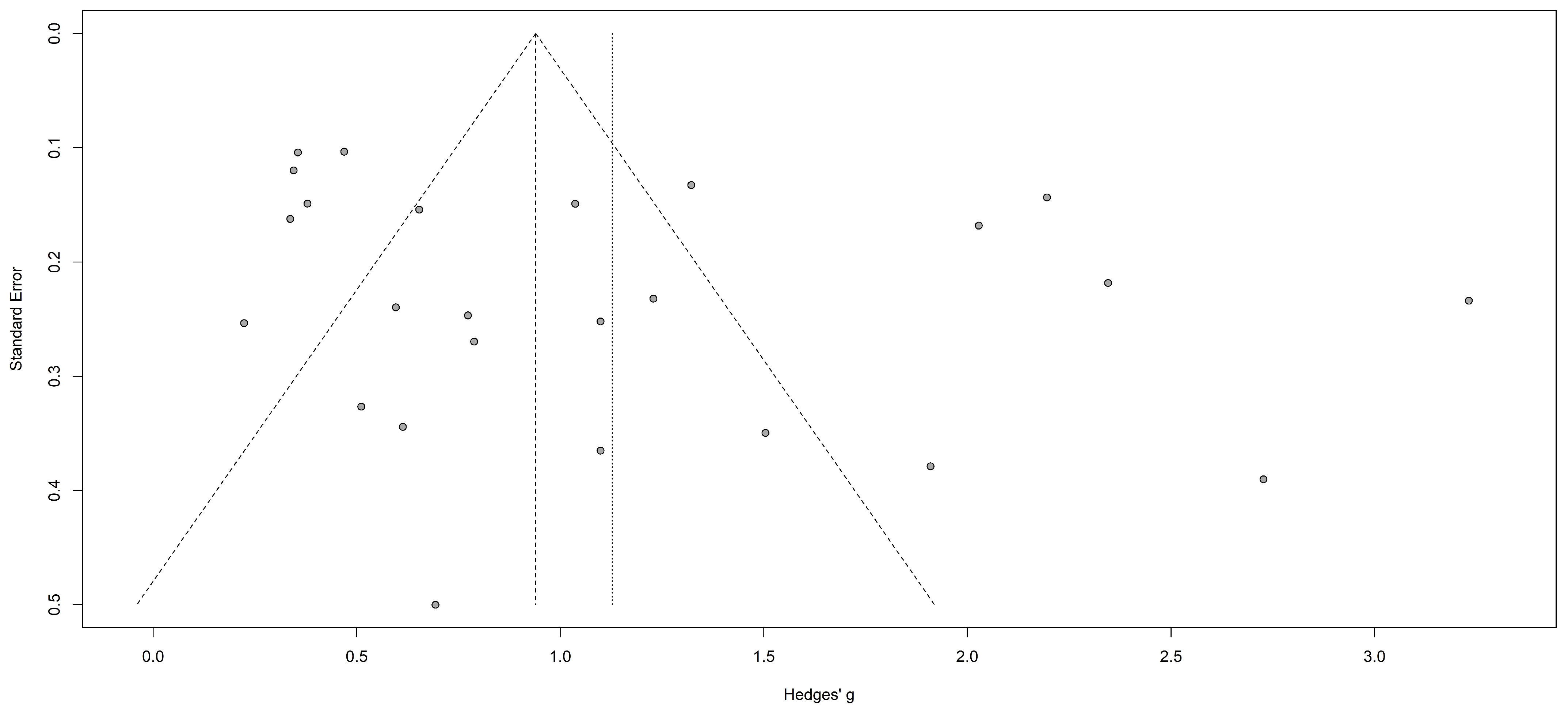
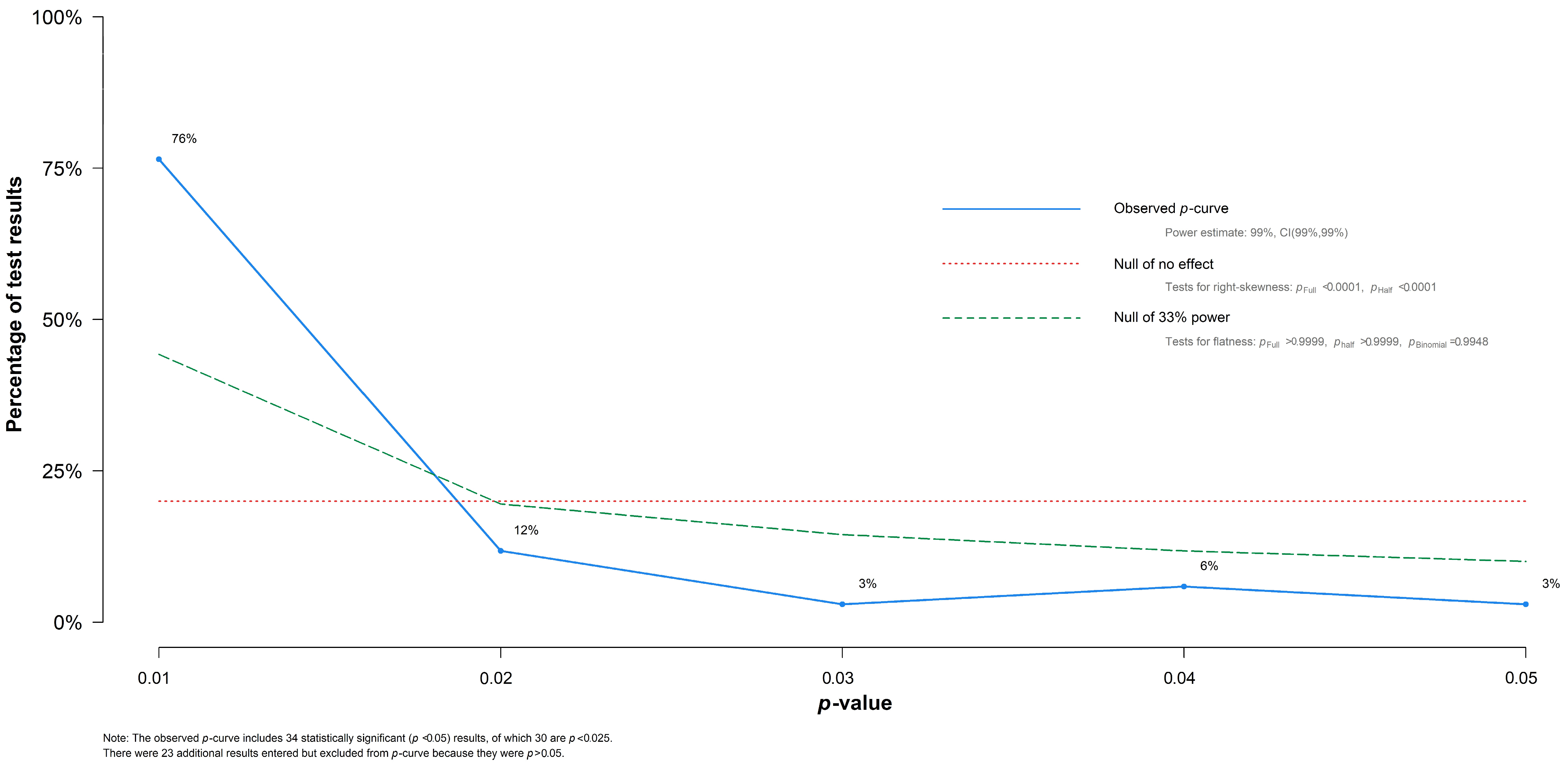
2.3. P-Curve Analysis and Detection of P-Hacking
2.4. Effectiveness of BV Treatment Types, Administration Routes, and Pregnancy State
Network Analysis
2.5. Evaluation of Probiotic Therapy in BV Treatment
2.6. The Geographical Disparity in CCR among BV Treatments
3. Discussion
3.1. Effectiveness of BV Treatments among Women
3.2. Characterization of the Lactobacilli Species in Probiotic Therapies
3.3. The Geographical Disparity in CCR among BV Treatments
4. Materials and Methods
4.1. Data Selection, Search Strategy, and Study Guidelines
4.2. Screening Process
4.3. Eligibility Criteria
4.4. Data Extraction and Quality Assessment
4.5. Data Analysis and Statistical Methods
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Romero, D.; Andreu, A. Vaginosis bacteriana. Enferm. Infecc. Microbiol. Clin. 2016, 34, 14–18. [Google Scholar] [CrossRef]
- Sobel, J. Bacterial vaginosis. Annu. Rev. Med. 2000, 51, 349–356. [Google Scholar] [CrossRef]
- Tamrakar, R.; Yamada, T.; Furuta, I.; Cho, K.; Morikawa, M.; Yamada, H.; Sakuragi, N.; Minakami, H. Association between Lactobacillus species and bacterial vaginosis-related bacteria, and bacterial vaginosis scores in pregnant Japanese women. BMC Infect. Dis. 2007, 7, 128. [Google Scholar] [CrossRef] [Green Version]
- Jones, A. Bacterial Vaginosis: A Review of Treatment, Recurrence, and Disparities. J. Nurse Pract. 2019, 15, 420–423. [Google Scholar] [CrossRef] [Green Version]
- Kumar, N.; Behera, B.; Sagiri, S.S.; Pal, K.; Ray, S.S.; Roy, S. Bacterial vaginosis: Etiology and modalities of treatment-A brief note. J. Pharm. Bioallied Sci. 2011, 3, 496–503. [Google Scholar] [CrossRef]
- Woodman, Z. Can one size fit all? Approach to bacterial vaginosis in sub-Saharan Africa. Ann. Clin. Microbiol. Antimicrob. 2016, 15, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrova, M.I.; Lievens, E.; Malik, S.; Imholz, N.; Lebeer, S. Lactobacillus species as biomarkers and agents that can promote various aspects of vaginal health. Front. Physiol. 2015, 6, 1–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borgdorff, H.; van der Veer, C.; van Houdt, R.; Alberts, C.J.; de Vries, H.J.; Bruisten, S.M.; Snijder, M.B.; Prins, M.; Geerlings, S.E.; van der Loeff, M.F.S.; et al. The association between ethnicity and vaginal microbiota composition in Amsterdam, The Netherlands. PLoS ONE 2017, 12, e0181135. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.M.; Chang, T.H.; Lin, F.M.; Liang, C.; Chiu, C.M.; Yang, T.L.; Yang, T.; Huang, C.Y.; Cheng, Y.N.; Chang, Y.A.; et al. Vaginal microbiome variances in sample groups categorized by clinical criteria of bacterial vaginosis. BMC Genom. 2018, 19, 876. [Google Scholar] [CrossRef] [PubMed]
