
The Effects of Vagus Nerve Stimulation on Animal Models of Stroke-Induced Injury: A Systematic Review


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search or Data Strategies
2.2. Inclusion and Exclusion Criteria
- The focus was not ischemic stroke
- They reported on therapeutic interventions other than VNS and rehabilitation
- They consisted of a review article, an abstract, a conference paper, or a book chapter
- They were published in a language other than English
- They were missing main parts of the text
2.3. Data Extraction and Analysis
2.4. Quality Assessment
2.5. Risk-of-Bias Assessment
- Was the induction of stroke ischemia and VNS treatment adequately randomized?
- Was the allocation to study groups adequately concealed?
- 3.
- Were the research personnel and animal subjects blinded to the study group?
- 4.
- Can we be confident in the exposure characterization?
- 5.
- Can we be confident in the outcome assessment?
- 6.
- Was outcome data complete without attrition or exclusion from the analysis?
- 7.
- Were all measured outcomes reported?
- For rating the “definitely low” risk of bias, there should be ample evidence of “low risk” of bias practices from the study. For example, if the risk of bias due to selection bias was rated as “definitely low,” there should be direct evidence that animals were assigned to any study group using adequate and proper randomization descriptions.
- “Probably low” risk of bias is rated when there is an indirect evidence of low risk of bias practices. This is rated based on the magnitude and direction of deviation from a high risk of bias. For example, if a selection bias was rated as “probably low” risk of bias, it means that the study’s authors stated that allocation was random but did not describe the method used for randomization.
- “Probably high” risk of bias is rated for a study when there is insufficient information or information not provided about relevant risk-of-bias practices. In the case of selection bias, for example, there is insufficient information provided about how animals were assigned to the study groups.
- “Definitely high” risk of bias can be rated when there is direct evidence of high risk-of-bias practices. For example, if a selection bias is rated as having a definitely high risk of bias, it means that there is direct evidence that animals were allocated to study groups using a non-random method such as the investigator’s judgement, the results of a laboratory test, or there was a lack of a concurrent control group, indicating that randomization did not cover all study groups.
3. Results
3.1. Bias Analysis
3.2. Characteristics of Included Studies

| Author and Year | Sex and Species | Sample Size | Parameters Assessed | Stroke Model | Stimulation Parameter | Positioning of Electrode | Fundamental Finding |
|---|---|---|---|---|---|---|---|
| Xiang et al., 2015 [21] | Male Wistar rats | 36 | Neurological deficit score, infarct volume, and pro-inflammatory cytokines | PMCAO | 20 Hz, 0.5 mA, 0.5 ms pulse width | Right cervical vagus nerve. | Applying 60 min VNS protects against cerebral ischemia by an anti-inflammatory mechanism neuroprotective effect is associated with the inhibition of expression of TNF-α and IL-6 |
| Ay et al., 2015 [22] | Male Wistar rats | 14 | Neurological deficit score, cerebral infarct volume | PMCAO | 0.5 mA, 0.5 ms pulse width, 20 Hz | Left cavum concha | Electric stimulation of the vagus nerve dermatome in the external ear activates brainstem afferent vagal nuclei and reduces infarct volume in rats. |
| Ay et al., 2016 [23] | Male spontaneously hypertensive rats | 8 | Neurological deficit score, infarct volume, microglial markers | PMCAO | 25 Hz, 1 ms, 5 kHz, 12 V sine waves 2-min trains. | Overlying skin over the right vagus nerve. | Transcutaneous VNS reduces tissue injury and functional deficits while activating the vagal relay center in the brain. This was linked to a reduction in brain inflammatory responses (i.e.,: Iba-1, CD68. TNF-α). |
| Yang et al., 2018 [24] | Spontaneous hypertensive rats | 12 | Blood brain barrier integrity, neuronal cell death, infarct size. | PMCAO | 25 Hz, 1 ms, 5 kHz, 15 V sine waves | Overlying skin over the right vagus nerve. | The neuroprotective role of transcutaneous VNS administrations during cerebral occlusion was investigated, and it was discovered that it spatially correlates with blood brain barrier integrity protection and infarct extent reduction. |
