


The Real Practice Prescribing Antibiotics in Outpatients: A Failed Control Case Assessed through the Simulated Patient Method

 ,
,  ,
,
Abstract
:1. Introduction
2. Results
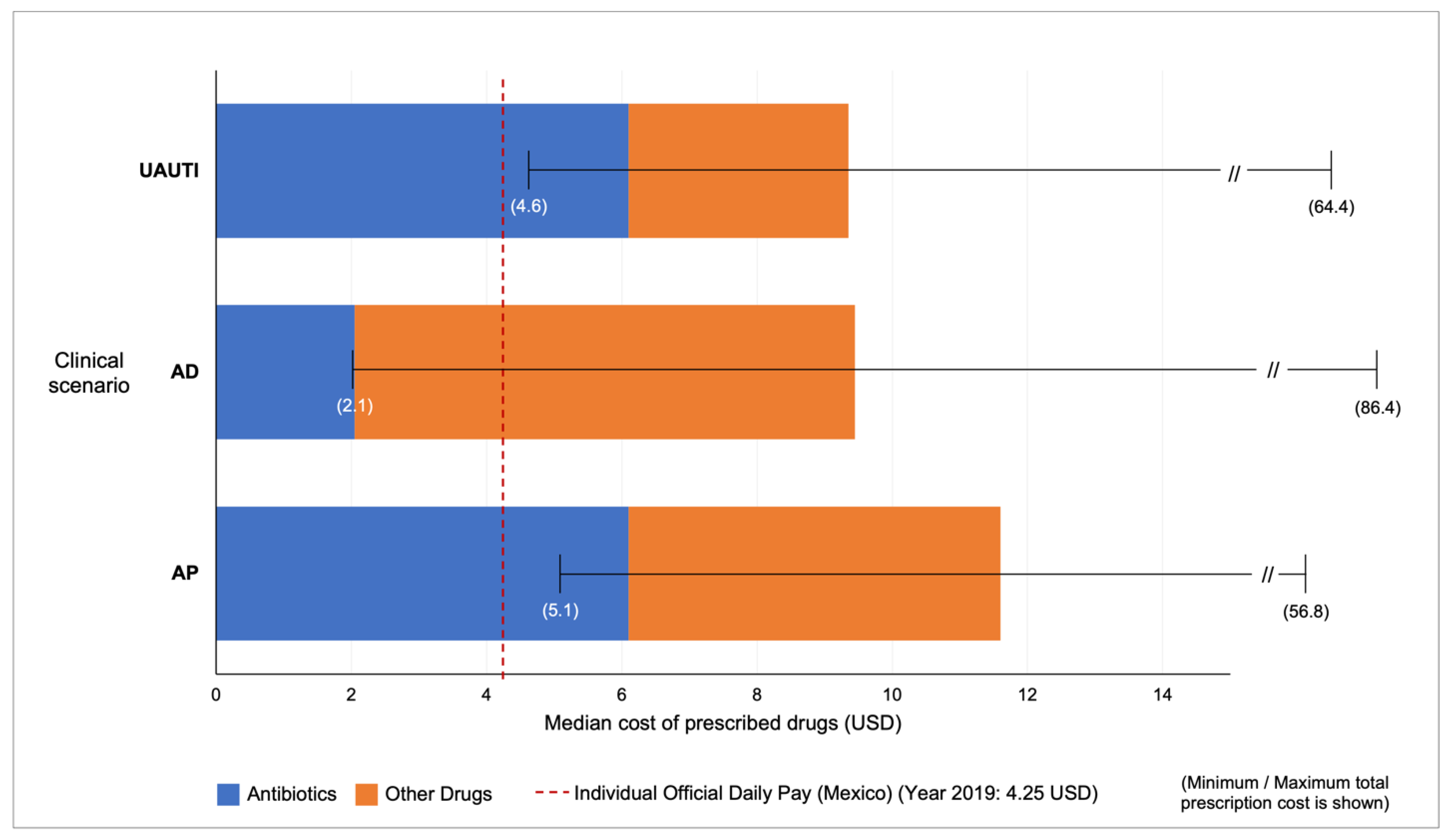
Costs
3. Discussion
4. Materials and Methods
4.1. Procedure
4.2. Sample Size
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gómez Dantés, O.; Sesma, S.; Becerril, V.M.; Knaul, F.M.; Arreola, H.; Frenk, J. Sistema de salud de México. Salud Pública Méx. 2011, 53, S220–S232. [Google Scholar]
- Valdespino, J.L.; Olaiz, G.; López-Barajas, M.P.; Mendoza, L.; Palma, O.; Velázquez, O.; Tapia, R.; Sepúlveda, J. Encuesta Nacional de Salud 2000. Tomo I. Vivienda, Población y Utilización de Servicios de Salud. Instituto Nacional de Salud Pública. 2003. Available online: https://ensanut.insp.mx/informes/ENSA_tomo1.pdf (accessed on 3 January 2022).