- Foessleitner, P.; Kiss, H.; Deinsberger, J.; Ott, J.; Zierhut, L.; Rosta, K.; Falcone, V.; Farr, A. Screening Pregnant Women for Bacterial Vaginosis Using a Point-of-Care Test: A Prospective Validation Study. J. Clin. Med. 2021, 10, 2275. [Google Scholar] [CrossRef]
- Joseph, R.J.; Ser, H.-L.; Kuai, Y.-H.; Tan, L.T.-H.; Arasoo, V.J.T.; Letchumanan, V.; Wang, L.; Pusparajah, P.; Goh, B.-H.; Ab Mutalib, N.-S.; et al. Finding a Balance in the Vaginal Microbiome: How Do We Treat and Prevent the Occurrence of Bacterial Vaginosis? Antibiotics 2021, 10, 719. [Google Scholar] [CrossRef] [PubMed]
- Hainer, B.L.; Gibson, M.V. Vaginitis: Diagnosis and treatment. Am. Fam. Physician 2011, 83, 807–815. [Google Scholar] [CrossRef]
- Amsel, R.; Totten, P.A.; Spiegel, C.A.; Chen, K.C.S.; Eschenbach, D.; Holmes, K.K. Nonspecific vaginitis. Diagnostic criteria and microbial and epidemiologic associations. Am. J. Med. 1983, 74, 14–22. [Google Scholar] [CrossRef]
- Donders, G.G.; Zodzika, J.; Rezeberga, D. Treatment of bacterial vaginosis: What we have and what we miss. Expert Opin. Pharmacother. 2014, 15, 645–657. [Google Scholar] [CrossRef] [PubMed]
- Van de Wijgert, J.H.H.M.; Borgdorff, H.; Verhelst, R.; Crucitti, T.; Francis, S.; Verstraelen, H.; Jespers, V. The vaginal microbiota: What have we learned after a decade of molecular characterization? PLoS ONE 2014, 9, e105998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beigi, R.H.; Austin, M.N.; Meyn, L.A.; Krohn, M.A.; Hillier, S.L. Antimicrobial resistance associated with the treatment of bacterial vaginosis. Am. J. Obstet. Gynecol. 2004, 191, 1124–1129. [Google Scholar] [CrossRef]
- Mastromarino, P.; Vitali, B.; Mosca, L. Bacterial vaginosis: A review on clinical trials with probiotics. New Microbiol. 2013, 36, 229–238. [Google Scholar] [PubMed]
- Mastromarino, P.; Macchia, S.; Meggiorini, L.; Trinchieri, V.; Mosca, L.; Perluigi, M.; Midulla, C. Effectiveness of Lactobacillus-containing vaginal tablets in the treatment of symptomatic bacterial vaginosis. Clin. Microbiol. Infect. 2009, 15, 67–74. [Google Scholar] [CrossRef] [Green Version]
- Anukam, K.C.; Osazuwa, E.; Osemene, G.I.; Ehigiagbe, F.; Bruce, A.W.; Reid, G. Clinical study comparing probiotic Lactobacillus GR-1 and RC-14 with metronidazole vaginal gel to treat symptomatic bacterial vaginosis. Microbes Infect. 2006, 8, 2772–2776. [Google Scholar] [CrossRef]
- Raja, I.M.; Basavareddy, A.; Mukherjee, D.; Meher, B.R. Randomized, double-blind, comparative study of oral metronidazole and tinidazole in treatment of bacterial vaginosis. Indian J. Pharmacol. 2016, 48, 654–658. [Google Scholar] [CrossRef] [PubMed]