| Lindemann et al., 2020 [25] | Male Wistar rats | 8 | Cerebral blood flow, infarct volume, neurological deficit score, sensorimotor function | PMCAO | 25 Hz, 0.5 mA, 0.3 ms pulse width | Overlying skin over the left vagus nerve. | Both VNS interventions limit the spread of cortical depolarization, resulting in a smaller stroke volume and improved motor outcome. |
| Zhang et al., 2021 [26] | Sprague-Dawley rats | 16 | TLR4/NFkB pathway, inflammatory cytokines | PMCAO | 0.5 mA, 20 Hz, 0.5 ms pulse width | Left cervical vagus nerve | TLR4/MyD88/NF-kB-dependent polarization of microglia towards M2 is mediated by VNS. |
| Lu et al., 2017 [27] | Male Sprague-Dawley (SD) rats weighing | 8 | neurological deficits score, infarct volume, a7nAChR expression biomarkers | PMCAO | 0.5 mA, 0.5 ms pulse width, 20 Hz | Left cervical vagus nerve | The application of VNS resulted in neuroprotection against ischemic injury, as well as anti-inflammatory responses. Inhibiting a7nAchR expression levels resulted in a significant worsening of neurological dysfunction, as well as an increase in cerebral infarct volume. |
| Long et al., 2022 [28] | Male Sprague–Dawley rats | 15 | White matter remyelination, ischemic volume, angiogenesis and the inflammation responses | PMCAO | 2 mA, 0.5 ms pulse width, 20 Hz | Left cavum concha | VNS treatment improves dysphagia by promoting angiogenesis, remylination, and inhibiting inflammatory responses in white matter. |
| Zhao et al., 2022 [29] | Male Sprague Dawley rats | 12 | Neurological deficit score, inflammatory markers | Longa thread embolization | 10 Hz, 1 mA, 0.5 ms pulse width | Left cymba concha | Seven days of auricular VNS promotes locomotor function recovery and inhibits IL-1, IL-6, and TNFα in the ischemic penumbra |
| Jiang et al., 2014 [30] | Male Sprague Dawley rats | 8 | Neurological deficit score, infarct volume, neuronal apoptosis, pro-inflammatory cytokines | Intraluminal occlusion technique | 20 Hz, 0.5 mA, 0.5 ms pulse width | Right cervical vagus nerve. | 60 min of VNS provides neuroprotection against acute cerebral I/R injury by suppressing inflammation and apoptosis in the ischemic penumbra. This was linked to cholinergic and α7nAchR/Akt pathway activation |
| Hiraki et al., 2012 [31] | Male Sprague-Dawley rats | 10 | Neurological deficit score, infarct volume | TMCAO | 20 Hz, 0.5 mA, 0.5 ms pulse width | Right cervical vagus nerve. | The experimental evaluations were compared after 24 h, 48 h, 1 day, 2 days, and 3 days. VNS improves neurological functional scores and the severity of an ischemic lesion. This effect lasts for three weeks. |
| Ay et al., 2011 [32] | Male Wistar rats | 8 | Cerebralblood flow, infarct volume, neurological deficit score | TMCAO | 0.5 mA, 30s, 0.5 ms, 20 Hz | Right and left cervical vagus nerve. | Both stimulation sides produced acute ischemic injury protection that was not mediated by changes in cerebral blood flow. |
| Zhang et al., 2017 [49] | Male Sprague–Dawley rats | 12 | Neuronal apoptosis, Neurological deficit score, infarct volume | TMCAO | 0.5 mA, 0.5 ms pulse width, 20 Hz | Right cervical va-gus nerve | L-PGDS levels increased in rats treated with VNS in the peri-infarct region. L-PGDS may play a role in VNS’s suppression of the apoptotic response to ischemic damage. |
| Jiang et al., 2015 [34] | Male Sprague–Dawley rats | 8 | Infarct volume, neurologic deficit score, neuronal apoptosis | TMCAO | 0.5 mA, 0.5 ms pulse width, 20 Hz | Right cervical vagus nerve | MiR-210 expression is increased in stimulated animals and has been linked to neuroprotection. The beneficial effects of VNS were reduced with miR-210 knockdown. |
| Ay et al., 2009 [35] | Male Wistar rats | 8 | Infarct volume, neurological deficit score | Filament occlusion. | 0.5 mA, 0.5 ms pulse width, 20 Hz | Right cervical vagus nerve. | VNS reduced infarct volume and improved functional score significantly. |
| Yang et al., 2022 [36] | Male Spontaneous hypertensive rats | 16 | IL-1B, Iba1 antibody level, a7nAchR level, neurodegeneration | Filament occlusion. | 15 V, 1 ms pulse width, 25 Hz | Left cervical vagus nerve. | The stimulation reduced brain injury by downregulating the MMPs/IL-1β signalling pathway. |
| Li et al., 2020 [37] | Male Sprague–Dawley rats | 8 | Neurological deficit score, neuronal damage, infarct volume, micro vessel density, endothelial cell proliferative condition, and angiogenesis | MCAO/R | 0.5 mA, 0.5 ms pulse width, 20 Hz | Left cavum concha | Auricular stimulation protected the brain from ischemic injury and was linked to angiogenesis activity. The effects of vagal stimulation were reduced by PPAR-γ silencing. |
| Jiang et al., 2016 [38] | Male Sprague-Dawley | 8 | Neurological deficit score, behavioral test, cerebral infarct volume, angiogenesis | MCAO/R | 0.5 mA, 0.5 ms pulse width, 20 Hz | Left cavum concha | Auricular VNS provided significant neuroprotection and increased angiogenesis. |
