
Antimicrobial Stewardship Activities in Public Healthcare Facilities in South Africa: A Baseline for Future Direction

 ,
, 


Abstract
:1. Introduction
2. Results
2.1. Awareness of Antimicrobial Resistance
2.2. Awareness of the Antimicrobial Resistance National Strategy Framework
2.3. Education, Communication and Public Awareness as the Basis of the Framework
2.3.1. Undergraduate Education
2.3.2. Continuous Education and In-Service Training
“…because we give education not just with dosages etc., but infection control that everyone involved in the care of a patient needs to know—small things like the catheter mustn’t be lying on the floor or on the bed. We also reiterate these points, for example, to sisters before giving drugs, examine the drip and see if there’s any inflammation or erythema or anything going on there, or alert and teaching them to prompt the doctor to look for those things if they’ve noticed it. So, not just in a formal sense of how, even how the antibiotic chart works but the small everyday things that continuous education, if it’s really helpful, makes a difference. And from the physiotherapist to the sister to the OT, everyone who comes to see the patient, remind them to be aware of that, and they do alert us to problems that we sometimes have missed, so that everyone involved in the care of a patient having that basic training really makes a difference”.(P#64; F19)
2.3.3. Communication and Feedback
“The pharmacy side does come and sometimes they revise, and they want to know the reasoning behind certain prescriptions, the duration of the dosage and I think that forms a kind of feedback function because a lot of times we may learn from that, that we should adjust our prescribing behaviour at times”.(P#27; community service MO; F3; 24-h CHC)
“… there has to be more active communication in terms of educating everyone that this is what our goal is of our hospital, what our aim is and having access to all the information so that everybody’s on the same page”.(P#23; pharmacist; F15; district hospital)
2.3.4. Public Awareness
2.4. Involvement of Management
2.5. Antimicrobial Champion
“I think the most important gap in all of this antibiotic stewardship is not having currently at least a weekly ward round with an infectious diseases specialist or someone who is orientated or coming from that background [e.g., an antimicrobial champion] … because they will question all the decision-making and educate on a weekly basis not only to consult on difficult patients where there needs to be a more specialist opinion, but they’ll look after the small things and they will orientate everyone. They’ll get everyone on board.”
2.6. Multidisciplinary Collaboration
2.7. Collaboration with Microbiology
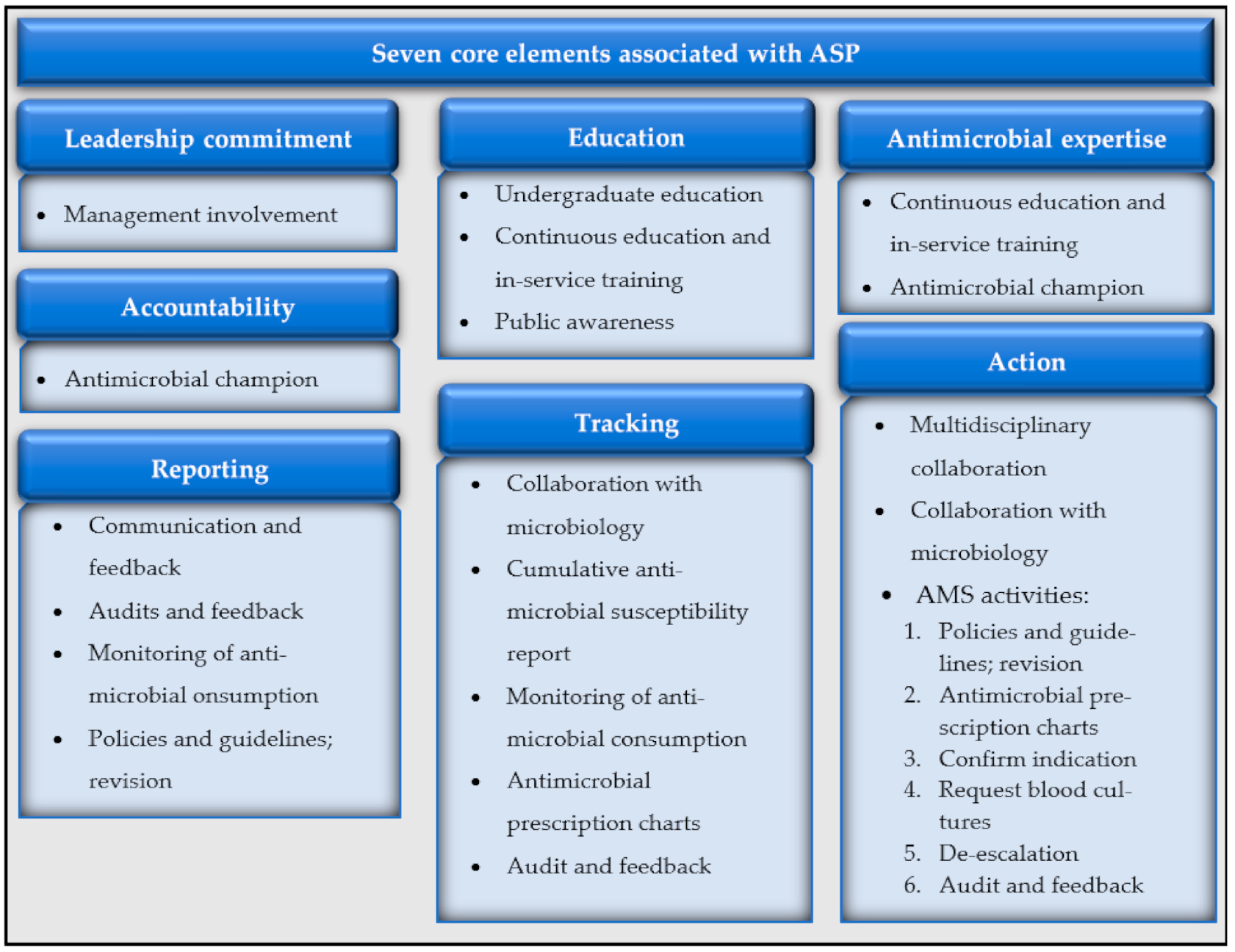
2.8. Antimicrobial Stewardship Activities
“… and we started with the antibiotic stewardship, the first month or two we were on 10% to 30% and now some months we get 80%”.[referring to correct antimicrobial prescribing] (P#52; operational manager; F22; 8-h CHC)
2.8.1. Policies, Guidelines and the Revision Thereof
“Some doctors are resistant and there are some that are willing to accommodate and say okay we’ll change it to correspond to the guidelines. Because we have disseminated our guidelines throughout the hospital in electronic format, so there is access to it in all the wards”.(P#24; pharmacist; F15; district hospital)
“I think in most instances it’s a lot of interns prescribing. They are not aware of the guidelines maybe, so they won’t even look at the guidelines”.(P#23; pharmacist; F15; district hospital)
“If someone is coming from outside, like if it’s a locum nurse or doctor, then they often, don’t know what the latest guidelines are, or... they don’t have the mobile app [with the guidelines]... they haven’t worked in primary healthcare for a long time”.(P#52; family physician; F22; 8-h CHC)
