
An Efficient DA-Net Architecture for Lung Nodule Segmentation



Abstract
:1. Introduction
2. Related Work
3. Materials and Methods
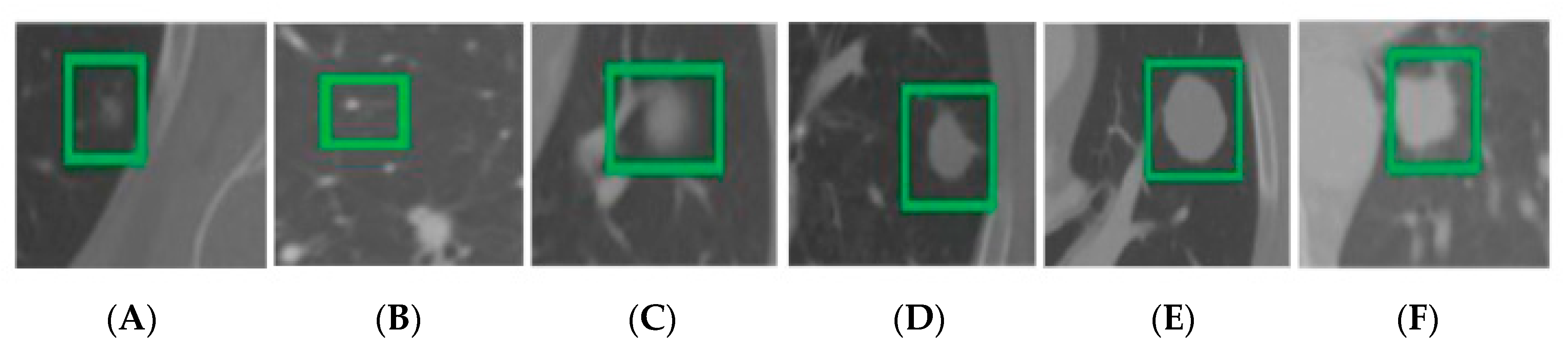
3.1. Dataset
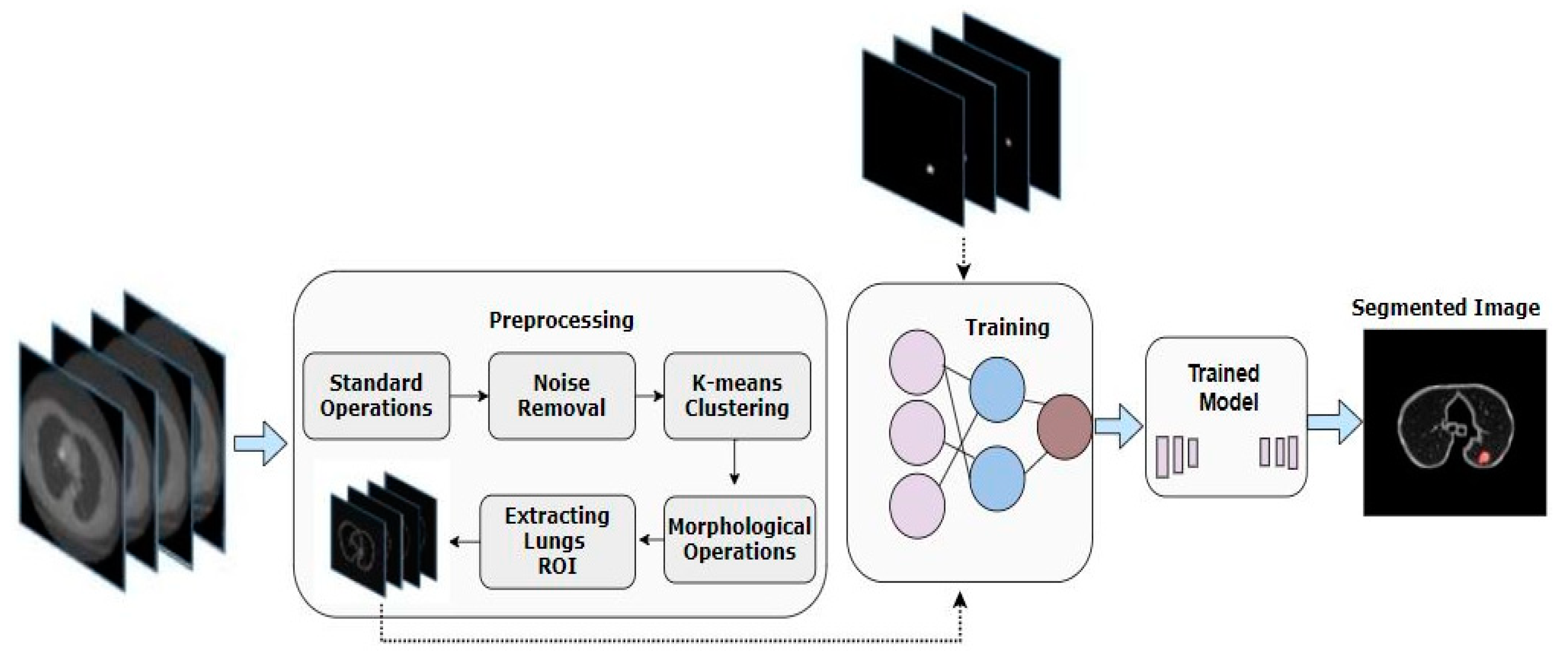
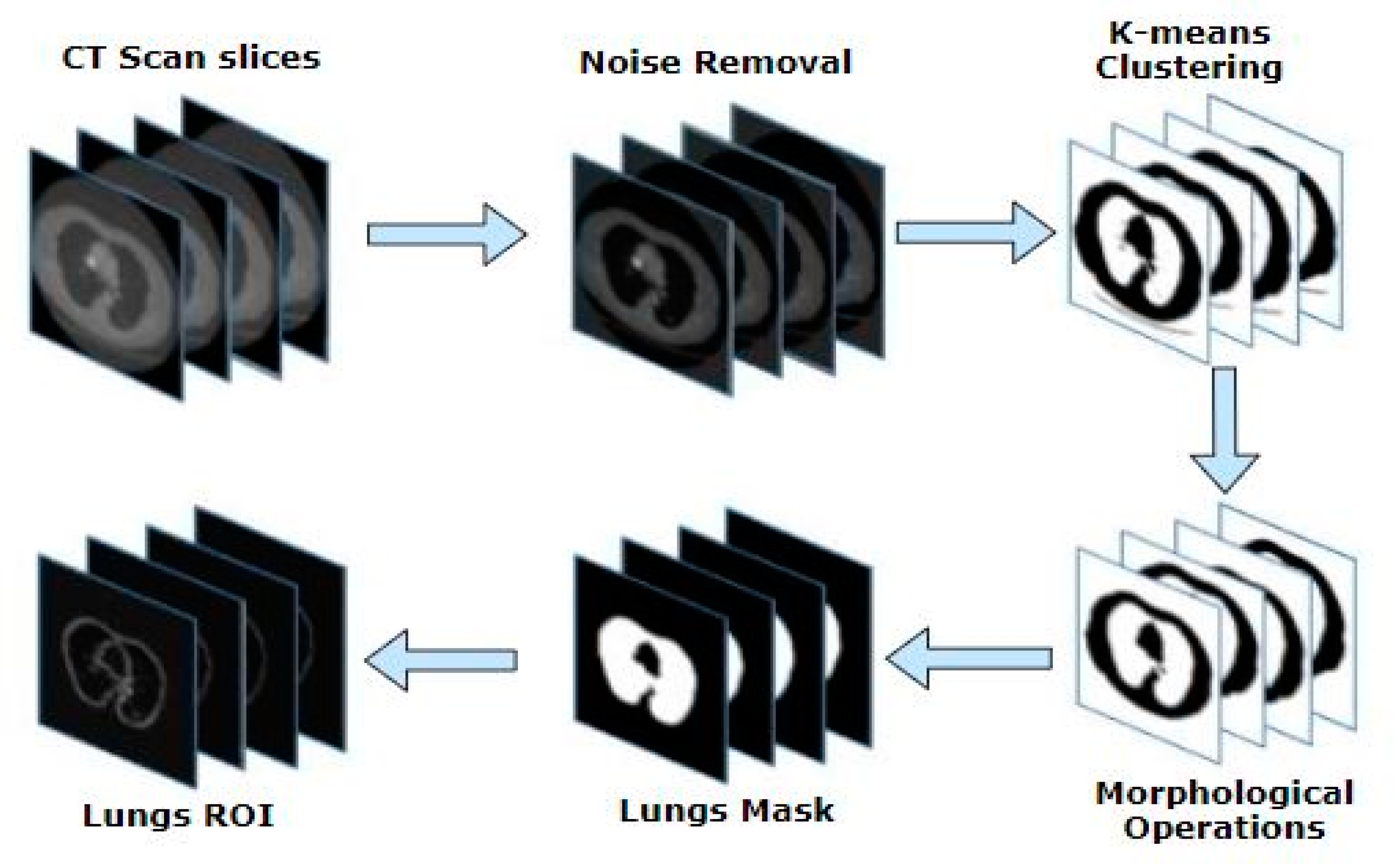
3.2. Pre-Processing
3.2.1. Standard Operations
3.2.2. Noise Removal Filters
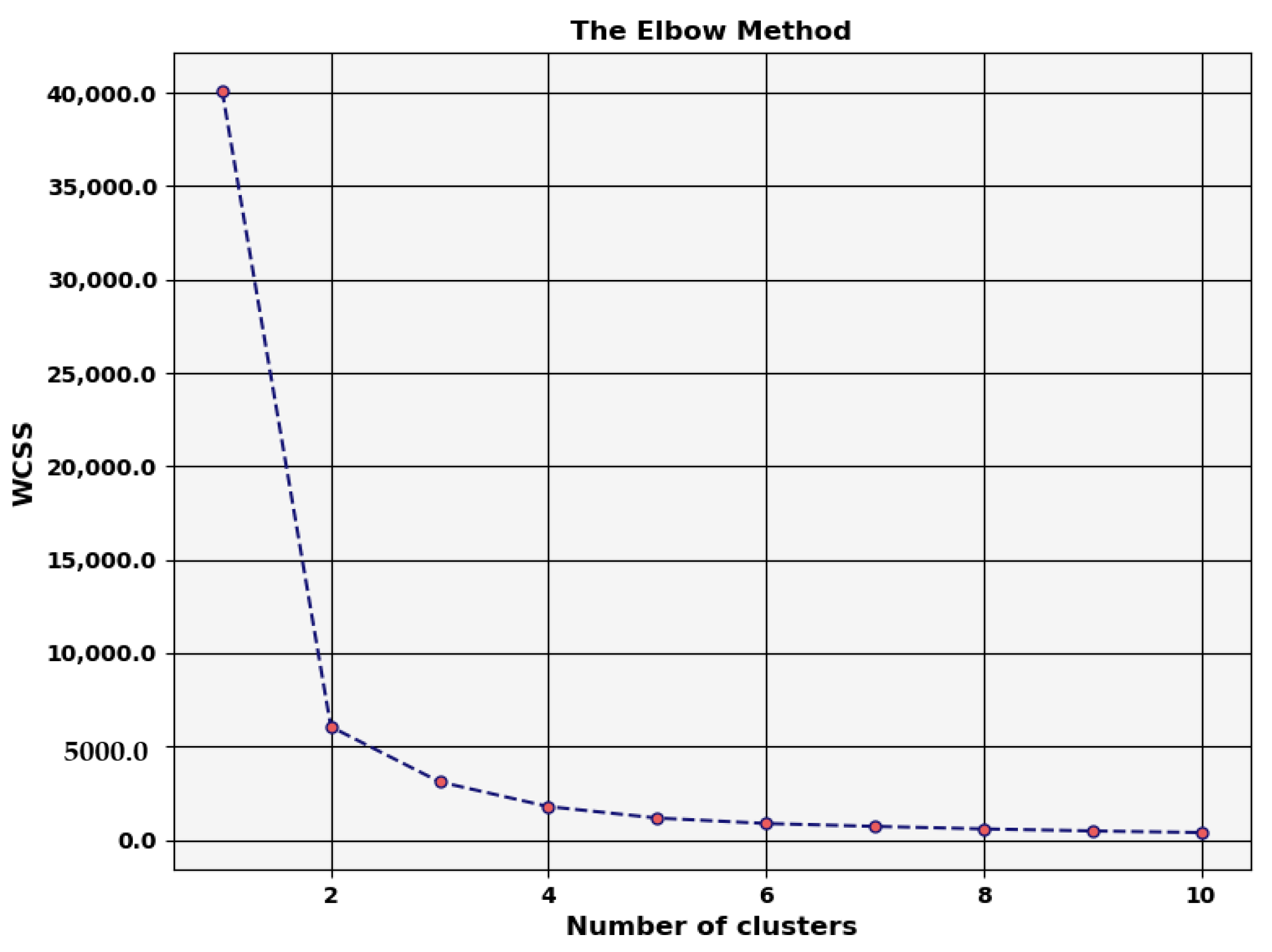
3.2.3. K-Means Clustering
3.2.4. Morphological Operations
3.2.5. Extracting Lung ROI
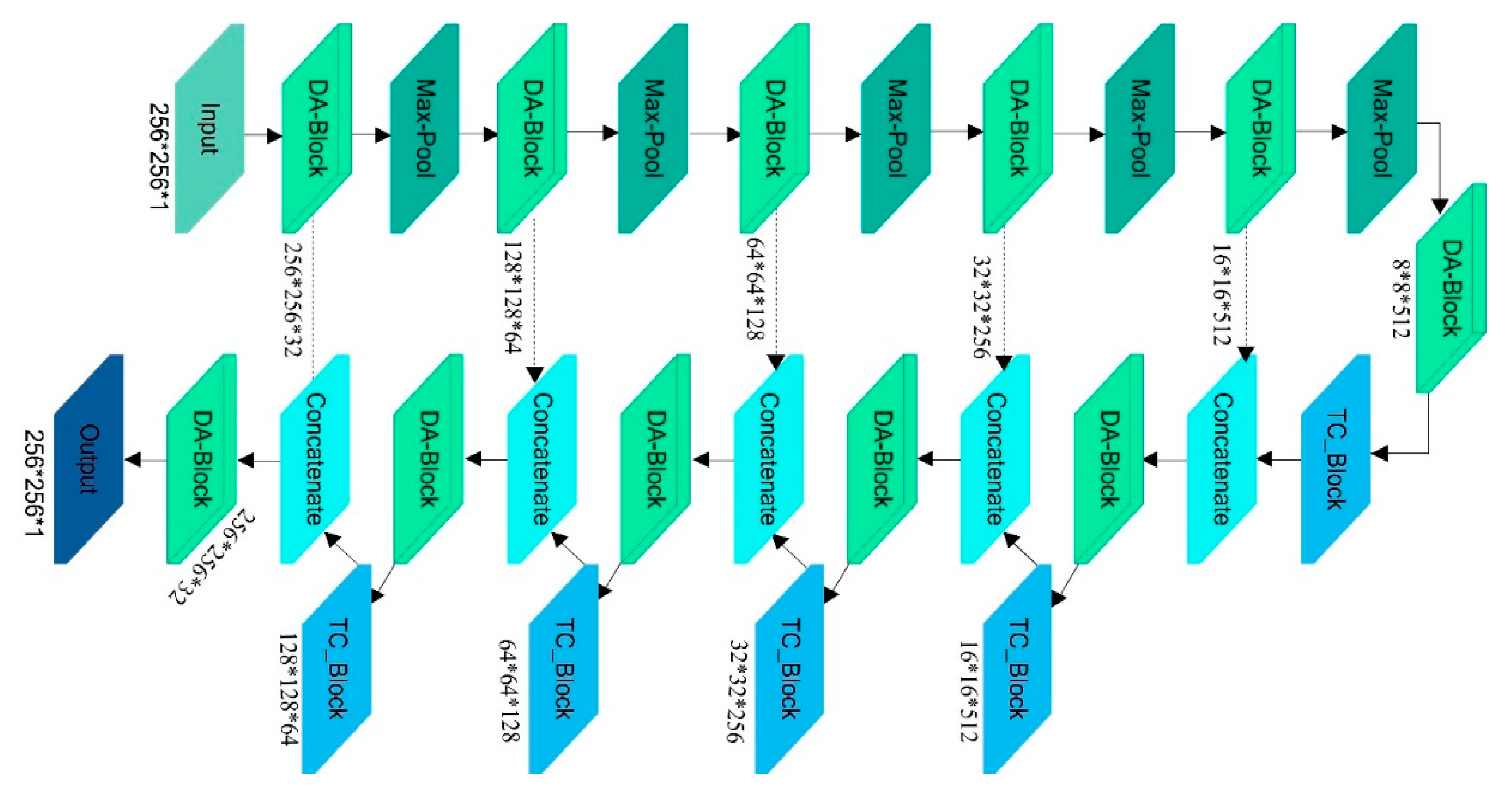
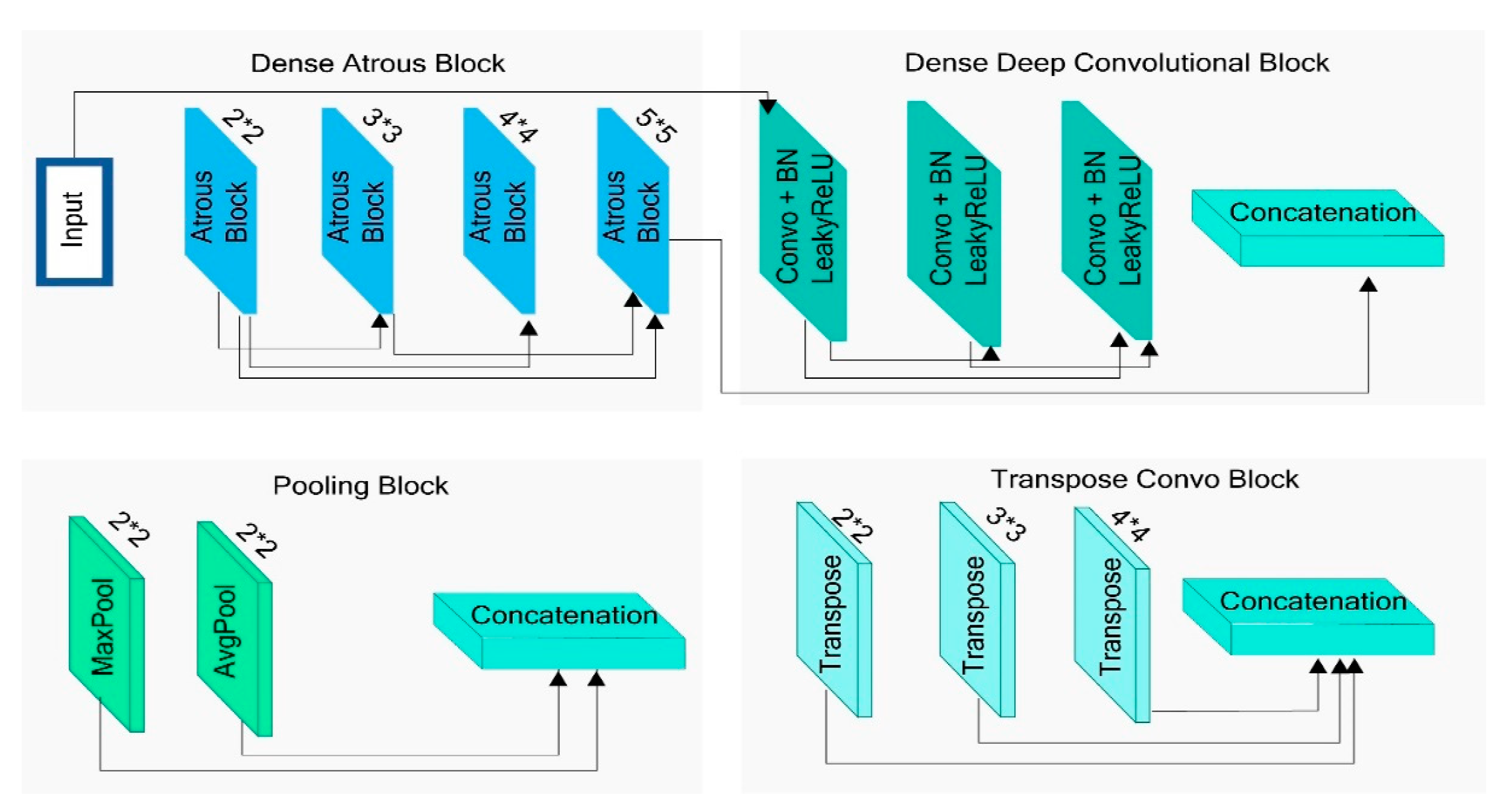
3.3. DA-Net Architecture
3.3.1. Encoder Path
3.3.2. Bottleneck Path
3.3.3. Decoder Path
3.4. Training Details and Hyper Parameters
4. Experiments and Results
4.1. Evaluation Criteria
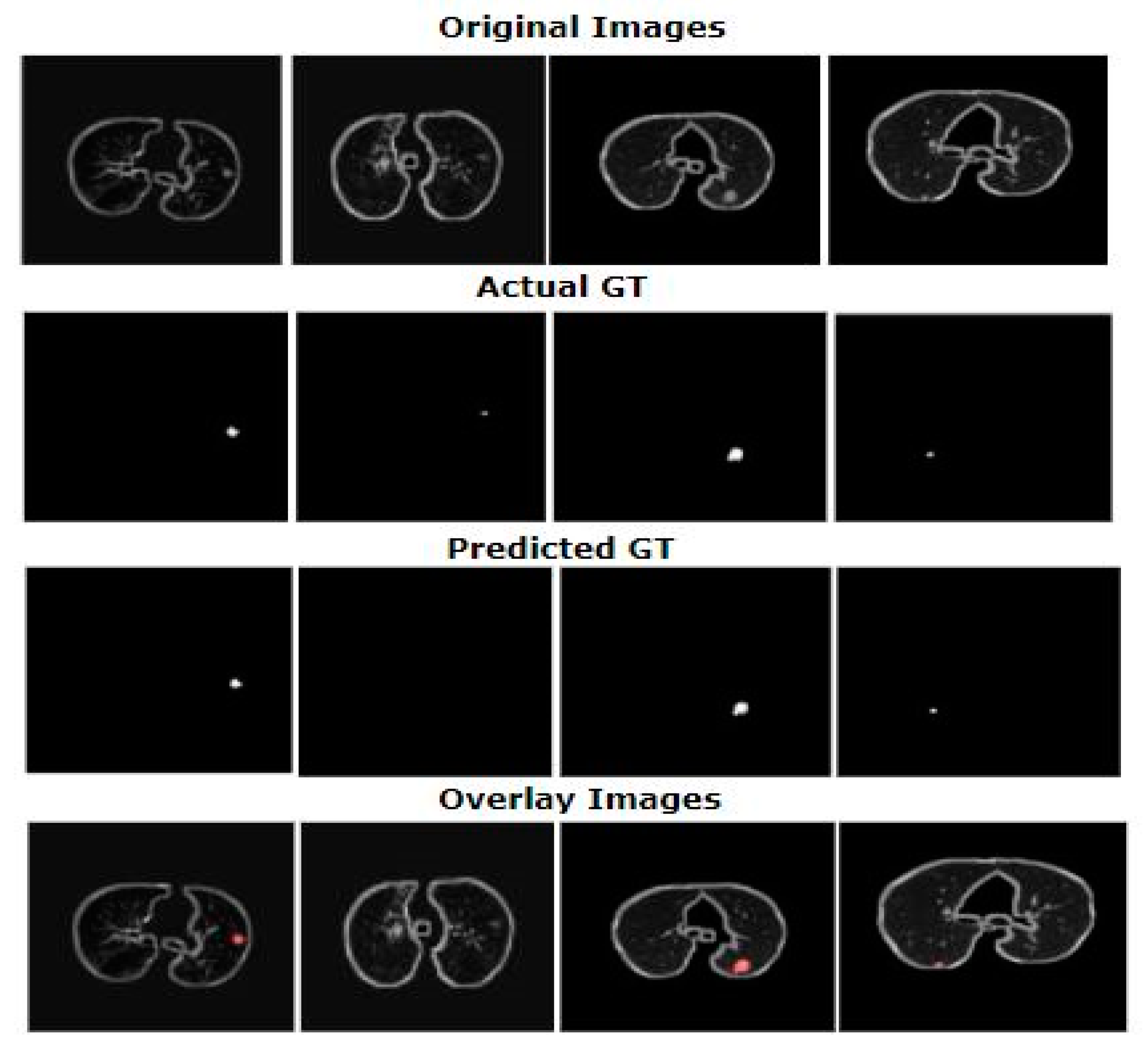
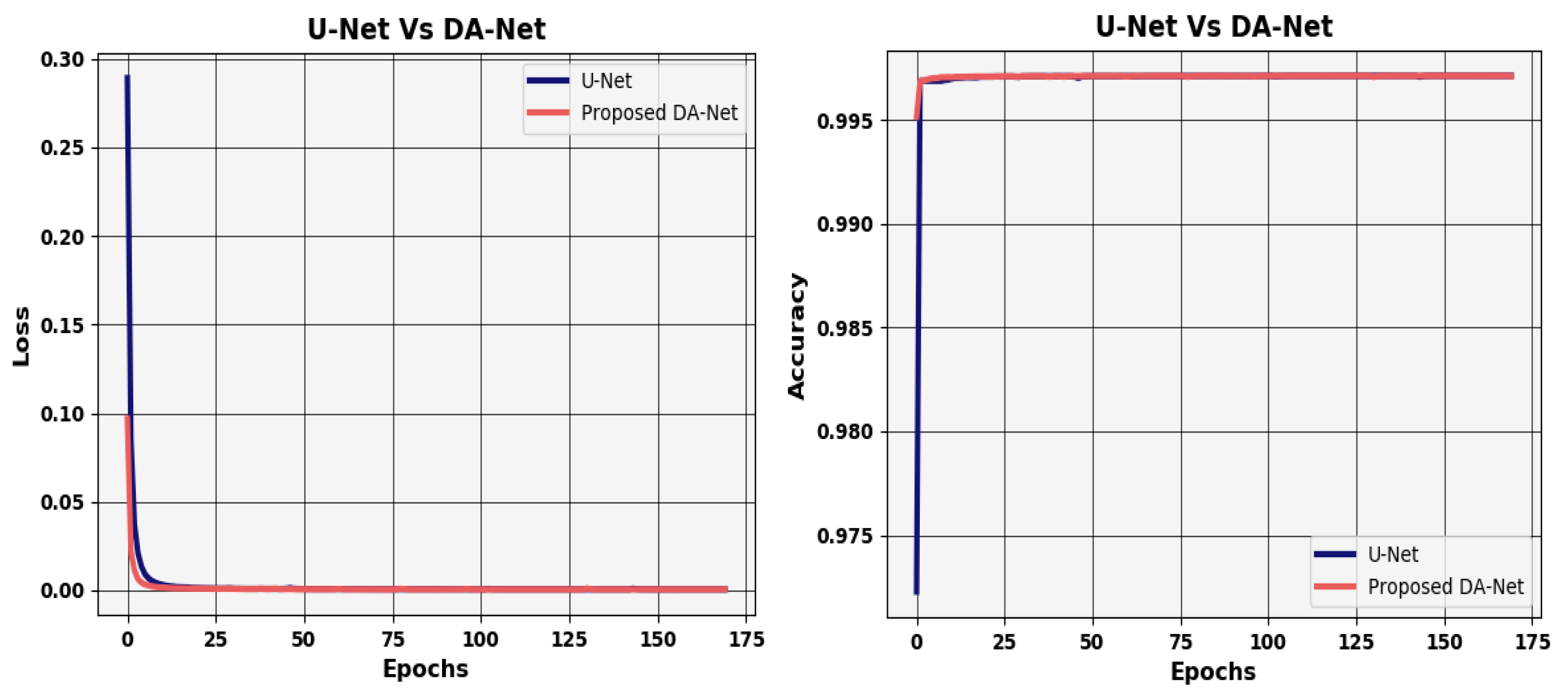
4.2. Results
4.3. Discussions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2016. CA Cancer J. Clin. 2016, 66, 7–30. [Google Scholar] [CrossRef] [Green Version]
- Firmino, M.; Morais, A.H.; Mendoça, R.M.; Dantas, M.R.; Hekis, H.R.; Valentim, R. Computer-Aided detection system for lung cancer in computed tomography scans: Review and future prospects. Biomed. Eng. Online 2014, 13, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Thomas, G.A.S.; Robinson, Y.H.; Julie, E.G.; Shanmuganathan, V.; Nam, Y.; Rho, S. Diabetic retinopathy diagnostics from retinal images based on deep convolutional networks. Preprints 2020. [Google Scholar] [CrossRef]
- Nawaz, H.; Maqsood, M.; Afzal, S.; Aadil, F.; Mehmood, I.; Rho, S. A deep feature-based real-time system for Alzheimer disease stage detection. Multimed. Tools Appl. 2020, 1–19. [Google Scholar] [CrossRef]
- Jung, S.; Moon, J.; Park, S.; Rho, S.; Baik, S.W.; Hwang, E. Bagging ensemble of multilayer perceptrons for missing electricity consumption data imputation. Sensors 2020, 20, 1772. [Google Scholar] [CrossRef] [Green Version]
- Aerts, H.J.; Velazquez, E.R.; Leijenaar, R.T.; Parmar, C.; Grossmann, P.; Carvalho, S.; Bussink, J.; Monshouwer, R.; Haibe-Kains, B.; Rietveld, D. Decoding tumour phenotype by noninvasive imaging using a quantitative radiomics approach. Nat. Commun. 2014, 5, 1–9. [Google Scholar] [CrossRef]
- Reeves, A.P.; Chan, A.B.; Yankelevitz, D.F.; Henschke, C.I.; Kressler, B.; Kostis, W.J. On measuring the change in size of pulmonary nodules. IEEE Trans. Med. Imaging 2006, 25, 435–450. [Google Scholar] [CrossRef] [PubMed]
