

Salivary Antioxidant Capacity and Magnesium in Generalized Anxiety Disorder

 , , , , , and
, , , , , and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Questionnaires
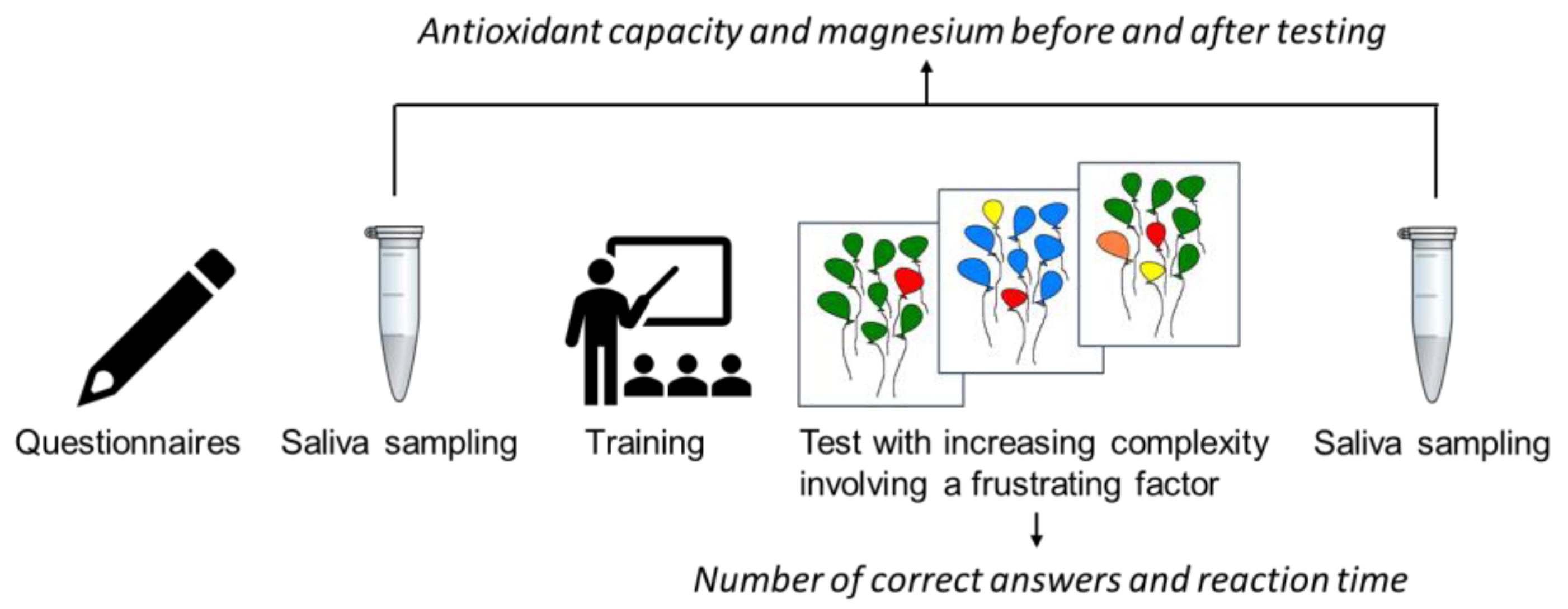
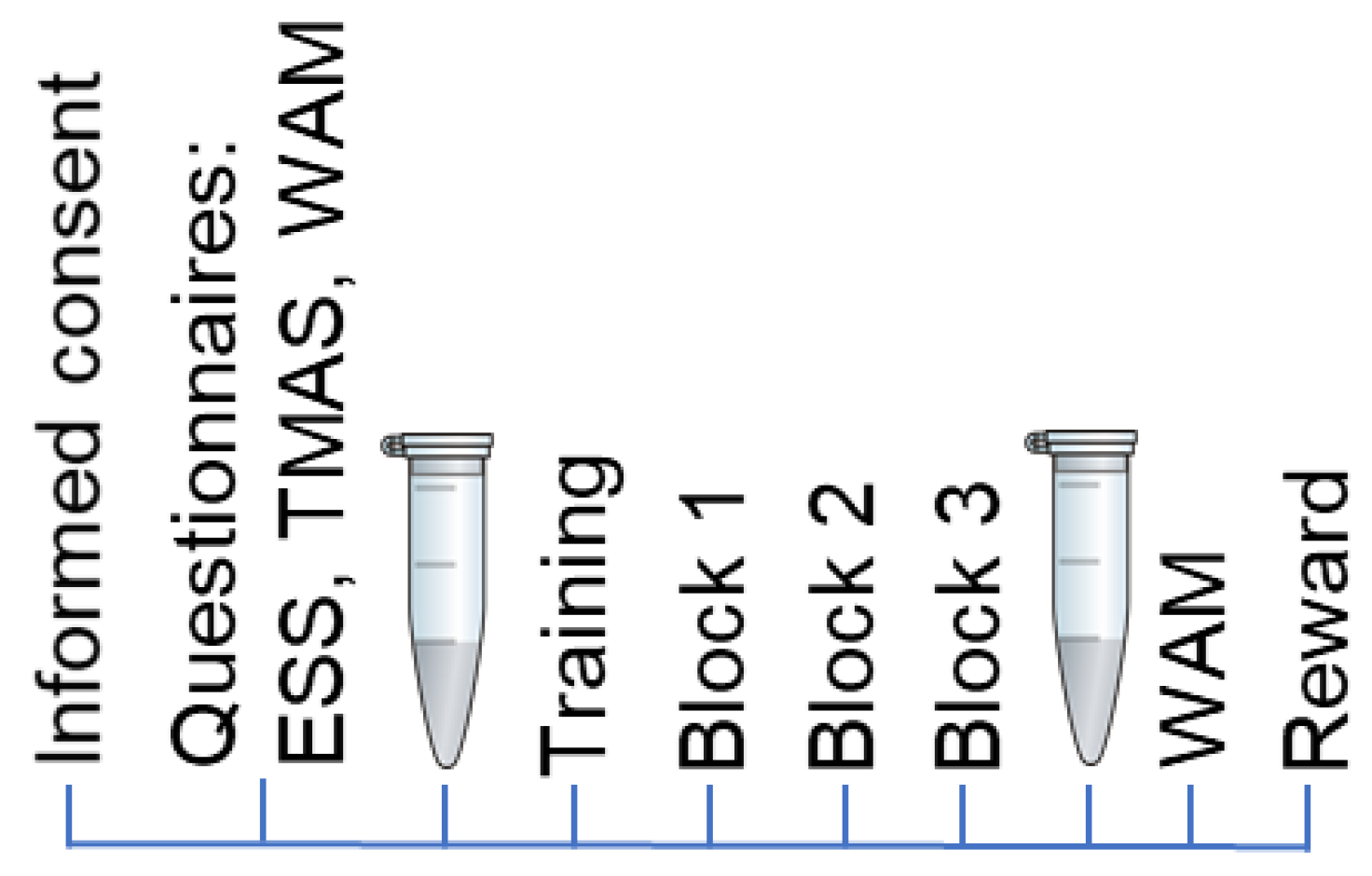
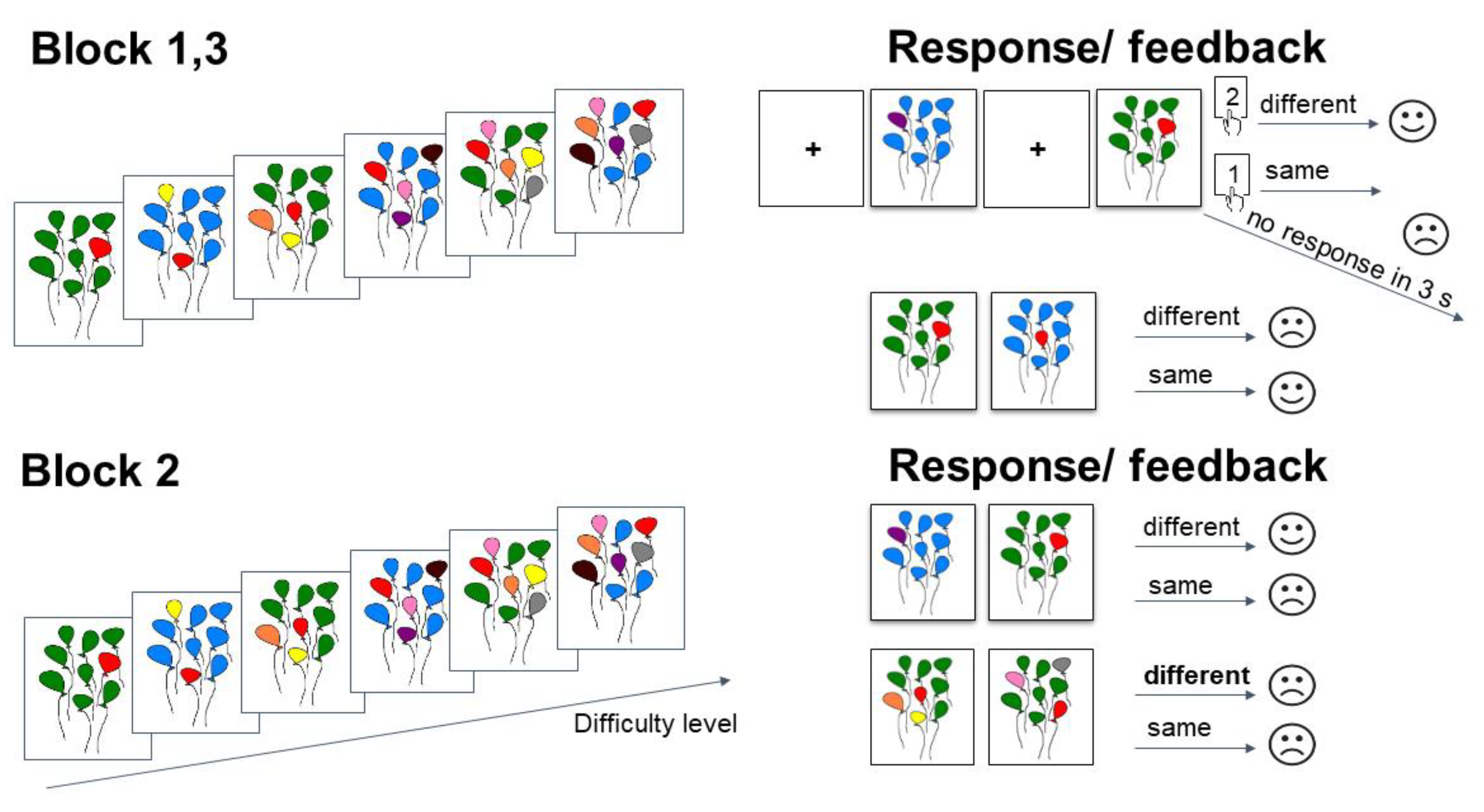
2.3. Stimuli and Protocol
2.4. Behavioral Data
2.5. Saliva Sampling
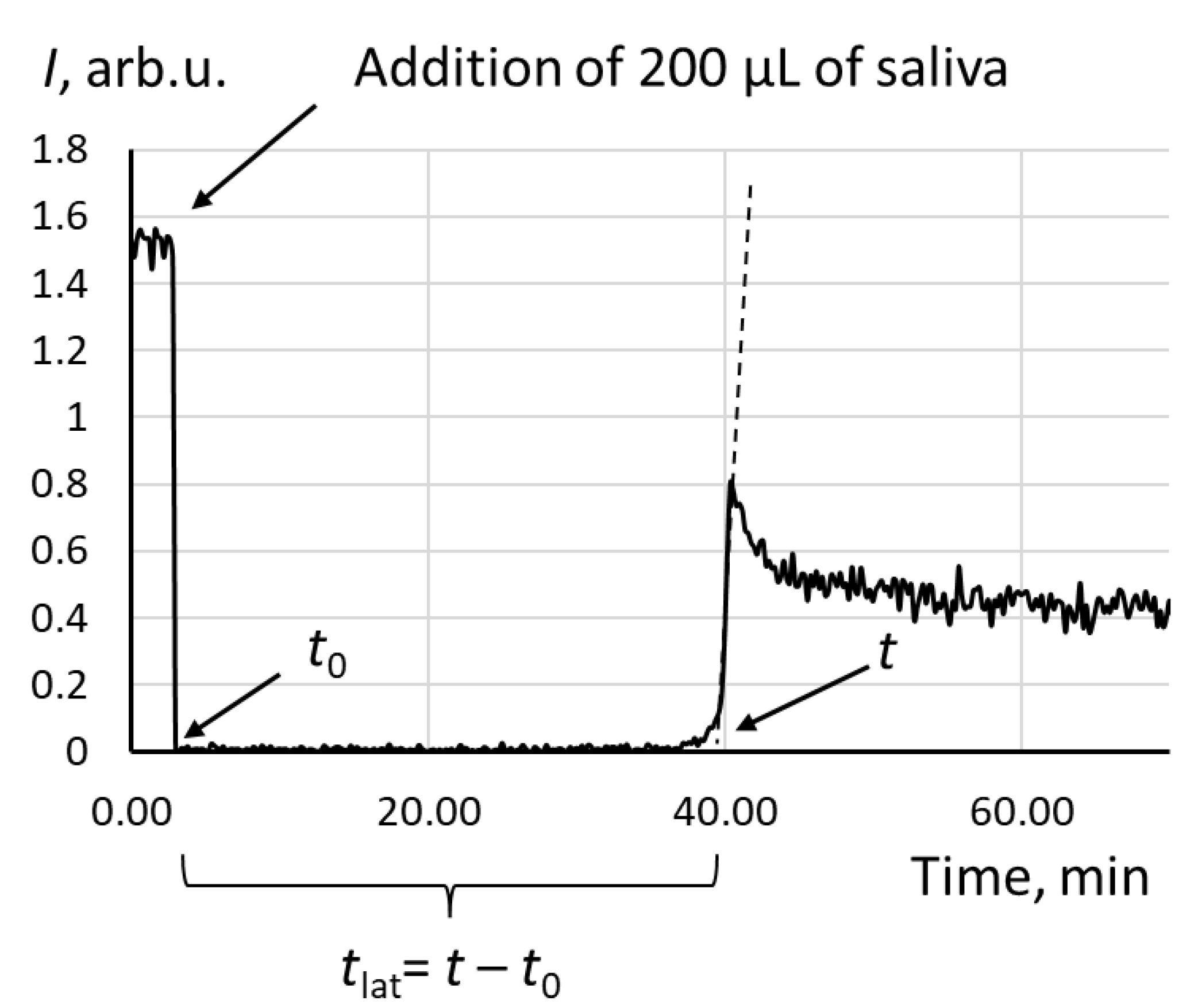
2.6. Assessment of Salivary Antioxidant Capacity
2.7. Quantitation of Magnesium
2.8. Statistical Analysis
3. Results
3.1. Behavioral Results
3.2. Total Antioxidant Capacity
3.3. Magnesium Quantitaion
3.4. Correlation Analysis between Saliva and Behavioral Results
4. Discussion
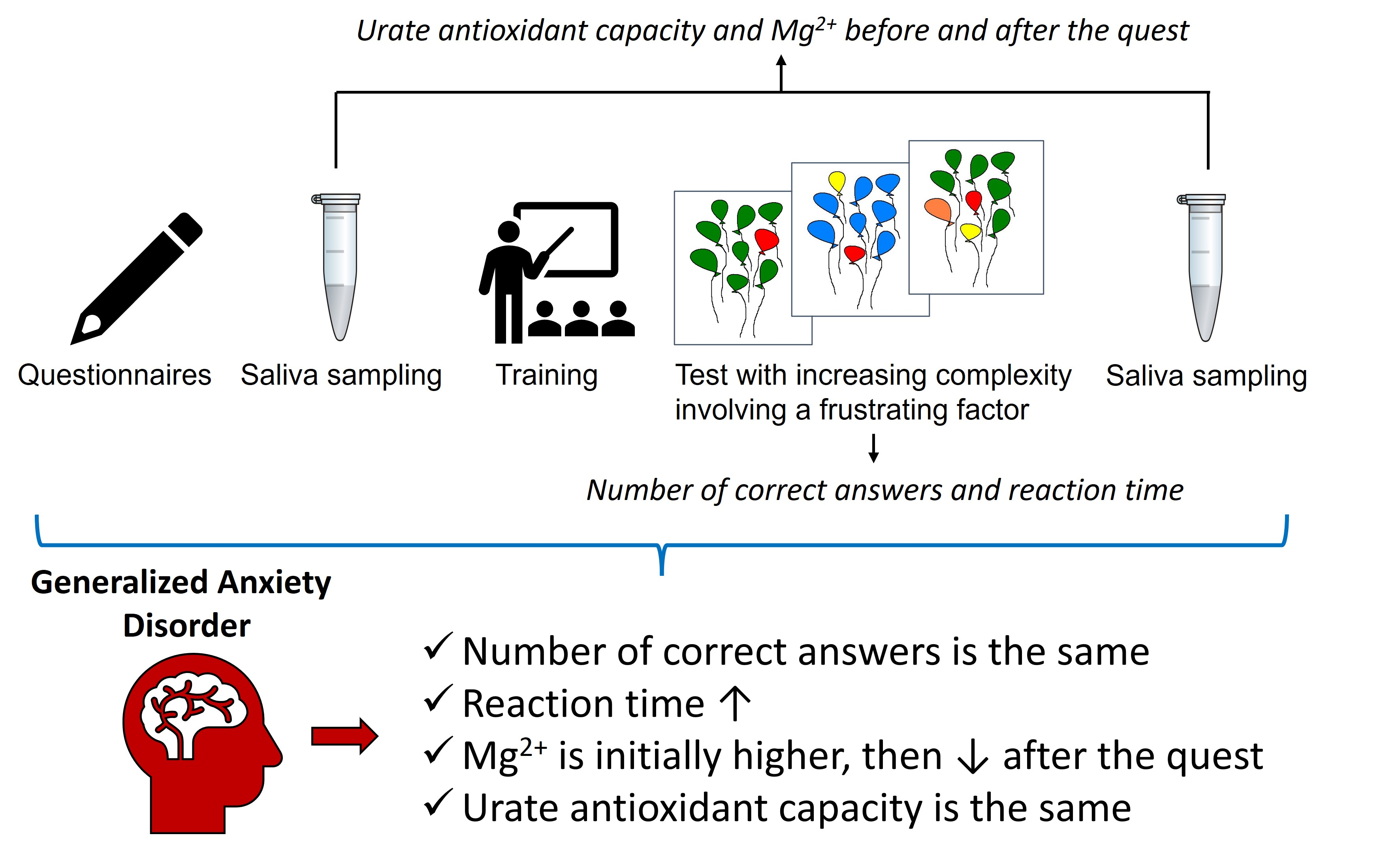
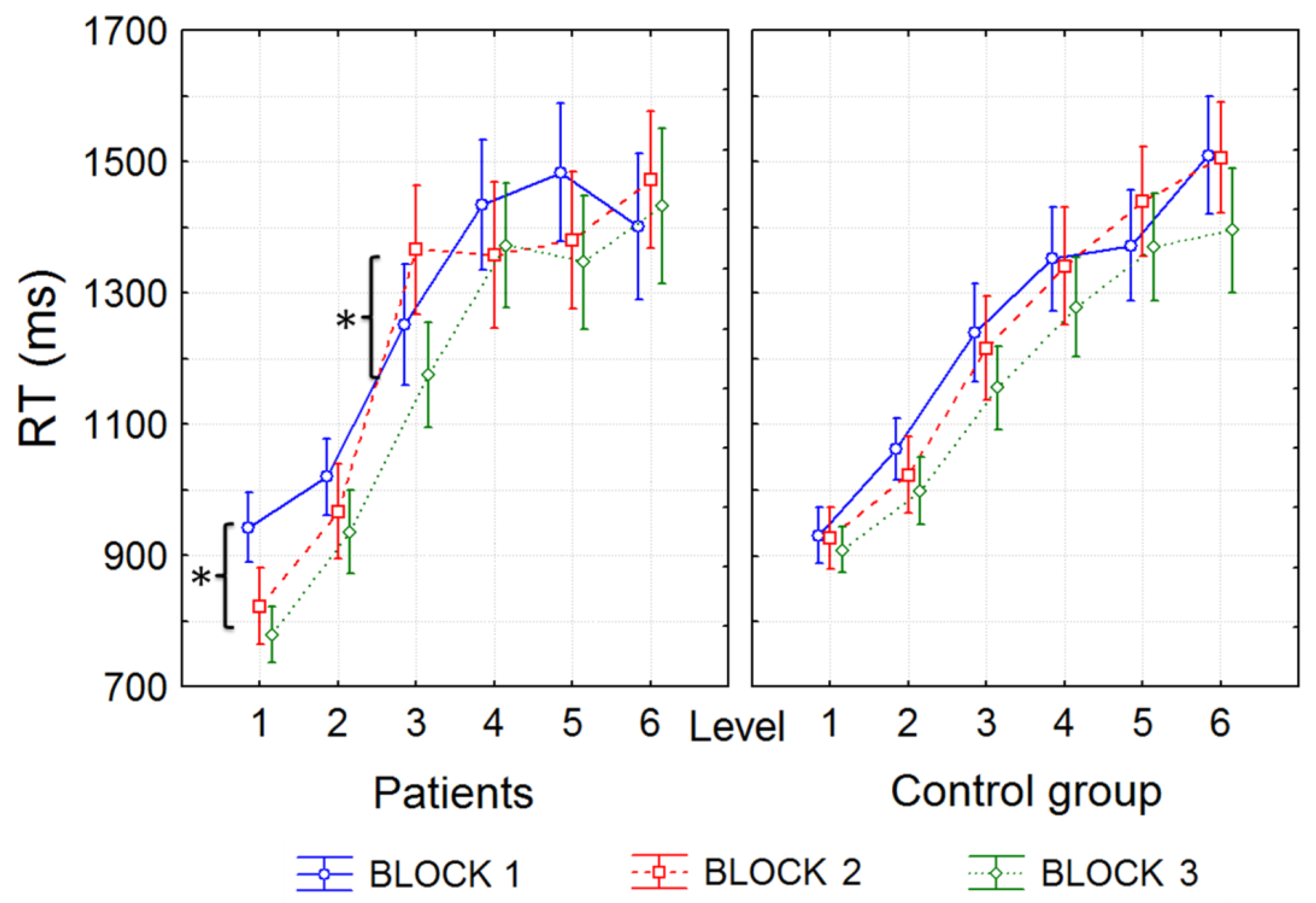
- There was no difference in the results of the quest (the number of correct answers and the total reward); however, anxious participants spent more time (the reaction time) at the moment of experimental frustration due to incorrect feedback and additional negative psycho-emotional load.
- There were no significant differences in antioxidant capacity in the groups both before and after the experimental session. Average antioxidant capacity also did not change significantly at the endpoint of the experiment. However, the endpoint antioxidant capacity correlated negatively with the reaction time in anxious patients in the second block (where the frustrating factor appeared).
- Magnesium in saliva was initially significantly higher in the group of anxious participants and decreased at the experiment endpoint; in healthy patients, there were no changes in salivary magnesium at the endpoint.
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- DeMartini, J.; Patel, G.; Fancher, T.L. Generalized Anxiety Disorder. Ann. Intern. Med. 2019, 170, ITC49–ITC64. [Google Scholar] [CrossRef]
- Malik, S.; Stead, T.S.; Mangal, R.; Ganti, L. General Anxiety Disorder in Youth: A National Survey. Health Psychol. Res. 2022, 10, 39578. [Google Scholar] [CrossRef] [PubMed]
- Gottschalk, M.G.; Domschke, K. Genetics of generalized anxiety disorder and related traits. Dialogues Clin. Neurosci. 2017, 19, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Park, S.E.; Kim, Y.H.; Yang, J.C.; Jeong, G.W. Comparative Functional Connectivity of Core Brain Regions between Implicit and Explicit Memory Tasks Underlying Negative Emotion in General Anxiety Disorder. Clin. Psychopharmacol. Neurosci. 2022, 20, 279–291. [Google Scholar] [CrossRef] [PubMed]
- Yuan, M.; Zhu, H.; Qiu, C.; Meng, Y.; Zhang, Y.; Ren, Z.; Li, Y.; Yuan, C.; Gao, M.; Lui, S.; et al. Altered regional and integrated resting-state brain activity in general social anxiety disorder patients before and after group cognitive behavior therapy. Psychiatry Res. Neuroimaging 2018, 272, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, E.; Lastra, S.; Urbina, M.; Carreira, I.; Lima, L. Serotonin, 5-hydroxyindoleacetic acid and serotonin transporter in blood peripheral lymphocytes of patients with generalized anxiety disorder. Int. Immunopharmacol. 2002, 2, 893–900. [Google Scholar] [CrossRef]
