
Trends in Antibiotic-Resistant Bacteria Isolated from Screening Clinical Samples in a Tertiary Care Hospital over the 2018–2022 Period


Abstract
:1. Introduction
2. Results
2.1. Number of Positive Patients, Isolates, Time to First Positive Screening, and Length of Carriage
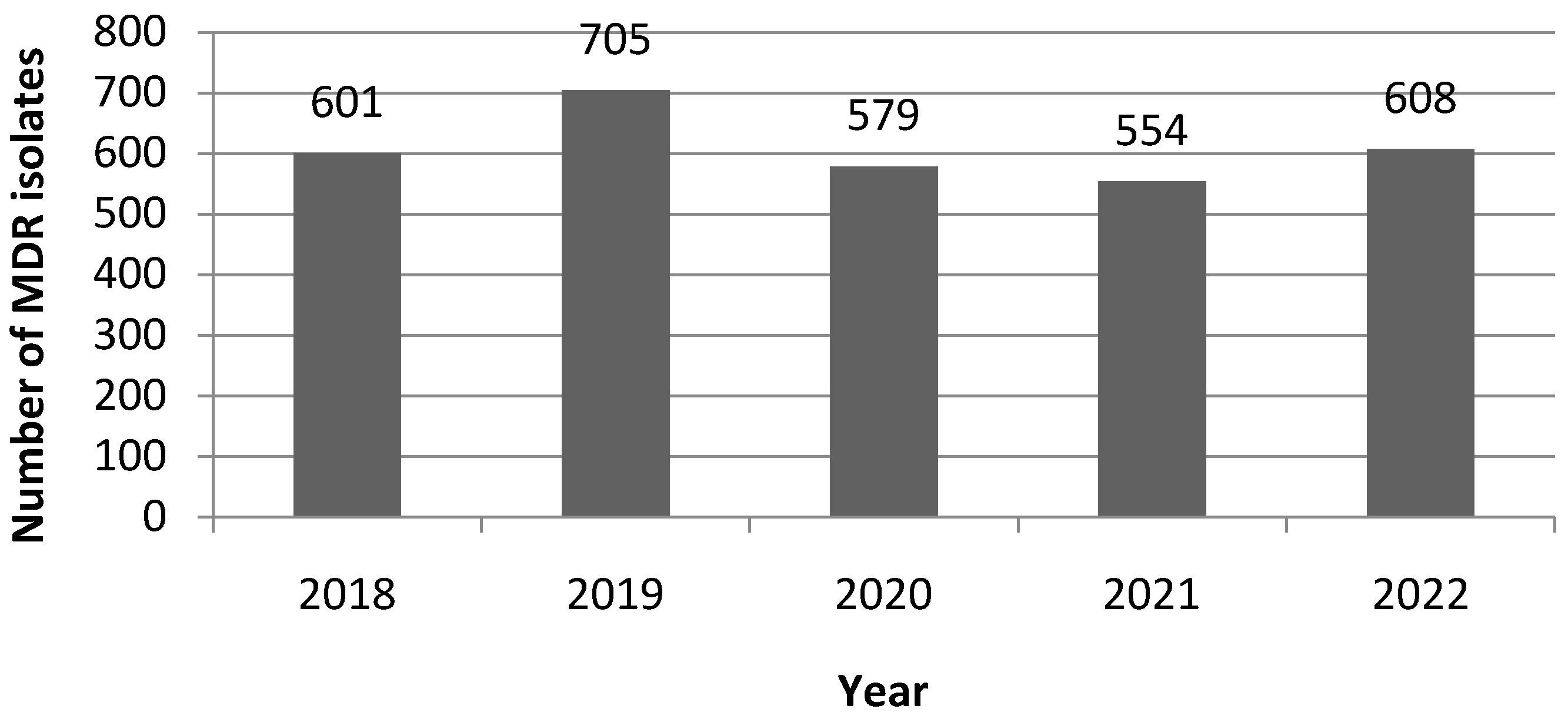
2.2. Time-Dependent Variations in the Number of MDR Isolates, MDR, and Carbapenemase Types
2.3. Species Isolation and Resistance Frequencies
2.4. MDR Bacteria Isolation According to the Type of Hospitalization Ward
3. Discussion
4. Materials and Methods
4.1. Study Design and Data Collection
4.2. MDR Screening Policy
4.3. Definitions and Outcomes
4.4. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- O’Neill, J. Tackling Drug-Resistant Infections Globally: Final Report and Recommendations. Available online: https://amr-review.org/sites/default/files/160525_Final%20paper_with%20cover.pdf (accessed on 14 July 2023).