- Lassen, B.; Jacobs, C.; Kuhnigk, J.; Van Ginneken, B.; Van Rikxoort, E. Robust semi-automatic segmentation of pulmonary subsolid nodules in chest computed tomography scans. Phys. Med. Biol. 2015, 60, 1307. [Google Scholar] [CrossRef]
- Farag, A.A.; Abd El Munim, H.E.; Graham, J.H.; Farag, A.A. A novel approach for lung nodules segmentation in chest CT using level sets. IEEE Trans. Image Process. 2013, 22, 5202–5213. [Google Scholar] [CrossRef]
- Kubota, T.; Jerebko, A.K.; Dewan, M.; Salganicoff, M.; Krishnan, A. Segmentation of pulmonary nodules of various densities with morphological approaches and convexity models. Med. Image Anal. 2011, 15, 133–154. [Google Scholar] [CrossRef]
- Zhang, G.; Jiang, S.; Yang, Z.; Gong, L.; Ma, X.; Zhou, Z.; Bao, C.; Liu, Q. Automatic nodule detection for lung cancer in CT images: A review. Comput. Biol. Med. 2018, 103, 287–300. [Google Scholar] [CrossRef]
- Paing, M.P.; Choomchuay, S. Ground glass opacity (GGO) nodules detection from lung CT scans. In Proceedings of the 2017 International Symposium on Electronics and Smart Devices (ISESD), Yogyakarta, Indonesia, 17–19 October 2017; pp. 230–235. [Google Scholar]
- Zhao, J.j.; Ji, G.H.; Xia, Y.; Zhang, X.L. Cavitary nodule segmentation in computed tomography images based on self-generating neural networks and particle swarm optimisation. Int. J. Bio-Inspired Comput. 2015, 7, 62–67. [Google Scholar] [CrossRef]
- Diciotti, S.; Lombardo, S.; Falchini, M.; Picozzi, G.; Mascalchi, M. Automated segmentation refinement of small lung nodules in CT scans by local shape analysis. IEEE Trans. Biomed. Eng. 2011, 58, 3418–3428. [Google Scholar] [CrossRef]
- Messay, T.; Hardie, R.C.; Rogers, S.K. A new computationally efficient CAD system for pulmonary nodule detection in CT imagery. Med. Image Anal. 2010, 14, 390–406. [Google Scholar] [CrossRef]
- Dehmeshki, J.; Amin, H.; Valdivieso, M.; Ye, X. Segmentation of pulmonary nodules in thoracic CT scans: A region growing approach. IEEE Trans. Med Imaging 2008, 27, 467–480. [Google Scholar] [CrossRef] [Green Version]
- Ye, X.; Beddoe, G.; Slabaugh, G. Automatic graph cut segmentation of lesions in CT using mean shift superpixels. Int. J. Biomed. Imaging 2010, 2010. [Google Scholar] [CrossRef]
- Messay, T.; Hardie, R.C.; Tuinstra, T.R. Segmentation of pulmonary nodules in computed tomography using a regression neural network approach and its application to the lung image database consortium and image database resource initiative dataset. Med. Image Anal. 2015, 22, 48–62. [Google Scholar] [CrossRef]