- Darwish, A.; Elnshar, E.M.; Hamadeh, S.M.; Makarem, M.H. Treatment options for bacterial vaginosis in patients at high risk of preterm labor and premature rupture of membranes. J. Obstet. Gynaecol. Res. 2007, 33, 781–787. [Google Scholar] [CrossRef]
- Ling, Z.; Liu, X.; Chen, W.; Luo, Y.; Yuan, L.; Xia, Y.; Nelson, K.E.; Huang, S.; Zhang, S.; Wang, Y.; et al. The Restoration of the Vaginal Microbiota After Treatment for Bacterial Vaginosis with Metronidazole or Probiotics. Microb. Ecol. 2013, 65, 773–780. [Google Scholar] [CrossRef]
- Larsson, P.G.; Stray-Pedersen, B.; Ryttig, K.R.; Larsen, S. Human lactobacilli as supplementation of clindamycin to patients with bacterial vaginosis reduce the recurrence rate; a 6-month, double-blind, randomized, placebo-controlled study. BMC Womens Health 2008, 8, 1–8. [Google Scholar] [CrossRef]
- Kekki, M. Vaginal clindamycin in preventing preterm birth and peripartal infections in asymptomatic women with bacterial vaginosis: A randomized, controlled trial. Obstet. Gynecol. 2001, 97, 643–648. [Google Scholar] [CrossRef]
- Martinez, R.C.R.; Franceschini, S.A.; Patta, M.C.; Quintana, S.M.; Gomes, B.C.; de Martinis, E.C.P.; Reid, G. Improved cure of bacterial vaginosis with single dose of tinidazole (2 g), Lactobacillus rhamnosus GR-1, and Lactobacillus reuteri RC-14: A randomized, double-blind, placebo-controlled trial. Can. J. Microbiol. 2009, 55, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Voorspoels, J.; Casteels, M.; Remon, J.P.; Temmerman, M. Local treatment of bacterial vaginosis with a bioadhesive metronidazole tablet. Eur. J. Obstet. Gynecol. Reprod. Biol. 2002, 105, 64–66. [Google Scholar] [CrossRef]
- Brandt, M.; Abels, C.; May, T.; Lohmann, K.; Schmidts-Winkler, I.; Hoyme, U.B. Intravaginally applied metronidazole is as effective as orally applied in the treatment of bacterial vaginosis, but exhibits significantly less side effects. Eur. J. Obstet. Gynecol. Reprod. Biol. 2008, 141, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Schwebke, J.R.; Desmond, R.A. Tinidazole vs. metronidazole for the treatment of bacterial vaginosis. Am. J. Obstet. Gynecol. 2011, 204, 211.e1–211.e6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thulkar, J.; Kriplani, A.; Agarwal, N. A comparative study of oral single dose of metronidazole, tinidazole, secnidazole and ornidazole in bacterial vaginosis. Indian J. Pharmacol. 2012, 44, 243–245. [Google Scholar] [CrossRef]
- Eriksson, K.; Carlsson, B.; Forsum, U.; Larsson, P.G. A double-blind treatment study of bacterial vaginosis with normal vaginal lactobacilli after an open treatment with vaginal clindamycin ovules. Acta Derm. Venereol. 2005, 85, 42–46. [Google Scholar] [CrossRef] [Green Version]
