
Effects of Exercise during Pregnancy on Postpartum Depression: A Systematic Review of Meta-Analyses

 ,
, 
 ,
,  ,
, 

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
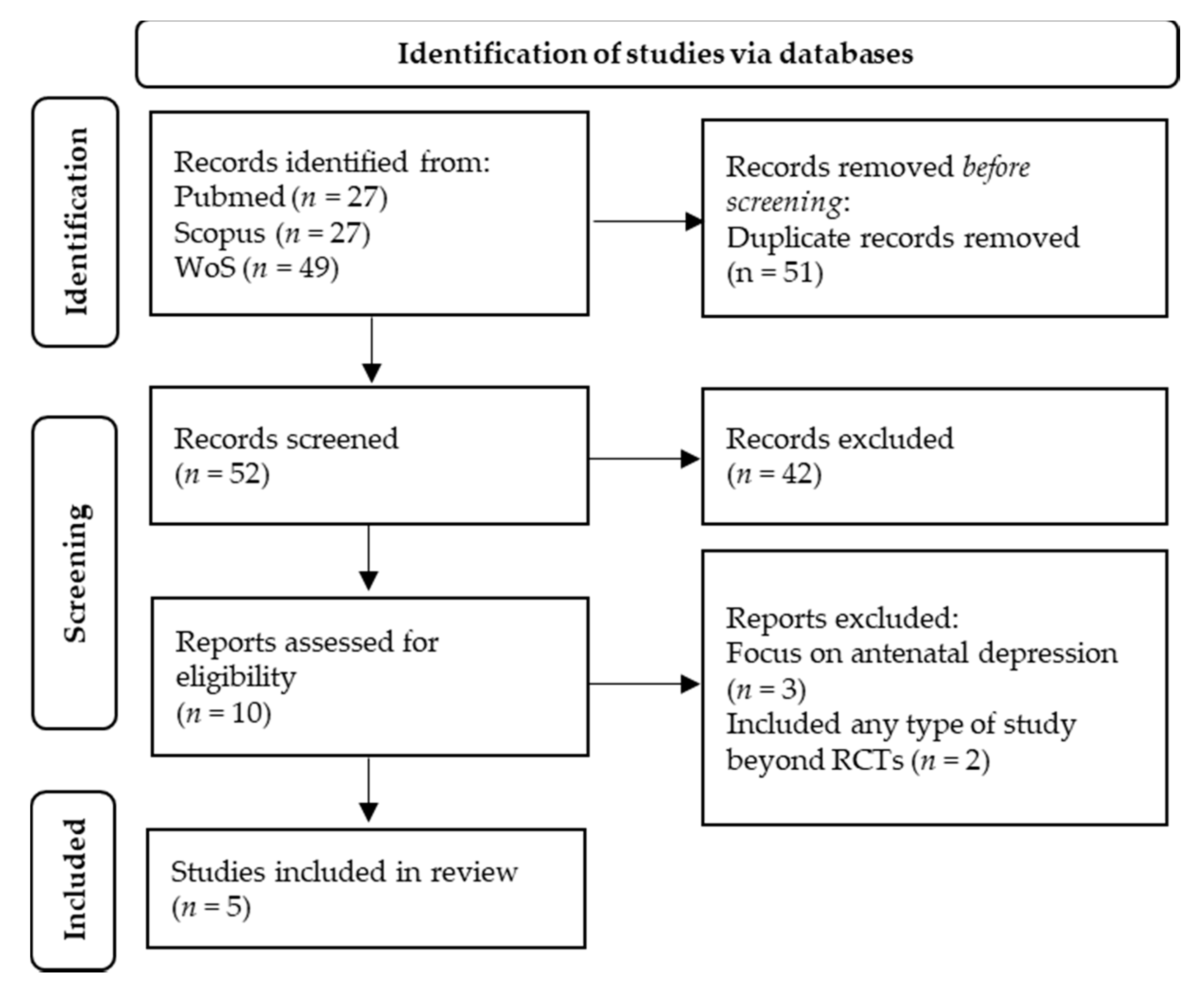
2.1. Literature Search
2.2. Eligibility Criteria
2.3. Quality Assessment
2.4. Data Extraction
2.5. Statistical Analysis
3. Results
3.1. Included Meta-Analyses
3.2. Characteristics of Meta-Analyses
3.2.1. Population
- (a)
- primiparous or multiparous postnatal women [30].