“… we have lots of problems with nosocomial sepsis and we’ve had a look from 2013 at all our patients who have been admitted there and seen what has been cultured from various samples and correlate it with the clinical picture of the patient and what antibiotic was sensitive to and what was the outcome of the patient. We’ve made up our own guidelines on the antibiotics that we used based on that. But it’s not ‘policed’ by a suitably qualified person or reviewed or compiled. It’s our own solution to the problem that we face”(P#74; specialist; F19; provincial tertiary hospital)
2.8.2. Antimicrobial Prescription Charts
“I also developed in the beginning a form with different colours that say to the doctors and the nurses who must do what, what information must be where and everything”.(P#62; clinical pharmacist; F5; district hospital)
2.8.3. Confirming Indication
2.8.4. Requesting of Blood Cultures
“When we do our audits, you’ll see that most of them don’t do a culture, because we have a box in our antibiotic [prescription chart]—‘Have you sent for a culture before initiation or not’, and most have ticked ‘No’. So, they’re just treating empirically”.(P#24; pharmacist; F15; district hospital)
“… instances where you look back in a patient’s history and you see that they’ve been taking one antibiotic for a number of weeks or months with no change for the same condition and then that warrants another review from the clinician”.(P#17; pharmacy manager; F14; 8-h CHC)
2.8.5. De-Escalation
2.8.6. Audit and Feedback
2.8.7. Cumulative Antimicrobial Susceptibility Report (Antibiogram)
2.8.8. Monitoring of Antimicrobial Consumption
“At times our files, sometimes previous clinical notes are lost or misplaced so we are not able to follow up the patient’s history chronologically. So, at times something might have been prescribed in the past and it wasn’t noted down, because the patient has had a replacement file, so then it might be prescribed again, because our patients are also unaware sometimes of what medication they’re taking”.(P#27; community service MO; F3; 24-h CHC)
“Many times I’ve seen with the filing office a patient will be prescribed a medication, the history is lost and they give the patient a new file. How can this patient be properly followed up?”.(P#44; pharmacist; F4; 24-h CHC)
3. Discussion
4. Materials and Methods
4.1. Design
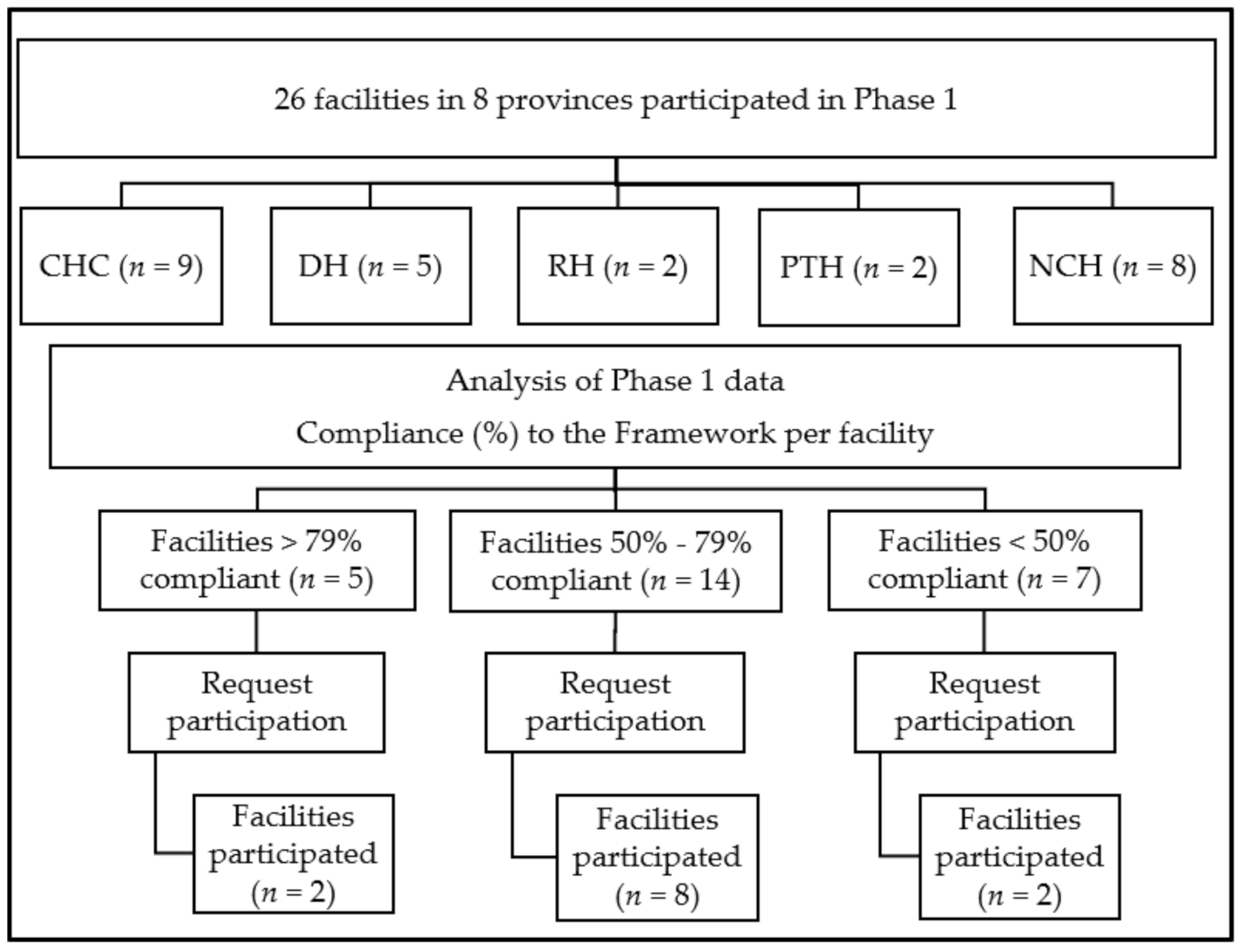
4.2. Setting
4.3. Participants
4.4. Data Collection Instruments and Process
4.5. Data Management and Analysis
4.6. Ethical Considerations
5. Recommendations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tacconelli, E.; Carrara, E.; Savoldi, A.; Harbarth, S.; Mendelson, M.; Monnet, D.L.; Pulcini, C.; Kahlmeter, G.; Kluytmans, J.; Carmeli, Y.; et al. Discovery, research, and development of new antibiotics: The WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect. Dis. 2018, 18, 318–327. [Google Scholar] [CrossRef]
- Cassini, A.; Hogberg, L.D.; Plachouras, D.; Quattrocchi, A.; Hoxha, A.; Simonsen, G.S.; Colomb-Cotinat, M.; Kretzschmar, M.E.; Devleesschauwer, B.; Cecchini, M.; et al. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: A population-level modelling analysis. Lancet Infect. Dis. 2019, 19, 56–66. [Google Scholar] [CrossRef] [Green Version]
- Hofer, U. The cost of antimicrobial resistance. Nat. Rev. Microbiol. 2019, 17, 3. [Google Scholar] [CrossRef] [PubMed]
- Founou, R.C.; Founou, L.L.; Essack, S.Y. Clinical and economic impact of antibiotic resistance in developing countries: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0189621. [Google Scholar] [CrossRef] [Green Version]
- Zhen, X.; Lundborg, C.S.; Sun, X.; Hu, X.; Dong, H. Economic burden of antibiotic resistance in ESKAPE organisms: A systematic review. Antimicrob. Resist. Infect. Control. 2019, 8, 137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathers, C. Global Burden of Disease. In International Encyclopedia of Public Health, 2nd ed.; Quah, S.R., Ed.; Academic Press: Oxford, UK, 2017; pp. 256–267. [Google Scholar] [CrossRef]