- WHO. Guidelines on Core Components of Infection Prevention and Control Programmes at the National and Acute Health Care Facility Level. Available online: https://www.who.int/publications/i/item/9789241549929 (accessed on 10 July 2023).
- WHO Publishes List of Bacteria for Which New Antibiotics Are Urgently Needed. Available online: https://www.who.int/en/news-room/detail/27-02-2017-who-publishes-list-of-bacteria-for-which-new-antibiotics-are-urgently-needed (accessed on 10 July 2023).
- Bonten, M.J.; Weinstein, R.A. The role of colonization in the pathogenesis of nosocomial infections. Infect. Control Hosp. Epidemiol. 1996, 17, 193–200. [Google Scholar] [CrossRef]
- Galoisy-Guibal, L.; Soubirou, J.L.; Desjeux, G.; Dusseau, J.Y.; Eve, O.; Escarment, J.; Ecochard, R. Screening for multidrug-resistant bacteria as a predictive test for subsequent onset of nosocomial infection. Infect. Control Hosp. Epidemiol. 2006, 27, 1233–1241. [Google Scholar] [CrossRef] [PubMed]
- Willems, R.P.J.; van Dijk, K.; Vehreschild, M.J.G.T.; Biehl, L.M.; Ket, J.C.F.; Remmelzwaal, S.; Vandenbroucke-Grauls, C.M.J.E. Incidence of infection with multidrug-resistant Gram-negative bacteria and vancomycin-resistant enterococci in carriers: A systematic review and meta-regression analysis. Lancet Infect Dis. 2023, 23, 719–731. [Google Scholar] [CrossRef] [PubMed]
- Magiorakos, A.P.; Burns, K.; Rodríguez Baño, J.; Borg, M.; Daikos, G.; Dumpis, U.; Lucet, J.C.; Moro, M.L.; Tacconelli, E.; Simonsen, G.S.; et al. Infection prevention and control measures and tools for the prevention of entry of carbapenem-resistant Enterobacteriaceae into healthcare settings: Guidance from the European Centre for Disease Prevention and Control. Antimicrob. Resist. Infect. Control 2017, 6, 113. [Google Scholar] [CrossRef]
- Arzilli, G.; Scardina, G.; Casigliani, V.; Petri, D.; Porretta, A.; Moi, M.; Lucenteforte, E.; Rello, J.; Lopalco, P.; Baggiani, A.; et al. Screening for antimicrobial-resistant Gram-negative bacteria in hospitalised patients, and risk of progression from colonisation to infection: Systematic review. J. Infect. 2022, 84, 119–130. [Google Scholar] [CrossRef] [PubMed]
- CDC’s Core Infection Prevention and Control Practices for Safe Healthcare Delivery in All Settings. Available online: https://www.cdc.gov/infectioncontrol/guidelines/core-practices/index.html (accessed on 10 July 2023).
- Guidance: Infection Prevention and Control Measures for Healthcare Workers in All Healthcare Settings. Carbapenem-Resistant Gram-Negative Bacilli. Available online: https://www.canada.ca/content/dam/phac-aspc/migration/phac-aspc/nois-sinp/guide/ipcm-mpci/pdf/guide-eng.pdf (accessed on 10 July 2023).
- Ministry of Health and Family Welfare Government of India. National Guidelines for Infection Prevention and Control in Healthcare Facilities. 2020. Available online: https://www.mohfw.gov.in/pdf/National%20Guidelines%20for%20IPC%20in%20HCF%20-%20final%281%29.pdf (accessed on 10 July 2023).