- Keshani, M.; Azimifar, Z.; Tajeripour, F.; Boostani, R. Lung nodule segmentation and recognition using SVM classifier and active contour modeling: A complete intelligent system. Comput. Biol. Med. 2013, 43, 287–300. [Google Scholar] [CrossRef]
- Ding, J.; Li, A.; Hu, Z.; Wang, L. Accurate pulmonary nodule detection in computed tomography images using deep convolutional neural networks. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Quebec City, QC, Canada, 10–14 September 2017; pp. 559–567. [Google Scholar]
- Pereira, S.; Pinto, A.; Alves, V.; Silva, C.A. Brain tumor segmentation using convolutional neural networks in MRI images. IEEE Trans. Med. Imaging 2016, 35, 1240–1251. [Google Scholar] [CrossRef] [PubMed]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]
- Lu, L.; Barbu, A.; Wolf, M.; Liang, J.; Salganicoff, M.; Comaniciu, D. Accurate polyp segmentation for 3D CT colongraphy using multi-staged probabilistic binary learning and compositional model. In Proceedings of the 2008 IEEE Conference on Computer Vision and Pattern Recognition, Anchorage, AK, USA, 23–28 June 2008; pp. 1–8. [Google Scholar]
- Kostis, W.J.; Reeves, A.P.; Yankelevitz, D.F.; Henschke, C.I. Three-Dimensional segmentation and growth-rate estimation of small pulmonary nodules in helical CT images. IEEE Trans. Med. Imaging 2003, 22, 1259–1274. [Google Scholar] [CrossRef]
- Shang, Y. Percolation on random networks with proliferation. Int. J. Mod. Phys. B 2018, 32, 1850359. [Google Scholar] [CrossRef]
- Sargent, D.; Park, S.Y. Semi-Automatic 3D lung nodule segmentation in CT using dynamic programming. In Image Processing, Proceedings of the Medical Imaging 2017, Orlando, Florida, USA, 11–16 February 2017; SPIE—International Society for Optics and Photonics: Bellingham, WA, USA, 2017; p. 101332R. [Google Scholar]
- Kuhnigk, J.-M.; Dicken, V.; Bornemann, L.; Bakai, A.; Wormanns, D.; Krass, S.; Peitgen, H.-O. Morphological segmentation and partial volume analysis for volumetry of solid pulmonary lesions in thoracic CT scans. IEEE Trans. Med. Imaging 2006, 25, 417–434. [Google Scholar] [CrossRef]
- Rebouças Filho, P.P.; da Silva Barros, A.C.; Almeida, J.S.; Rodrigues, J.; de Albuquerque, V.H.C. A new effective and powerful medical image segmentation algorithm based on optimum path snakes. Appl. Soft Comput. 2019, 76, 649–670. [Google Scholar] [CrossRef]
