

Effects of 24 Weeks of a Supervised Walk Training on Knee Muscle Strength and Quality of Life in Older Female Total Knee Arthroplasty: A Retrospective Cohort Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
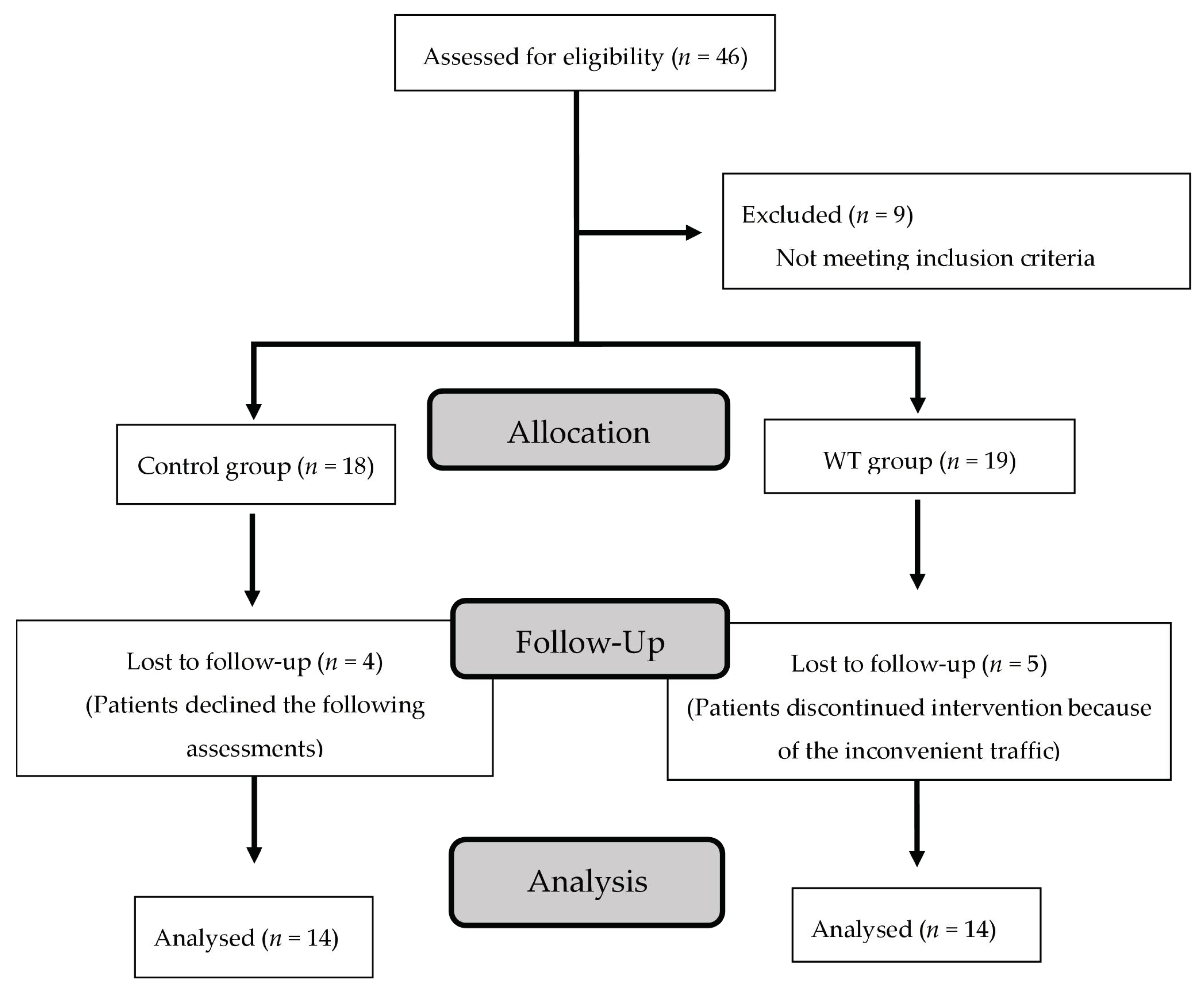
2.1. Participants
2.2. Sample Size
2.3. WT Course
2.4. Muscle strength
2.5. Functional Fitness Test
2.6. Knee Injury and Osteoarthritis Outcome Score (KOOS) Questionnaire
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hussain, S.M.; Neilly, D.W.; Baliga, S.; Patil, S.; Meek, R. Knee osteoarthritis: A review of management options. Scott. Med. J. 2016, 61, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Schiavone Panni, A.; Falez, F.; D’Apolito, R.; Corona, K.; Perisano, C.; Vasso, M. Long-term follow-up of a non-randomised prospective cohort of one hundred and ninety two total knee arthroplasties using the NexGen implant. Int. Orthop. 2017, 41, 1155–1162. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.A.; Yu, S.; Chen, L.; Cleveland, J.D. Rates of Total Joint Replacement in the United States: Future Projections to 2020–2040 Using the National Inpatient Sample. J. Rheumatol. 2019, 46, 1134–1140. [Google Scholar] [CrossRef] [PubMed]
- Paravlic, A.H.; Kovac, S.; Pisot, R.; Marusic, U. Neurostructural correlates of strength decrease following total knee arthroplasty: A systematic review of the literature with meta-analysis. Bosn. J. Basic Med. Sci. 2020, 20, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Paravlic, A.H.; Meulenberg, C.J.; Drole, K. The Time Course of Quadriceps Strength Recovery After Total Knee Arthroplasty Is Influenced by Body Mass Index, Sex, and Age of Patients: Systematic Review and Meta-Analysis. Front. Med. 2022, 9, 865412. [Google Scholar] [CrossRef]
- Pozzi, F.; Snyder-Mackler, L.; Zeni, J. Physical exercise after knee arthroplasty: A systematic review of controlled trials. Eur. J. Phys. Rehabil. Med. 2013, 49, 877–892. [Google Scholar]
- Hsu, W.H.; Hsu, W.B.; Shen, W.J.; Lin, Z.R.; Chang, S.H.; Hsu, R.W. Circuit training enhances function in patients undergoing total knee arthroplasty: A retrospective cohort study. J. Orthop. Surg. Res. 2017, 12, 156. [Google Scholar] [CrossRef] [Green Version]
- Hsu, W.H.; Hsu, W.B.; Shen, W.J.; Lin, Z.R.; Chang, S.H.; Hsu, R.W. Twenty-four-week hospital-based progressive resistance training on functional recovery in female patients post total knee arthroplasty. Knee 2019, 26, 729–736. [Google Scholar] [CrossRef]
- Henderson, K.G.; Wallis, J.A.; Snowdon, D.A. Active physiotherapy interventions following total knee arthroplasty in the hospital and inpatient rehabilitation settings: A systematic review and meta-analysis. Physiotherapy 2018, 104, 25–35. [Google Scholar] [CrossRef]