| Ekici F et al., 2013 [39] | Male Wistar albino rats | 7 | neurological deficit score, infarct area | MCAO/R | 1 mA, 500 µs pulse width, 20 Hz | Left cervical vagus nerve | VNS-treated animals had a higher neurologic score and a smaller infarct region. This was linked to higher antioxidant levels in brain samples. |
| Sun et al., 2012 [40] | Male Sprague-Dawley rats | 8 | Cerebral blood flow, infarct volume, Neurological score | PMCAO and MCAO/R | 0.5 mA, 0.3 ms pulse width, 20 Hz | Right cervical vagus nerve | VNS neuroprotection against stroke in both temporary and permanent ischemia is unrelated to cerebral blood flow. |
| Jiang et al., 2015 [41] | Male Sprague-Dawley rats | 6 | Neurological deficit score, cerebral infarct volume, inflammatory markers | MCAO/R | 0.5 mA, 0.5 ms pulse width, 20 Hz | Right cervical vagus nerve | PPARγ may participate in the process by which VNS modulates the neuro-inflammatory response following ischemia/reperfusion in rats. |
| Zhao et al., 2019 [42] | Male C57BL/6 mice | 6 | Infarct volume, neurological deficit score, neuronal apoptosis, microglial polarization | MCAO/R | 25 Hz, 1 ms, 5 kHz sine waves average voltage of 15 V for 60 min | Left cer-vical va-gus nerve | Non-invasive VNS-mediated microglia activation via IL-17A signalling reduces neuronal apoptosis while promoting microglial M2 polarisation. |
| Li et al., 2020 [50] | Male Sprague–Dawley rats | 8 | Neurological recovery function, α7nAchR activation, axonal plasticity | MCAO/R | 0.5 mA, 20 Hz, 0.5 ms pulse width | Left cavum conchae | Transcutaneous VNS increased the expression of a7nAchR in the ischemic cortex. This was linked to better neuro-behavioral performance and increased axonal plasticity. |
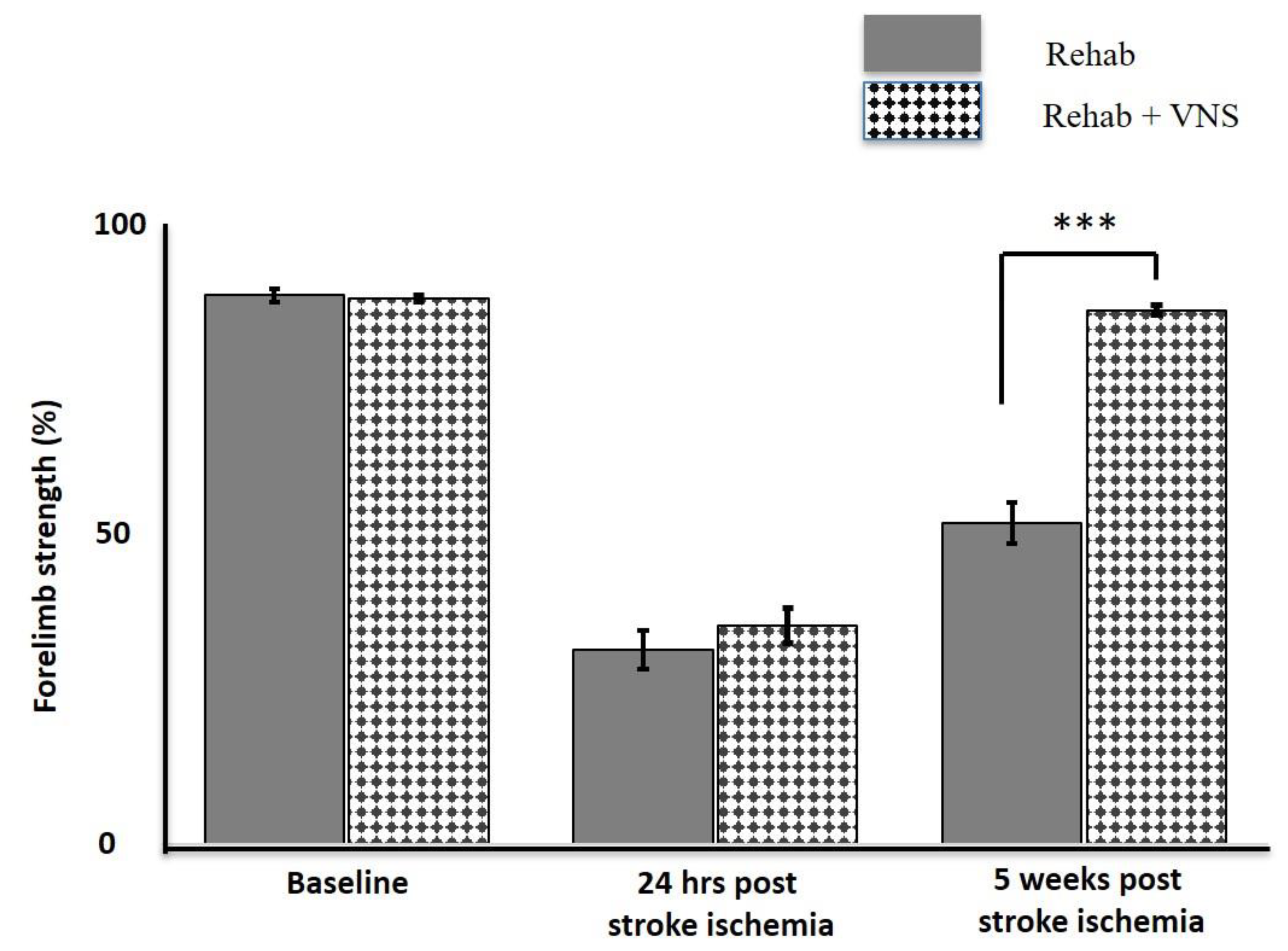
| Khodaparast et al., 2013 [43] | Female Sprague–Dawley rats | 16 | forelimb function, ischemic size | Endothelin −1 injection | 0.8 mA, 100 μs pulse width, 30 Hz | Right cervical vagus nerve | In comparison to training alone, VNS combined with physical rehabilitation resulted in significant recovery of forelimb strength. The ischemic size was unaffected. |
| Hays et al., 2014 [44] | Female Sprague-Dawley rats | 16 | Forelimb strength | Endothelin −1 injection | 0.8 mA, 100 µs pulse width, 30 Hz. | Left cervical vagus nerve | Vagus nerve stimulation administered after 2 h of forelimb training is less effective than VNS administered in conjunction with forelimb training. |
| Hays et al., 2016 [45] | Female Fisher rats | 8–9 | forelimb function, ischemic size | Endothelin −1 injection | 0.8 mA, 100 μs pulse width, 30 Hz | Right cervical vagus nerve | In aged rats, VNS combined with rehabilitative training improves forelimb function recovery compared to rehabilitative training alone. |
| Khodaparast et al., 2014 [46] | Female Sprague-Dawley rats | 10 | Motor functions, infarct volume | Endothelin −1 injection | 0.8 mA, 100 μs pulse width, 30 Hz | Right cervical vagus nerve | Combining VNS with motor rehabilitation can help with stroke recovery. During motor rehabilitation, VNS was used to restore rapid improvement and return to pre-lesion performance. |
| Khodaparast et al., 2016 [47] | Female Sprague-Dawley rats | 9–10 | Forelimb strength, lesion size | Endothelin −1 injection | 0.8 mA, 100 μs pulse width, 30 Hz | Right cervical vagus nerve | VNS combined with rehabilitative training significantly improves forelimb function recovery. The benefits of VNS on forelimb function were maintained after stimulation was stopped. There are no differences in lesion size. |
| Meyers et al., 2018 [48] | Female Sprague-Dawley rats | 6–8 | Forelimb strength, lesion size | Endothelin −1 injection | 0.8 mA, 100 ms pulse width, 30 Hz | Left cervical vagus nerve | VNS combined with rehabilitative training increases neuroplasticity in corticospinal motor networks to task-relevant musculature, which may provide insight into the neural changes that support VNS-dependent recovery improvement. |
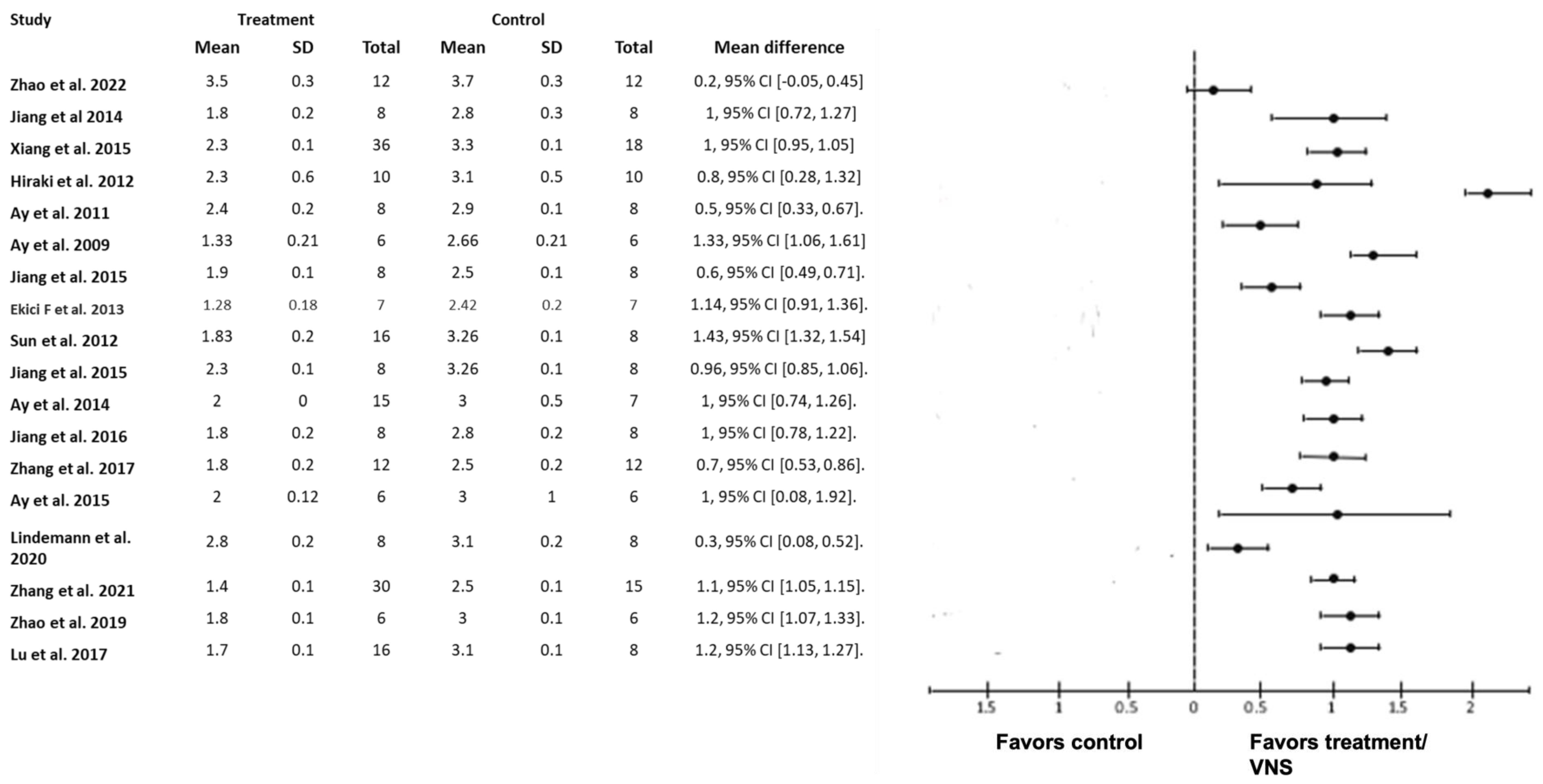
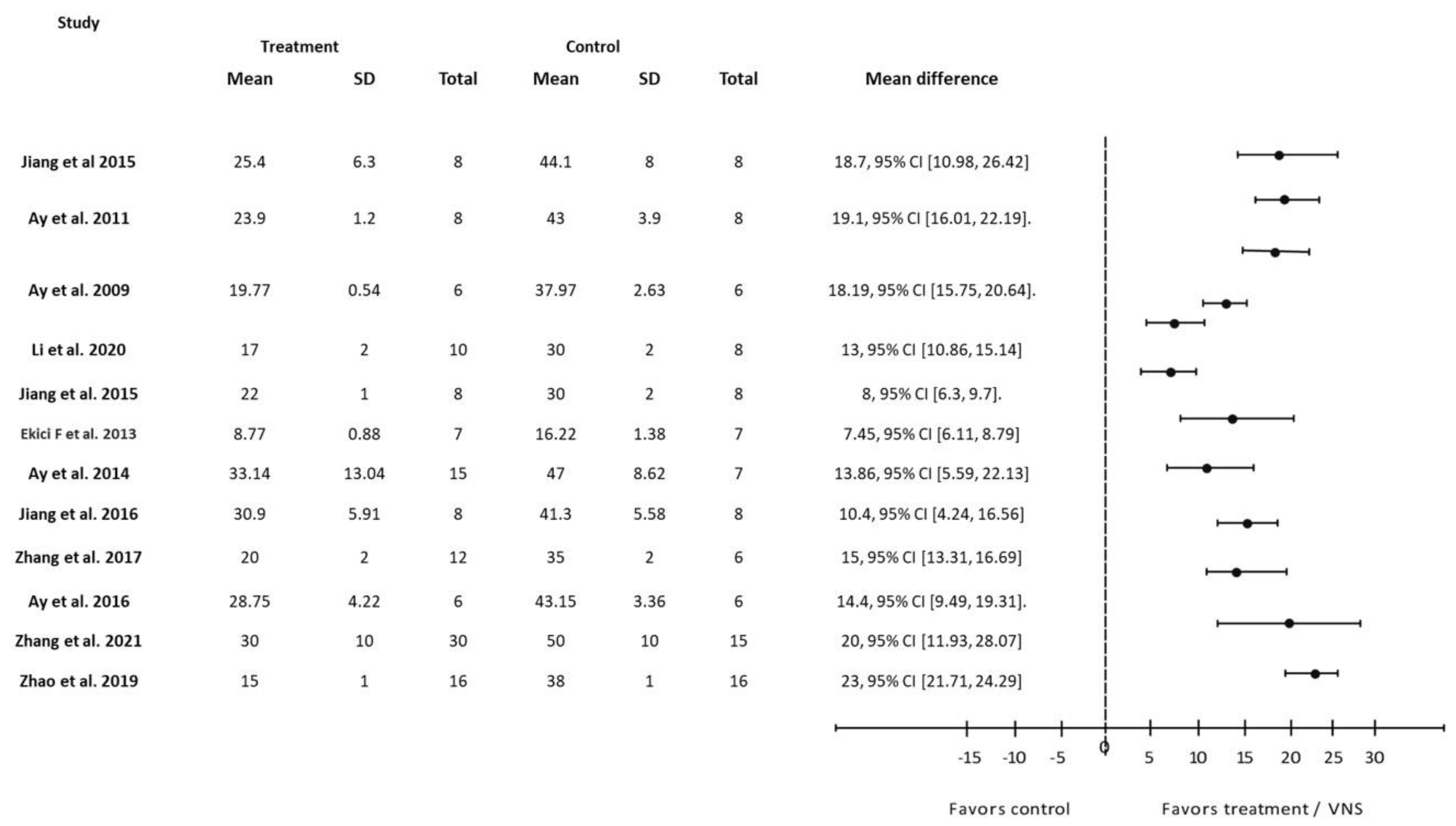
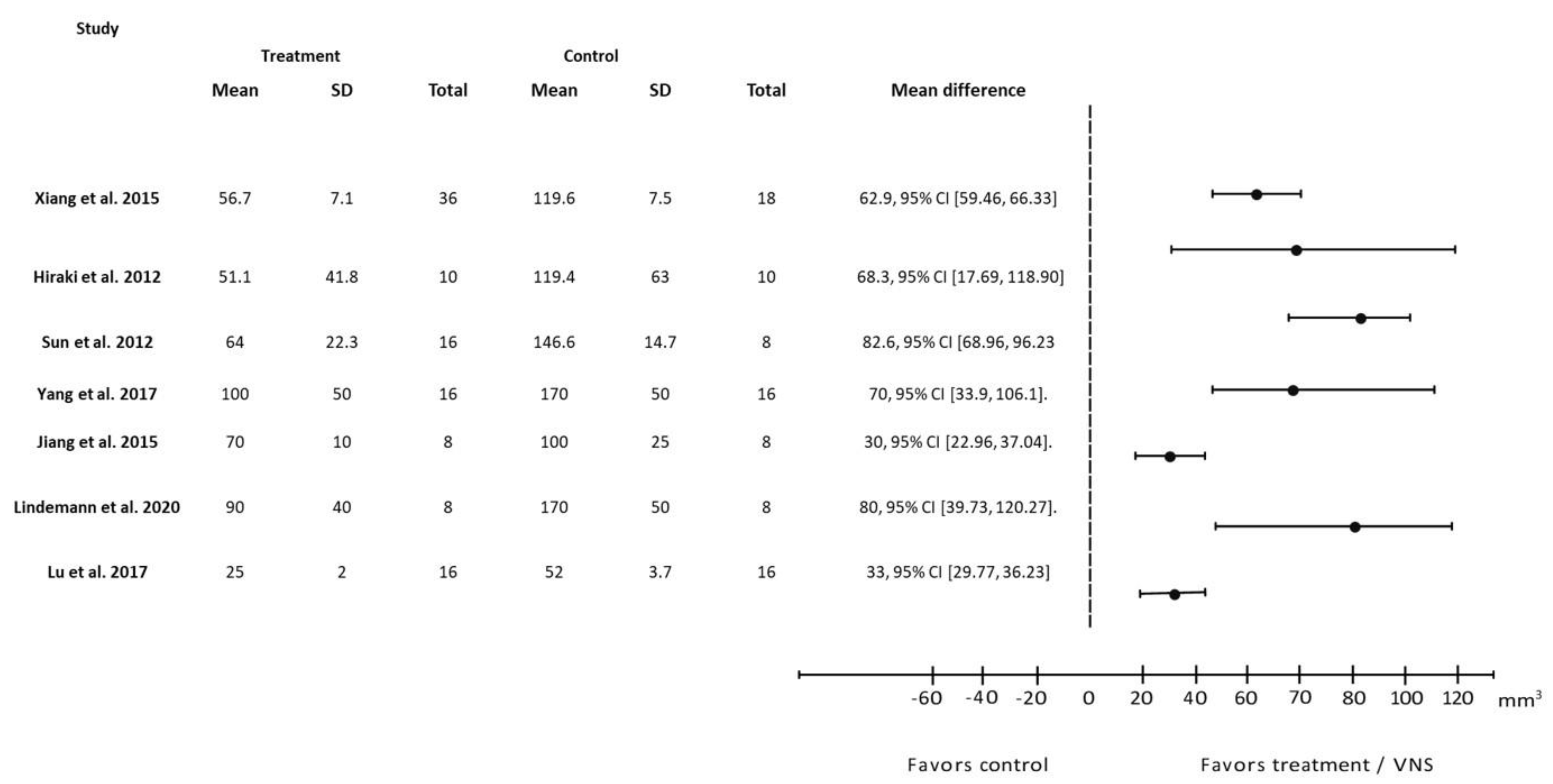
3.3. Prognostic Factors for Acute Stroke Ischemia



3.4. Biomarker Analysis
| Parameters | Biomarkers | Studies with Reported Effects of VNS | ||
|---|---|---|---|---|
| Increased | No Effect | Decreased | ||
| Inflammatory cytokines | TNFα | - | Yang, et al. [36] | * Zhao, et al. [29] * Jiang, et al. [30] * Xiang, et al. [21] * Jiang, et al. [41] * Ay, et al. [23] * Long, et al. [28] * Zhang, et al. [51] |