- Schwebke, J.R.; Desmond, R.A. A randomized trial of the duration of therapy with metronidazole plus or minus azithromycin for treatment of symptomatic bacterial vaginosis. Clin. Infect. Dis. 2015, 44, 213–219. [Google Scholar] [CrossRef]
- Paavonen, J.; Mangioni, C.; Martin, M.A.; Wajszczuk, C.P. Vaginal clindamycin and oral metronidazole for bacterial vaginosis: A randomized trial. Obstet. Gynecol. 2000, 96, 256–260. [Google Scholar] [CrossRef]
- Kurkinen-Räty, M.; Vuopala, S.; Koskela, M.; Kekki, M.; Kurki, T.; Paavonen, J.; Jouppila, P. A randomised controlled trial of vaginal clindamycin for early pregnancy bacterial vaginosis. Br. J. Obstet. Gynaecol. 2000, 107, 1427–1432. [Google Scholar] [CrossRef] [Green Version]
- Sobel, J.; Peipert, J.F.; McGregor, J.A.; Livengood, C.; Martin, M.; Robbins, J.; Wajszczuk, C.P. Efficacy of clindamycin vaginal ovule (3-day treatment) vs. clindamycin vaginal cream (7-day treatment) in bacterial vaginosis. Infect. Dis. Obstet. Gynecol. 2001, 9, 9–15. [Google Scholar] [CrossRef] [Green Version]
- Larsson, P.G.; Brandsborg, E.; Forsum, U.; Pendharkar, S.; Andersen, K.K.; Nasic, S.; Hammarström, L.; Marcotte, H. Extended antimicrobial treatment of bacterial vaginosis combined with human lactobacilli to find the best treatment and minimize the risk of relapses. BMC Infect. Dis. 2011, 11, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Hantoushzadeh, S.; Golshahi, F.; Javadian, P.; Khazardoost, S.; Aram, S.; Hashemi, S.; Mirarmandehi, B.; Borna, S. Comparative efficacy of probiotic yoghurt and clindamycin in treatment of bacterial vaginosis in pregnant women: A randomized clinical trial. J. Matern. Neonatal Med. 2012, 25, 1021–1024. [Google Scholar] [CrossRef]
- Kovachev, S.; Vatcheva-Dobrevski, R. Efficacy of combined 5-nitroimidazole and probiotic therapy of bacterial vaginosis: Randomized open trial. Akusherstvo I Ginekologiia 2013, 52, 19–26. [Google Scholar] [PubMed]
- Kovachev, S.; Dobrevski-Vacheva, R. Probiotic monotherapy of bacterial vaginosis: A open, randomized trial. Akusherstvo I Ginekol. 2013, 52, 36–42. [Google Scholar]
- Vujic, G.; Jajac Knez, A.; Despot Stefanovic, V.; Kuzmic Vrbanovic, V. Efficacy of orally applied probiotic capsules for bacterial vaginosis and other vaginal infections: A double-blind, randomized, placebo-controlled study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 168, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Bradshaw, C.S.; Pirotta, M.; de Guingand, D.; Hocking, J.S.; Morton, A.N.; Garland, S.M.; Fehler, G.; Morrow, A.; Walker, S.; Vodstrcil, L.A.; et al. Efficacy of oral metronidazole with vaginal clindamycin or vaginal probiotic for bacterial vaginosis: Randomised placebo-controlled double-blind trial. PLoS ONE 2012, 7, e34540. [Google Scholar] [CrossRef] [PubMed]