- Hiyama, Y.; Kamitani, T.; Wada, O.; Mizuno, K.; Yamada, M. Effects of Group-Based Exercise on Range of Motion, Muscle Strength, Functional Ability, and Pain During the Acute Phase After Total Knee Arthroplasty: A Controlled Clinical Trial. J. Orthop. Sports Phys. Ther. 2016, 46, 742–748. [Google Scholar] [CrossRef] [Green Version]
- Han, A.S.; Nairn, L.; Harmer, A.R.; Crosbie, J.; March, L.; Parker, D.; Crawford, R.; Fransen, M. Early rehabilitation after total knee replacement surgery: A multicenter, noninferiority, randomized clinical trial comparing a home exercise program with usual outpatient care. Arthritis Care Res. 2015, 67, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Li, P.; Lin, F. Influence of structured telephone follow-up on patient compliance with rehabilitation after total knee arthroplasty. Patient Prefer. Adherence 2016, 10, 257–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sipila, S.; Tirkkonen, A.; Hanninen, T.; Laukkanen, P.; Alen, M.; Fielding, R.A.; Kivipelto, M.; Kokko, K.; Kulmala, J.; Rantanen, T.; et al. Promoting safe walking among older people: The effects of a physical and cognitive training intervention vs. physical training alone on mobility and falls among older community-dwelling men and women (the PASSWORD study): Design and methods of a randomized controlled trial. BMC Geriatr. 2018, 18, 215. [Google Scholar] [CrossRef] [Green Version]
- Monteagudo, P.; Roldan, A.; Cordellat, A.; Gomez-Cabrera, M.C.; Blasco-Lafarga, C. Continuous Compared to Accumulated Walking-Training on Physical Function and Health-Related Quality of Life in Sedentary Older Persons. Int. J. Environ. Res. Public Health 2020, 17, 6060. [Google Scholar] [CrossRef] [PubMed]
- Les, A.; Guszkowska, M.; Piotrowska, J.; Rutkowska, I. Changes in perceived quality of life and subjective age in older women participating in Nordic Walking classes and memory training. J. Sports Med. Phys. Fit. 2019, 59, 1783–1790. [Google Scholar] [CrossRef]
- Whitlock, K.G.; Piponov, H.I.; Shah, S.H.; Wang, O.J.; Gonzalez, M.H. Gender Role in Total Knee Arthroplasty: A Retrospective Analysis of Perioperative Outcomes in US Patients. J. Arthroplast. 2016, 31, 2736–2740. [Google Scholar] [CrossRef]
- Deshpande, P.R.; Rajan, S.; Sudeepthi, B.L.; Abdul Nazir, C.P. Patient-reported outcomes: A new era in clinical research. Perspect. Clin. Res. 2011, 2, 137–144. [Google Scholar] [CrossRef]
- Roos, E.M.; Toksvig-Larsen, S. Knee injury and Osteoarthritis Outcome Score (KOOS)—Validation and comparison to the WOMAC in total knee replacement. Health Qual. Life Outcomes 2003, 1, 17. [Google Scholar] [CrossRef] [Green Version]