| IL1β | - | Ay, et al. [30] | * Jiang, et al. [30] * Jiang, et al. [41] * Zhang, et al. [26] ** Long, et al. [28] ** Zhao, et al. [29] ** Yang, et al. [36] | |
| IL6 | - | - | * Jiang, et al. [30] * Xiang, et al. [21] ** Zhang, et al. [33] ** Zhao, et al. [29] | |
| Angiogenesis | VEGF | * Long, et al. [28] * Li, et al. [37] * Jiang, et al. [38] | - | - |
| BDNF | * Li, et al. [37] * Jiang, et al. [38] | - | - | |
| FGF2 | ** Long, et al. [28] | - | - | |
| p-eNOS | * Jiang, et al. [38] * Li, et al. [37] | - | - | |
| Apoptosis | Cleaved caspase 3 | - | - | * Jiang, et al. [30], * Zhang, et al. [49] |
| p-Akt | * Jiang, et al. [30] * Zhang, et al. [49] | - | - | |
| Bcl-2 | * Zhang, et al. [49] | - | - | |


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
4. Discussion
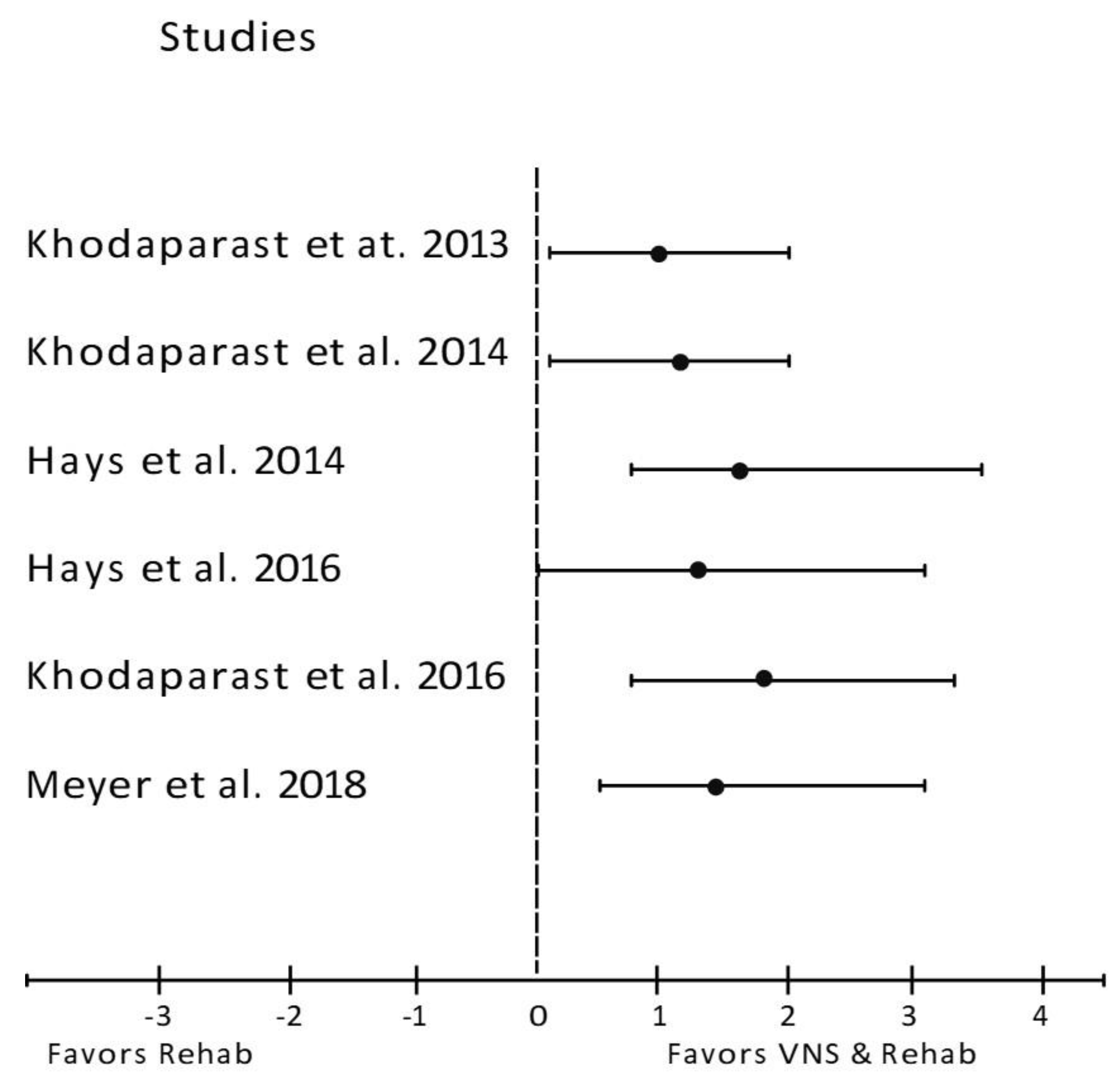
4.1. VNS Improves the Primary Indications of Stroke in Infarct Volume, Neurological Deficit Score, and Forelimb Strength
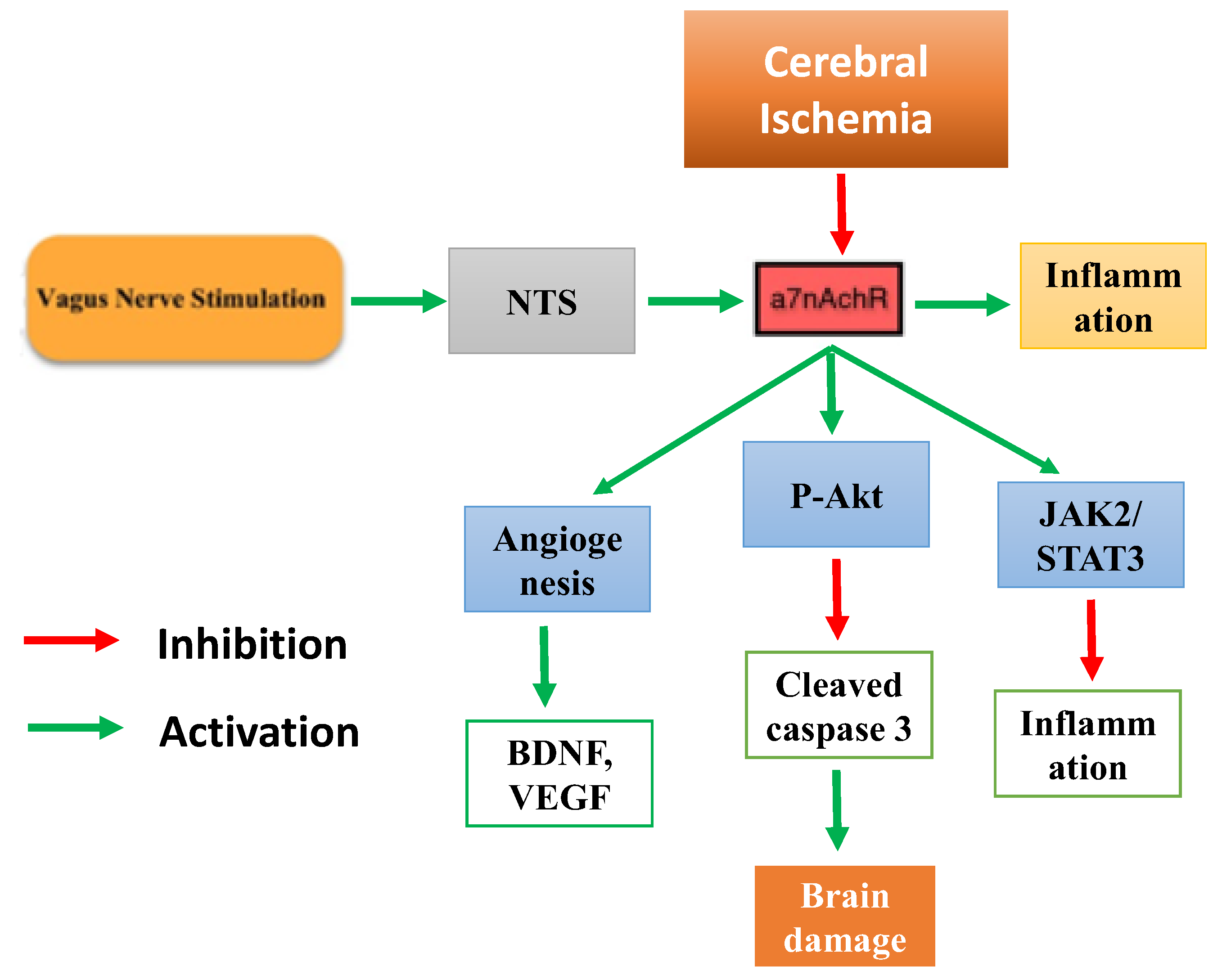
4.2. VNS Improves Stroke via the Nicotinic Anti-Inflammatory Pathway
4.3. Apoptosis
4.4. Angiogenesis
4.5. Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Feigin, V.L.; Roth, G.A.; Naghavi, M.; Parmar, P.; Krishnamurthi, R.; Chugh, S.; Mensah, G.A.; Norrving, B.; Shiue, I.; Ng, M.; et al. Global burden of stroke and risk factors in 188 countries, during 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet Neurol. 2016, 15, 913–924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuriakose, D.; Xiao, Z. Pathophysiology and Treatment of Stroke: Present Status and Future Perspectives. Int. J. Mol. Sci. 2020, 21, 7609. [Google Scholar] [CrossRef] [PubMed]
- Sandercock, P.; Wardlaw, J.M.; Lindley, R.I.; Dennis, M.; Cohen, G.; Murray, G.; Innes, K.; Venables, G.; Czlonkowska, A.; Kobayashi, A.; et al. The benefits and harms of intravenous thrombolysis with recombinant tissue plasminogen activator within 6 h of acute ischaemic stroke (the third international stroke trial [IST-3]): A randomised controlled trial. Lancet 2012, 379, 2352–2363. [Google Scholar] [PubMed] [Green Version]
- Hui, C.; Tadi, P.; Patti, L. Ischemic Stroke. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Catanese, L.; Tarsia, J.; Fisher, M. Acute Ischemic Stroke Therapy Overview. Circ. Res. 2017, 120, 541–558. [Google Scholar] [CrossRef] [PubMed]
- Herpich, F.; Rincon, F. Management of Acute Ischemic Stroke. Crit. Care Med. 2020, 48, 1654–1663. [Google Scholar] [CrossRef]
- Knecht, T.; Borlongan, C.; Dela Peña, I. Combination therapy for ischemic stroke: Novel approaches to lengthen therapeutic window of tissue plasminogen activator. Brain Circ. 2018, 4, 99–108. [Google Scholar]
- Spindler, P.; Bohlmann, K.; Straub, H.-B.; Vajkoczy, P.; Schneider, U.C. Effects of vagus nerve stimulation on symptoms of depression in patients with difficult-to-treat epilepsy. Seizure 2019, 69, 77–79. [Google Scholar] [CrossRef]
- Austelle, C.W.; O’Leary, G.H.; Thompson, S.; Gruber, E.; Kahn, A.; Manett, A.J.; Short, B.; Badran, B.W. A Comprehensive Review of Vagus Nerve Stimulation for Depression. Neuromodulation 2022, 25, 309–315. [Google Scholar] [CrossRef]
- Engineer, N.D.; Kimberley, T.J.; Prudente, C.N.; Dawson, J.; Tarver, W.B.; Hays, S.A. Targeted Vagus Nerve Stimulation for Rehabilitation After Stroke. Front. Neurosci. 2019, 13, 280. [Google Scholar] [CrossRef] [Green Version]
- Chung, C.H.; Bretherton, B.; Zainalabidin, S.; Deuchars, S.A.; Deuchars, J.; Mahadi, M.K. Mediation of Cardiac Macrophage Activity via Auricular Vagal Nerve Stimulation Ameliorates Cardiac Ischemia/Reperfusion Injury. Front. Neurosci. 2020, 14, 906. [Google Scholar] [CrossRef]
- Parada, E.; Egea, J.; Romero, A.; del Barrio, L.; García, A.G.; López, M.G. Poststress treatment with PNU282987 can rescue SH-SY5Y cells undergoing apoptosis via α7 nicotinic receptors linked to a Jak2/Akt/HO-1 signaling pathway. Free Radic. Biol. Med. 2010, 49, 1815–1821. [Google Scholar] [CrossRef]
- Cheyuo, C.; Jacob, A.; Wu, R.; Zhou, M.; Coppa, G.F.; Wang, P. The parasympathetic nervous system in the quest for stroke therapeutics. J. Cereb. Blood Flow Metab. 2011, 31, 1187–1195. [Google Scholar] [CrossRef]
- Dawson, J.; Liu, C.Y.; Francisco, G.E.; Cramer, S.C.; Wolf, S.L.; Dixit, A.; Alexander, J.; Ali, R.; Brown, B.L.; Feng, W.; et al. Vagus nerve stimulation paired with rehabilitation for upper limb motor function after ischaemic stroke (VNS-REHAB): A randomised, blinded, pivotal, device trial. Lancet 2021, 397, 1545–1553. [Google Scholar] [CrossRef]
- Xie, Y.L.; Wang, S.; Wu, Q.; Chen, X. Vagus nerve stimulation for upper limb motor impairment after ischemic stroke: A meta-analysis. Medicine 2021, 100, e27871. [Google Scholar] [CrossRef]