- Gerra, G.; Zaimovic, A.; Zambelli, U.; Timpano, M.; Reali, N.; Bernasconi, S.; Brambilla, F. Neuroendocrine responses to psychological stress in adolescents with anxiety disorder. Neuropsychobiology 2000, 42, 82–92. [Google Scholar] [CrossRef]
- Seddon, K.; Morris, K.; Bailey, J.; Potokar, J.; Rich, A.; Wilson, S.; Bettica, P.; Nutt, D.J. Effects of 7.5% CO2 challenge in generalized anxiety disorder. J. Psychopharmacol. 2011, 25, 43–51. [Google Scholar] [CrossRef]
- Bandelow, B.; Baldwin, D.; Abelli, M.; Bolea-Alamanac, B.; Bourin, M.; Chamberlain, S.R.; Cinosi, E.; Davies, S.; Domschke, K.; Fineberg, N.; et al. Biological markers for anxiety disorders, OCD and PTSD: A consensus statement. Part II: Neurochemistry, neurophysiology and neurocognition. World J. Biol. Psychiatry 2017, 18, 162–214. [Google Scholar] [CrossRef]
- Bankier, B.; Barajas, J.; Martinez-Rumayor, A.; Januzzi, J.L. Association between C-reactive protein and generalized anxiety disorder in stable coronary heart disease patients. Eur. Heart J. 2008, 29, 2212–2217. [Google Scholar] [CrossRef] [Green Version]
- Tofani, T.; Mannelli, L.; Zanardelli, M.; Ghelardini, C.; Pallanti, S. P.1.f.003 an immunologic profile study in drug-näive generalized anxiety non depressed patients: A pilot study. Eur. Neuropsychopharmacol. 2015, 25, S226. [Google Scholar] [CrossRef]
- Wang, X.; Lin, J.; Liu, Q.; Lv, X.; Wang, G.; Wei, J.; Zhu, G.; Chen, Q.; Tian, H.; Zhang, K.; et al. Major depressive disorder comorbid with general anxiety disorder: Associations among neuroticism, adult stress, and the inflammatory index. J. Psychiatr. Res. 2022, 148, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Dong, Z.; Shen, X.; Hao, Y.; Li, J.; Li, H.; Xu, H.; Yin, L.; Kuang, W. Gut Microbiome: A Potential Indicator for Differential Diagnosis of Major Depressive Disorder and General Anxiety Disorder. Front. Psychiatry 2021, 12, 651536. [Google Scholar] [CrossRef]
- Bulut, M.; Selek, S.; Bez, Y.; Karababa, I.F.; Kaya, M.C.; Gunes, M.; Emhan, A.; Aksoy, N.; Sir, A. Reduced PON1 enzymatic activity and increased lipid hydroperoxide levels that point out oxidative stress in generalized anxiety disorder. J. Affect. Disord. 2013, 150, 829–833. [Google Scholar] [CrossRef] [PubMed]
- Kaya, M.C.; Bez, Y.; Karababa, I.F.; Emhan, A.; Aksoy, N.; Bulut, M.; Gunes, M.; Atli, A.; Selek, S. Decreased serum sulphydryl levels as a sign of increased oxidative stress in generalized anxiety disorder. Psychiatry Investig. 2013, 10, 281–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emhan, A.; Selek, S.; Bayazit, H.; Fatih Karababa, I.; Kati, M.; Aksoy, N. Evaluation of oxidative and antioxidative parameters in generalized anxiety disorder. Psychiatry Res. 2015, 230, 806–810. [Google Scholar] [CrossRef] [PubMed]
- Ercan, A.C.; Bahceci, B.; Polat, S.; Cenker, O.C.; Bahceci, I.; Koroglu, A.; Sahin, K.; Hocaoglu, C. Oxidative status and prolidase activities in generalized anxiety disorder. Asian J. Psychiatry 2017, 25, 118–122. [Google Scholar] [CrossRef]