- (b)
- women who were between 4 weeks and 18 months postpartum [35].
- (c)
- postpartum women with and without depression [32].
- (d)
- women up to 1 year postpartum [33].
- (e)
- pregnant women with a single foetus and an uncomplicated pregnancy, or women who had a child aged between 6 weeks and 18 months [34].
3.2.2. Intervention
3.2.3. Comparison
3.2.4. Outcomes Measure
3.2.5. Adverse Events
3.3. Methodological Quality
3.4. Quality of Evidence
3.5. Results of Individual Meta-Analyses
3.6. Subgroup Analyses
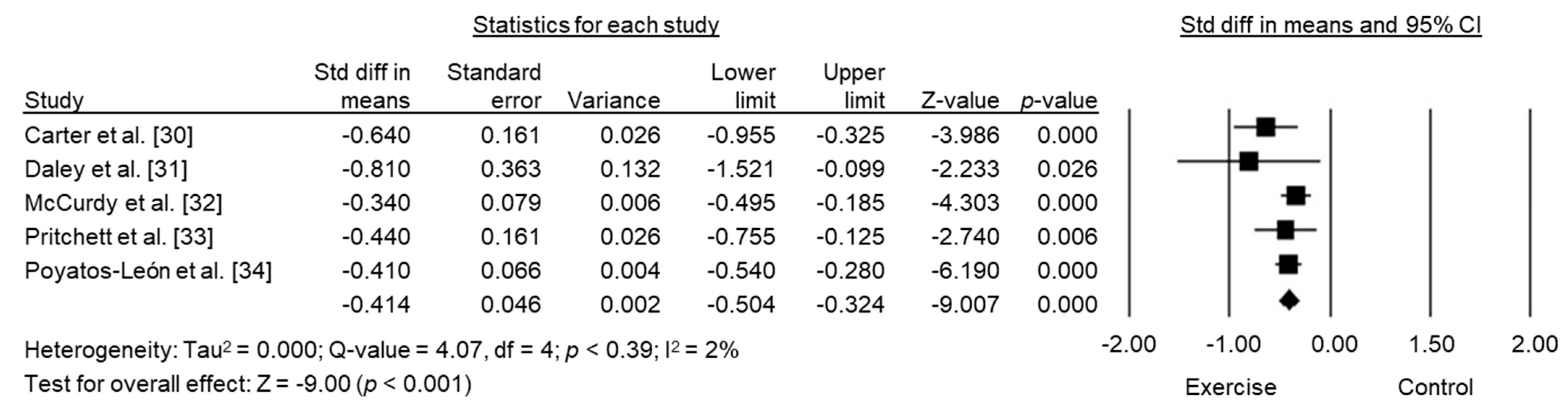
3.7. Pooled Summary SMD across Meta-Analyses
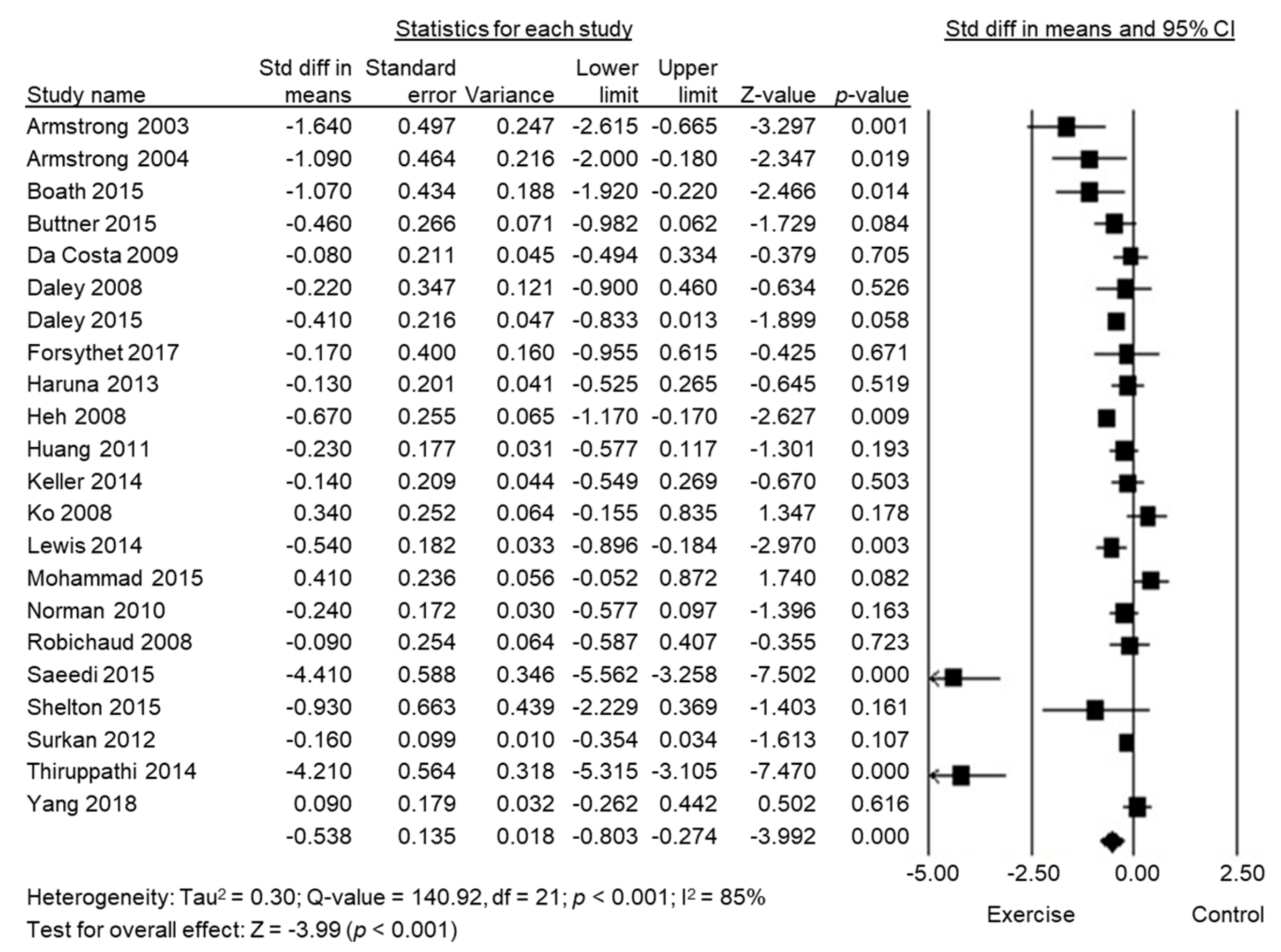
3.8. Pooled Summary SMD across Studies without Overlap
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gavin, N.I.; Gaynes, B.N.; Lohr, K.N.; Meltzer-Brody, S.; Gartlehner, G.; Swinson, T. Perinatal depression: A systematic review of prevalence and incidence. Obstet. Gynecol. 2005, 106, 1071–1083. [Google Scholar] [CrossRef]
- Woody, C.A.; Ferrari, A.J.; Siskind, D.J.; Whiteford, H.A.; Harris, M.G. A systematic review and meta-regression of the prevalence and incidence of perinatal depression. J. Affect. Disord. 2017, 219, 86–92. [Google Scholar] [CrossRef] [Green Version]
- Gaynes, B.N.; Gavin, N.; Meltzer-Brody, S.; Lohr, K.N.; Swinson, T.; Gartlehner, G.; Brody, S.; Miller, W.C. Perinatal Depression: Prevalence, Screening Accuracy, and Screening Outcomes: Evidence Report/Technology Assessment, Number 119. PsycEXTRA Dataset 2005, 2005, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Klein, M.H.; Essex, M.J. Pregnant or depressed? The effect of overlap between symptoms of depression and somatic complaints of pregnancy on rates of major depression in the second trimester. Depression 1994, 2, 308–314. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Logsdon, M.C.; Wisner, K.L.; Pinto-Foltz, M.D. The Impact of Postpartum Depression on Mothering. J. Obstet. Gynecol. Neonatal Nurs. 2006, 35, 652–658. [Google Scholar] [CrossRef]
- Cornish, A.; McMahon, C.; Ungerer, J.; Barnett, B.; Kowalenko, N.; Tennant, C. Postnatal depression and infant cognitive and motor development in the second postnatal year: The impact of depression chronicity and infant gender. Infant Behav. Dev. 2005, 28, 407–417. [Google Scholar] [CrossRef]
- Sanger, C.; Iles, J.; Andrew, C.S.; Ramchandani, P. Associations between postnatal maternal depression and psychological outcomes in adolescent offspring: A systematic review. Arch. Women’s Ment. Health 2015, 18, 147–162. [Google Scholar] [CrossRef] [PubMed]
- Iliadis, S.I.; Skalkidou, A.; Ranstrand, H.; Georgakis, M.K.; Axfors, C.; Papadopoulos, F.C. Self-Harm Thoughts Postpartum as a Marker for Long-Term Morbidity. Front. Public Health 2018, 6, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wisner, K.L.; Sit, D.K.Y.; McShea, M.C.; Rizzo, D.M.; Zoretich, R.A.; Hughes, C.L.; Eng, H.F.; Luther, J.F.; Wisniewski, S.; Costantino, M.L.; et al. Onset Timing, Thoughts of Self-harm, and Diagnoses in Postpartum Women with Screen-Positive Depression Findings. JAMA Psychiatry 2013, 70, 490–498. [Google Scholar] [CrossRef] [PubMed]