- Wang, J.; Guo, H. Automatic approach for lung segmentation with juxta-pleural nodules from thoracic CT based on contour tracing and correction. Comput. Math. Methods Med. 2016, 2016, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Nithila, E.E.; Kumar, S. Segmentation of lung nodule in CT data using active contour model and fuzzy C-mean clustering. Alex. Eng. J. 2016, 55, 2583–2588. [Google Scholar] [CrossRef] [Green Version]
- Chan, T.F.; Vese, L.A. Active contours without edges. IEEE Trans. Image Process. 2001, 10, 266–277. [Google Scholar] [CrossRef] [Green Version]
- Peng, J.; Heisterkamp, D.R.; Dai, H.K. Adaptive quasiconformal kernel nearest neighbor classification. IEEE Trans. Pattern Anal. Mach. Intell. 2004, 26, 656–661. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.; Gould, S.; Salzmann, M. Segmentation of developing human embryo in time-lapse microscopy. In Proceedings of the 2016 IEEE 13th International Symposium on Biomedical Imaging (ISBI), Prague, Czech Republic, 13–16 April 2016; pp. 930–934. [Google Scholar]
- Lu, L.; Bi, J.; Wolf, M.; Salganicoff, M. Effective 3D object detection and regression using probabilistic segmentation features in CT images. In Proceedings of the 2011 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Colorado Springs, CO, USA, 20–25 June 2011; pp. 1049–1056. [Google Scholar]
- Mukhopadhyay, S. A segmentation framework of pulmonary nodules in lung CT images. J. Digit. Imaging 2016, 29, 86–103. [Google Scholar] [CrossRef] [Green Version]
- Shen, S.; Bui, A.A.; Cong, J.; Hsu, W. An automated lung segmentation approach using bidirectional chain codes to improve nodule detection accuracy. Comput. Biol. Med. 2015, 57, 139–149. [Google Scholar] [CrossRef]
- Lu, L.; Devarakota, P.; Vikal, S.; Wu, D.; Zheng, Y.; Wolf, M. Computer aided diagnosis using multilevel image features on large-scale evaluation. In Proceedings of the International MICCAI Workshop on Medical Computer Vision, Nagoya, Japan, 26 September 2013; pp. 161–174. [Google Scholar]
- Wu, D.; Lu, L.; Bi, J.; Shinagawa, Y.; Boyer, K.; Krishnan, A.; Salganicoff, M. Stratified learning of local anatomical context for lung nodules in CT images. In Proceedings of the 2010 IEEE Computer Society Conference on Computer Vision and Pattern Recognition, San Francisco, CA, USA, 13–18 June 2010; pp. 2791–2798. [Google Scholar]
- Hu, Y.; Menon, P.G. A neural network approach to lung nodule segmentation. In Image Processing, Proceedings of the Medical Imaging 2016, San Diego, CA, USA, 27 February 2016; SPIE—International Society for Optics and Photonics: Piscataway, NJ, USA, 2017; p. 978420. [Google Scholar]