- Ahlback, S. Osteoarthrosis of the knee. A radiographic investigation. Acta Radiol. Diagn. 1968, 227, 7–72. [Google Scholar]
- Chun, E.H.; Kim, Y.J.; Woo, J.H. Which is your choice for prolonging the analgesic duration of single-shot interscalene brachial blocks for arthroscopic shoulder surgery? intravenous dexamethasone 5 mg vs. perineural dexamethasone 5 mg randomized, controlled, clinical trial. Medicine 2016, 95, e3828. [Google Scholar] [CrossRef]
- Savkin, R.; Buker, N.; Gungor, H.R. The effects of preoperative neuromuscular electrical stimulation on the postoperative quadriceps muscle strength and functional status in patients with fast-track total knee arthroplasty. Acta Orthop. Belg. 2021, 87, 735–744. [Google Scholar] [CrossRef] [PubMed]
- Schimpl, M.; Moore, C.; Lederer, C.; Neuhaus, A.; Sambrook, J.; Danesh, J.; Ouwehand, W.; Daumer, M. Association between walking speed and age in healthy, free-living individuals using mobile accelerometry—A cross-sectional study. PLoS ONE 2011, 6, e23299. [Google Scholar] [CrossRef] [PubMed]
- Serwe, K.M.; Swartz, A.M.; Hart, T.L.; Strath, S.J. Effectiveness of long and short bout walking on increasing physical activity in women. J. Women’s Health 2011, 20, 247–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riebe, D.; Liguori, G.; Magal, M. ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Wolters Kluwer/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2018. [Google Scholar]
- Bazett-Jones, D.M.; Cobb, S.C.; Joshi, M.N.; Cashin, S.E.; Earl, J.E. Normalizing hip muscle strength: Establishing body-size-independent measurements. Arch. Phys. Med. Rehabil. 2011, 92, 76–82. [Google Scholar] [CrossRef]
- Rikli, R.E.; Jones, C.J. Development and validation of criterion-referenced clinically relevant fitness standards for maintaining physical independence in later years. Gerontologist 2013, 53, 255–267. [Google Scholar] [CrossRef] [PubMed]
- Peer, M.A.; Lane, J. The Knee Injury and Osteoarthritis Outcome Score (KOOS): A review of its psychometric properties in people undergoing total knee arthroplasty. J. Orthop. Sports Phys. Ther. 2013, 43, 20–28. [Google Scholar] [CrossRef]
- Liang, K.-Y.; Zeger, S.L. Longitudinal data analysis using generalized linear models. Biometrika 1986, 73, 13–22. [Google Scholar] [CrossRef]
- Sawilowsky, S. New effect size rules of thumb. J. Mod. Appl. Stat. Methods 2009, 8, 467–474. [Google Scholar] [CrossRef]
- Unver, B.; Kalkan, S.; Yuksel, E.; Kahraman, T.; Karatosun, V. Reliability of the 50-foot walk test and 30-sec chair stand test in total knee arthroplasty. Acta Ortop. Bras. 2015, 23, 184–187. [Google Scholar] [CrossRef] [Green Version]