- Guintivano, J.; Sullivan, P.F.; Stuebe, A.M.; Penders, T.; Thorp, J.; Rubinow, D.R.; Meltzer-Brody, S. Adverse life events, psychiatric history, and biological predictors of postpartum depression in an ethnically diverse sample of postpartum women. Psychol. Med. 2018, 48, 1190–1200. [Google Scholar] [CrossRef]
- American Psychiatric Association. Practice Guideline for the Treatment of Patients with Major Depressive Disorder; American Psychiatric Association: Washington, DC, USA, 2010. [Google Scholar]
- Turner, K.M.; Sharp, D.; Folkes, L.; Chew-Graham, C. Women’s views and experiences of antidepressants as a treatment for postnatal depression: A qualitative study. Fam. Pract. 2008, 25, 450–455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Oliveria Melo, A.S.; Silva, J.L.; Tavares, J.S.; Barros, V.O.; Leite, D.F.; Amorim, M.M. Effect of a physical exercise program during pregnancy on uteroplacental and fetal blood flow and fetal growth: A randomized controlled trial. Obstet. Gynecol. 2012, 120, 302–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Price, B.B.; Amini, S.B.; Kappeler, K. Exercise in pregnancy: Effect on fitness and obstetric outcomes-a randomized trial. Med. Sci. Sports Exerc. 2012, 44, 2263–2269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muktabhant, B.; Lumbiganon, P.; Ngamjarus, C.; Dowswell, T. Interventions for preventing excessive weight gain during pregnancy. Cochrane Database Syst. Rev. 2012, 4, Cd007145. [Google Scholar]
- Elliott-Sale, K.J.; Barnett, C.T.; Sale, C. Exercise interventions for weight management during pregnancy and up to 1 year postpartum among normal weight, overweight and obese women: A systematic review and meta-analysis. Br. J. Sports Med. 2015, 49, 1336–1342. [Google Scholar] [CrossRef]
- Liddle, S.D.; Pennick, V. Interventions for preventing and treating low-back and pelvic pain during pregnancy. Cochrane Database Syst. Rev. 2015, 2015, CD001139. [Google Scholar] [CrossRef]
- Owe, K.M.; Bjelland, E.K.; Stuge, B.; Orsini, N.; Eberhard-Gran, M.; Vangen, S. Exercise level before pregnancy and engaging in high-impact sports reduce the risk of pelvic girdle pain: A population-based cohort study of 39 184 women. Br. J. Sports Med. 2016, 50, 817–822. [Google Scholar] [CrossRef] [Green Version]
- Artal, R.; O’Toole, M.; White, S. Guidelines of the American College of Obstetricians and Gynecologists for exercise during pregnancy and the postpartum period. Br. J. Sports Med. 2003, 37, 6–12. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, A.; van der Waerden, J.; Melchior, M.; Bolze, C.; El-Khoury, F.; Pryor, L. Physical activity during pregnancy and postpartum depression: Systematic review and meta-analysis. J. Affect. Disord. 2019, 246, 29–41. [Google Scholar] [CrossRef] [PubMed]