- Maes, M.; Bonifacio, K.L.; Morelli, N.R.; Vargas, H.O.; Moreira, E.G.; St Stoyanov, D.; Barbosa, D.S.; Carvalho, A.F.; Nunes, S.O.V. Generalized Anxiety Disorder (GAD) and Comorbid Major Depression with GAD Are Characterized by Enhanced Nitro-oxidative Stress, Increased Lipid Peroxidation, and Lowered Lipid-Associated Antioxidant Defenses. Neurotox. Res. 2018, 34, 489–510. [Google Scholar] [CrossRef]
- Roomruangwong, C.; Simeonova, D.S.; Stoyanov, D.S.; Anderson, G.; Carvalho, A.; Maes, M. Common Environmental Factors May Underpin the Comorbidity between Generalized Anxiety Disorder and Mood Disorders via Activated Nitro-Oxidative Pathways. Curr. Top. Med. Chem. 2018, 18, 1621–1640. [Google Scholar] [CrossRef]
- Islam, M.R.; Ahmed, M.U.; Islam, M.S.; Sayeed, M.S.; Sadia, F.; Chowdhury, Z.S.; Nahar, Z.; Hasnat, A. Comparative analysis of serum malondialdehyde, antioxidant vitamins and immunoglobulin levels in patients suffering from generalized anxiety disorder. Drug Res. 2014, 64, 406–411. [Google Scholar] [CrossRef]
- Cuciureanu, M.D.; Vink, R. Magnesium and stress. In Magnesium in the Central Nervous System; Vink, R., Nechifor, M., Eds.; University of Adelaide Press: Adelaide, Australia, 2011. [Google Scholar]
- Islam, M.R.; Ahmed, M.U.; Mitu, S.A.; Islam, M.S.; Rahman, G.K.; Qusar, M.M.; Hasnat, A. Comparative analysis of serum zinc, copper, manganese, iron, calcium, and magnesium level and complexity of interelement relations in generalized anxiety disorder patients. Biol. Trace Elem. Res. 2013, 154, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Oddoux, S.; Violette, P.; Cornet, J.; Akkoyun-Farinez, J.; Besnier, M.; Noel, A.; Rouillon, F. Effect of a Dietary Supplement Combining Bioactive Peptides and Magnesium on Adjustment Disorder with Anxiety: A Clinical Trial in General Practice. Nutrients 2022, 14, 2425. [Google Scholar] [CrossRef] [PubMed]
- Zhang, A.; Sun, H.; Wang, X. Saliva metabolomics opens door to biomarker discovery, disease diagnosis, and treatment. Appl. Biochem. Biotechnol. 2012, 168, 1718–1727. [Google Scholar] [CrossRef]
- Jarai, T.; Maasz, G.; Burian, A.; Bona, A.; Jambor, E.; Gerlinger, I.; Mark, L. Mass spectrometry-based salivary proteomics for the discovery of head and neck squamous cell carcinoma. Pathol. Oncol. Res. 2012, 18, 623–628. [Google Scholar] [CrossRef]
- Gardner, A.; Carpenter, G.; So, P.W. Salivary Metabolomics: From Diagnostic Biomarker Discovery to Investigating Biological Function. Metabolites 2020, 10, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hyvarinen, E.; Savolainen, M.; Mikkonen, J.J.W.; Kullaa, A.M. Salivary Metabolomics for Diagnosis and Monitoring Diseases: Challenges and Possibilities. Metabolites 2021, 11, 587. [Google Scholar] [CrossRef] [PubMed]
- Baima, G.; Iaderosa, G.; Citterio, F.; Grossi, S.; Romano, F.; Berta, G.N.; Buduneli, N.; Aimetti, M. Salivary metabolomics for the diagnosis of periodontal diseases: A systematic review with methodological quality assessment. Metabolomics 2021, 17, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Nijakowski, K.; Gruszczynski, D.; Kopala, D.; Surdacka, A. Salivary Metabolomics for Oral Squamous Cell Carcinoma Diagnosis: A Systematic Review. Metabolites 2022, 12, 294. [Google Scholar] [CrossRef]