- South African Medical Research Council (SAMRC). Burden of Health and Disease in South Africa: Medical Research Council Briefing. Meeting Report. 2016. Available online: https://pmg.org.za/committee-meeting/22198/ (accessed on 15 February 2017).
- Essack, S.Y.; Desta, A.T.; Abotsi, R.E.; Agoba, E.E. Antimicrobial resistance in the WHO African region: Current status and roadmap for action. J. Public Health 2017, 39, 8–13. [Google Scholar] [CrossRef] [Green Version]
- Llor, C.; Bjerrum, L. Antimicrobial resistance: Risk associated with antibiotic overuse and initiatives to reduce the problem. Ther. Adv. Drug Saf. 2014, 5, 229–241. [Google Scholar] [CrossRef] [Green Version]
- Zhussupova, G.; Skvirskaya, G.; Reshetnikov, V.; Dragojevic-Simic, V.; Rancic, N.; Utepova, D.; Jakovljevic, M. The Evaluation of Antibiotic Consumption at the Inpatient Level in Kazakhstan from 2011 to 2018. Antibiotics 2020, 9, 57. [Google Scholar] [CrossRef] [Green Version]
- WHO. Antimicrobial resistance. Fact Sheet. 2018. Available online: http://www.who.int/mediacentre/factsheets/fs194/en/ (accessed on 27 March 2019).
- Tadesse, B.T.; Ashley, E.A.; Ongarello, S.; Havumaki, J.; Wijegoonewardena, M.; Gonzalez, I.J.; Dittrich, S. Antimicrobial resistance in Africa: A systematic review. BMC Infect. Dis 2017, 17, 616. [Google Scholar] [CrossRef]
- Jakovljevic, M.; Getzen, T.E. Growth of Global Health Spending Share in Low and Middle Income Countries. Front. Pharmacol. 2016, 7. [Google Scholar] [CrossRef] [Green Version]
- Jakovljevic, M.; Potapchik, E.; Popovich, L.; Barik, D.; Getzen, T.E. Evolving Health Expenditure Landscape of the BRICS Nations and Projections to 2025. Health Econ. 2017, 26, 844–852. [Google Scholar] [CrossRef] [PubMed]
- Meyer, J.C.; Schellack, N.; Stokes, J.; Lancaster, R.; Zeeman, H.; Defty, D.; Godman, B.; Steel, G. Ongoing Initiatives to Improve the Quality and Efficiency of Medicine Use within the Public Healthcare System in South Africa; A Preliminary Study. Front. Pharmacol. 2017, 8, 751. [Google Scholar] [CrossRef] [Green Version]
- Godman, B.; Grobler, C.; Van-De-Lisle, M.; Wale, J.; Barbosa, W.B.; Massele, A.; Opondo, P.; Petrova, G.; Tachkov, K.; Sefah, I.; et al. Pharmacotherapeutic interventions for bipolar disorder type II: Addressing multiple symptoms and approaches with a particular emphasis on strategies in lower and middle-income countries. Expert Opin. Pharmacother. 2019, 20, 2237–2255. [Google Scholar] [CrossRef] [PubMed]
- Godman, B.; Basu, D.; Pillay, Y.; Almeida, P.; Mwita, J.C.; Rwegerera, G.M.; Anand Paramadhas, B.D.; Tiroyakgosi, C.; Patrick, O.; Niba, L.L.; et al. Ongoing and planned activities to improve the management of patients with Type 1 diabetes across Africa; implications for the future. Hosp. Pract. 2020, 48, 51–67. [Google Scholar] [CrossRef]
- Godman, B.; Basu, D.; Pillay, Y.; Mwita, J.C.; Rwegerera, G.M.; Anand Paramadhas, B.D.; Tiroyakgosi, C.; Okwen, P.M.; Niba, L.L.; Nonvignon, J.; et al. Review of Ongoing Activities and Challenges to Improve the Care of Patients With Type 2 Diabetes Across Africa and the Implications for the Future. Front. Pharmacol. 2020, 11, 108. [Google Scholar] [CrossRef]
- Jakovljevic, M.; Timofeyev, Y.; Ekkert, N.V.; Fedorova, J.V.; Skvirskaya, G.; Bolevich, S.; Reshetnikov, V.A. The impact of health expenditures on public health in BRICS nations. J. Sport Health Sci. 2019, 8, 516–519. [Google Scholar] [CrossRef] [PubMed]
- National Department of Health (NDoH). Antimicrobial Resistance. National Strategy Framework 2014–2024. Pretoria, South Africa. Available online: https://www.jpiamr.eu/wp-content/uploads/2018/10/Antimicrobial-Resistance-National-Strategy-Framework-2014-2024_South-Africa.pdf (accessed on 2 April 2017).