- Davenport, M.H.; McCurdy, A.P.; Mottola, M.F.; Skow, R.J.; Meah, V.L.; Poitras, V.J.; Garcia, A.J.; Gray, C.E.; Barrowman, N.; Riske, L.; et al. Impact of prenatal exercise on both prenatal and postnatal anxiety and depressive symptoms: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1376–1385. [Google Scholar] [CrossRef]
- Kwon, R.; Kasper, K.; London, S.; Haas, D.M. A systematic review: The effects of yoga on pregnancy. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 250, 171–177. [Google Scholar] [CrossRef]
- Ioannidis, J.P. Integration of evidence from multiple meta-analyses: A primer on umbrella reviews, treatment networks and multiple treatments meta-analyses. Can. Med. Assoc. J. 2009, 181, 488–493. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Smith, V.; DeVane, D.; Begley, C.M.; Clarke, M. Methodology in conducting a systematic review of systematic reviews of healthcare interventions. BMC Med. Res. Methodol. 2011, 11, 15. [Google Scholar] [CrossRef] [Green Version]
- Shea, B.J.; Grimshaw, J.M.; Wells, G.A.; Boers, M.; Andersson, N.; Hamel, C.; Porter, A.C.; Tugwell, P.; Moher, D.; Bouter, L.M. Development of AMSTAR: A measurement tool to assess the methodological quality of systematic reviews. BMC Med. Res. Methodol. 2007, 7, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Carter, T.; Bastounis, A.; Guo, B.; Morrell, C.J. The effectiveness of exercise-based interventions for preventing or treating postpartum depression: A systematic review and meta-analysis. Arch. Women’s Ment. Health 2019, 22, 37–53. [Google Scholar] [CrossRef] [PubMed]
- Daley, A.; Jolly, K.; MacArthur, C. The effectiveness of exercise in the management of post-natal depression: Systematic review and meta-analysis. Fam. Pract. 2009, 26, 154–162. [Google Scholar] [CrossRef] [Green Version]
- McCurdy, A.P.; Boulé, N.G.; Sivak, A.; Davenport, M.H. Effects of Exercise on Mild-to-Moderate Depressive Symptoms in the Postpartum Period: A Meta-analysis. Obstet. Gynecol. 2017, 129, 1087–1097. [Google Scholar] [CrossRef]
- Pritchett, R.V.; Daley, A.J.; Jolly, K. Does aerobic exercise reduce postpartum depressive symptoms? A systematic review and meta-analysis. Br. J. Gen. Pract. 2017, 67, e684–e691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poyatos-León, R.; García-Hermoso, A.; Sanabria-Martínez, G.; Alvarez-Bueno, C.; Cavero-Redondo, I.; Martínez-Vizcaíno, V. Effects of exercise-based interventions on postpartum depression: A meta-analysis of randomized controlled trials. Birth 2017, 44, 200–208. [Google Scholar] [CrossRef]