- Ko, V.; Naylor, J.M.; Harris, I.A.; Crosbie, J.; Yeo, A.E. The six-minute walk test is an excellent predictor of functional ambulation after total knee arthroplasty. BMC Musculoskelet. Disord. 2013, 14, 145. [Google Scholar] [CrossRef] [Green Version]
- Rossi, M.D.; Hasson, S.; Kohia, M.; Pineda, E.; Bryan, W. Mobility and perceived function after total knee arthroplasty. J. Arthroplasty 2006, 21, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Calatayud, J.; Casana, J.; Ezzatvar, Y.; Jakobsen, M.D.; Sundstrup, E.; Andersen, L.L. High-intensity preoperative training improves physical and functional recovery in the early post-operative periods after total knee arthroplasty: A randomized controlled trial. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 2864–2872. [Google Scholar] [CrossRef] [PubMed]
- Fransen, M.; McConnell, S.; Harmer, A.R.; Van der Esch, M.; Simic, M.; Bennell, K.L. Exercise for osteoarthritis of the knee. Cochrane Database Syst. Rev. 2015, 1, CD004376. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, M.; Sawano, S.; Kugo, M.; Maegawa, S.; Kawasaki, T.; Ichihashi, N. Physical Activity Promotes Gait Improvement in Patients with Total Knee Arthroplasty. J. Arthroplasty 2016, 31, 984–988. [Google Scholar] [CrossRef] [PubMed]
- Mizner, R.L.; Petterson, S.C.; Stevens, J.E.; Axe, M.J.; Snyder-Mackler, L. Preoperative quadriceps strength predicts functional ability one year after total knee arthroplasty. J. Rheumatol. 2005, 32, 1533–1539. [Google Scholar]
- Mizner, R.L.; Petterson, S.C.; Snyder-Mackler, L. Quadriceps strength and the time course of functional recovery after total knee arthroplasty. J. Orthop. Sports Phys. Ther. 2005, 35, 424–436. [Google Scholar] [CrossRef] [Green Version]
- Mizner, R.L.; Petterson, S.C.; Stevens, J.E.; Vandenborne, K.; Snyder-Mackler, L. Early quadriceps strength loss after total knee arthroplasty. The contributions of muscle atrophy and failure of voluntary muscle activation. J. Bone Joint Surg. Am. 2005, 87, 1047–1053. [Google Scholar] [CrossRef]
- Mizner, R.L.; Snyder-Mackler, L. Altered loading during walking and sit-to-stand is affected by quadriceps weakness after total knee arthroplasty. J. Orthop. Res. 2005, 23, 1083–1090. [Google Scholar] [CrossRef]
- Saleh, K.J.; Lee, L.W.; Gandhi, R.; Ingersoll, C.D.; Mahomed, N.N.; Sheibani-Rad, S.; Novicoff, W.M.; Mihalko, W.M. Quadriceps strength in relation to total knee arthroplasty outcomes. Instr. Course Lect. 2010, 59, 119–130. [Google Scholar]