- Godman, B.; Egwuenu, A.; Haque, M.; Malande, O.O.; Schellack, N.; Kumar, S.; Saleem, Z.; Sneddon, J.; Hoxha, I.; Islam, S.; et al. Strategies to Improve Antimicrobial Utilization with a Special Focus on Developing Countries. Life 2021, 11, 528. [Google Scholar] [CrossRef] [PubMed]
- McEwen, S.A.; Collignon, P.J. Antimicrobial Resistance: A One Health Perspective. Microbiol. Spectr. 2018, 6. [Google Scholar] [CrossRef] [Green Version]
- National Department of Health (NDoH). Guidelines on Implementation of the Antimicrobial Strategy in South Africa: One Health Approach and Governance. Pretoria, South Africa. 2017. Available online: http://www.health.gov.za/index.php/antimicrobial-resistance?download=2194:antimicrobial-stewardship-guidelines-governance-june2017 (accessed on 10 June 2017).
- Furst, J.; Cizman, M.; Mrak, J.; Kos, D.; Campbell, S.; Coenen, S.; Gustafsson, L.L.; Furst, L.; Godman, B. The influence of a sustained multifaceted approach to improve antibiotic prescribing in Slovenia during the past decade: Findings and implications. Expert Rev. Anti Infect. Ther. 2015, 13, 279–289. [Google Scholar] [CrossRef] [PubMed]
- Abilova, V.; Kurdi, A.; Godman, B. Ongoing initiatives in Azerbaijan to improve the use of antibiotics; findings and implications. Expert Rev. Anti-Infect. Ther. 2018, 16, 77–84. [Google Scholar] [CrossRef]
- Bojanic, L.; Markovic-Pekovic, V.; Skrbic, R.; Stojakovic, N.; Ethermanovic, M.; Bojanic, J.; Furst, J.; Kurdi, A.B.; Godman, B. Recent Initiatives in the Republic of Srpska to Enhance Appropriate Use of Antibiotics in Ambulatory Care; Their Influence and Implications. Front. Pharmacol. 2018, 9, 442. [Google Scholar] [CrossRef] [PubMed]
- Wojkowska-Mach, J.; Godman, B.; Glassman, A.; Kurdi, A.; Pilc, A.; Rozanska, A.; Skoczyński, S.; Wałaszek, M.; Bochenek, T. Antibiotic consumption and antimicrobial resistance in Poland; findings and implications. Antimicrob. Resist. Infect. Control. 2018, 7, 136. [Google Scholar] [CrossRef] [Green Version]
- National Department of Health, Republic of South Africa. Implementation Plan for The Antimicrobial Resistance Strategy Framework in South Africa: 2014–2019. 2015. Available online: http://www.health.gov.za/index.php/antimicrobial-resistance (accessed on 8 January 2020).
- National Health Insurance Bill [Online]. Pretoria, South Africa. 2019. Available online: https://www.gov.za/sites/default/files/gcis_document/201908/national-health-insurance-bill-b-11-2019.pdf (accessed on 8 January 2020).
- Statistics South Africa. General Household Survey (2017). 2018. Available online: http://www.statssa.gov.za/publications/P0318/P03182017.pdf (accessed on 17 March 2020).
- Cullinan, K. Health Services in South Africa: A basic introduction. Health-e News Service, 2006. Available online: https://health-e.org.za/2006/01/29/health-services-in-south-africa-a-basic-introduction/ (accessed on 5 March 2019).
- Schellack, N.; Benjamin, D.; Brink, A.; Duse, A.; Faure, K.; Goff, D.; Mendelson, M.; Meyer, J.; Miot, J.; Perovic, O.; et al. A situational analysis of current antimicrobial governance, regulation, and utilization in South Africa. Int. J. Infect. Dis. 2017, 64, 100–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engler, D.; Meyer, J.C.; Schellack, N.; Kurdi, A.; Godman, B. Compliance with South Africa’s Antimicrobial Resistance National Strategy Framework: Are we there yet? J. Chemother. 2021, 33, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Ofori-Asenso, R.; Brhlikova, P.; Pollock, A.M. Prescribing indicators at primary health care centers within the WHO African region: A systematic analysis (1995–2015). BMC Public Health 2016, 16, 724. [Google Scholar] [CrossRef] [Green Version]
- Godman, B.; Haque, M.; McKimm, J.; Abu Bakar, M.; Sneddon, J.; Wale, J.; Campbell, S.; Martin, A.P.; Hoxha, I.; Abilova, V.; et al. Ongoing strategies to improve the management of upper respiratory tract infections and reduce inappropriate antibiotic use particularly among lower and middle-income countries: Findings and implications for the future. Curr. Med. Res. Opin. 2020, 36, 301–327. [Google Scholar] [CrossRef]
- Niaz, Q.; Godman, B.; Massele, A.; Campbell, S.; Kurdi, A.; Kagoya, H.R.; Kibuule, D. Validity of World Health Organisation prescribing indicators in Namibia’s primary healthcare: Findings and implications. Int. J. Qual. Health Care 2019, 31, 338–345. [Google Scholar] [CrossRef] [Green Version]
- Niaz, Q.; Godman, B.; Campbell, S.; Kibuule, D. Compliance to prescribing guidelines among public health care facilities in Namibia; findings and implications. Int. J. Clin. Pharm. 2020, 42, 1227–1236. [Google Scholar] [CrossRef]
- Matsitse, T.B.; Helberg, E.; Meyer, J.C.; Godman, B.; Massele, A.; Schellack, N. Compliance with the primary health care treatment guidelines and the essential medicines list in the management of sexually transmitted infections in correctional centres in South Africa: Findings and implications. Expert Rev. Anti-Infect. Ther. 2017, 15, 963–972. [Google Scholar] [CrossRef] [PubMed]
- Sefah, I.A.; Essah, D.O.; Kurdi, A.; Sneddon, J.; Alalbila, T.M.; Kordorwu, H.; Godman, B. Assessment of adherence to pneumonia guidelines and its determinants in an ambulatory care clinic in Ghana: Findings and implications for the future. JAC Antimicrob. Resist. 2021, 3, dlab080. [Google Scholar] [CrossRef]