- Olaiz-Fernández, G.; Rivera-Dommarco, J.; Shamah-Levy, T.; Rojas, R.; Villalpando-Hernández, S.; Hernández-Avila, M.; Sepúlveda-Amor, J. Encuesta Nacional de Salud y Nutrición 2006. Instituto Nacional de Salud Pública. 2006. Available online: https://ensanut.insp.mx/informes/ensanut2006.pdf (accessed on 3 January 2022).
- Gutiérrez, J.P.; Rivera-Dommarco, J.; Shamah-Levy, T.; Villalpando-Hernández, S.; Franco, A.; Cuevas-Nasu, L.; Romero-Martínez, M.; Hernández-Ávila, M. Encuesta Nacional de Salud y Nutrición 2012. Resultados Nacionales. Instituto Nacional de Salud Pública. 2012. Available online: https://ensanut.insp.mx/informes/ENSANUT2012ResultadosNacionales.pdf (accessed on 3 January 2022).
- Chu, M.; Garcia-Cuellar, R. Farmacias Similares: Private and Public Health Care for the Base of the Pyramid in Mexico. Harvard Business School Case 307-092, January 2007. (Revised April 2011). Harvard Business School. Available online: https://hbsp.harvard.edu/product/307092-PDF-ENG (accessed on 3 January 2022).
- Comisión Federal Para la Protección Contra Riesgos Sanitarios (COFEPRIS); Secretaría de Salud. Avanza la Estrategia Para Regular Consultorios en Farmacias (Comunicado de Prensa, 29/Ene/2014). Available online: https://www.gob.mx/cofepris/prensa/avanza-la-estrategia-para-regular-consultorios-en-farmacias-62847 (accessed on 3 January 2022).
- Secretaría de Salud. Acuerdo por el que determinan los lineamientos a los que estará sujeta a la venta y dispensación de antibióticos. Diario Oficial de la Federación, 27 May 2010. [Google Scholar]
- Fundación Mexicana Para la Salud (FUNSALUD). Estudio Sobre la Práctica de la Atención Médica en Consultorios Médicos Adyacentes a Farmacias Privadas. FUNSALUD. 2014. Available online: http://funsalud.org.mx/portal/wp-content/uploads/2015/07/Informe-final-CAF-v300615-e-book.pdf (accessed on 3 January 2022).
- Lezama-Fernández, M.A. Consultorios adyacentes a farmacias privadas: Calidad de los servicios de salud y calidad de vida laboral (CAF). Rev. Conamed 2016, 21, 3–4. Available online: https://www.medigraphic.com/cgi-bin/new/resumen.cgi?IDARTICULO=79468 (accessed on 3 January 2022).
- Díaz-Portillo, S.P.; Idrovo, A.J.; Dreser, A.; Bonilla, F.R.; Matías-Juan, B.; Wirtz, V.J. Consultorios adyacentes a farmacias privadas en México: Infraestructura y características del personal médico y su remuneración. Salud Pública Méx. 2015, 57, 320–328. [Google Scholar]
- Perez-Cuevas, R.; Doubova, S.V.; Wirtz, V.J.; Servan-Mori, E.; Dreser, A.; Hernández-Ávila, M. Effects of the expansion of doctors’ offices adjacent to private pharmacies in Mexico: Secondary data analysis of a national survey. BMJ Open 2014, 4, e004669. [Google Scholar] [CrossRef]
- World Health Organization (WHO). The World Health Report 2006: Working Together for Health. WHO. Available online: https://apps.who.int/iris/handle/10665/43432 (accessed on 3 January 2022).