- Panneerselvam, K.; Ishikawa, S.; Krishnan, R.; Sugimoto, M. Salivary Metabolomics for Oral Cancer Detection: A Narrative Review. Metabolites 2022, 12, 436. [Google Scholar] [CrossRef]
- Sugimoto, M. Salivary metabolomics for cancer detection. Expert Rev. Proteom. 2020, 17, 639–648. [Google Scholar] [CrossRef]
- Sturque, J.; Berquet, A.; Loison-Robert, L.S.; Ahossi, V.; Zwetyenga, N. Interest of studying the saliva metabolome, transcriptome and microbiome in screening for pancreatic cancer. J. Stomatol. Oral Maxillofac. Surg. 2019, 120, 554–558. [Google Scholar] [CrossRef]
- Battino, M.; Ferreiro, M.S.; Gallardo, I.; Newman, H.N.; Bullon, P. The antioxidant capacity of saliva. J. Clin. Periodontol. 2002, 29, 189–194. [Google Scholar] [CrossRef] [Green Version]
- Ialongo, C. Preanalytic of total antioxidant capacity assays performed in serum, plasma, urine and saliva. Clin. Biochem. 2017, 50, 356–363. [Google Scholar] [CrossRef]
- Peluso, I.; Raguzzini, A. Salivary and Urinary Total Antioxidant Capacity as Biomarkers of Oxidative Stress in Humans. Pathol. Res. Int. 2016, 2016, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gawron-Skarbek, A.; Prymont-Przyminska, A.; Sobczak, A.; Guligowska, A.; Kostka, T.; Nowak, D.; Szatko, F. A comparison of native and non-urate Total Antioxidant Capacity of fasting plasma and saliva among middle-aged and older subjects. Redox Rep. 2018, 23, 57–62. [Google Scholar] [CrossRef] [Green Version]
- Baima, G.; Iaderosa, G.; Corana, M.; Romano, F.; Citterio, F.; Giacomino, A.; Berta, G.N.; Aimetti, M. Macro and trace elements signature of periodontitis in saliva: A systematic review with quality assessment of ionomics studies. J. Periodontal Res. 2022, 57, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Inonu, E.; Hakki, S.S.; Kayis, S.A.; Nielsen, F.H. The Association Between Some Macro and Trace Elements in Saliva and Periodontal Status. Biol. Trace Elem. Res. 2020, 197, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Romano, F.; Castiblanco, A.; Spadotto, F.; Di Scipio, F.; Malandrino, M.; Berta, G.N.; Aimetti, M. ICP-Mass-Spectrometry Ionic Profile of Whole Saliva in Patients with Untreated and Treated Periodontitis. Biomedicines 2020, 8, 354. [Google Scholar] [CrossRef] [PubMed]
- Abbas, A.; Fadhil, N.; Gathwan, K.; Obadi, D.; Talal, S. Evaluation of Some Salivary Elements in Chronic Periodontitis Patients. IOSR J. Dent. Med. Sci. 2017, 16, 46–50. [Google Scholar] [CrossRef]
- Manea, A.; Nechifor, M. Research on plasma and saliva levels of some bivalent cations in patients with chronic periodontitis (salivary cations in chronic periodontitis). Med. Surg. J. 2014, 118, 439–449. [Google Scholar]
- Huang, Y.; Zhu, M.; Li, Z.; Sa, R.; Chu, Q.; Zhang, Q.; Zhang, H.; Tang, W.; Zhang, M.; Yin, H. Mass spectrometry-based metabolomic profiling identifies alterations in salivary redox status and fatty acid metabolism in response to inflammation and oxidative stress in periodontal disease. Free. Radic. Biol. Med. 2014, 70, 223–232. [Google Scholar] [CrossRef]
- Abid Aun, W. Inorganic ions level in saliva of patients with chronic periodontitis & healthy subjects. In Proceedings of the First National Conference for Iraqi Dental Colleges, Baghdad, Iraq, 24–26 February 2012; Volume 24. [Google Scholar]