- Petterson, S.C.; Mizner, R.L.; Stevens, J.E.; Raisis, L.; Bodenstab, A.; Newcomb, W.; Snyder-Mackler, L. Improved function from progressive strengthening interventions after total knee arthroplasty: A randomized clinical trial with an imbedded prospective cohort. Arthritis Rheum. 2009, 61, 174–183. [Google Scholar] [CrossRef]
- Johnson, A.W.; Myrer, J.W.; Hunter, I.; Feland, J.B.; Hopkins, J.T.; Draper, D.O.; Eggett, D. Whole-body vibration strengthening compared to traditional strengthening during physical therapy in individuals with total knee arthroplasty. Physiother. Theory Pract. 2010, 26, 215–225. [Google Scholar] [CrossRef] [PubMed]
- Accettura, A.J.; Brenneman, E.C.; Stratford, P.W.; Maly, M.R. Knee Extensor Power Relates to Mobility Performance in People with Knee Osteoarthritis: Cross-Sectional Analysis. Phys. Ther. 2015, 95, 989–995. [Google Scholar] [CrossRef] [PubMed]
- Pua, Y.H.; Seah, F.J.; Clark, R.A.; Lian-Li Poon, C.; Tan, J.W.; Chong, H.C. Factors associated with gait speed recovery after total knee arthroplasty: A longitudinal study. Semin. Arthritis Rheum. 2017, 46, 544–551. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characters | CON (N = 14) | WT (N = 14) | p | ES |
|---|---|---|---|---|
| Age (years) | 68.5 ± 6.6 | 69.7 ± 2.8 | 0.372 | 0.23 |
| Height (cm) | 152.0 ± 5.8 | 152.8 ± 4.9 | 0.877 | 0.14 |
| Weight (kg) | 65.9 ± 11.5 | 66.4 ± 9.8 | 0.682 | 0.04 |
| BMI (kg/m2) | 28.4 ± 4.0 | 28.4 ± 3.4 | 0.567 | 0.01 |
| Pre-operation | ||||
| Muscle strength | ||||
| HE (Nm/kg) | 72.0 ± 8.2 | 79.0 ± 9.2 | 0.571 | 0.80 |
| HF (Nm/kg) | 32.4 ± 3.5 | 31.3 ± 4.1 | 0.844 | 0.28 |
| KE (Nm/kg) | 42.1 ± 2.9 | 41.5 ± 5.3 | 0.941 | 0.14 |
| KF (Nm/kg) | 41.8 ± 3.0 | 45.2 ± 2.4 | 0.376 | 1.25 |
| Functional test | ||||
| 6MWT (m) | 309.1 ± 31.4 | 326.1 ± 29.7 | 0.693 | 0.55 |
| 8UG (sec) | 9.5 ± 1.6 | 10.7 ± 1.3 | 0.541 | 0.82 |
| 30s-CST (Times) | 10.6 ± 1.1 | 10.4 ± 0.9 | 0.836 | 0.19 |
| KOOS | ||||
| Sym | 63.9 ± 5.1 | 63.7 ± 6.3 | 0.983 | 0.03 |
| Pain | 65.6 ± 4.8 | 63.8 ± 5.6 | 0.817 | 0.31 |
| ADL | 64.5 ± 4.9 | 68.4 ± 6.2 | 0.611 | 0.69 |
| Sports | 40.6 ± 7.1 | 35.5 ± 4.4 | 0.550 | 0.86 |
| QoL | 61.1 ± 5.4 | 51.5 ± 5.8 | 0.218 | 1.71 |
| (Nm/kg) | Baseline | Mid-Exercise | Post-Exercise | Follow-Up | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CON | WT | ES | p | CON | WT | ES | p | CON | WT | ES | p | CON | WT | ES | p | |
| HE | 71.5 ± 5.4 | 85.9 ± 9.9 | 1.58 | 0.199 | 74.6 ± 9.6 | 102.6 ± 12.5 | 2.51 | 0.074 | 77.5 ± 8.0 | 116.9 ± 11.3 § | 4.02 | 0.004 * | 87.6 ± 10.6 | 106.8 ± 9.4 § | 1.91 | 0.177 |
| HF | 27. 6 ± 2.8 | 33.4 ± 3.6 | 1.79 | 0.190 | 26.4 ± 4.3 | 34.5 ± 4.2 | 1.90 | 0.172 | 27.4 ± 3.6 | 37.1 ± 4.7 | 2.32 | 0.094 | 29.6 ± 3.1 | 33.9 ± 5.4 | 0.97 | 0.452 |