- Haut Conseil de la Santé Publique. Actualisation des Recommandations Relatives à la Maîtrise de la Diffusion des Bactéries Hautement Résistantes aux Antibiotiques Emergentes (BHRe). 2019. Available online: https://www.hcsp.fr/explore.cgi/avisrapportsdomaine?clefr=758 (accessed on 10 July 2023).
- Société Française d’Hygiène Hospitalière. Recommandations nationales, Prévention de la transmission croisée: Précautions complémentaires contact, Consensus formalisé d’experts, Avril 2009. Hygiènes 2009, XVII, 81–138. [Google Scholar]
- Lai, C.C.; Chen, S.Y.; Ko, W.C.; Hsueh, P.R. Increasedantimicrobialresistanceduring the COVID-19 pandemic. Int. J. Antimicrob. Agents. 2021, 57, 106324. [Google Scholar] [CrossRef]
- Bedenić, B.; Luxner, J.; Car, H.; Sardelić, S.; Bogdan, M.; Varda-Brkić, D.; Šuto, S.; Grisold, A.; Beader, N.; Zarfel, G. Emergence and spread of Enterobacterales with multiple carbapenemases after COVID-19 pandemic. Pathogens 2023, 12, 677. [Google Scholar] [CrossRef]
- European Center for Disease Prevention and Control. Antimicrobial Resistance Surveillance in Europe 2022–2020 Data 2022. Available online: https://www.ecdc.europa.eu/en/publications-data/antimicrobial-resistance-surveillance-europe-2022-2020-data (accessed on 15 July 2023).
- Araos, R.; Smith, R.M.; Styczynski, A.; Sánchez, F.; Acevedo, J.; Maureira, L.; Paredes, C.; González, M.; Rivas, L.; Spencer-Sandino, M.; et al. High burden of intestinal colonization with antimicrobial-resistant bacteria in Chile: An antibiotic resistance in communities and hospitals (ARCH) study. Clin. Infect. Dis. 2023, 77, S75–S81. [Google Scholar] [CrossRef]
- Gales, A.C.; Stone, G.; Sahm, D.F.; Wise, M.G.; Utt, E. Incidence of ESBLs and carbapenemases among Enterobacterales and carbapenemases in Pseudomonas aeruginosa isolates collected globally: Results from ATLAS 2017–2019. J. Antimicrob. Chemother. 2023, 78, 1606–1615. [Google Scholar] [CrossRef]
- Hadjirin, N.F.; van Tonder, A.J.; Blane, B.; Lees, J.A.; Kumar, N.; Delappe, N.; Brennan, W.; McGrath, E.; Parkhill, J.; Cormican, M.; et al. Dissemination of carbapenemase-producing Enterobacterales in Ireland from 2012 to 2017: A retrospective genomic surveillance study. Microb. Genom. 2023, 9, mgen000924. [Google Scholar] [CrossRef]
- Nobrega, D.; Peirano, G.; Matsumura, Y.; Pitout, J.D.D. Molecular epidemiology of global carbapenemase-producing Citrobacter spp. (2015–2017). Microbiol. Spectr. 2023, 11, e0414422. [Google Scholar] [CrossRef] [PubMed]
- Hamerlinck, H.; Aerssens, A.; Boelens, J.; Dehaene, A.; McMahon, M.; Messiaen, A.S.; Vandendriessche, S.; Velghe, A.; Leroux-Roels, I.; Verhasselt, B. Sanitary installations and wastewater plumbing as reservoir for the long-term circulation and transmission of carbapenemase producing Citrobacter freundii clones in a hospital setting. Antimicrob. Resist. Infect. Control 2023, 12, 58. [Google Scholar] [CrossRef] [PubMed]