- Zhirkov, A.A.; Yagov, V.V.; Antonenko, A.A.; Korotkov, A.S.; Zuev, B.K. Determination of the Mineral Composition of Human Saliva by Microplasma Atomic Emission Spectroscopy. J. Anal. Chem. 2020, 75, 63–66. [Google Scholar] [CrossRef]
- Johns, M.W. A new method for measuring daytime sleepiness: The Epworth sleepiness scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, J.A. A personality scale of manifest anxiety. J. Abnorm. Soc. Psychol. 1953, 48, 285–290. [Google Scholar] [CrossRef] [PubMed]
- Doskin, V.A.; Lavrentieva, N.A.; Miroshnikov, M.P.; Sharay, V.B. Test of differentiated self-assessment of the functional state. Quest. Psychol. 1973, 6, 141–145. [Google Scholar]
- Bachurina, V.; Arsalidou, M. Multiple levels of mental attentional demand modulate peak saccade velocity and blink rate. Heliyon 2022, 8, e08826. [Google Scholar] [CrossRef] [PubMed]
- Portnova, G.V.; Liaukovich, K.M.; Vasil’eva, L.N.; Alshanslaya, E.I. Vegetative and Behavioral Parameters with Increased Cognitive Load in Healthy Volunteers. Pavlov. J. High. Nervious Act. 2022, 72, 504–519. [Google Scholar] [CrossRef]
- Arsalidou, M.; Pascual-Leone, J.; Johnson, J. Misleading cues improve developmental assessment of working memory capacity: The color matching tasks. Cogn. Dev. 2010, 25, 262–277. [Google Scholar] [CrossRef]
- Alekseev, A.V.; Proskurnina, E.V.; Vladimirov, Y.A. Determination of Antioxidants by Sensitized Chemiluminescence Using 2,2′-azo-bis(2-amidinopropane). Mosc. Univ. Chem. Bull. 2012, 67, 127–132. [Google Scholar] [CrossRef]
- van Veen, J.F.; van Vliet, I.M.; de Rijk, R.H.; van Pelt, J.; Mertens, B.; Fekkes, D.; Zitman, F.G. Tryptophan depletion affects the autonomic stress response in generalized social anxiety disorder. Psychoneuroendocrinology 2009, 34, 1590–1594. [Google Scholar] [CrossRef]
- Hoehn-Saric, R.; McLeod, D.R.; Zimmerli, W.D. Somatic manifestations in women with generalized anxiety disorder. Psychophysiological responses to psychological stress. Arch. Gen. Psychiatry 1989, 46, 1113–1119. [Google Scholar] [CrossRef] [PubMed]
- Fisher, A.J.; Newman, M.G. Heart rate and autonomic response to stress after experimental induction of worry versus relaxation in healthy, high-worry, and generalized anxiety disorder individuals. Biol. Psychol. 2013, 93, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Tamura, A.; Maruyama, Y.; Ishitobi, Y.; Kawano, A.; Ando, T.; Ikeda, R.; Inoue, A.; Imanaga, J.; Okamoto, S.; Kanehisa, M.; et al. Salivary alpha-amylase and cortisol responsiveness following electrical stimulation stress in patients with the generalized type of social anxiety disorder. Pharmacopsychiatry 2013, 46, 225–260. [Google Scholar] [CrossRef] [PubMed]
- Funke, R.; Eichler, A.; Distler, J.; Golub, Y.; Kratz, O.; Moll, G.H. Stress system dysregulation in pediatric generalized anxiety disorder associated with comorbid depression. Stress Health 2017, 33, 518–529. [Google Scholar] [CrossRef] [PubMed]