- Redgrave, J.N.; Moore, L.; Oyekunle, T.; Ebrahim, M.; Falidas, K.; Snowdon, N.; Ali, A.; Majid, A. Transcutaneous Auricular Vagus Nerve Stimulation with Concurrent Upper Limb Repetitive Task Practice for Poststroke Motor Recovery: A Pilot Study. J. Stroke Cerebrovasc. Dis. 2018, 27, 1998–2005. [Google Scholar] [CrossRef]
- Baig, S.S.; Falidas, K.; Laud, P.J.; Snowdon, N.; Farooq, M.U.; Ali, A.; Majid, A.; Redgrave, J.N. Transcutaneous Auricular Vagus Nerve Stimulation with Upper Limb Repetitive Task Practice May Improve Sensory Recovery in Chronic Stroke. J. Stroke Cerebrovasc. Dis. 2019, 28, 104348. [Google Scholar] [CrossRef]
- Langendam, M.W.; Magnuson, K.; Williams, A.R.; Walker, V.R.; Howdeshell, K.L.; Rooney, A.A.; Hooijmans, C.R. Developing a database of systematic reviews of animal studies. Regul. Toxicol. Pharmacol. RTP 2021, 123, 104940. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- US Department of Health and Human Services. OHAT, Risk of Bias Rating Tool for Human and Animal Studies; US Department of Health and Human Services: Triangle Park, NC, USA, 2015. [Google Scholar]
- Xiang, Y.X.; Wang, W.X.; Xue, Z.; Zhu, L.; Wang, S.B.; Sun, Z.H. Electrical stimulation of the vagus nerve protects against cerebral ischemic injury through an anti-infammatory mechanism. Neural Regen. Res. 2015, 10, 576–582. [Google Scholar]
- Ay, I.; Napadow, V.; Ay, H. Electrical stimulation of the vagus nerve dermatome in the external ear is protective in rat cerebral ischemia. Brain Stimul. 2015, 8, 7–12. [Google Scholar] [CrossRef] [Green Version]
- Ay, I.; Nasser, R.; Simon, B.; Ay, H. Transcutaneous Cervical Vagus Nerve Stimulation Ameliorates Acute Ischemic Injury in Rats. Brain Stimul. 2016, 9, 166–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.; Yang, L.Y.; Orban, L.; Cuylear, D.; Thompson, J.; Simon, B.; Yang, Y. Non-invasive vagus nerve stimulation reduces blood-brain barrier disruption in a rat model of ischemic stroke. Brain Stimul. 2018, 11, 689–698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindemann, J.; Rakers, C.; Matuskova, H.; Simon, B.J.; Kinfe, T.; Petzold, G.C. Vagus nerve stimulation reduces spreading depolarization burden and cortical infarct volume in a rat model of stroke. PLoS ONE 2020, 15, e0236444. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Liu, Y.; Wang, S.; Long, L.; Zang, Q.; Ma, J.; Yu, L.; Jia, G. Vagus nerve stimulation mediates microglia M1/2 polarization via inhibition of TLR4 pathway after ischemic stroke. Biochem. Biophys. Res. Commun. 2021, 577, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Lu, X.X.; Hong, Z.Q.; Tan, Z.; Sui, M.H.; Zhuang, Z.Q.; Liu, H.H.; Zheng, X.Y.; Yan, T.B.; Geng, D.F.; Jin, D.M. Nicotinic Acetylcholine Receptor Alpha7 Subunit Mediates Vagus Nerve Stimulation-Induced Neuroprotection in Acute Permanent Cerebral Ischemia by a7nAchR/JAK2 Pathway. Med. Sci. Monit. 2017, 23, 6072–6081. [Google Scholar] [CrossRef] [Green Version]
- Long, L.; Zang, Q.; Jia, G.; Fan, M.; Zhang, L.; Qi, Y.; Liu, Y.; Yu, L.; Wang, S. Transcutaneous Auricular Vagus Nerve Stimulation Promotes White Matter Repair and Improves Dysphagia Symptoms in Cerebral Ischemia Model Rats. Front. Behav. Neurosci. 2022, 16, 811419. [Google Scholar] [CrossRef]
- Zhao, J.J.; Wang, Z.H.; Zhang, Y.J.; Wang, W.J.; Cheng, A.F.; Rong, P.J.; Shan, C.L. The mechanisms through which auricular vagus nerve stimulation protects against cerebral ischemia/reperfusion injury. Neural Regen. Res. 2022, 17, 594–600. [Google Scholar]
- Jiang, Y.; Li, L.; Liu, B.; Zhang, Y.; Chen, Q.; Li, C. Vagus nerve stimulation attenuates cerebral ischemia and reperfusion injury via endogenous cholinergic pathway in rat. PLoS ONE 2014, 9, e102342. [Google Scholar] [CrossRef]
- Hiraki, T.; Baker, W.; Greenberg, J.H. Effect of vagus nerve stimulation during transient focal cerebral ischemia on chronic outcome in rats. J. Neurosci. Res. 2012, 90, 887–894. [Google Scholar] [CrossRef] [Green Version]
- Ay, I.; Sorensen, A.G.; Ay, H. Vagus nerve stimulation reduces infarct size in rat focal cerebral ischemia: An unlikely role for cerebral blood flow. Brain Res. 2011, 1392, 110–115. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Q.; Lu, Y.; Bian, H.; Guo, L.; Zhu, H. Activation of the α7 nicotinic receptor promotes lipopolysaccharide-induced conversion of M1 microglia to M2. Am. J. Transl. Res. 2017, 9, 971–985. [Google Scholar]
- Jiang, Y.; Li, L.; Tan, X.; Liu, B.; Zhang, Y.; Li, C. miR-210 mediates vagus nerve stimulation-induced antioxidant stress and anti-apoptosis reactions following cerebral ischemia/reperfusion injury in rats. J. Neurochem. 2015, 134, 173–181. [Google Scholar] [CrossRef]