- Mullié, C. Carbapenem-resistant Acinetobacter baumannii spread in Amiens University Hospital, France. J. Prev. Infect. Control 2018, 4, 14–15. [Google Scholar] [CrossRef]
- Bezabih, Y.M.; Bezabih, A.; Dion, M.; Batard, E.; Teka, S.; Obole, A.; Dessalegn, N.; Enyew, A.; Roujeinikova, A.; Alamneh, E.; et al. Comparison of the global prevalence and trend of human intestinal carriage of ESBL-producing Escherichia coli between healthcare and community settings: A systematic review and meta-analysis. JAC Antimicrob. Resist. 2022, 4, dlac048. [Google Scholar] [CrossRef]
- Ling, W.; Peri, A.M.; Furuya-Kanamori, L.; Harris, P.N.A.; Paterson, D.L. Carriage duration and household transmission of Enterobacteralesproducing extended-spectrum beta-lactamase in the community: A systematic review and meta-analysis. Microb. Drug Resist. 2022, 28, 795–805. [Google Scholar] [CrossRef]
- Hopkins, K.L.; Ellaby, N.; Ellington, M.J.; Doumith, M.; Mustafa, N.; Meunier, D.; Woodford, N. Diversity of carbapenemase-producing Enterobacterales in England as revealed by whole-genome sequencing of isolates referred to a national reference laboratory over a 30-month period. J. Med. Microbiol. 2022, 71, 001518. [Google Scholar] [CrossRef]
- Hernández-García, M.; García-Castillo, M.; Bou, G.; Cercenado, E.; Delgado-Valverde, M.; Oliver, A.; Pitart, C.; Rodríguez-Lozano, J.; Tormo, N.; Melo-Cristino, J.; et al. Imipenem-relebactam susceptibility in Enterobacterales isolates recovered from ICU patients from Spain and Portugal (SUPERIOR and STEP Studies). Microbiol. Spectr. 2022, 10, e0292722. [Google Scholar] [CrossRef]
- Martirosov, D.M.; Lodise, T.P. Emerging trends in epidemiology and management of infections caused by carbapenem-resistant Enterobacteriaceae. Diagn. Microbiol. Infect. Dis. 2016, 85, 266–275. [Google Scholar] [CrossRef]
- Mullié, C.; Lemonnier, D.; Adjidé, C.C.; Maizel, J.; Mismacque, G.; Cappe, A.; Carles, T.; Pierson-Marchandise, M.; Zerbib, Y. Nosocomial outbreak of monoclonal VIM carbapenemase-producing Enterobacter cloacae complex in an intensive care unit during the COVID-19 pandemic: An integrated approach. J. Hosp. Infect. 2022, 120, 48–56. [Google Scholar] [CrossRef]
- Neidhöfer, C.; Buechler, C.; Neidhöfer, G.; Bierbaum, G.; Hannet, I.; Hoerauf, A.; Parčina, M. Global distribution patterns of carbapenemase-encoding bacteria in a new light: Clues on a role for ethnicity. Front. Cell. Infect. Microbiol. 2021, 11, 659753. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Patients Number (%) | Time to First Positive Screening (Days) | Length of Carriage (Days) |
|---|---|---|---|
| 2018 | 534 (21.9) | 3 [1–10] 1 | 15 [7–34.75] 1 |
| 2019 | 570 (23.3) | 3 [1–11] | 14 [7–35] |
| 2020 | 457 (18.7) | 4 [1–13] | 14.5 [7–35.75] |
| 2021 | 420 (17.2) | 3 [1–10] | 13 [7–35] |
| 2022 | 461(18.9) | 4 [2–12] | 15 [7–45.75] |
| Total | 2442 (100) | 3 [1–11] | 19 [7–70] |
| Species | Time to Positivity 1 | Total 1 | |
|---|---|---|---|
| ≤48 h | >48 h | ||
| C. freundii | 1.6 * (7.2) | 3.3 * (11.4) | 2.6 (10.3) |
