1. Introduction
Spinal cord injury (SCI) is both a medical and social issue causing severe disability. Most post-traumatic tissue degeneration is caused by multiple secondary injuries involving several closely related processes such as a blood-brain barrier dysfunction, local inflammation, neuronal death, demyelination, and impaired neural pathways [
1]. SCI can lead to a severe motor, sensory, and autonomic dysfunction. At present, there is no effective method to restore an injured spinal cord [
2].
There is a possibility to overcome the consequences of SCI by using cell therapy. For this purpose, both stem/progenitor cells and specialized cells (Schwann cells, olfactory epithelial cells, etc.) have been used [
2,
3,
4]. Nevertheless, cells, which might be easily and minimally invasively isolated from the adult body for subsequent autotransplantation to a recipient, remain the most promising for clinical use. Peripheral blood is an attractive and available source for isolation, freezing, and storage for subsequent fundamental research and clinical use.
It has been previously shown that both transplantation of granulocyte colony-stimulating factor-mobilized peripheral blood mononuclear cells (PBMCs) and CD34
+-PBMCs promoted angiogenesis, axonal regeneration, and the preservation of myelin, contributing to functional recovery [
5]. Kijima et al. (2009) demonstrated that human CD133
+ PBMCs locally transplanted into an injured peripheral nerve of rats could enhance vasculogenesis, providing the microenvironment required for axonal regeneration [
6]. The results of the above-mentioned study suggest that mobilized stem fraction of PBMCs might play the role in the creation of a microenvironment promoting neuroregeneration and functional recovery. However, the therapeutic efficacy of PBMCs against SCI, excluding preliminary sorting or mobilization of stem cells, remains unclear.
Scaffolds are used as a vehicle to deliver stem cells into the site of injury; they fill the post-traumatic cavity, thereby promoting axonal growth and acting as a “biological bridge” [
7]. The potential of biodegradable natural and synthetic scaffolds has been assessed for maintaining the viability of transplanted cells and creating an enabling microenvironment in vitro and in vivo [
7,
8,
9]. The findings of Itosaka et al. (2009) suggest that a fibrin matrix (FM) might be one of the most promising candidates for a scaffold due to the low risk of developing rejection reactions, it is physiologically more flexible, it has good plasticity, and it is easily implanted into the injured spinal cord [
10].
In this study, we aimed to evaluate the therapeutic potential of the application of peripheral blood mononuclear cells embedded in FM in a subacute period of SCI in pigs based on the injured spinal cord structural and functional recovery criteria.
2. Materials and Methods
2.1. Isolation and Adenoviral Transduction of PBMCs
The study was approved by the Kazan Federal University Animal Care and Use Committee (Permit Number 2, 5 May 2015). Peripheral venous blood was taken from healthy 4-month-old female pot-bellied pigs (8 kg).
Blood samples were collected in vacuum test tubes (Apexlab, Moscow, Russia) supplemented with an ethylenediaminetetraacetic acid (EDTA) solution. All procedures were performed in a biosafety class 2 cell culture laboratory. Primarily, 5 mL of whole blood was mixed with an equal volume of Dulbecco’s phosphate-buffered saline (DPBS, PanEco, Moscow, Russia) in a sterile 15 mL tube. The diluted blood sample was accurately applied to a ficoll solution (ficoll density—1.077 g/cm3, PanEco), then centrifuged at 1900 rpm for 20 min without break.
After centrifugation, the fraction of white blood cells was transferred into a new 15 mL tube. The cells were washed with DPBS twice (5 min at 1400 rpm). Red blood cells were lyzed in a lysis solution (155 mM NH4Cl, 10 mM KHCO3, 0.1 mM EDTA, pH 7.3) for 5 min. The cells were washed with DPBS and resuspended in RPMI-1640 media (PanEco) supplemented with 10% fetal bovine serum (HyClone, Chicago, IL, USA), 2 mM L-glutamine, and 1% mixed penicillin–streptomycin (PanEco). Isolated cells were incubated for 24 h, then washed twice with DPBS.
Isolated PBMCs were seeded onto 10 cm cultural dishes at 8 × 106 cells per plate. The isolated PBMCs were genetically modified with Ad5-EGFP with multiplicity of infection (MOI) 10 and incubated in a humidified chamber containing 5% CO2 at 37 °C. Green fluorescence was measured at 24 h by flow cytometry on Guava easyCyte (Merck Millipore). After 24 h, PBMCs transduced with Ad5-EGFP exhibited green fluorescence at a 29.8 ± 4% rate.