- Daley, A.J.; Jolly, K.; Sharp, D.J.; Turner, K.M.; Blamey, R.V.; Coleman, S.; McGuinness, M.; Roalfe, A.K.; Jones, I.; MacArthur, C. The effectiveness of exercise as a treatment for postnatal depression: Study protocol. BMC Pregnancy Childbirth 2012, 12, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dennis, C.-L.; Dowswell, T. Psychosocial and psychological interventions for preventing postpartum depression. Cochrane Database Syst. Rev. 2013, 2013, 001134. [Google Scholar] [CrossRef] [PubMed]
- Bower, P.; Kontopantelis, E.; Sutton, A.; Kendrick, T.; Richards, D.; Gilbody, S.; Knowles, S.; Cuijpers, P.; Andersson, G.; Christensen, H.; et al. Influence of initial severity of depression on effectiveness of low intensity interventions: Meta-analysis of individual patient data. BMJ 2013, 346, f540. [Google Scholar] [CrossRef] [Green Version]
- Nascimento, S.L.; Pudwell, J.; Surita, F.; Adamo, K.; Smith, G. The effect of physical exercise strategies on weight loss in postpartum women: A systematic review and meta-analysis. Int. J. Obes. 2013, 38, 626–635. [Google Scholar] [CrossRef]
- Sobhgol, S.S.; Priddis, H.; Smith, C.A.; Dahlen, H. The Effect of Pelvic Floor Muscle Exercise on Female Sexual Function During Pregnancy and Postpartum: A Systematic Review. Sex. Med. Rev. 2019, 7, 13–28. [Google Scholar] [CrossRef]
- Davenport, M.H.; Nagpal, T.S.; Mottola, M.F.; Skow, R.J.; Riske, L.; Poitras, V.J.; Garcia, A.J.; Gray, C.; Barrowman, N.; Meah, V.L.; et al. Prenatal exercise (including but not limited to pelvic floor muscle training) and urinary incontinence during and following pregnancy: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1397–1404. [Google Scholar] [CrossRef]
- Kate, M.; Renee, K. Exercise and breastfeeding. Breastfeed. Rev. 2012, 20, 39–42. [Google Scholar]
- Howard, L.M.; Megnin-Viggars, O.; Symington, I.; Pilling, S.; On behalf of the Guideline Development Group. Antenatal and postnatal mental health: Summary of updated NICE guidance. BMJ 2014, 349, g7394. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Reference | Included RCT’s | Population | Interventions Characteristics | Comparison | Outcomes Measures |
|---|---|---|---|---|---|
| Carter et al. [30] | 17 | 1927 primiparous or multiparous postnatal women. | Exercise-based (supervised, unsupervised, coaching-based, motivational, behavioural-oriented, universal, targeted or treatment based, in a community or clinical context). | Any control condition (including exercise). | Depression symptoms using a validated assessment tool (e.g., EPDS and PHQ). |
| Daley et al. [31] | 5 | 221 women who were between 4 weeks and 18 months postpartum. | The exercise was defined as any planned, structured and repetitive bodily movement. Trials involving exercise with additional interventions (co-interventions) were eligible. | Social support intervention and standard care. | Clinical interview screened for probable depression using a recognised or diagnosed according to the clinical judgment of a health professional. |