- Anukam, K.; Osazuwa, E.; Ahonkhai, I.; Ngwu, M.; Osemene, G.; Bruce, A.W.; Reid, G. Augmentation of antimicrobial metronidazole therapy of bacterial vaginosis with oral probiotic Lactobacillus rhamnosus GR-1 and Lactobacillus reuteri RC-14: Randomized, double-blind, placebo controlled trial. Microbes Infect. 2006, 8, 1450–1454. [Google Scholar] [CrossRef]
- Marcone, V.; Calzolari, E.; Bertini, M. Effectiveness of vaginal administration of Lactobacillus rhamnosus following conventional metronidazole therapy: How to lower the rate of bacterial vaginosis recurrences. New Microbiol. 2008, 31, 429–433. [Google Scholar]
- Ratna Sudha, M.; Yelikar, K.A.; Deshpande, S. Clinical Study of Bacillus coagulans Unique IS-2 (ATCC PTA-11748) in the Treatment of Patients with Bacterial Vaginosis. Indian J. Microbiol. 2012, 52, 396–399. [Google Scholar] [CrossRef] [Green Version]
- Bohbot, J.M.; Daraï, E.; Bretelle, F.; Brami, G.; Daniel, C.; Cardot, J.M. Efficacy and safety of vaginally administered lyophilized Lactobacillus crispatus IP 174178 in the prevention of bacterial vaginosis recurrence. J. Gynecol. Obstet. Hum. Reprod. 2018, 47, 81–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruiz, F.O.; Gerbaldo, G.; Asurmendi, P.; Pascual, L.M.; Giordano, W.; Barberis, I.L. Antimicrobial Activity, Inhibition of Urogenital Pathogens, and Synergistic Interactions between Lactobacillus Strains. Curr. Microbiol. 2009, 59, 497–501. [Google Scholar] [CrossRef] [PubMed]
- Altermann, E.; Klaenhammer, T.R. Group-specific comparison of four lactobacilli isolated from human sources using differential blast analysis. Genes Nutr. 2011, 6, 319–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, M.; Hidalgo-Cantabrana, C.; Goh, Y.J.; Sanozky-Dawes, R.; Barrangou, R. Comparative Analysis of Lactobacillus gasseri and Lactobacillus crispatus Isolated From Human Urogenital and Gastrointestinal Tracts. Front. Microbiol. 2020, 10, 3146. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Zeng, X.; Zhang, Y.; Kwong, J.S.W.; Zhang, C.; Li, S.; Sun, F.; Niu, Y.; Du, L. The methodological quality assessment tools for preclinical and clinical studies, systematic review and meta-analysis, and clinical practice guideline: A systematic review. J. Evid. Based. Med. 2015, 8, 2–10. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Sutton, A.J.; Ioannidis, J.P.A.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.; Rücker, G.; Harbord, R.M.; Schmid, C.H.; et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 2011, 343, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Lin, L.; Chu, H. Quantifying publication bias in meta-analysis. Biometrics 2018, 74, 785–794. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author, Year | Region | Country | Age Group (Years) | Pregnancy | Clinical Cure Rate (%) | Treatment Assays * | References |