| KE | 40.3 ± 5.1 | 45.2 ± 4.9 | 1.17 | 0.476 | 45.9 ± 4.1 | 57.6 ± 5.7 § | 2.36 | 0.091 | 48.2 ± 2.4 | 73.1 ± 7.5 § | 4.47 | 0.001 * | 54.2 ± 3.2 § | 71.4 ± 6.6 § | 3.31 | 0.019 * |
| KF | 43.6 ± 4.0 | 46.1 ± 3.0 | 0.70 | 0.615 | 49.8 ± 3.6 | 54.1 ± 4.0 | 1.13 | 0.406 | 43.7 ± 3.3 | 64.4 ± 4.1 § | 5.62 | 0.001 * | 43.1 ± 3.0 | 65.0 ± 2.6 § | 1.27 | 0.001 * |
| ES | p | ||||||
|---|---|---|---|---|---|---|---|
| Variable | Mid-Exercise | Post-Exercise | Follow-Up | Mid-Exercise | Post-Exercise | Follow-Up | |
| WT | HE | 1.48 | 2.92 | 2.17 | 0.211 | 0.002 | 0.024 |
| HF | 0.28 | 0.88 | 0.11 | 0.751 | 0.514 | 0.154 | |
| KE | 2.33 | 4.40 | 4.51 | 0.032 | 0.001 | 0.012 | |
| KF | 2.26 | 5.09 | 6.73 | 0.301 | 0.002 | 0.001 | |
| CON | HE | 0.40 | 0.88 | 1.91 | 0.468 | 0.216 | 0.165 |
| HF | 0.33 | 0.06 | 0.68 | 0.532 | 0.151 | 0.205 | |
| KE | 1.21 | 1.98 | 3.26 | 0.541 | 0.304 | 0.023 | |
| KF | 1.63 | 0.03 | 0.14 | 0.665 | 0.501 | 0.487 | |
| Baseline | Mid-Exercise | Post-Exercise | Follow-Up | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CON | WT | ES | p | CON | WT | ES | p | CON | WT | ES | p | CON | WT | ES | p | |
| 6MWT (m) | 331.0 ± 16.5 | 341.3 ± 20.5 | 0.55 | 0.696 | 346.6 ± 14.8 | 375.2 ± 21.4 § | 1.55 | 0.271 | 346.1 ± 16.8 | 400.1 ± 23.8 § | 2.62 | 0.40 | 345.8 ± 16.5 | 405.5 ± 30.7 § | 2.42 | 0.093 |
| 8UG (sec) | 10.4 ± 0.7 | 9.5 ± 0.7 | 1.28 | 0.386 | 9.1 ± 0.5 | 8.5 ± 0.5 § | 1.20 | 0.427 | 9.1 ± 0.8 | 8.6 ± 0.8 § | 0.62 | 0.692 | 9.2 ± 0.6 | 8.3 ± 0.7 § | 1.38 | 0.302 |
| 30s-CST (Times) | 11.9 ± 0.9 | 12.2 ± 0.7 | 0.37 | 0.764 | 12.6 ± 0.6 | 14.0 ± 1.0 | 1.69 | 0.238 | 12.6 ± 0.8 | 14.21 ± 1.0 | 1.76 | 0.211 | 12.8 ± 0.7 | 14.0 ± 1.2 | 1.22 | 0.370 |
| ES | p | ||||||
|---|---|---|---|---|---|---|---|
| Variable | Mid-Exercise | Post-Exercise | Follow-Up | Mid-Exercise | Post-Exercise | Follow-Up | |
| WT | 6MWT | 1.62 | 2.65 | 2.46 | 0.031 | 0.012 | 0.001 |
| 8UG | 1.64 | 1.20 | 1.71 | 0.029 | 0.031 | 0.002 | |
| 30s-CST | 2.09 | 2.33 | 1.83 | 0.376 | 0.471 | 0.389 | |
| CON | 6MWT | 0.96 | 0.90 | 0.85 | 0.588 | 0.546 | 0.437 |
| 8UG | 2.14 | 1.73 | 1.84 | 0.632 | 0.652 | 0.594 | |
| 30s-CST | 0.92 | 0.82 | 1.12 | 0.417 | 0.374 | 0.360 | |
| Baseline | Mid-Exercise | Post-Exercise | Follow-Up | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CON | WT | ES | p | CON | WT | ES | p | CON | WT | ES | p | CON | WT | ES | p | |
| Sym | 62.1 ± 4.9 | 71.1 ± 5.4 | 1.74 | 0.200 | 71.2 ± 5.7 § | 76.0 ± 4.7 | 0.91 | 0.487 | 70.9 ± 4.9 | 78.2 ± 3.9 | 1.64 | 0.253 | 83.0 ± 4.1 § | 86.7 ± 3.8 § | 0.93 | 0.514 |
| Pain | 78.2 ± 3.4 | 79.5 ± 4.4 | 0.33 | 0.794 | 84.8 ± 3.5 | 87.6 ± 4.0 | 0.74 | 0.584 | 84.3 ± 4.3 | 90.5 ± 2.0 § | 1.84 | 0.185 | 91.1 ± 3.1 § | 97.3 ± 1.5 § | 2.54 | 0.072 |