- Comisión Federal Para la Protección Contra Riesgos Sanitarios (COFEPRIS); Secretaría de Salud. Informe de Rendición de Cuentas de Conclusión de la Administración 2012–2018. Available online: http://sipot.cofepris.gob.mx/Archivos/juridico/COFE/Informe_Consolidado.pdf (accessed on 3 January 2022).
- Churchouse, C.; McCafferty, C. Standardized Patients Versus Simulated Patients: Is There a Difference? Clin. Simul. Nurs. 2012, 8, e363–e365. [Google Scholar] [CrossRef]
- Austin, Z.; Gregory, P.; Tabak, D. Simulated patients vs. standardized patients in objective structured clinical examinations. Am. J. Pharm. Educ. 2006, 70, 119. [Google Scholar] [CrossRef]
- Sylvia, S.; Shi, Y.; Xue, H.; Tian, X.; Wang, H.; Liu, Q.; Medina, A.; Rozelle, S. Survey using incognito standardized patients shows poor quality care in China’s rural clinics. Health Policy Plan 2015, 30, 322–333. [Google Scholar] [CrossRef] [PubMed]
- Ozuah, P.O.; Reznik, M. Using unannounced standardized patients to assess residents’ competency in asthma severity classification. Ambul. Pediatr. 2008, 8, 139–142. [Google Scholar] [CrossRef]
- Das, J.; Holla, A.; Das, V.; Mohanan, M.; Tabak, D.; Chan, B. In urban and rural India, a standardized patient study showed low levels of provider training and huge quality gaps. Health Aff. (Millwood) 2012, 31, 2774–2784. [Google Scholar] [CrossRef]
- Satyanarayana, S.; Kwan, A.; Daniels, B.; Subbaraman, R.; McDowell, A.; Bergkvist, S.; Das, R.K.; Das, V.; Das, J.; Pai, M. Use of standardised patients to assess antibiotic dispensing for tuberculosis by pharmacies in urban India: A cross-sectional study. Lancet Infect. Dis. 2016, 16, 1261–1268. [Google Scholar] [CrossRef]
- Miller, R.; Goodman, C. Do chain pharmacies perform better than independent pharmacies? Evidence from a standardised patient study of the management of childhood diarrhoea and suspected tuberculosis in urban India. BMJ Glob. Health 2017, 2, e000457. [Google Scholar] [CrossRef] [PubMed]
- Howley, L.; Szauter, K.; Perkowski, L.; Clifton, M.; McNaughton, N.; on behalf of the Association of Standardized Patient Educators (ASPE). Quality of standardised patient research reports in the medical education literature: Review and recommendations. Med. Educ. 2008, 42, 350–358. [Google Scholar] [CrossRef] [PubMed]
- Centro Nacional de Excelencia Tecnológica en Salud (CENETEC); Secretaría de Salud. Atención, Diagnóstico y Tratamiento de Diarrea Aguda en Adultos en el Primer Nivel de Atención (Guía de Referencia Rápida) (05 de octubre de 2015). Available online: https://www.gob.mx/salud/documentos/atencion-diagnostico-y-tratamiento-de-diarrea-aguda-en-adultos-en-el-primer-nivel-de-atencion-guia-de-referencia-rapida (accessed on 3 January 2022).
- Centro Nacional de Excelencia Tecnológica en Salud (CENETEC); Secretaría de Salud. Guía de Práctica Clínica. Diagnóstico y tratamiento de Faringoamigdalitis Aguda. Evidencias y Recomendaciones (2009). Available online: http://www.cenetec-difusion.com/CMGPC/IMSS-073-08/ER.pdf (accessed on 3 January 2022).