- Ay, I.; Lu, J.; Ay, H.; Gregory Sorensen, A. Vagus nerve stimulation reduces infarct size in rat focal cerebral ischemia. Neurosci. Lett. 2009, 459, 147–151. [Google Scholar] [CrossRef]
- Yang, L.Y.; Bhaskar, K.; Thompson, J.; Duval, K.; Torbey, M.; Yang, Y. Non-invasive vagus nerve stimulation reduced neuron-derived IL-1β and neuroinflammation in acute ischemic rat brain. Brain Hemorrhages 2022, 3, 45–56. [Google Scholar] [CrossRef]
- Li, J.; Zhang, K.; Zhang, Q.; Zhou, X.; Wen, L.; Ma, J.; Niu, L.; Li, C. PPAR-γ Mediates Ta-VNS-Induced Angiogenesis and Subsequent Functional Recovery after Experimental Stroke in Rats. BioMed Res. Int. 2020, 2020, 8163789. [Google Scholar]
- Jiang, Y.; Li, L.; Ma, J.; Zhang, L.; Niu, F.; Feng, T.; Li, C. Auricular vagus nerve stimulation promotes functional recovery and enhances the post-ischemic angiogenic response in an ischemia/reperfusion rat model. Neurochem. Int. 2016, 97, 73–82. [Google Scholar] [CrossRef]
- Ekici, F.; Karson, A.; Dillioglugil, M.O.; Gurol, G.; Kir, H.M.; Ates, N. The effects of vagal nerve stimulation in focal cerebral ischemia and reperfusion model. Turk. Neurosurg. 2013, 23, 451–457. [Google Scholar]
- Sun, Z.; Baker, W.; Hiraki, T.; Greenberg, J.H. The effect of right vagus nerve stimulation on focal cerebral ischemia: An experimental study in the rat. Brain Stimul. 2012, 5, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Jiang, Y.; Li, L.; Liu, B.; Zhang, Y.; Chen, Q.; Li, C. PPARγ upregulation induced by vagus nerve stimulation exerts anti-inflammatory effect in cerebral ischemia/reperfusion rats. Med. Sci. Monit. 2015, 21, 268–275. [Google Scholar]
- Zhao, X.P.; Zhao, Y.; Qin, X.Y.; Wan, L.Y.; Fan, X.X. Non-invasive Vagus Nerve Stimulation Protects Against Cerebral Ischemia/Reperfusion Injury and Promotes Microglial M2 Polarization Via Interleukin-17A Inhibition. J. Mol. Neurosci. 2019, 67, 217–226. [Google Scholar] [CrossRef]
- Khodaparast, N.; Hays, S.A.; Sloan, A.M.; Hulsey, D.R.; Ruiz, A.; Pantoja, M.; Rennaker, R.L., 2nd; Kilgard, M.P. Vagus nerve stimulation during rehabilitative training improves forelimb strength following ischemic stroke. Neurobiol. Dis. 2013, 60, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Hays, S.A.; Khodaparast, N.; Ruiz, A.; Sloan, A.M.; Hulsey, D.R.; Rennaker, R.L., 2nd; Kilgard, M.P. The timing and amount of vagus nerve stimulation during rehabilitative training affect poststroke recovery of forelimb strength. Neuroreport 2014, 25, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Hays, S.A.; Ruiz, A.; Bethea, T.; Khodaparast, N.; Carmel, J.B.; Rennaker, R.L., 2nd; Kilgard, M.P. Vagus nerve stimulation during rehabilitative training enhances recovery of forelimb function after ischemic stroke in aged rats. Neurobiol. Aging 2016, 43, 111–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khodaparast, N.; Hays, S.A.; Sloan, A.M.; Fayyaz, T.; Hulsey, D.R.; Rennaker, R.L., 2nd; Kilgard, M.P. Vagus nerve stimulation delivered during motor rehabilitation improves recovery in a rat model of stroke. Neurorehabil. Neural Repair 2014, 28, 698–706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khodaparast, N.; Kilgard, M.P.; Casavant, R.; Ruiz, A.; Qureshi, I.; Ganzer, P.D.; Rennaker, R.L., 2nd; Hays, S.A. Vagus Nerve Stimulation During Rehabilitative Training Improves Forelimb Recovery After Chronic Ischemic Stroke in Rats. Neurorehabil. Neural Repair 2016, 30, 676–684. [Google Scholar] [CrossRef] [Green Version]
- Meyers, E.C.; Solorzano, B.R.; James, J.; Ganzer, P.D.; Lai, E.S.; Rennaker, R.L.; Kilgard, M.P.; Hays, S.A. Vagus Nerve Stimulation Enhances Stable Plasticity and Generalization of Stroke Recovery. Stroke 2018, 49, 710–717. [Google Scholar] [CrossRef]
- Zhang, L.; Ma, J.; Jin, X.; Jia, G.; Jiang, Y.; Li, C. L-PGDS Mediates Vagus Nerve Stimulation-Induced Neuroprotection in a Rat Model of Ischemic Stroke by Suppressing the Apoptotic Response. Neurochem. Res. 2017, 42, 644–655. [Google Scholar] [CrossRef]
- Li, J.; Zhang, Q.; Li, S.; Niu, L.; Ma, J.; Wen, L.; Zhang, L.; Li, C. α7nAchR mediates transcutaneous auricular vagus nerve stimulation-induced neuroprotection in a rat model of ischemic stroke by enhancing axonal plasticity. Neurosci. Lett. 2020, 730, 135031. [Google Scholar] [CrossRef]
- Zhang, L.N.; Zhang, X.W.; Li, C.Q.; Guo, J.; Chen, Y.P.; Chen, S.L. Vagal Nerve Stimulation Protects Against Cerebral Ischemia-Reperfusion Injury in Rats by Inhibiting Autophagy and Apoptosis. Neuropsychiatr. Dis. Treat. 2021, 17, 905–913. [Google Scholar] [CrossRef]