| Mc Curdy et al. [32] | 16 | 1327 postpartum women with and without depression. | Postpartum exercise (supervised or unsupervised exercise interventions). | Standard care. | Depressive symptoms or depressive episodes assessed by a validated questionnaire (e.g., EPDS, CES-D and HDRS). |
| Pritchett et al. [33] | 13 | 1734 women up to 1 year postpartum. | Aerobic exercise, counselling exercise and group exercise. | Standard care. | Depressive symptoms measured by questionnaire or diagnostic interview. |
| Poyatos-León et al. [34] | 12 | 932 pregnant women with a single foetus and an uncomplicated pregnancy or women who had a child aged between 6 weeks and 18 months: 471 in the intervention group and 461 in the control group. | Stretching and breathing exercises, a walking program, cardiovascular exercises, mixed cardiovascular and strength exercises, Pilates and yoga exercises and home-based programs. | Any intervention during pregnancy and postpartum period. | Depression scale: the EPDS or the BDI. |
| AMSTAR 2 Criteria | Carter et al. [30] | Daley et al. [31] | McCurdy et al. [32] | Pritchett et al. [33] | Poyatos-León et al. [34] |
|---|---|---|---|---|---|
| 1. Did the research questions and inclusion criteria for the review include the components of PICO? | V | - | - | V | - |
| 2. Did the report of the review contain an explicit statement that the review methods were established before the conduct of the review, and did the report justify any significant deviations from the protocol? | V | - | - | V | V |
| 3. Did the review authors explain their selection of the study designs for inclusion in the review? | V | V | V | V | V |
| 4. Did the review authors use a comprehensive literature search strategy? | V | V | V | V | V |
| 5. Did the review authors perform study selection in duplicate? | V | X | V | V | V |
| 6. Did the review authors perform data extraction in duplicate? | V | V | V | V | V |
| 7. Did the review authors provide a list of excluded studies and justify the exclusions? | V | V | V | V | V |
| 8. Did the review authors describe the included studies in adequate detail? | V | V | V | V | V |
| 9. Did the review authors use a satisfactory technique for assessing the risk of bias (RoB) in individual studies included in the review? | V | V | V | V | V |
| 10. Did the review authors report on funding sources for the studies included in the review? | - | - | - | - | - |
| 11. If meta-analysis was performed, did the review authors use appropriate methods for statistical combination of results? | V | V | V | V | V |
| 12. If meta-analysis was performed, did the review authors assess the potential impact of RoB in individual studies on the results of the meta-analysis or other evidence synthesis? | V | - | V | V | V |