2.2. Spinal Cord Injury and Experimental Groups
Animals were exposed to surgical manipulations after intubation anesthesia, appropriate pre-operation preparation, and adequate analgesia/pain control. Premedication consisted of intramuscular injection of xylazine (0.6 mg/kg, Bimeda, Dublin, Ireland) and ketamine (5 mg/kg, Hospira, Lake Forest, IL, USA). After propofol induction (IV, 2–6 mg/kg, Fresenius Kabi, Bad Homburg, Germany), endotracheal intubation was conducted using isoflurane (1.3%, Laboratorios Karizoo, Barcelona, Spain) throughout the intervention.
After laminectomy, the anesthetized pigs were subjected to a dosed contusion at the spinal T 10 level with a metal impactor weighing 50 g dropped from a height of 20 cm, followed by compression with the same weight for 10 min. Then, muscles of the back were sutured layer by layer. A urinary catheter (10 Fr, Jorgensen Laboratories Inc., Loveland, CO, USA) was inserted 3–5 days after surgery. Cefazolin (25 mg/kg, Sintez, Kurgan, Russia) and ketoprofen (1 mg/kg, AVZ, Moscow, Russia) were given as intramuscular injections. The pigs were housed separately within the first 48 h, then in pairs.
At 6 weeks after injury, after removing synechiae and making several longitudinal incisions in the dura mater (2–3 incisions with a length of 2–3 mm at a distance of 2–3 mm from each other), 8 × 106 PBMCs per pig, enclosed in 150 μL fibrin glue (Tissucol, Baxter, Deerfield, Illinois, USA) (the experimental group—FM+PBMCs, n = 5) were applied on top of the injury. Animals of the control group were applied with cell-free 150 μL FM under similar conditions (the control group—FM, n = 5). In addition, two pigs were used to evaluate the distribution of Ad5–EGFP-transduced PBMCs in the area of SCI on day 14 after application. After the wound was sutured layer by layer, cefazoline (25 mg/kg, Pharmasyntez, Moscow, Russia) and ketoprofen (1 mg/kg, Moscow Endocrine Plant, Moscow, Russia) were injected (1 mg/kg) intramuscularly for 5 days.
A subacute period was chosen for cell transplantation as the autologous transplantation of PBMCs is technically feasible in clinical practice when autologous PBMCs derived from a patient can be applied.
2.3. Motor Function Testing with PTIBS
To evaluate the effectiveness of motor function recovery, the Porcine Thoracic Injury Behavioral Scale (PTIBS) was used [
11]. The PTIBS is a 10-point scale that describes various stages of hindlimb function. Score 1 represents no active hindlimb movement and the rump and knees are on the ground, with Score 10 describing normal ambulation with normal balance. Locomotor recovery in the study groups was video-recorded as previously described [
12]. Motor function assessments were scored simultaneously by two supervisors who were blinded to the study groups.
2.4. Electrophysiological Studies
Electrophysiological tests were performed for intact and experimental pigs 2 and 11 weeks after SCI as previously described [
12].
Figure 1 provides a schematic illustration of the electrode positions on the pigs. The animal’s neuromotor function was assessed by stimulating electromyography. M- and H-waves from the tibialis anterior muscle were recorded in response to stimulation of the sciatic nerve. Monopolar needle electrodes were used for both recording and reference. An active electrode was inserted into the middle of the muscle belly, with the reference electrode implanted within a region of the tendomuscular junction. Electrical stimulation of the sciatic nerve was carried out with square-wave single stimuli lasting for 0.2 ms. For stimulation, monopolar needle electrodes were inserted subcutaneously within the area where the sciatic nerve exits from the pelvis.
To evaluate pyramidal tracts, transcranial electrical stimulation (TES) was used. Motor evoked potentials (MEPs) were registered from the tibialis anterior muscle using the same technique as that for the M-response. Transcranial stimulation was performed by needle electrodes inserted under the scalp up to the contact with the skull bone. The cathode was placed in the middle approximately 0.5 cm caudally from the interorbital line, and the anode was placed in the middle near the occipital bone. Here, 0.1 ms stimuli with intensities ranging from 20 to 400 V were used.
Somatosensory evoked potentials (SEPs) were used to evaluate the posterior columns of the spinal cord. To register them, monopolar needle electrodes were subcutaneously inserted. To register potentials from the lumbar level, an active electrode was inserted over the upper lumbar vertebrae, and the reference electrode was inserted over the middle thoracic vertebrae. For registration of the scalp, an active electrode was inserted over the vertex, and the reference electrode was inserted over the snout. The electrical stimulation of the tail was performed by round electrodes with a stimulus duration of 0.2 ms. The stimulus intensity was chosen by tail movements (the smallest stimulus provoking tail movements was used).