- Salim, S. Oxidative stress and psychological disorders. Curr. Neuropharmacol. 2014, 12, 140–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Millart, H.; Durlach, V.; Durlach, J. Red blood cell magnesium concentrations: Analytical problems and significance. Magnes. Res. 1995, 8, 65–76. [Google Scholar]
- Boyle, N.B.; Lawton, C.; Dye, L. The Effects of Magnesium Supplementation on Subjective Anxiety and Stress-A Systematic Review. Nutrients 2017, 9, 429. [Google Scholar] [CrossRef] [Green Version]
- Cieslak, M.; Jedrzejewska, T.; Zgirski, A. Determinations of magnesium, iron and copper in the saliva of healthy subjects. Czas. Stomatol. 1990, 43, 202–206. [Google Scholar] [PubMed]
- Czegeny, Z.S.; Chicharro, J.L.; Fernandez, P.; Gutierrez, A.; Camara, C. Homogeneity and stability studies on sodium, calcium, magnesium, and manganese in human saliva. Biol. Trace Elem. Res. 2001, 79, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Machado, A.; Maneiras, R.; Bordalo, A.A.; Mesquita, R.B.R. Monitoring glucose, calcium, and magnesium levels in saliva as a non-invasive analysis by sequential injection multi-parametric determination. Talanta 2018, 186, 192–199. [Google Scholar] [CrossRef] [Green Version]
- Seo, J.W.; Park, T.J. Magnesium metabolism. Electrolytes Blood Press. 2008, 6, 86–95. [Google Scholar] [CrossRef] [Green Version]
- Gradinaru, I.; Ghiciuc, C.M.; Popescu, E.; Nechifor, C.; Mandreci, I.; Nechifor, M. Blood plasma and saliva levels of magnesium and other bivalent cations in patients with parotid gland tumors. Magnes. Res. 2007, 20, 254–258. [Google Scholar] [PubMed]
- Durlach, J.; Bac, P.; Bara, M.; Guiet-Bara, A. Physiopathology of symptomatic and latent forms of central nervous hyperexcitability due to magnesium deficiency: A current general scheme. Magnes. Res. 2000, 13, 293–302. [Google Scholar] [PubMed]
- Omiya, K.; Akashi, Y.J.; Yoneyama, K.; Osada, N.; Tanabe, K.; Miyake, F. Heart-Rate response to sympathetic nervous stimulation, exercise, and magnesium concentration in various sleep conditions. Int. J. Sport Nutr. Exerc. Metab. 2009, 19, 127–135. [Google Scholar] [CrossRef]
- Murck, H. Magnesium and affective disorders. Nutr. Neurosci. 2002, 5, 375–389. [Google Scholar] [CrossRef]
- Grases, G.; Perez-Castello, J.A.; Sanchis, P.; Casero, A.; Perello, J.; Isern, B.; Rigo, E.; Grases, F. Anxiety and stress among science students. Study of calcium and magnesium alterations. Magnes. Res. 2006, 19, 102–106. [Google Scholar]
- Sartori, S.B.; Whittle, N.; Hetzenauer, A.; Singewald, N. Magnesium deficiency induces anxiety and HPA axis dysregulation: Modulation by therapeutic drug treatment. Neuropharmacology 2012, 62, 304–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samejima, H.; Tanabe, K.; Suzuki, N.; Omiya, K.; Murayama, M. Magnesium dynamics and sympathetic nervous system activity in patients with chronic heart failure. Jpn. Circ. J. 1999, 63, 267–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Appenrodt, E.; Schnabel, R.; Schwarzberg, H. Vasopressin administration modulates anxiety-related behavior in rats. Physiol. Behav. 1998, 64, 543–547. [Google Scholar] [CrossRef] [PubMed]