- Jung, J.; Hong, H.; Goo, J.M. Ground-Glass nodule segmentation in chest CT images using asymmetric multi-phase deformable model and pulmonary vessel removal. Comput. Biol. Med. 2018, 92, 128–138. [Google Scholar] [CrossRef]
- Gonçalves, L.; Novo, J.; Campilho, A. Hessian based approaches for 3D lung nodule segmentation. Expert Syst. Appl. 2016, 61, 1–15. [Google Scholar] [CrossRef]
- Shen, W.; Zhou, M.; Yang, F.; Yu, D.; Dong, D.; Yang, C.; Zang, Y.; Tian, J. Multi-Crop convolutional neural networks for lung nodule malignancy suspiciousness classification. Pattern Recognit. 2017, 61, 663–673. [Google Scholar] [CrossRef]
- Gao, W.; Zhou, Z.-H. Dropout rademacher complexity of deep neural networks. Sci. China Inf. Sci. 2016, 59, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Zhou, M.; Liu, Z.; Liu, Z.; Gu, D.; Zang, Y.; Dong, D.; Gevaert, O.; Tian, J. Central focused convolutional neural networks: Developing a data-driven model for lung nodule segmentation. Med. Image Anal. 2017, 40, 172–183. [Google Scholar] [CrossRef]
- Wang, S.; Zhou, M.; Gevaert, O.; Tang, Z.; Dong, D.; Liu, Z.; Jie, T. A multi-view deep convolutional neural networks for lung nodule segmentation. In Proceedings of the 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju Island, Korea, 11–15 July 2017; pp. 1752–1755. [Google Scholar]
- Zhao, X.; Sun, W.; Qian, W.; Qi, S.; Sun, J.; Zhang, B.; Yang, Z. Fine-Grained lung nodule segmentation with pyramid deconvolutional neural network. In Computer-Aided Diagnosis, Proceedings of the Medical Imaging 2019, San Diego, CA, USA, 17–20 February 2019; SPIE—International Society for Optics and Photonics: Bellingham, WA, USA, 2019; p. 109503S. [Google Scholar]
- Huang, X.; Sun, W.; Tseng, T.-L.B.; Li, C.; Qian, W. Fast and fully-automated detection and segmentation of pulmonary nodules in thoracic CT scans using deep convolutional neural networks. Comput. Med. Imaging Graph. 2019, 74, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Long, J.; Shelhamer, E.; Darrell, T. Fully convolutional models for semantic segmentation. In Proceedings of the 2015 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Boston, MA, USA, 7–12 June 2015; p. 4. [Google Scholar]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional networks for biomedical image segmentation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Munich, Germany, 5–9 October 2015; pp. 234–241. [Google Scholar]