- Centro Nacional de Excelencia Tecnológica en Salud (CENETEC); Secretaría de Salud. Guía de Práctica Clínica. Diagnóstico y Tratamiento de la Infección Aguda, no Complicada del Tracto Urinario en la Mujer. Evidencias y Recomendaciones (2009). Available online: http://www.cenetec-difusion.com/CMGPC/IMSS-077-08/ER.pdf (accessed on 3 January 2022).
- Smith, D.R.M.; Dolk, F.C.K.; Pouwels, K.B.; Christie, M.; Robotham, J.; Smieszek, T. Defining the appropriateness and inappropriateness of antibiotic prescribing in primary care. J. Antimicrob. Chemother. 2018, 73 (Suppl. S2), ii11–ii18. [Google Scholar] [CrossRef]
- Fleming-Dutra, K.E.; Hersh, A.L.; Shapiro, D.J.; Bartoces, M.; Enns, E.A.; File, T.M., Jr.; Finkelstein, J.A.; Gerber, J.S.; Hyun, D.Y.; Linder, J.A.; et al. Prevalence of Inappropriate Antibiotic Prescriptions Among US Ambulatory Care Visits, 2010–2011. J. Am. Med. Assoc. 2016, 315, 1864–1873. [Google Scholar] [CrossRef]
- Kotwani, A.; Chaudhury, R.R.; Holloway, K. Antibiotic-prescribing practices of primary care prescribers for acute diarrhea in New Delhi, India. Value Health 2012, 15 (Suppl. S1), S116–S119. [Google Scholar] [CrossRef]
- Supcharassaeng, S.; Suankratay, C. Antibiotic prescription for adults with acute diarrhea at King Chulalongkorn Memorial Hospital, Thailand. J. Med. Assoc. Thail. 2011, 94, 545–550. [Google Scholar]
- Pérez-Vega, A.I. Cumplimento Normativo en el Control de la Venta y la Dispensación de Antibióticos en Farmacias y Perspectivas en México en Combate a la Resistencia Antimicrobiana (RAM). Boletin. Conamed. 2018, 4, 17–20. Available online: http://www.conamed.gob.mx/gobmx/boletin/pdf/boletin22/Cumplimento.pdf (accessed on 3 January 2022).
- Leyva-Flores, R.; Bronfman, M.; Erviti-Erice, J. Simulated clients in drugstores: Prescriptive behaviour of drugstore attendants. J. Soc. Adm. Pharm. 2000, 17, 151–158. [Google Scholar]
- Leyva, R.; Erviti, J.; Bronfman, M.; Gassman, N. Consumo de medicamentos en farmacias privadas: Los medicamentos inseguros. In Coords. Salud, Cambio Social y Política. Perspectivas Desde América Latina; Bronfman, M., Castro, R., Eds.; Edamex: Mexico City, Mexico, 1999; pp. 493–508. [Google Scholar]
- Li, J.; Song, X.; Yang, T.; Chen, Y.; Gong, Y.; Yin, X.; Lu, Z. A Systematic Review of Antibiotic Prescription Associated with Upper Respiratory Tract Infections in China. Medicine 2016, 95, e3587. [Google Scholar] [CrossRef]
- McKay, R.; Mah, A.; Law, M.R.; McGrail, K.; Patrick, D.M. Systematic Review of Factors Associated with Antibiotic Prescribing for Respiratory Tract Infections. Antimicrob. Agents Chemother. 2016, 60, 4106–4118. [Google Scholar] [CrossRef]
- Mohsen, S.; Dickinson, J.A.; Somayaji, R. Update on the adverse effects of antimicrobial therapies in community practice. Can. Fam. Physician 2020, 66, 651–659. [Google Scholar] [PubMed]


{kind=link}
| Antimicrobial | n | % |
|---|---|---|
| Aminopenicillin/Benzylpenicillin | 30 | 29.7 |
| Macrolide | 17 | 16.8 |
| Cephalosporins | 12 | 11.8 |
| Quinolones | 9 | 8.9 |
| Clindamycin | 1 | 0.9 |
| Fosfomycin | 1 | 0.9 |
| Total with at least one antibiotic | 70 | 69.3 |
| Amantadine | 25 | 24.7 |
| No antibiotic | 11 | 10.8 |
| Antimicrobial | n | % |