- O’Collins, V.E.; Donnan, G.A.; Macleod, M.R.; Howells, D.W. Chapter 20—Animal Models of Ischemic Stroke Versus Clinical Stroke: Comparison of Infarct Size, Cause, Location, Study Design, and Efficacy of Experimental Therapies. In Animal Models for the Study of Human Disease, 2nd ed.; Conn, P.M., Ed.; Academic Press: Cambridge, MA, USA, 2017; pp. 481–523. [Google Scholar]
- Tourdias, T.; Renou, P.; Sibon, I.; Asselineau, J.; Bracoud, L.; Dumoulin, M.; Rouanet, F.; Orgogozo, J.M.; Dousset, V. Final cerebral infarct volume is predictable by MR imaging at 1 week. AJNR Am. J. Neuroradiol. 2011, 32, 352–358. [Google Scholar] [CrossRef] [Green Version]
- Abeysinghe, H.C.S.; Roulston, C.L. A Complete Guide to Using the Endothelin-1 Model of Stroke in Conscious Rats for Acute and Long-Term Recovery Studies. Methods Mol. Biol. 2018, 1717, 115–133. [Google Scholar]
- Tracey, K.J. Physiology and immunology of the cholinergic antiinflammatory pathway. J. Clin. Investig. 2007, 117, 289–296. [Google Scholar] [CrossRef] [Green Version]
- Oke, S.L.; Tracey, K.J. The inflammatory reflex and the role of complementary and alternative medical therapies. Ann. N. Y. Acad. Sci. 2009, 1172, 172–180. [Google Scholar] [CrossRef]
- Chunchai, T.; Samniang, B.; Sripetchwandee, J.; Pintana, H.; Pongkan, W.; Kumfu, S.; Shinlapawittayatorn, K.; KenKnight, B.H.; Chattipakorn, N.; Chattipakorn, S.C. Vagus Nerve Stimulation Exerts the Neuroprotective Effects in Obese-Insulin Resistant Rats, Leading to the Improvement of Cognitive Function. Sci. Rep. 2016, 6, 26866. [Google Scholar] [CrossRef] [Green Version]
- Lazou, A.; Iliodromitis, E.K.; Cieslak, D.; Voskarides, K.; Mousikos, S.; Bofilis, E.; Kremastinos, D.T. Ischemic but not mechanical preconditioning attenuates ischemia/reperfusion induced myocardial apoptosis in anaesthetized rabbits: The role of Bcl-2 family proteins and ERK1/2. Apoptosis 2006, 11, 2195–2204. [Google Scholar] [CrossRef]
- Ma, J.; Zhang, L.; He, G.; Tan, X.; Jin, X.; Li, C. Transcutaneous auricular vagus nerve stimulation regulates expression of growth differentiation factor 11 and activin-like kinase 5 in cerebral ischemia/reperfusion rats. J. Neurol. Sci. 2016, 369, 27–35. [Google Scholar] [CrossRef]
- Kawada, T.; Yamazaki, T.; Akiyama, T.; Li, M.; Zheng, C.; Shishido, T.; Mori, H.; Sugimachi, M. Angiotensin II attenuates myocardial interstitial acetylcholine release in response to vagal stimulation. Am. J. Physiol.-Heart Circ. Physiol. 2007, 293, H2516–H2522. [Google Scholar] [CrossRef]
- Du, L.; Yang, Z.; Sheng, H.; Liu, M.; Sun, Q. Effects of Long-Term Vagus Nerve Electrical Stimulation Therapy on Acute Cerebral Infarction and Neurological Function Recovery in Post MCAO Mice. Oxid. Med. Cell. Longev. 2022, 2022, 8131391. [Google Scholar] [CrossRef]
- Alrafiah, A.; Alofi, E.; Almohaya, Y.; Hamami, A.; Qadah, T.; Almaghrabi, S.; Hakami, N.; Alrawaili, M.; Tayeb, H. Angiogenesis Biomarkers in Ischemic Stroke Patients. J. Inflamm. Res. 2021, 14, 4893–4900. [Google Scholar] [CrossRef]
- Seto, S.W.; Chang, D.; Jenkins, A.; Bensoussan, A.; Kiat, H. Angiogenesis in Ischemic Stroke and Angiogenic Effects of Chinese Herbal Medicine. J. Clin. Med. 2016, 5, 56. [Google Scholar] [CrossRef] [Green Version]
- Arenillas, J.F.; Sobrino, T.; Castillo, J.; Dávalos, A. The role of angiogenesis in damage and recovery from ischemic stroke. Curr. Treat. Opt. Cardiovasc. Med. 2007, 9, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Yuan, H.; Silberstein, S.D. Vagus Nerve and Vagus Nerve Stimulation, a Comprehensive Review: Part II. Headache 2016, 56, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Wang, X.; O’Connor, M.; Wang, G.; Han, F. Brain-Derived Neurotrophic Factor and Its Potential Therapeutic Role in Stroke Comorbidities. Neural Plast. 2020, 2020, 1969482. [Google Scholar] [CrossRef] [PubMed]
- Navaratna, D.; Guo, S.; Arai, K.; Lo, E.H. Mechanisms and targets for angiogenic therapy after stroke. Cell Adhes. Migr. 2009, 3, 216–223. [Google Scholar] [CrossRef] [Green Version]
- Zhao, G.; Li, W.Y.; Chen, D.; Henry, J.R.; Li, H.Y.; Chen, Z.; Zia-Ebrahimi, M.; Bloem, L.; Zhai, Y.; Huss, K.; et al. A novel, selective inhibitor of fibroblast growth factor receptors that shows a potent broad spectrum of antitumor activity in several tumor xenograft models. Mol. Cancer Ther. 2011, 10, 2200–2210. [Google Scholar] [CrossRef] [Green Version]
- Kallmann, B.A.; Wagner, S.; Hummel, V.; Buttmann, M.; Bayas, A.; Tonn, J.C.; Rieckmann, P. Characteristic gene expression profile of primary human cerebral endothelial cells. FASEB J. 2002, 16, 589–591. [Google Scholar] [CrossRef]