| 13. Did the review authors account for RoB in individual studies when interpreting/discussing the results of the review? | V | - | - | V | V |
| 14. Did the review authors provide a satisfactory explanation for, and discussion of, any heterogeneity observed in the results of the review? | V | V | V | V | V |
| 15. If they performed quantitative synthesis, did the review authors carry out an adequate investigation of publication bias (small study bias) and discuss its likely impact on the review results? | V | - | - | - | V |
| 16. Did the review authors report any potential sources of conflict of interest, including any funding they received for conducting the review? | V | V | V | V | V |
| MQR | LQR | LQR | MQR | MQR |
| Reference | SMD (95% CI) | I2 (%) | Conclusions |
|---|---|---|---|
| Carter et al. [30] | −0.64 (−0.96 to −0.33) | 86.0% | Statistically significant medium treatment effect of exercise over control conditions for depression symptoms in postpartum women up to 52 weeks after childbirth. |
| Daley et al. [31] | −0.81 (−1.53 to −0.10) | 81.7% | Exercise can reduce postpartum depression, but this finding is contingent on one trial that included exercise as a co-intervention. |
| McCurdy et al. [32] | −0.34 (−0.50 to 0.19) | 37% | Post-intervention depressive symptoms were lower in the exercise compared with the control group. In women with depression, exercise improved the odds of resolving depression post-intervention by 54%. |
| Pritchett et al. [33] | −0.44 (−0.75 to −0.12) | 85.0% | Exercise interventions significantly reduced depressive symptoms |
| Poyatos-León et al. [34] | −0.41 (−0.28 to −0.54) | 33.1% | Decrease in postpartum depressive symptom scores favour of the physical activity group. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marconcin, P.; Peralta, M.; Gouveia, É.R.; Ferrari, G.; Carraça, E.; Ihle, A.; Marques, A. Effects of Exercise during Pregnancy on Postpartum Depression: A Systematic Review of Meta-Analyses. Biology 2021, 10, 1331. https://doi.org/10.3390/biology10121331
Marconcin P, Peralta M, Gouveia ÉR, Ferrari G, Carraça E, Ihle A, Marques A. Effects of Exercise during Pregnancy on Postpartum Depression: A Systematic Review of Meta-Analyses. Biology. 2021; 10(12):1331. https://doi.org/10.3390/biology10121331
Chicago/Turabian StyleMarconcin, Priscila, Miguel Peralta, Élvio R. Gouveia, Gerson Ferrari, Eliana Carraça, Andreas Ihle, and Adilson Marques. 2021. "Effects of Exercise during Pregnancy on Postpartum Depression: A Systematic Review of Meta-Analyses" Biology 10, no. 12: 1331. https://doi.org/10.3390/biology10121331
APA StyleMarconcin, P., Peralta, M., Gouveia, É. R., Ferrari, G., Carraça, E., Ihle, A., & Marques, A. (2021). Effects of Exercise during Pregnancy on Postpartum Depression: A Systematic Review of Meta-Analyses. Biology, 10(12), 1331. https://doi.org/10.3390/biology10121331