- De Bruycker, M.; Van den Bergh, R.; Dahmane, A.; Khogali, M.; Schiavetti, B.; Nzomukunda, Y.; Alders, P.; Allaouna, M.; Cloquet, C.; Enarson, D.A.; et al. Non-adherence to standard treatment guidelines in a rural paediatric hospital in Sierra Leone. Public Health Action 2013, 3, 118–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rezal, R.S.; Hassali, M.A.; Alrasheedy, A.A.; Saleem, F.; Yusof, F.A.; Kamal, M.; Mohd Din, R.; Godman, B. Prescribing patterns for upper respiratory tract infections: A prescription-review of primary care practice in Kedah, Malaysia, and the implications. Expert Rev. Anti-Infect. Ther. 2015, 13, 1547–1556. [Google Scholar] [CrossRef] [Green Version]
- Gasson, J.; Blockman, M.; Willems, B. Antibiotic prescribing practice and adherence to guidelines in primary care in the Cape Town Metro District, South Africa. S. Afr. Med. J. 2018, 108, 304–310. [Google Scholar] [CrossRef]
- Ncube, N.B.; Solanki, G.C.; Kredo, T.; Lalloo, R. Antibiotic prescription patterns of South African general medical practitioners for treatment of acute bronchitis. S. Afr. Med. J. 2017, 107, 119–122. [Google Scholar] [CrossRef] [Green Version]
- McLeod, M.; Ahmad, R.; Shebl, N.A.; Micallef, C.; Sim, F.; Holmes, A. A whole-health-economy approach to antimicrobial stewardship: Analysis of current models and future direction. PLoS Med. 2019, 16, e1002774. [Google Scholar] [CrossRef]
- Davey, P.; Marwick, C.A.; Scott, C.L.; Charani, E.; McNeil, K.; Brown, E.; Gould, I.M.; Ramsay, C.R.; Michie, S. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst. Rev. 2017, 2, Cd003543. [Google Scholar] [CrossRef] [Green Version]
- Nathwani, D.; Varghese, D.; Stephens, J.; Ansari, W.; Martin, S.; Charbonneau, C. Value of hospital antimicrobial stewardship programs [ASPs]: A systematic review. Antimicrob. Resist. Infect. Control. 2019, 8, 35. [Google Scholar] [CrossRef]
- Cox, J.A.; Vlieghe, E.; Mendelson, M.; Wertheim, H.; Ndegwa, L.; Villegas, M.V.; Gould, I.; Levy Hara, G. Antibiotic stewardship in low- and middle-income countries: The same but different? Clin. Microbiol. Infect. 2017, 23, 812–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fadare, J.O.; Ogunleye, O.; Iliyasu, G.; Adeoti, A.; Schellack, N.; Engler, D.; Massele, A.; Godman, B. Status of antimicrobial stewardship programmes in Nigerian tertiary healthcare facilities: Findings and implications. J. Glob. Antimicrob. Resist. 2019, 17, 132–136. [Google Scholar] [CrossRef] [Green Version]
- Ogunleye, O.O.; Fadare, J.O.; Yinka-Ogunleye, A.F.; Anand Paramadhas, B.D.; Godman, B. Determinants of antibiotic prescribing among doctors in a Nigerian urban tertiary hospital. Hosp. Pract. 2019, 47, 53–58. [Google Scholar] [CrossRef]
- Kalungia, A.C.; Mwambula, H.; Munkombwe, D.; Marshall, S.; Schellack, N.; May, C.; Jones, A.S.C.; Godman, B. Antimicrobial stewardship knowledge and perception among physicians and pharmacists at leading tertiary teaching hospitals in Zambia: Implications for future policy and practice. J. Chemother. 2019, 31, 378–387. [Google Scholar] [CrossRef]
- Schellack, N.; Bronkhorst, E.; Messina, A.P.; Coetzee, R.; Godman, B.; Gous, A.G.S.; Kolman, S.; Labuschagne, Q.; Malan, L.; Messina, A.P.; et al. SASOCP position statement on the pharmacist’s role in antibiotic stewardship 2018. S. Afr. J. Infect. Dis. 2018, 33, 28–35. [Google Scholar] [CrossRef] [Green Version]
- Boyles, T.H.; Naicker, V.; Rawoot, N.; Raubenheimer, P.J.; Eick, B.; Mendelson, M. Sustained reduction in antibiotic consumption in a South African public sector hospital; Four year outcomes from the Groote Schuur Hospital antibiotic stewardship program. S. Afr. Med. J. 2017, 107, 115–118. [Google Scholar] [CrossRef] [Green Version]
- Khdour, M.R.; Hallak, H.O.; Aldeyab, M.A.; Nasif, M.A.; Khalili, A.M.; Dallashi, A.A.; Khofash, M.B.; Scott, M.G. Impact of antimicrobial stewardship programme on hospitalized patients at the intensive care unit: A prospective audit and feedback study. Br. J. Clin. Pharmacol. 2018, 84, 708–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, Y.; Shen, P.; Zheng, B.; Zhou, K.; Luo, Q.; Li, L. Change in Antibiotic Use in Secondary and Tertiary Hospitals Nationwide After a National Antimicrobial Stewardship Campaign Was Launched in China, 2011-2016: An Observational Study. J. Infect. Dis. 2020, 221, S148–S155. [Google Scholar] [CrossRef]
- van den Bergh, D.; Messina, A.P.; Goff, D.A.; van Jaarsveld, A.; Coetzee, R.; de Wet, Y.; Bronkhorst, E.; Brink, A.; Mendelson, M.; Richards, G.A.; et al. A pharmacist-led prospective antibiotic stewardship intervention improves compliance to community-acquired pneumonia guidelines in 39 public and private hospitals across South Africa. Int. J. Antimicrob. Agents 2020, 56, 106189. [Google Scholar] [CrossRef] [PubMed]
- Mwita, J.C.; Ogunleye, O.O.; Olalekan, A.; Kalungia, A.C.; Kurdi, A.; Saleem, Z.; Sneddon, J.; Godman, B. Key Issues Surrounding Appropriate Antibiotic Use for Prevention of Surgical Site Infections in Low- and Middle-Income Countries: A Narrative Review and the Implications. Int. J. Gen. Med. 2021, 14, 515–530. [Google Scholar] [CrossRef]
- Munkholm, L.; Rubin, O. The global governance of antimicrobial resistance: A cross-country study of alignment between the global action plan and national action plans. Glob. Health 2020, 16, 109. [Google Scholar] [CrossRef]
- Sangeda, R.Z.; Kibona, J.; Munishi, C.; Arabi, F.; Manyanga, V.P.; Mwambete, K.D.; Horumpende, P.G. Assessment of Implementation of Antimicrobial Resistance Surveillance and Antimicrobial Stewardship Programs in Tanzanian Health Facilities a Year After Launch of the National Action Plan. Front. Public Health 2020, 8, 454. [Google Scholar] [CrossRef]
- Zaney, G.D. Ghana’s National Action Plan On AMR Implementation On Course―But It Requires Support From All. 2019. Available online: https://allafrica.com/stories/201908270183.html (accessed on 15 April 2021).