- Schäbitz, W.R.; Steigleder, T.; Cooper-Kuhn, C.M.; Schwab, S.; Sommer, C.; Schneider, A.; Kuhn, H.G. Intravenous brain-derived neurotrophic factor enhances poststroke sensorimotor recovery and stimulates neurogenesis. Stroke 2007, 38, 2165–2172. [Google Scholar] [CrossRef] [Green Version]
- Hossmann, K.-A. The Two Pathophysiologies of Focal Brain Ischemia: Implications for Translational Stroke Research. J. Cereb. Blood Flow Metab. 2012, 32, 1310–1316. [Google Scholar] [CrossRef] [Green Version]
- Verma, N.; Mudge, J.D.; Kasole, M.; Chen, R.C.; Blanz, S.L.; Trevathan, J.K.; Lovett, E.G.; Williams, J.C.; Ludwig, K.A. Auricular Vagus Neuromodulation—A Systematic Review on Quality of Evidence and Clinical Effects. Front. Neurosci. 2021, 15, 664740. [Google Scholar] [CrossRef]
- Pelot, N.A.; Goldhagen, G.B.; Cariello, J.E.; Musselman, E.D.; Clissold, K.A.; Ezzell, J.A.; Grill, W.M. Quantified Morphology of the Cervical and Subdiaphragmatic Vagus Nerves of Human, Pig, and Rat. Front. Neurosci. 2020, 14, 601479. [Google Scholar] [CrossRef]
- Mahadi, K.M.; Lall, V.K.; Deuchars, S.A.; Deuchars, J. Cardiovascular autonomic effects of transcutaneous auricular nerve stimulation via the tragus in the rat involve spinal cervical sensory afferent pathways. Brain Stimul. 2019, 12, 1151–1158. [Google Scholar] [CrossRef]
- Cooper, C.M.; Farrand, A.Q.; Andresen, M.C.; Beaumont, E. Vagus nerve stimulation activates nucleus of solitary tract neurons via supramedullary pathways. J. Physiol. 2021, 599, 5261–5279. [Google Scholar] [CrossRef]
- Go, Y.Y.; Ju, W.M.; Lee, C.M.; Chae, S.W.; Song, J.J. Different Transcutaneous Auricular Vagus Nerve Stimulation Parameters Modulate the Anti-Inflammatory Effects on Lipopolysaccharide-Induced Acute Inflammation in Mice. Biomedicines 2022, 10, 247. [Google Scholar] [CrossRef]
- Zucker, I.; Beery, A.K. Males still dominate animal studies. Nature 2010, 465, 690. [Google Scholar] [CrossRef]
- Karp, N.A.; Reavey, N. Sex bias in preclinical research and an exploration of how to change the status quo. Br. J. Pharmacol. 2019, 176, 4107–4118. [Google Scholar] [CrossRef]


| Study | Selection Bias | Performance Bias | Attrition/Exclusion Bias | Detection Bias | Selective Reporting Bias |
|---|---|---|---|---|---|
| Xiang et al. 2015 [21] | ++ | − | + | + | ++ |
| Ay et al. 2015 [22] | ++ | ++ | + | + | ++ |
| Ay et al. 2016 [23] | ++ | ++ | + | − | ++ |
| Yang et al. 2018 [24] | ++ | ++ | + | ++ | + |
| Lindemann et al. 2020 [25] | ++ | + | + | + | + |
| Zhang et al. 2021 [26] | ++ | ++ | + | ++ | ++ |
| Lu et al. 2017 [27] | ++ | + | + | + | ++ |
| Long et al. 2022 [28] | ++ | ++ | + | + | ++ |
| Zhao et al. 2022 [29] | ++ | ++ | − | + | + |
| Jiang et al. 2014 [30] | + | ++ | + | + | ++ |
| Hiraki et al. 2012 [31] | ++ | + | + | + | ++ |
| Ay et al. 2011 [32] | + | + | + | + | + |
| Zhang et al. 2017 [33] | + | ++ | + | ++ | ++ |
| Jiang et al. 2015 [34] | ++ | ++ | + | ++ | ++ |
| Ay et al. 2009 [35] | ++ | ++ | + | + | ++ |
| Yang et al. 2022 [36] | ++ | + | + | + | + |
| Li et al. 2020 [37] | + | + | + | − | ++ |
| Jiang et al. 2016 [38] | + | + | + | − | ++ |
| Ekici et al. 2013 [39] | ++ | ++ | + | + | ++ |
| Sun et al. 2012 [40] | ++ | + | + | − | ++ |
| Jiang et al. 2015 [41] | ++ | ++ | + | − | ++ |
| Zhao et al. 2019 [42] | ++ | ++ | + | + | ++ |
| Li et al. 2020 [37] | ++ | ++ | + | ++ | ++ |
| Khodaprast et al. 2013 [43] | ++ | ++ | + | + | ++ |
| Hays et al. 2014 [44] | ++ | ++ | + | ++ | ++ |
| Hays et al. 2016 [45] | ++ | ++ | + | ++ | ++ |
| Khodaparast et al. 2014 [46] | ++ | ++ | + | ++ | ++ |
| Khodaparast et al. 2016 [47] | + | − | + | − | ++ |
| Meyers et al. 2018 [48] | ++ | + | + | ++ | + |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hasan, M.Y.; Siran, R.; Mahadi, M.K. The Effects of Vagus Nerve Stimulation on Animal Models of Stroke-Induced Injury: A Systematic Review. Biology 2023, 12, 555. https://doi.org/10.3390/biology12040555
Hasan MY, Siran R, Mahadi MK. The Effects of Vagus Nerve Stimulation on Animal Models of Stroke-Induced Injury: A Systematic Review. Biology. 2023; 12(4):555. https://doi.org/10.3390/biology12040555
Chicago/Turabian StyleHasan, Mohammad Yusuf, Rosfaiizah Siran, and Mohd Kaisan Mahadi. 2023. "The Effects of Vagus Nerve Stimulation on Animal Models of Stroke-Induced Injury: A Systematic Review" Biology 12, no. 4: 555. https://doi.org/10.3390/biology12040555
APA StyleHasan, M. Y., Siran, R., & Mahadi, M. K. (2023). The Effects of Vagus Nerve Stimulation on Animal Models of Stroke-Induced Injury: A Systematic Review. Biology, 12(4), 555. https://doi.org/10.3390/biology12040555