- Çiçek, Ö.; Abdulkadir, A.; Lienkamp, S.S.; Brox, T.; Ronneberger, O. 3D U-Net: Learning dense volumetric segmentation from sparse annotation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Athens, Greece, 17–21 October 2016; pp. 424–432. [Google Scholar]
- Armato, S.G., III; McLennan, G.; Bidaut, L.; McNitt-Gray, M.F.; Meyer, C.R.; Reeves, A.P.; Zhao, B.; Aberle, D.R.; Henschke, C.I.; Hoffman, E.A. The lung image database consortium (LIDC) and image database resource initiative (IDRI): A completed reference database of lung nodules on CT scans. Med. Phys. 2011, 38, 915–931. [Google Scholar] [CrossRef] [PubMed]
- Ning, C.-Y.; Liu, S.-F.; Qu, M. Research on removing noise in medical image based on median filter method. In Proceedings of the 2009 IEEE International Symposium on IT in Medicine & Education, Jinan, China, 14–16 August 2009; pp. 384–388. [Google Scholar]
- Jagatheeswari, P.; Suresh Kumar, S.; Rajaram, M. Contrast enhancement for medical images based on histogram equalization followed by median filter. In Proceedings of the International Conference on Man-Machine Systems (ICoMMS), Batu Ferringhi, Malaysia, 11–13 October 2009. [Google Scholar]
- Krissian, K.; Aja-Fernández, S. Noise-Driven anisotropic diffusion filtering of MRI. IEEE Trans. Image Process. 2009, 18, 2265–2274. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.; Nachamai, M. Noise removal and filtering techniques used in medical images. Orient. J. Comp. Sci. Technol. 2017, 10. [Google Scholar] [CrossRef] [Green Version]
- Bhonsle, D.; Chandra, V.; Sinha, G. Medical image denoising using bilateral filter. Int. J. Image Graph. Signal Process. 2012, 4. [Google Scholar] [CrossRef] [Green Version]
- Ali, H.M. MRI medical image denoising by fundamental filters. In High-Resolution Neuroimaging-Basic Physical Principles and Clinical Applications; InTech: London, UK, 2018; pp. 111–124. [Google Scholar]
- Pohle, R.; Toennies, K.D. Segmentation of medical images using adaptive region growing. In Image Processing, Proceedings of the Medical Imaging 2001, San Diego, CA, USA, 17–22 February 2001; SPIE—International Society for Optics and Photonics: Bellingham, WA, USA, 2001; pp. 1337–1346. [Google Scholar]
- Senthilkumaran, N.; Vaithegi, S. Image segmentation by using thresholding techniques for medical images. Comput. Sci. Eng. Int. J. 2016, 6, 1–13. [Google Scholar]
- Ng, H.; Ong, S.; Foong, K.; Goh, P.-S.; Nowinski, W. Medical image segmentation using K-means clustering and improved watershed algorithm. In Proceedings of the 2006 IEEE Southwest Symposium on Image Analysis and Interpretation, Denver, CO, USA, 26–28 March 2006; pp. 61–65. [Google Scholar]