- Saleem, Z.; Godman, B.; Azhar, F.; Kalungia, A.C.; Fadare, J.; Opanga, S.; Markovic-Pekovic, V.; Hoxha, I.; Saeed, A.; Al-Gethamy, M.; et al. Progress on the national action plan of Pakistan on antimicrobial resistance (AMR): A scoping review and the implications. Expert Rev. Anti-Infect. Ther. 2021. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.S.; Durrance-Bagale, A.; Mateus, A.; Sultana, Z.; Hasan, R.; Hanefeld, J. What are the barriers to implementing national antimicrobial resistance action plans? A novel mixed-methods policy analysis in Pakistan. Health Policy Plan. 2020, 35, 973–982. [Google Scholar] [CrossRef] [PubMed]
- Majumder, M.A.A.; Rahman, S.; Cohall, D.; Bharatha, A.; Singh, K.; Haque, M.; Gittens-St Hilaire, M. Antimicrobial Stewardship: Fighting Antimicrobial Resistance and Protecting Global Public Health. Infect. Drug Resist. 2020, 13, 4713–4738. [Google Scholar] [CrossRef]
- Haque, M.; Godman, B. Potential Strategies to Improve Antimicrobial Utilisation in Hospitals in Bangladesh Building on Experiences Across Developing Countries. Bangladesh J. Med. Sci. 2021, 19, 469–477. [Google Scholar] [CrossRef]
- Pulcini, C.; Binda, F.; Lamkang, A.S.; Trett, A.; Charani, E.; Goff, D.A.; Harbarth, S.; Hinrichsen, S.L.; Levy-Hara, G.; Mendelson, M.; et al. Developing core elements and checklist items for global hospital antimicrobial stewardship programmes: A consensus approach. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2019, 25, 20–25. [Google Scholar] [CrossRef] [Green Version]
- CDC. The Core Elements of Human Antibiotic Stewardship Programs in Resource -Limited Settings: National and Hospital Levels. 2018. Available online: https://www.cdc.gov/antibiotic-use/healthcare/implementation.html (accessed on 28 June 2021).
- Massele, A.; Tiroyakgosi, C.; Matome, M.; Desta, A.; Muller, A.; Paramadhas, B.D.; Malone, B.; Kurusa, G.; Didimalang, T.; Moyo, M.; et al. Research activities to improve the utilization of antibiotics in Africa. Expert Rev. Pharm. Outcomes Res. 2017, 17, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afriyie, D.K.; Sefah, I.A.; Sneddon, J.; Malcolm, W.; McKinney, R.; Cooper, L.; Kurdi, A.; Godman, B.; Seaton, R.A. Antimicrobial point prevalence surveys in two Ghanaian hospitals: Opportunities for antimicrobial stewardship. JAC Antimicrob. Resist. 2020, 2, dlaa001. [Google Scholar] [CrossRef] [Green Version]
- Mendelson, M.; Matsoso, M. The South African antimicrobial resistance strategy framework. AMR Control 2015, 2015, 54–61. [Google Scholar]
- Pulcini, C.; Gyssens, I.C. How to educate prescribers in antimicrobial stewardship practices. Virulence 2013, 4, 192–202. [Google Scholar] [CrossRef] [Green Version]
- Mao, W.; Vu, H.; Xie, Z.; Chen, W.; Tang, S. Systematic review on irrational use of medicines in China and Vietnam. PLoS ONE 2015, 10, e0117710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riaz, H.; Godman, B.; Hussain, S.; Malik, F.; Mahmood, S.; Shami, A.; Bashir, S. Prescribing of bisphosphonates and antibiotics in Pakistan: Challenges and opportunities for the future. JPHSR 2015, 6, 111–121. [Google Scholar] [CrossRef] [Green Version]
- Fadare, J.O.; Oshikoya, K.A.; Ogunleye, O.O.; Desalu, O.O.; Ferrario, A.; Enwere, O.O.; Adeoti, A.; Sunmonu, T.A.; Massele, A.; Baker, A.; et al. Drug promotional activities in Nigeria: Impact on the prescribing patterns and practices of medical practitioners and the implications. Hosp. Pract. (1995) 2018, 46, 77–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathew, P.; Sivaraman, S.; Chandy, S. Communication strategies for improving public awareness on appropriate antibiotic use: Bridging a vital gap for action on antibiotic resistance. J. Fam. Med. Prim. Care 2019, 8, 1867–1871. [Google Scholar] [CrossRef] [PubMed]
- National Department of Health (NDoH). Guidelines for the Prevention and Containment of Antimicrobial Resistance in South African Hospitals. Pretoria, South Africa. 2018. Available online: www.health.gov.za/index.php/antimicrobial (accessed on 7 November 2019).