|---|---|---|---|---|---|---|---|
| Raja, 2016 | Asia | India | 18–51 | No | 107/114 (93.86) | AB | [20] |
| Darwish, 2007 | Africa | Egypt | 20–27 | Yes | 91/156 (58.33) | AB | [21] |
| Ling, 2012 | Asia | China | NR | No | 45/55 (81.81) | AB, PB | [22] |
| Larsson, 2008 | Europe | Norway | 18–53 | No | 24/37 (64.86) | AB + PB | [23] |
| Kekki, 2002 | Europe | Finland | 17–43 | Yes | 123/187 (65.77) | AB | [24] |
| Martínez, 2009 | America | Brazil | 16–51 | No | 44/64 (68.75) | AB, AB + PB | [25] |
| Voorspoels, 2002 | Europe | Belgium | NR | No | 49/76 (64.47) | AB | [26] |
| Brandt, 2008 | Europe | Germany | 18–50 | No | 240/263(91.25) | AB | [27] |
| Schwebke, 2011 | America | USA | 21–35 | No | 168/287 (58.53) | AB | [28] |
| Thulkar, 2012 | Asia | India | 20–40 | No | 304/344 (88.37) | AB | [29] |
| Eriksson, 2005 | Europe | Sweden, Finland & Norway | 18–53 | No | 111/187 (59.35) | AB, AB + PB | [30] |
| Schwebke, 2015 | America | USA | 20–35 | No | 144/308 (46.75) | AB | [31] |
| Paavonen, 2000 | Europe | Finland | 16–60 | No | 172/233(73.82) | AB | [32] |
| Kurkinen, 2000 | Europe | Finland | 22–34 | Yes | 54/62 (87.09) | AB | [33] |
| Sobel, 2001 | America | USA | 16–58 | No | 270/342 (78.94) | AB | [34] |
| Larsson, 2011 | Europe | Sweden | 19–55 | No | 35/63 (55.55) | AB + PB | [35] |
| Hantoushzadeh, 2012 | Asia | Iran | 23–33 | Yes | 481/500 (96.20) | AB, PB | [36] |
| Kovachev, 2013a | Europe | Bulgaria | NR | No | 485/539 (89.98) | AB, AB + PB | [37] |
| Kovachev, 2013b | Europe | Bulgaria | NR | No | 224/381 (58.79) | AB, PB, AB + PB | [38] |
| Vujic, 2013 | Europe | Croatia | 18–58 | No | 243/395 (61.52) | PB | [39] |
| Anukam, 2006a | Africa | Nigeria | 18–50 | No | 30/40 (75.00) | AB, PB | [19] |
| Bradshaw, 2012 | Oceania | Australia | 18–50 | No | 381/408 (93.38) | AB, AB + PB | [40] |
| Anukam, 2006b | Africa | Nigeria | 18–44 | No | 82/106 (77.35) | AB, AB + PB | [41] |
| Mastromarino, 2009 | Europe | Italy | 23–45 | No | 12/18 (66.66) | PB | [18] |
| Marcone, 2008 | Europe | Italy | 18–40 | No | 63/84 (75.00) | AB, AB + PB | [42] |
| Ratna, 2011 | Asia | India | 30–36 | No | 25/40 (62.50) | AB, AB + PB | [43] |
| Bohbot, 2018 | Europe | France | NR | No | 52/76 (68.42) | AB, AB + PB | [44] |
| Treatment | k = 57 (Trials) | Clinical Cure Rate (95% CI) | Egger’s Test | Random Effects Model | |||
|---|---|---|---|---|---|---|---|
| p * | t | Q | I2 | p ** | |||
| Only antibiotics | 35 | 74.6 (69.1–79.3) | 0.091 | 0.7396 | 283.42 | 88.0 | 0.8453 |