|---|---|---|
| TMP/SMZ | 35 | 27.6 |
| Quinolones | 26 | 20.5 |
| Aminopenicillin | 4 | 3.1 |
| Cephalosporins | 3 | 2.4 |
| Aminoglycoside | 3 | 2.4 |
| Tetracycline | 2 | 1.6 |
| Chloramphenicol | 1 | 0.8 |
| Macrolide | 1 | 0.8 |
| Total with at least one antibiotic | 75 | 59 |
| At least one antiparasitic drug | 28 | 22 |
| ‘Intestinal antiseptics’ | 14 | 11 |
| No antibiotic | 23 | 18.1 |
| Antimicrobial | n | % |
|---|---|---|
| Quinolones | 38 | 73 |
| Nitrofurantoin | 8 | 15.4 |
| TMP/SMZ | 5 | 9.6 |
| Cephalosporins | 2 | 3.8 |
| Aminopenicillin | 1 | 1.9 |
| Aminoglycoside | 2 | 3.8 |
| Macrolide | 1 | 1.9 |
| Total with at least one antibiotic | 51 | 98 |
| No antibiotic | 1 | 1.9 |
| Clinical Scenario | Symptoms | Management |
|---|---|---|
| Acute pharyngitis (AP) | -Sore throat -Dry cough -Runny nose -Conjunctival irritation (no secretion) -No fever Onset of symptoms: two days | Symptomatic treatment: paracetamol 500 mg orally every 8 h for 3–5 days or ;non-steroidal anti-inflammatory orally every 12 h for 3–5 days |
| Acute diarrhoea (AD) | -Abdominal pain -Loose stools (4–5 per day without mucus or blood) -Occasional nausea -No fever Onset of symptoms: 1 day | Oral rehydration solutions Astringent diet Watch for alarm signs of dehydration |
| Uncomplicated acute urinary tract infection in adult women (UAUTI) | -Dysuria -Urinary frequency and urgency -Abdominal discomfort -No fever -Onset of symptoms: 2 days | 1st line treatment: (a) trimethoprim/sulfamethoxazole 160 mg/800 mg, twice daily for three days or nitrofurantoin 100 mg twice daily for 7 days. If after 3 day symptoms persist, request urine culture and initiate ciprofloxacin 250 mg twice daily for 3 days. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miranda-Novales, M.G.; Flores-Moreno, K.; Rodríguez-Álvarez, M.; López-Vidal, Y.; Soto-Hernández, J.L.; Solórzano Santos, F.; Ponce-de-León-Rosales, S. The Real Practice Prescribing Antibiotics in Outpatients: A Failed Control Case Assessed through the Simulated Patient Method. Antibiotics 2023, 12, 915. https://doi.org/10.3390/antibiotics12050915
Miranda-Novales MG, Flores-Moreno K, Rodríguez-Álvarez M, López-Vidal Y, Soto-Hernández JL, Solórzano Santos F, Ponce-de-León-Rosales S. The Real Practice Prescribing Antibiotics in Outpatients: A Failed Control Case Assessed through the Simulated Patient Method. Antibiotics. 2023; 12(5):915. https://doi.org/10.3390/antibiotics12050915
Chicago/Turabian StyleMiranda-Novales, María Guadalupe, Karen Flores-Moreno, Mauricio Rodríguez-Álvarez, Yolanda López-Vidal, José Luis Soto-Hernández, Fortino Solórzano Santos, and Samuel Ponce-de-León-Rosales. 2023. "The Real Practice Prescribing Antibiotics in Outpatients: A Failed Control Case Assessed through the Simulated Patient Method" Antibiotics 12, no. 5: 915. https://doi.org/10.3390/antibiotics12050915
APA StyleMiranda-Novales, M. G., Flores-Moreno, K., Rodríguez-Álvarez, M., López-Vidal, Y., Soto-Hernández, J. L., Solórzano Santos, F., & Ponce-de-León-Rosales, S. (2023). The Real Practice Prescribing Antibiotics in Outpatients: A Failed Control Case Assessed through the Simulated Patient Method. Antibiotics, 12(5), 915. https://doi.org/10.3390/antibiotics12050915