- Olaru, I.D.; Meierkord, A.; Godman, B.; Ngwenya, C.; Fitzgerald, F.; Dondo, V.; Ferrand, R.A.; Kranzer, K. Assessment of antimicrobial use and prescribing practices among pediatric inpatients in Zimbabwe. J. Chemother. 2020, 32, 456–459. [Google Scholar] [CrossRef]
- van der Sandt, N.; Schellack, N.; Mabope, L.A.; Mawela, M.P.B.; Kruger, D.; Godman, B. Surgical Antimicrobial Prophylaxis Among Pediatric Patients in South Africa Comparing Two Healthcare Settings. Pediatric Infect. Dis. J. 2019, 38, 122–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sneddon, J.; Cooper, L.; Afriyie, D.K.; Sefah, I.A.; Cockburn, A.; Kerr, F.; Cameron, E.; Goldthorpe, J.; Kurdi, A.; Seaton, R.A. Supporting antimicrobial stewardship in Ghana: Evaluation of the impact of training on knowledge and attitudes of healthcare professionals in two hospitals. JAC-Antimicrob. Resist. 2020, 2. [Google Scholar] [CrossRef]
- Babatola, A.O.; Fadare, J.O.; Olatunya, O.S.; Obiako, R.; Enwere, O.; Kalungia, A.; Ojo, T.O.; Sunmonu, T.A.; Desalu, O.; Godman, B. Addressing antimicrobial resistance in Nigerian hospitals: Exploring physicians prescribing behavior, knowledge, and perception of antimicrobial resistance and stewardship programs. Expert Rev. Anti-Infect. Ther. 2021, 19, 537–546. [Google Scholar] [CrossRef]
- Huttner, B.; Saam, M.; Moja, L.; Mah, K.; Sprenger, M.; Harbarth, S.; Magrini, N. How to improve antibiotic awareness campaigns: Findings of a WHO global survey. BMJ Glob. Health 2019, 4, e001239. [Google Scholar] [CrossRef]
- Akpan, M.R.; Isemin, N.U.; Udoh, A.E.; Ashiru-Oredope, D. Implementation of antimicrobial stewardship programmes in African countries: A systematic literature review. J. Glob. Antimicrob. Resist. 2020, 22, 317–324. [Google Scholar] [CrossRef]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Soucy, J.R.; Westwood, D.; Daneman, N.; MacFadden, D.R. Antibiotic prescribing in patients with COVID-19: Rapid review and meta-analysis. Clin. Microbiol. Infect. Off. 2021, 27, 520–531. [Google Scholar] [CrossRef]
- Hsu, J. How covid-19 is accelerating the threat of antimicrobial resistance. BMJ 2020, 369, m1983. [Google Scholar] [CrossRef]
- Palavecino, E.L.; Williamson, J.C.; Ohl, C.A. Collaborative Antimicrobial Stewardship: Working with Microbiology. Infect. Dis. Clin. N. Am. 2020, 34, 51–65. [Google Scholar] [CrossRef] [PubMed]
- Kuper, K.M.; Hamilton, K.W. Collaborative Antimicrobial Stewardship: Working with Information Technology. Infect. Dis. Clin. N. Am. 2020, 34, 31–49. [Google Scholar] [CrossRef] [PubMed]
- South African National Department of Health. National Guideline for the Establishment and Functioning of Pharmaceutical and Therapeutics Committees in South Africa. 13 December 2019. Available online: http://www.health.gov.za/index.php/affordable-medicines/category/544-pharmaceutical-and-therapeutics-committees (accessed on 3 November 2019).
- Matlala, M.; Gous, A.G.; Godman, B.; Meyer, J.C. Structure and activities of pharmacy and therapeutics committees among public hospitals in South Africa; findings and implications. Expert Rev. Clin. Pharmacol. 2017, 10, 1273–1280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mashaba, T.P.; Matlala, M.; Godman, B.; Meyer, J.C. Implementation and monitoring of decisions by pharmacy and therapeutics committees in South African public sector hospitals. Expert Rev. Clin. Pharmacol. 2019, 12, 159–168. [Google Scholar] [CrossRef]
- Bjorkhem-Bergman, L.; Andersen-Karlsson, E.; Laing, R.; Diogene, E.; Melien, O.; Jirlow, M.; Malmstrom, R.E.; Vogler, S.; Godman, B.; Gustafsson, L.L. Interface management of pharmacotherapy. Joint hospital and primary care drug recommendations. Eur. J. Clin. Pharmacol. 2013, 69 (Suppl. 1), 73–78. [Google Scholar] [CrossRef] [PubMed]
- Eriksen, J.; Gustafsson, L.L.; Ateva, K.; Bastholm-Rahmner, P.; Ovesjo, M.L.; Jirlow, M.; Juhasz-Haverinen, M.; Larfars, G.; Malmstrom, R.E.; Wettermark, B.; et al. High adherence to the ‘Wise List’ treatment recommendations in Stockholm: A 15-year retrospective review of a multifaceted approach promoting rational use of medicines. BMJ Open 2017, 7, e014345. [Google Scholar] [CrossRef] [Green Version]
- Godman, B.; Fadare, J.; Kwon, H.Y.; Dias, C.Z.; Kurdi, A.; Dias Godói, I.P.; Kibuule, D.; Hoxha, I.; Opanga, S.; Saleem, Z.; et al. Evidence-based public policy making for medicines across countries: Findings and implications for the future. J. Comp. Eff. Res. 2021, 10, 1019–1052. [Google Scholar] [CrossRef]
- Colbeck, M.; Lockwood, C.; Peters, M.; Fulbrook, P.; McCabe, D. The effect of evidence-based, treatment-oriented, clinical practice guidelines on improving patient care outcomes: A systematic review protocol. JBI Database Syst. Rev. Implement. Rep. 2016, 14, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Almatar, M.; Peterson, G.M.; Thompson, A.; McKenzie, D.; Anderson, T.; Zaidi, S.T. Clinical Pathway and Monthly Feedback Improve Adherence to Antibiotic Guideline Recommendations for Community-Acquired Pneumonia. PLoS ONE 2016, 11, e0159467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakwatumbah, S.; Kibuule, D.; Godman, B.; Haakuria, V.; Kalemeera, F.; Baker, A.; Mubita, M. Compliance to guidelines for the prescribing of antibiotics in acute infections at Namibia’s national referral hospital: A pilot study and the implications. Expert Rev. Anti-Infect. Ther. 2017, 15, 713–721. [Google Scholar] [CrossRef] [Green Version]
- Elias, C.; Moja, L.; Mertz, D.; Loeb, M.; Forte, G.; Magrini, N. Guideline recommendations and antimicrobial resistance: The need for a change. BMJ Open 2017, 7, e016264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babarinde, O.S.; Labuschagne, Q.; Schellack, N.; Goff, B.A. Stop Waiting on the World to Change: Guiding Behavior to Improve Antibiotic. Pharmacy Practice News, 2018. Available online: https://www.pharmacypracticenews.com/Review-Articles/Article/04-18/Stop-Waiting-on-the-World-to-Change-Guiding-Behavior-To-Improve-Antibiotic-Stewardship/48356 (accessed on 4 November 2019).