2.5. Histological Methods
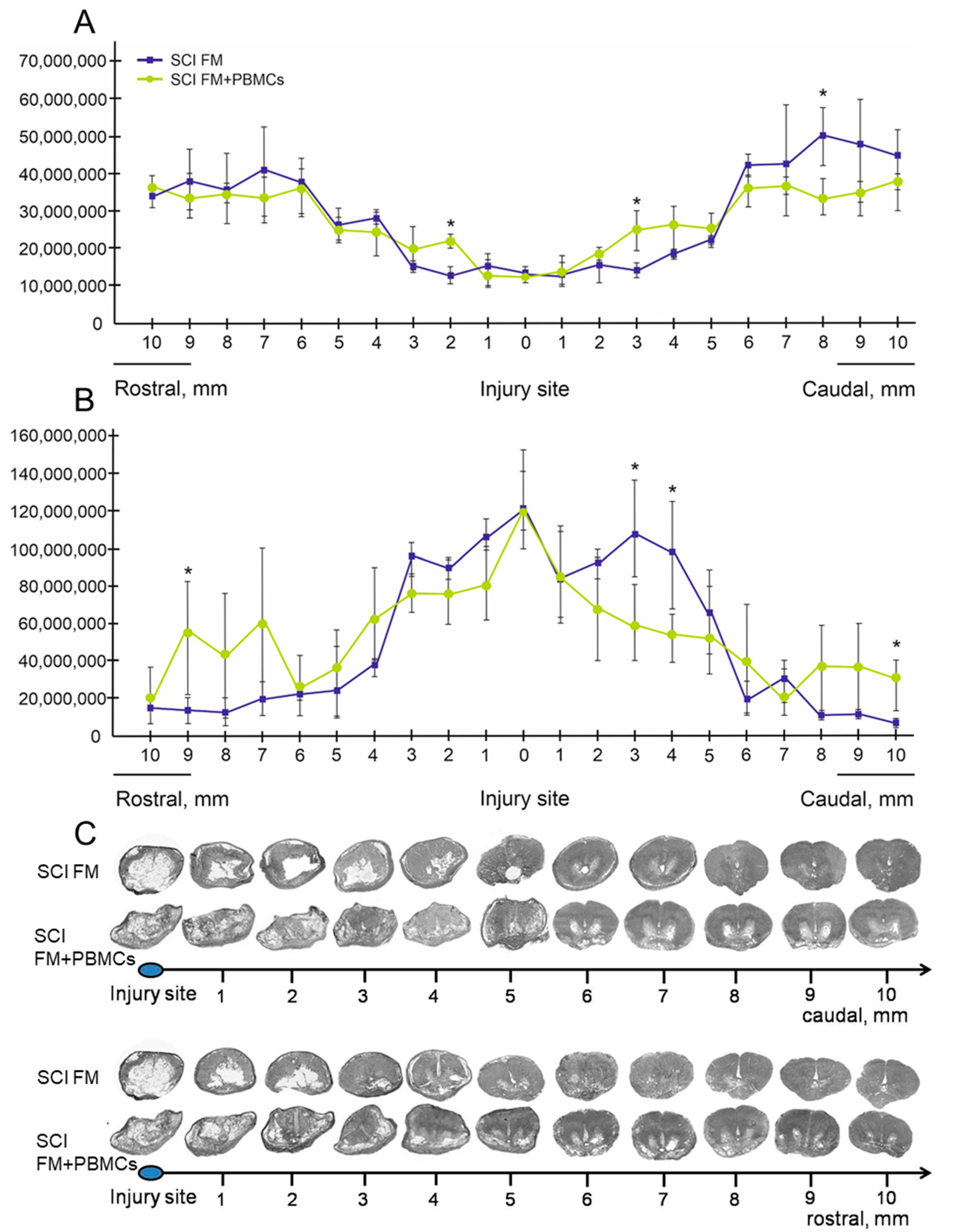
At 4 months after treatment, the animals were anesthetized and perfused with a 4% paraformaldehyde solution (4 °C). A fragment of the spinal cord (8 cm) was taken from the spinal column and fixed in a 4% paraformaldehyde solution for 2 days. Then, the sample was transferred into 30% sucrose. Cryostat cross-sections of the spinal cord over 1 cm from the injury epicenter rostrally and caudally were stained with azur-eosin. The stained sections were embedded into vitrogel and studied under the APERIO CS2 scanner (Leica). The Aperio imagescope software was used to measure the tissue area.
2.6. Cytokine Assay
The multiplex analysis was performed using the MILLIPLEX MAP Porcine Cytokine/Chemokine (magnetic) kit #PCYTMG-23K-13PX (Millipore) as previously described [
12]. Each experiment was done in triplicates. The kit enables a simultaneous multiplex analysis of 13 pig cytokines/chemokines/interleukins in a 25-μL aliquot of porcine cerebrospinal fluid (CSF) and blood serum obtained before SCI and on days 7 and 14 post-injury.