- Bunck, M.; Czibere, L.; Horvath, C.; Graf, C.; Frank, E.; Kessler, M.S.; Murgatroyd, C.; Muller-Myhsok, B.; Gonik, M.; Weber, P.; et al. A hypomorphic vasopressin allele prevents anxiety-related behavior. PLoS ONE 2009, 4, e5129. [Google Scholar] [CrossRef] [Green Version]
- Fodor, A.; Kovacs, K.B.; Balazsfi, D.; Klausz, B.; Pinter, O.; Demeter, K.; Daviu, N.; Rabasa, C.; Rotllant, D.; Nadal, R.; et al. Depressive- and anxiety-like behaviors and stress-related neuronal activation in vasopressin-deficient female Brattleboro rats. Physiol. Behav. 2016, 158, 100–111. [Google Scholar] [CrossRef] [PubMed]
- Uzun, N.; Akca, O.F.; Kilinc, I.; Balci, T. Oxytocin and Vasopressin Levels and Related Factors in Adolescents with Social Phobia and Other Anxiety Disorders. Clin. Psychopharmacol. Neurosci. 2022, 20, 330–342. [Google Scholar] [CrossRef] [PubMed]
- Jeong, Y.K.; Oh, Y.I.; Song, K.H.; Seo, K.W. Evaluation of salivary vasopressin as an acute stress biomarker in healthy dogs with stress due to noise and environmental challenges. BMC Vet. Res. 2020, 16, 331. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, K.; Ohmomo, H.; Shutoh, F.; Nogami, H.; Hisano, S. Presentation of noise during acute restraint stress attenuates expression of immediate early genes and arginine vasopressin in the hypothalamic paraventricular nucleus but not corticosterone secretion in rats. Neurosci. Res. 2015, 96, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Bouby, N.; Trinh-Trang-Tan, M.M.; Bankir, L. Stimulation of tubular reabsorption of magnesium and calcium by antidiuretic hormone in conscious rats. Study in Brattleboro rats with hereditary hypothalamic diabetes insipidus. Pflügers Arch. 1984, 402, 458–464. [Google Scholar] [CrossRef]
- Opankovic, A.; Milovanovic, S.; Radosavljevic, B.; Cavic, M.; Besu Zizak, I.; Bukumiric, Z.; Latas, M.; Medic, B.; Vuckovic, S.; Srebro, D.; et al. Correlation of Ionized Magnesium with the Parameters of Oxidative Stress as Potential Biomarkers in Patients with Anxiety and Depression: A Pilot Study. Dose-Response 2022, 20, 15593258221116741. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Method | Salivary Mg, mg/L |
|---|---|---|
| [38] | Inductively coupled plasma mass spectrometry | 8.23 ± 3.78 |
| [39] | Inductively coupled plasma mass spectrometry | 6.31 ± 0.59 |
| [40] | Flame atomic absorption spectroscopy | 10.24 ± 3.49 |
| [41] | Atomic absorption spectroscopy | 0.81 ± 0.001 |
| [42] | Inductively coupled plasma mass spectrometry | 1.46 ± 0.83 |
| [43] | Flame atomic absorption spectroscopy | 7.3 ± 1.7 |
| [44] | Microwave plasma atomic emission spectroscopy | 7.6 ± 0.2 |
| This study | Electrothermal atomization atomic absorption spectroscopy | 7.6 ± 2.1 |
| Participants | Age | Gender | TMAS 1 | ESS 2 |
|---|---|---|---|---|
| Control group | 30.2 ± 10.1 | f = 10; m = 7 | 11.2 ± 5.8 | 8.7 ± 3.2 |
| Generalized anxiety disorder | 28.1 ± 9.3 p = 0.69 | f = 9; m = 6 | 33.7 ± 7.4 p < 0.0001 | 8.2 ± 4.2 p = 0.78 |
| Drying (°C)/(s) | Charring (°C)/(s) | Atomization (°C) | Cleaning (°C) |
|---|---|---|---|
| 95/40 | 900/8 | 2200 | 2200 |
| Experimental Set | Limit of Quantitation, µg/L | Linear Regression | R2 | Reproducibility, % | Recovery, % |
|---|---|---|---|---|---|