- Feiring, E.; Walter, A.B. Antimicrobial stewardship: A qualitative study of the development of national guidelines for antibiotic use in hospitals. BMC Health Serv. Res. 2017, 17, 747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mpinda-Joseph, P.; Anand Paramadhas, B.D.; Reyes, G.; Maruatona, M.B.; Chise, M.; Monokwane-Thupiso, B.B.; Souda, S.; Tiroyakgosi, C.; Godman, B. Healthcare-associated infections including neonatal bloodstream infections in a leading tertiary hospital in Botswana. Hosp. Pract. (1995) 2019, 47, 203–210. [Google Scholar] [CrossRef] [Green Version]
- Schoonenboom, J.; Johnson, R.B. How to Construct a Mixed Methods Research Design. Koln. Z. Fur Soziologie Soz. 2017, 69, 107–131. [Google Scholar] [CrossRef] [PubMed]
- Mathers, N.; Fox, N.; Hunn, A. Surveys and Questionnaire Revision. The NIHR RDS for the East Midlands/Yorkshire & the Humber. 2009. Available online: https://www.rds-yh.nihr.ac.uk/wp-content/uploads/2013/05/12_Surveys_and_Questionnaires_Revision_2009.pdf (accessed on 26 September 2019).
- Kruger, D.; Dlamini, N.N.; Meyer, J.C.; Godman, B.; Kurdi, A.; Lennon, M.; Bennie, M.; Schellack, N. Development of a web-based application to improve data collection of antimicrobial utilization in the public health care system in South Africa. Hosp. Pract. 2021, 1–10. [Google Scholar] [CrossRef]
- Skosana, P.P.; Schellack, N.; Godman, B.; Kurdi, A.; Bennie, M.; Kruger, D.; Meyer, J.C. A point prevalence survey of antimicrobial utilisation patterns and quality indices amongst hospitals in South Africa; findings and implications. Expert Rev. Anti-Infect. Ther. 2021, 1–13. [Google Scholar] [CrossRef]
- Whitehead, B.; Owen, P.; Henshaw, L.; Beddingham, E.; Simmons, M. Supporting newly qualified nurse transition: A case study in a UK hospital. Nurse Educ. Today 2016, 36, 58–63. [Google Scholar] [CrossRef] [Green Version]
- Lincoln, Y.S.; Guba, E.G. Naturalistic Inquiry; Sage Publications: Newbury Park, CA, USA, 1985. [Google Scholar]
- Almalki, S. Integrating Quantitative and Qualitative Data in Mixed Methods Research—Challenges and Benefits. J. Educ. Learn. Arch. 2016, 5, 288–296. [Google Scholar] [CrossRef]
- Nyumba, T.O.; Wilson, K.; Derrick, C.J.; Mukherjee, N. The use of focus group discussion methodology: Insights from two decades of application in conservation. Methods Ecol. Evol. 2018, 9, 20–32. [Google Scholar] [CrossRef] [Green Version]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Vaismoradi, M.; Turunen, H.; Bondas, T. Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nurs. Health Sci. 2013, 15, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Richards, L. Handling Qualitative Data: A Practical Guide; Sage: London, UK, 2014; Available online: https://uk.sagepub.com/en-gb/eur/handling-qualitative-data/book241828 (accessed on 26 September 2019).
- Lowman, W. Active surveillance of hospital-acquired infections in South Africa: Implementation, impact and challenges. S. Afr. Med. J. 2016, 106, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schroeder, L.; Amukele, T.; Pai, M. Why the World Needs an Essential Diagnostic List. Forbes, 2016. Available online: https://www.forbes.com/sites/sciencebiz/2016/08/04/why-the-world-needs-an-essential-diagnostics-list/#40107fa14015 (accessed on 31 October 2019).



{kind=link}
{kind=link}
| Figure | Profession | Total; n (%) | |||
|---|---|---|---|---|---|
| Doctors | Pharmacists | Nursing | |||
| Community health centres | 2 | 3 | 4 | 9 (34.6%) | |
| Referral hospitals | District | 2 | 3 | - | 5 (19.2%) |
| Regional | - | 1 | 1 | 2 (7.7%) | |
| Provincial tertiary | 1 | 1 | - | 2 (7.7%) | |
| National central hospitals | - | 8 | - | 8 (30.8%) | |
| Total; n (%) | 5 (19.2%) | 16 (61.5%) | 5 (19.2%) | 26 | |
| Disciplines | Clinical Associate * | Medical | Microbiology | Nursing | Pharmacy | Expert | Undisclosed | Total |
| Number of participants | 2 (2.4%) | 18 (21.7%) | 4 (4.8%) | 20 (24.1%) | 28 (33.7%) | 9 (10.8%) | 2 (2.4%) | 83 |
| Duration in Current Position | ||||||||
| 1–4 years | 27 (32.5%) | 5–10 years | 18 (21.7%) | >10 years | 21 (25.3%) | Undisclosed | 17 (20.5%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Engler, D.; Meyer, J.C.; Schellack, N.; Kurdi, A.; Godman, B. Antimicrobial Stewardship Activities in Public Healthcare Facilities in South Africa: A Baseline for Future Direction. Antibiotics 2021, 10, 996. https://doi.org/10.3390/antibiotics10080996
Engler D, Meyer JC, Schellack N, Kurdi A, Godman B. Antimicrobial Stewardship Activities in Public Healthcare Facilities in South Africa: A Baseline for Future Direction. Antibiotics. 2021; 10(8):996. https://doi.org/10.3390/antibiotics10080996
Chicago/Turabian StyleEngler, Deirdré, Johanna Catharina Meyer, Natalie Schellack, Amanj Kurdi, and Brian Godman. 2021. "Antimicrobial Stewardship Activities in Public Healthcare Facilities in South Africa: A Baseline for Future Direction" Antibiotics 10, no. 8: 996. https://doi.org/10.3390/antibiotics10080996
APA StyleEngler, D., Meyer, J. C., Schellack, N., Kurdi, A., & Godman, B. (2021). Antimicrobial Stewardship Activities in Public Healthcare Facilities in South Africa: A Baseline for Future Direction. Antibiotics, 10(8), 996. https://doi.org/10.3390/antibiotics10080996