| Conjugate (antibiotic + probiotic) | 16 | 74.1 (63.1–82.7) | 0. 296 | 0.9101 | 89.10 | 83.2 | |
| Only probiotics | 6 | 79.7 (59.3–91.4) | - | 1.1347 | 105.03 | 95.2 | |
| Pregnancy | |||||||
| No | 49 | 74.3 (69.4–78.6) | 0.046 | 0.7554 | 385.57 | 87.6 | 0.5946 |
| Yes | 8 | 78.6 (61.0–89.6) | - | 1.1908 | 122.26 | 94.3 | |
| Treatment | P-Score | Odds Ratio (95 % IC) | p * |
|---|---|---|---|
| Oral AB (clindamycin) and Local AB (5-nitroimidazole) + PB | 0.9208 | 44.4355 (3.8078; 518.5520) | 0.0025 |
| Oral AB (5-nitroimidazole) + PB | 0.8213 | 19.0430 (2.0464; 177.2109) | 0.0096 |
| Local AB (5-nitroimidazole) and Oral PB | 0.6783 | 9.7905 (0.6850; 139.9286) | 0.0927 |
| Oral AB (clindamycin) and Local AB (5-nitroimidazole) | 0.5757 | 6.7642 (0.2703; 169.2481) | 0.2446 |
| Oral AB (5-nitroimidazole) and Local PB | 0.5561 | 5.4659 (0.3630; 82.2974) | 0.2196 |
| Only local PB | 0.5431 | 4.7222 (1.2726; 17.5231) | 0.0203 |
| Only oral PB | 0.5102 | 4.3564 (0.5799; 32.7269) | 0.1526 |
| Local AB (clindamycin) + PB | 0.4856 | 3.9458 (0.3049; 51.0635) | 0.2934 |
| Only oral AB (clindamycin) | 0.4802 | 3.8568 (0.2989; 49.7715) | 0.3009 |
| Local AB (5-nitroimidazole) + PB | 0.4551 | 3.5051 (0.3416; 35.9620) | 0.2910 |
| Only oral AB (5-nitroimidazole) | 0.3188 | 2.1864 (0.4660; 10.2584) | 0.3213 |
| Only local AB (5-nitroimidazole) | 0.2891 | 2.0026 (0.6686; 5.9983) | 0.2147 |
| Only local AB (clindamycin) | 0.2681 | 1.8320 (0.4772; 7.0333) | 0.3778 |
| Placebo | - | - | - |
| Number of Lactobacilli Species a | k | CCR (95% CI) | Random Effects Model | |||
|---|---|---|---|---|---|---|
| T | Q | I2 | p * | |||
| 1 b | 4 | 82.6 (74.5–88.5) | 0 | 2.89 | 0 | <0.0001 |
| 2 | 10 | 77.3 (62.9–87.3) | 1.0376 | 145.15 | 93.8 | |
| 3 | 7 | 56.5 (48.5–64.2) | 0 | 3.72 | 0.0 | |
| Combinations (2 strains) | ||||||
| L. rhamnosus + L. acidophilus | 3 | 79.7 (37.4–96.3) | 1.6510 | 115.94 | 98.3 | 0.2413 |
| L. rhamnosus + L. gasseri | 2 | 63.0 (48.3–75.6) | 0 | 0.27 | 0.0 | |
| L. rhamnosus + L. reuteri | 5 | 80.8 (62.0–91.6) | 0.9469 | 23.62 | 83.1 | |
| Combinations (3 strains) | ||||||
| L. crispatus + L. gasseri + L. jensenii | 2 | 45.9 (22.5–71.4) | 0.4557 | 1.52 | 34.4 | 0.6728 |
| L. rhamnosus + L. gasseri (2 strains) | 2 | 61.3 (33.9–83.1) | 0 | 0.32 | 0.0 | |
| Other c | 3 | 57.9 (48.9–66.5) | 0 | 0.71 | 0.0 | |
| Includes L. rhamnosus? | ||||||
| No | 7 | 70.0 (53.9–82.4) | 0.7112 | 15.14 | 60.4 | 0.6010 |
| Yes | 14 | 74.8 (63.1–83.7) | 0.9333 | 155.50 | 91.6 | |
| L. rhamnosus with antibiotics? | ||||||
| Yes | 11 | 77.4 (64.4–86.7) | 0.9548 | 74.43 | 86.6 | 0.1323 |
| No | 3 | 61.3 (42.0–77.5) | 0.6031 | 21.55 | 90.7 | |
| Includes L. reuteri? | ||||||