| Set #1 | 2.05 | y = 0.0049x + 0.0266 | 0.9971 | 5.0 | 103.16 |
| Set #2 | 2.05 | y = 0.0049x + 0.0275 | 0.9955 | 4.5 | 103.16 |
| Set #3 | 2.05 | y = 0.0049x + 0.0261 | 0.9975 | 4.9 | 103.16 |
| Set #4 | 2.34 | y = 0.0043x + 0.0212 | 0.9997 | 3.7 | 101.48 |
| Set #5 | 2.34 | y = 0.0043x + 0.0235 | 0.9971 | 4.2 | 101.48 |
| Method | One Independent Variable | Levels | Peculiarities of Samples | p-Value | Advantages | Disadvantages |
|---|---|---|---|---|---|---|
| One-way and repeated-measures ANOVA with Bonferroni test | Yes | Two levels and more | Independent | Yes | Results are free from errors of scaling and constant bias | Not applied for intercorrelations |
| Mann–Whitney U test | Yes | Two levels | Independent | Yes | A simple non-parametric test | Requires a number of critical samplings |
| Wilcoxon matched pair test | Yes | Two levels | Dependent | Yes | Applies to limited sample size, otherwise z-score can be used | No intrinsic clarity for the spread of shift values |
| The Spearman’s rank correlation test | Yes | Two levels | Dependent | Yes | The assumption of normal distribution is not required | Possibility of misinterpretation |
| Cohorts | Timing | Me(Q1; Q3), Min | p-Values for GAD vs. Control | p-Values for after vs. before |
|---|---|---|---|---|
| Control group | Before the experimental session | 44.3 (35.9; 47.0) | ||
| GAD patients | 37.6 (32.2; 38.2) | 0.38 | ||
| Control group | After the experimental session | 34.8 (33.1; 35.8) | 0.54 | |
| GAD patients | 37.6 (35.4; 38.6) | 0.75 | 0.86 |
| Cohorts | Timing | Me(Q1; Q3), mg/L | p-Values for GAD vs. Control | p-Values for after vs. before |
|---|---|---|---|---|
| Control group | Before the experimental session | 7.4 (5.3; 7.9) | ||
| GAD patients | 13.5 (11.2; 14.7) | 0.04 | ||
| Control group | After the experimental session | 7.4 (5.5; 9.4) | 0.88 | |
| GAD patients | 7.6 (7.4; 8.8) | 0.69 | 0.04 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Proskurnina, E.V.; Liaukovich, K.M.; Bychkovskaya, L.S.; Mikheev, I.V.; Alshanskaia, E.I.; Proskurnin, M.A.; Martynova, O.V.; Portnova, G.V. Salivary Antioxidant Capacity and Magnesium in Generalized Anxiety Disorder. Metabolites 2023, 13, 73. https://doi.org/10.3390/metabo13010073
Proskurnina EV, Liaukovich KM, Bychkovskaya LS, Mikheev IV, Alshanskaia EI, Proskurnin MA, Martynova OV, Portnova GV. Salivary Antioxidant Capacity and Magnesium in Generalized Anxiety Disorder. Metabolites. 2023; 13(1):73. https://doi.org/10.3390/metabo13010073
Chicago/Turabian StyleProskurnina, Elena V., Krystsina M. Liaukovich, Lyubov S. Bychkovskaya, Ivan V. Mikheev, Evgenia I. Alshanskaia, Mikhail A. Proskurnin, Olga V. Martynova, and Galina V. Portnova. 2023. "Salivary Antioxidant Capacity and Magnesium in Generalized Anxiety Disorder" Metabolites 13, no. 1: 73. https://doi.org/10.3390/metabo13010073
APA StyleProskurnina, E. V., Liaukovich, K. M., Bychkovskaya, L. S., Mikheev, I. V., Alshanskaia, E. I., Proskurnin, M. A., Martynova, O. V., & Portnova, G. V. (2023). Salivary Antioxidant Capacity and Magnesium in Generalized Anxiety Disorder. Metabolites, 13(1), 73. https://doi.org/10.3390/metabo13010073