| ADL | 76.3 ± 3.2 | 76.6 ± 4.7 | 0.07 | 0.923 | 80.2 ± 5.1 | 89.8 ± 2.4§ | 2.40 | 0.083 | 78.7 ± 5.1 | 87.6 ± 2.6 § | 2.19 | 0.118 | 92.0 ± 2.5 § | 94.6 ± 1.3 § | 1.30 | 0.322 |
| Sports | 47.0 ± 5.2 | 42.3 ± 2.8 | 1.12 | 0.439 | 43.6 ± 3.8 | 50.5 ± 4.5 | 1.65 | 0.229 | 45.1 ± 4.7 | 44.0 ± 2.8 | 0.28 | 0.835 | 45.2 ± 3.8 | 45.6 ± 4.9 | 0.09 | 0.936 |
| QoL | 56.6 ± 4.7 | 60.0 ± 6.3 | 0.61 | 0.696 | 64.6 ± 7.3 | 71.4 ± 6.0 | 1.01 | 0.474 | 63.4 ± 5.8 | 72.8 ± 4.3 § | 1.84 | 0.193 | 68.1 ± 5.8 | 91.0 ± 2.8 § | 5.02 | 0.001 * |
| ES | p | ||||||
|---|---|---|---|---|---|---|---|
| Variable | Mid-Exercise | Post-Exercise | Follow-Up | Mid-Exercise | Post-Exercise | Follow-Up | |
| WT | Sym | 0.97 | 1.51 | 3.34 | 0.521 | 0.321 | 0.002 |
| Pain | 1.93 | 3.22 | 5.42 | 0.074 | 0.024 | 0.002 | |
| ADL | 3.54 | 2.90 | 5.22 | 0.032 | 0.008 | 0.002 | |
| Sports | 2.19 | 0.61 | 0.83 | 0.658 | 0.713 | 0.072 | |
| QoL | 1.85 | 2.37 | 6.36 | 0.067 | 0.012 | 0.001 | |
| CON | Sym | 1.71 | 1.80 | 4.63 | 0.047 | 0.051 | 0.035 |
| Pain | 1.91 | 1.57 | 3.97 | 0.514 | 0.624 | 0.041 | |
| ADL | 0.92 | 0.56 | 5.47 | 0.727 | 0.694 | 0.037 | |
| Sports | 0.75 | 0.38 | 0.40 | 0.865 | 0.792 | 0.698 | |
| QoL | 1.30 | 1.29 | 2.18 | 0.476 | 0.523 | 0.331 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, W.-H.; Hsu, W.-B.; Lin, Z.-R.; Chang, S.-H.; Fan, C.-H.; Kuo, L.-T.; Hsu, W.-W.R. Effects of 24 Weeks of a Supervised Walk Training on Knee Muscle Strength and Quality of Life in Older Female Total Knee Arthroplasty: A Retrospective Cohort Study. Healthcare 2023, 11, 356. https://doi.org/10.3390/healthcare11030356
Hsu W-H, Hsu W-B, Lin Z-R, Chang S-H, Fan C-H, Kuo L-T, Hsu W-WR. Effects of 24 Weeks of a Supervised Walk Training on Knee Muscle Strength and Quality of Life in Older Female Total Knee Arthroplasty: A Retrospective Cohort Study. Healthcare. 2023; 11(3):356. https://doi.org/10.3390/healthcare11030356
Chicago/Turabian StyleHsu, Wei-Hsiu, Wei-Bin Hsu, Zin-Rong Lin, Shr-Hsin Chang, Chun-Hao Fan, Liang-Tseng Kuo, and Wen-Wei Robert Hsu. 2023. "Effects of 24 Weeks of a Supervised Walk Training on Knee Muscle Strength and Quality of Life in Older Female Total Knee Arthroplasty: A Retrospective Cohort Study" Healthcare 11, no. 3: 356. https://doi.org/10.3390/healthcare11030356
APA StyleHsu, W. -H., Hsu, W. -B., Lin, Z. -R., Chang, S. -H., Fan, C. -H., Kuo, L. -T., & Hsu, W. -W. R. (2023). Effects of 24 Weeks of a Supervised Walk Training on Knee Muscle Strength and Quality of Life in Older Female Total Knee Arthroplasty: A Retrospective Cohort Study. Healthcare, 11(3), 356. https://doi.org/10.3390/healthcare11030356