| No | 15 | 71.8 (57.1–83.0) | 1.1589 | 136.89 | 89.8 | 0.6953 |
| Yes | 6 | 75.3 (62.2–84.9) | 0.6225 | 26.31 | 81.0 | |
| L. reuteri with antibiotics? | ||||||
| Yes | 4 | 77.6 (52.9–91.4) | 1.0339 | 19.86 | 84.9 | 0.9496 |
| No | 2 | 76.4 (38.0–94.5) | 1.1000 | 5.27 | 81.0 | |
| Includes L. acidophilus? | ||||||
| No | 18 | 71.4 (63.8–78.0) | 0.5355 | 49.68 | 65.8 | 0.6427 |
| Yes | 3 | 79.7 (37.4–96.3) | 1.6510 | 115.94 | 98.3 | |
| L. acidophilus with antibiotics? | ||||||
| Yes | 2 | 90.4 (84.9–94.1) | 0.2775 | 2.20 | 54.5 | <0.0001 |
| No | 1 | 42.7 (34.8–50.9) | - | 0.00 | - | |
| Includes L. gasseri? | ||||||
| No | 14 | 79.3 (68.7–87.0) | 0.9565 | 173.70 | 92.1 | 0.0051 |
| Yes d | 7 | 58.4 (47.8–68.2) | 0 | 3.89 | 0.0 | |
| Sub-Groups Region (≥3 Studies) a | k (Trials) | Clinical Cure Rate (95% CI) (%) | Egger’s Test | Random Model | |||
|---|---|---|---|---|---|---|---|
| p * | t | Q | I2 | p ** | |||
| Europe | 30 | 71.1 (64.4–76.9) | 0.378 | 0.7551 | 267.62 | 89.2 | 0.0085 |
| Asia | 12 | 90.0 (81.7–94.8) | 0.298 | 1.1241 | 90.56 | 87.9 | |
| Africa | 8 | 67.6 (56.1–77.4) | - | 0.5882 | 24.73 | 71.7 | |
| North America | 5 | 67.8 (56.4- 77.4) | - | 0.5170 | 30.87 | 87.0 | |
| Country (≥3 studies) a | |||||||
| India | 8 | 87.9 (76.8–94.1) | - | 1.0057 | 44.37 | 84.2 | 0.0069 |
| Sweden | 7 | 55.7 (43.0–67.7) | - | 0.0 | 3.33 | 0.0 | |
| Bulgaria | 5 | 77.1 (51.9–91.3) | - | 1.2791 | 166.01 | 97.6 | |
| Egypt | 4 | 58.3 (47.0–68.8) | - | 0.3257 | 5.90 | 49.1 | |
| Nigeria | 4 | 78.0 (59.4–89.5) | - | 0.7580 | 11.65 | 74.2 | |
| Italy | 3 | 72.9 (59.6–83.1) | - | 0.3423 | 3.41 | 41.3 | |
| Belgium | 3 | 64.4 (53.1–74.3) | - | 0.0 | 0.24 | 0.0 | |
| USA | 5 | 67.8 (56.4–77.4) | - | 0.5170 | 30.87 | 87.0 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muñoz-Barreno, A.; Cabezas-Mera, F.; Tejera, E.; Machado, A. Comparative Effectiveness of Treatments for Bacterial Vaginosis: A Network Meta-Analysis. Antibiotics 2021, 10, 978. https://doi.org/10.3390/antibiotics10080978
Muñoz-Barreno A, Cabezas-Mera F, Tejera E, Machado A. Comparative Effectiveness of Treatments for Bacterial Vaginosis: A Network Meta-Analysis. Antibiotics. 2021; 10(8):978. https://doi.org/10.3390/antibiotics10080978
Chicago/Turabian StyleMuñoz-Barreno, Alison, Fausto Cabezas-Mera, Eduardo Tejera, and António Machado. 2021. "Comparative Effectiveness of Treatments for Bacterial Vaginosis: A Network Meta-Analysis" Antibiotics 10, no. 8: 978. https://doi.org/10.3390/antibiotics10080978
APA StyleMuñoz-Barreno, A., Cabezas-Mera, F., Tejera, E., & Machado, A. (2021). Comparative Effectiveness of Treatments for Bacterial Vaginosis: A Network Meta-Analysis. Antibiotics, 10(8), 978. https://doi.org/10.3390/antibiotics10080978