| E. cloacae complex | 4.0 ** (7.2 $) | 11.4 ** (18.8 $) | 8.4 (15.7) |
| E. coli | 54.1 ** (40 £) | 30.9 ** (20.1 £) | 40.4 (25.5) |
| K. pneumoniae | 21.4 ** (36.4) | 37.1 ** (34.9) | 30.6 (35.3) |
| Other enterobacterales | 2.2 *** (3.6) | 4.1 *** (9.4) | 3.3 (7.8) |
| Total enterobacterales | 83.3 † (94.5) | 86.7 † (94.6) | 85.3 (94.6) |
| A. baumannii2 | 1.0 ** (1.8) | 4.0 ** (5.4) | 2.8 (4.4) |
| P. aeruginosa | 0.1 (1.8) | 0.1 (0) | 0.1 (0.5) |
| P. putida | 0.1 (1.8) | 0 (0) | 0.1 (0.5) |
| E. faecium | 0.2 | 0.2 | 0.2 |
| S. aureus | 15.3 ** | 8.9 ** | 11.5 |
| Total | 100 (100) | 100 (100) | 100 (100) |
| Species | Proportion (n) a | Median b | Interquartile Range b | |
|---|---|---|---|---|
| All wards | Acinetobacter baumannii | 2.8 (80) | 14.5 | 6–25.25 |
| Citrobacter freundii | 2.6 (73) | 10 | 3–15 | |
| Enterobacter cloacae complex | 8.4 (238) | 10 | 3–23 | |
| Escherichia coli | 40.4 (1148) | 2 | 1–5 | |
| Klebsiella pneumoniae | 30.8 (875) | 7 | 2–16 | |
| Staphylococcus aureus | 11.5 (327) | 2 | 1–4 | |
| High-risk wards | Acinetobacter baumannii | 3.3 (53) | 18 * | 8–29 |
| Citrobacter freundii | 1.6 (26) † | 10.5 | 2–19.25 | |
| Enterobacter cloacae complex | 10.0 (159) ‡ | 11 | 4–23 | |
| Escherichia coli | 36.4 (581) £ | 2 | 1–6 | |
| Klebsiella pneumoniae | 31.6 (505) | 8 ** | 3–17 | |
| Staphylococcus aureus | 13.5 (216) £ | 2 | 1–4 | |
| Medium/Low-risk wards | Acinetobacter baumannii | 2.2 (27) | 8 * | 3.5–17 |
| Citrobacter freundii | 3.8 (47) † | 8 | 3–14.5 | |
| Enterobacter cloacae complex | 6.3 (79) ‡ | 8 | 2–18 | |
| Escherichia coli | 45.5 (567) £ | 2 | 1–5 | |
| Klebsiella pneumoniae | 29.7 (370) | 5 ** | 2–13.75 | |
| Staphylococcus aureus | 8.9 (111) £ | 2 | 1–4.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lemonnier, D.; Machuel, M.; Obin, O.; Outurquin, G.; Adjidé, C.; Mullié, C. Trends in Antibiotic-Resistant Bacteria Isolated from Screening Clinical Samples in a Tertiary Care Hospital over the 2018–2022 Period. Antibiotics 2023, 12, 1314. https://doi.org/10.3390/antibiotics12081314
Lemonnier D, Machuel M, Obin O, Outurquin G, Adjidé C, Mullié C. Trends in Antibiotic-Resistant Bacteria Isolated from Screening Clinical Samples in a Tertiary Care Hospital over the 2018–2022 Period. Antibiotics. 2023; 12(8):1314. https://doi.org/10.3390/antibiotics12081314
Chicago/Turabian StyleLemonnier, Delphine, Marine Machuel, Odile Obin, Gaëtan Outurquin, Crespin Adjidé, and Catherine Mullié. 2023. "Trends in Antibiotic-Resistant Bacteria Isolated from Screening Clinical Samples in a Tertiary Care Hospital over the 2018–2022 Period" Antibiotics 12, no. 8: 1314. https://doi.org/10.3390/antibiotics12081314
APA StyleLemonnier, D., Machuel, M., Obin, O., Outurquin, G., Adjidé, C., & Mullié, C. (2023). Trends in Antibiotic-Resistant Bacteria Isolated from Screening Clinical Samples in a Tertiary Care Hospital over the 2018–2022 Period. Antibiotics, 12(8), 1314. https://doi.org/10.3390/antibiotics12081314