2.7. Statistical Analysis
To process the results obtained, Origin 7 Pro software was used. Data are presented as mean ± standard deviation (SD). A one-way analysis of variance (ANOVA) with a Tukey’s test were used for multiple comparisons between all study groups. All analyses were performed in a blinded manner with respect to the study groups. The significance level lower than 0.05 (p < 0.05) was accepted for all statistical data.
4. Discussion
The fundamentals of SCI cell therapy have specific features which should be taken into consideration for the regenerative potential of transplanted cells to be most effectively employed. A spinal cord injury is generally an acute condition which requires urgent medical intervention. In this regard, and taking into account the rapid development of inflammatory and immune processes, regenerative therapy with the use of autologous cells in a subacute period of the disorder is preferable [
4,
13]. At the same time, delayed application of cells is possible as part of a scaffold in a second surgical intervention when a neurosurgeon has access to the surface of the spinal cord. In this case, the peripheral blood presents the most available and convenient source for the clinical use of autologous adult cells.
In our study, PBMCs were for the first time tested in a model of SCI in large animals when evaluating functional and structural parameters as well as blood serum and CSF cytokine/chemokine profiles in a delayed period after therapy. In addition, the migration activity of PBMCs embedded in FM and applied on the area of the SCI was evaluated. The findings indicate that PBMCs can penetrate into the spinal cord and concentrate primarily in the grey matter. However, it should be noted that a part of PBMCs has remained within epidural fibrosis by day 14 after application to the area of the SCI. This might be due to a low PBMC migration rate and the resulting enclosure of some cells in rapidly forming synechias. For example, in our previous study, adipose-derived mesenchymal stem cells embedded in FM transplanted into the area of the SCI in pigs had a higher migration rate into the spinal cord and a smaller number of them in synechias [
12]. It is worth noting that PBMCs were not detected in the spinal cord on day 7 after intravenous transplantation to rats with the SCI [
14]. When intraspinally transplanted PBSCs were detected 2 mm rostrally and caudally from the epicenter of SCI in mice, their number gradually decreased with time [
5].
The behavior analysis with the PTIBS did not show significant differences in the motor function recovery in pigs of the control (FM alone) and experimental (FM+PBMC) groups, despite the positive effect of PBMCs as evidenced by electrophysiological data confirming partial recovery of conduction in the posterior columns of the spinal cord. An intraperitoneal injection of PBMCs-secretome was previously shown in a rat SCI model to improve locomotor activity [
15]. Intraspinal transplantation of G–CSF-mobilized peripheral blood stem cells (PBSCs) also promoted functional recovery in a mouse model of SCI [
5]. Even a week after a single intravenous injection to rats with SCIs, human peripheral blood-derived CD133
+ cells provided significant functional recovery [
16]. These results in rodents are encouraging; however, it seems to be impossible to compare them with our findings to the full extent as different populations of PBMCs and animal models were used.
That tissue structure can be improved in the setting of PBMC transplantation to rodents with SCIs, as been previously shown; a decreased area of abnormal cavities and less damage of the myelin sheath were noted [
5,
16,
17]. In our study, the application of FM+PBMCs at the site of the SCI improved tissue integrity and reduced the area of abnormal cavities near the epicenter of injury, compared to the control group, without stimulating the regenerative processes at a distance.
The CSF cytokine/chemokine profile showed an increased IL-18 level on day 7 after the application of FM+PBMCs. Being the main immunoregulatory cytokine, IL-18 plays an important role protecting the organism against infections and tumors [
18]. At the same time, CSF IL-1Ra level increased in animals treated with FM+PBMCs compared to intact controls (i.e., prior to SCI) and was lower when compared with the SCI group treated with FM alone. Thus, mechanisms preventing the activation of the intracellular inflammatory signaling cascade of IL-1 were noted to develop in both groups, though to a different extent.
The treatment of rat SCI with the PBMCs-secretome was previously found to increase CXCL-1 and IL-10 expression levels in plasma [
15]. In our study, serum IL-10 level increased in both study groups compared to intact pigs prior to SCI. However, on day 7 after the application of FM+PBMCs, we detected an upregulated secretion of pro-inflammatory IFN-g in serum samples; IFN-g is known to be one of the triggers of microglia activation and release of neurotoxic factors [
19]. At 2 weeks after treatment, IFN-g levels were similar in both groups; however, there were differences in the IL-18 levels, with a higher value in the FM+PBMC group. Thus, our results show the cytokine imbalance to occur without significantly shifting toward pro-inflammatory or anti-inflammatory cytokine cascades. The data obtained confirm our previous research [
20], demonstrating the complexity of inflammatory reactions and immunological response after the SCI, as well as their widespread prevalence, which is supported by cytokine profile changes in blood serum. Further investigations of the complex cytokine imbalance that occurs after the SCI, including that associated with cell-based therapy, are required in order to determine whether it can be correlated with the severity of injury and a clinical prognosis.



 and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}