- Vijay, J.; Subhashini, J. An efficient brain tumor detection methodology using K-means clustering algoriftnn. In Proceedings of the 2013 International Conference on Communication and Signal Processing, Melmaruvathur, India, 3–5 April 2013; pp. 653–657. [Google Scholar]
- Firoz, R.; Ali, M.S.; Khan, M.N.U.; Hossain, M.K.; Islam, M.K.; Shahinuzzaman, M. Medical image enhancement using morphological transformation. J. Data Anal. Inf. Process. 2016, 4, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Ioffe, S.; Szegedy, C. Batch normalization: Accelerating deep network training by reducing internal covariate shift. In Proceedings of the International Conference on Machine Learning, Lille, France, 6–11 July 2015; pp. 448–456. [Google Scholar]
- Liew, S.S.; Khalil-Hani, M.; Bakhteri, R. Bounded activation functions for enhanced training stability of deep neural networks on visual pattern recognition problems. Neurocomputing 2016, 216, 718–734. [Google Scholar] [CrossRef]
- Nair, V.; Hinton, G.E. Rectified linear units improve restricted boltzmann machines. In Proceedings of the International Conference on Machine Learning (ICML), Haifa, Israel, 21–24 June 2010. [Google Scholar]
- Shang, Y. Consensus formation of two-level opinion dynamics. Acta Math. Sci. 2014, 34, 1029–1040. [Google Scholar] [CrossRef]
- Bukhari, M.; Bajwa, K.B.; Gillani, S.; Maqsood, M.; Durrani, M.Y.; Mehmood, I.; Ugail, H.; Rho, S. An efficient gait recognition method for known and unknown covariate conditions. IEEE Access 2020, 9, 6465–6477. [Google Scholar] [CrossRef]
- Jifara, W.; Jiang, F.; Rho, S.; Cheng, M.; Liu, S. Medical image denoising using convolutional neural network: A residual learning approach. J. Supercomput. 2019, 75, 704–718. [Google Scholar] [CrossRef]
- Muhammad, K.; Ahmad, J.; Mehmood, I.; Rho, S.; Baik, S.W. Convolutional neural networks based fire detection in surveillance videos. IEEE Access 2018, 6, 18174–18183. [Google Scholar] [CrossRef]
- Kalsoom, A.; Maqsood, M.; Ghazanfar, M.A.; Aadil, F.; Rho, S. A dimensionality reduction-based efficient software fault prediction using Fisher linear discriminant analysis (FLDA). J. Supercomput. 2018, 74, 4568–4602. [Google Scholar] [CrossRef]
- Jiang, F.; Grigorev, A.; Rho, S.; Tian, Z.; Fu, Y.; Jifara, W.; Adil, K.; Liu, S. Medical image semantic segmentation based on deep learning. Neural Comput. Appl. 2018, 29, 1257–1265. [Google Scholar] [CrossRef]
- Jiang, J.; Hu, Y.C.; Liu, C.J.; Halpenny, D.; Hellmann, M.D.; Deasy, J.O.; Mageras, G.; Veeraraghavan, H. Multiple resolution residually connected feature streams for automatic lung tumor segmentation from CT images. IEEE Trans. Med. Imaging 2019, 38, 134–144. [Google Scholar] [CrossRef]
- Huang, X.; Shan, J.; Vaidya, V. Lung nodule detection in CT using 3D convolutional neural networks. In Proceedings of the 2017 IEEE 14th International Symposium on Biomedical Imaging (ISBI 2017), Melbourne, Australia, 18–21 April 2017; pp. 379–383. [Google Scholar]
- Wu, B.; Zhou, Z.; Wang, J.; Wang, Y. Joint learning for pulmonary nodule segmentation, attributes and malignancy prediction. In Proceedings of the 2018 IEEE 15th International Symposium on Biomedical Imaging (ISBI 2018), Washington, DC, USA, 4–7 April 2018; pp. 1109–1113. [Google Scholar]
- Hancock, M.C.; Magnan, J.F. Lung nodule segmentation via level set machine learning. arXiv 2019, arXiv:1910.03191. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sr. No. | Models | Dice Score | IOU Score | SVD | Sensitivity |
|---|---|---|---|---|---|
| 1 | U-Net [49] | 71.0 | 62.8 | 0.29 | 70.2 |
| 2 | DA-Net | 81 | 71.6 | 0.19 | 87.2 |
| Sr. No. | Method | Dice Score | IOU Score | Year |
|---|---|---|---|---|
| 1 | Wang et al. [44] | 77.67% | - | 2017 |
| 2 | Jiang et al. [72] | 68% | - | 2019 |
| 3 | Huang et al. [73] | 80.52 | - | 2017 |
| 4 | Qian et al. [46] | 62.8 | 71.93 | 2019 |
| 5 | Hancock et al. [75] | - | 71.85 | 2019 |
| 6 | Huang et al. [47] | - | 70.24 | 2019 |
| 7 | Wu et al. [74] | 74.05 | 58 | 2018 |
| 8 | Shen et al. [42] | 78.55 | - | 2016 |
| 9 | U-Net [49] | 71.0 | 62.8 | 2015 |
| 10 | Proposed DA-Net | 81 | 71.6 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maqsood, M.; Yasmin, S.; Mehmood, I.; Bukhari, M.; Kim, M. An Efficient DA-Net Architecture for Lung Nodule Segmentation. Mathematics 2021, 9, 1457. https://doi.org/10.3390/math9131457
Maqsood M, Yasmin S, Mehmood I, Bukhari M, Kim M. An Efficient DA-Net Architecture for Lung Nodule Segmentation. Mathematics. 2021; 9(13):1457. https://doi.org/10.3390/math9131457
Chicago/Turabian StyleMaqsood, Muazzam, Sadaf Yasmin, Irfan Mehmood, Maryam Bukhari, and Mucheol Kim. 2021. "An Efficient DA-Net Architecture for Lung Nodule Segmentation" Mathematics 9, no. 13: 1457. https://doi.org/10.3390/math9131457
APA StyleMaqsood, M., Yasmin, S., Mehmood, I., Bukhari, M., & Kim, M. (2021). An Efficient DA-Net Architecture for Lung Nodule Segmentation. Mathematics, 9(13), 1457. https://doi.org/10.3390/math9131457