
Effects of Lifestyle Interventions on the Improvement of Chronic Non-Specific Low Back Pain: A Systematic Review and Network Meta-Analysis

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Data Sources and Search
2.3. Study Selection
2.4. Data Extraction Process
2.5. Assessment of Methodological Quality and Risk of Bias
2.6. Statistical Analysis
3. Results
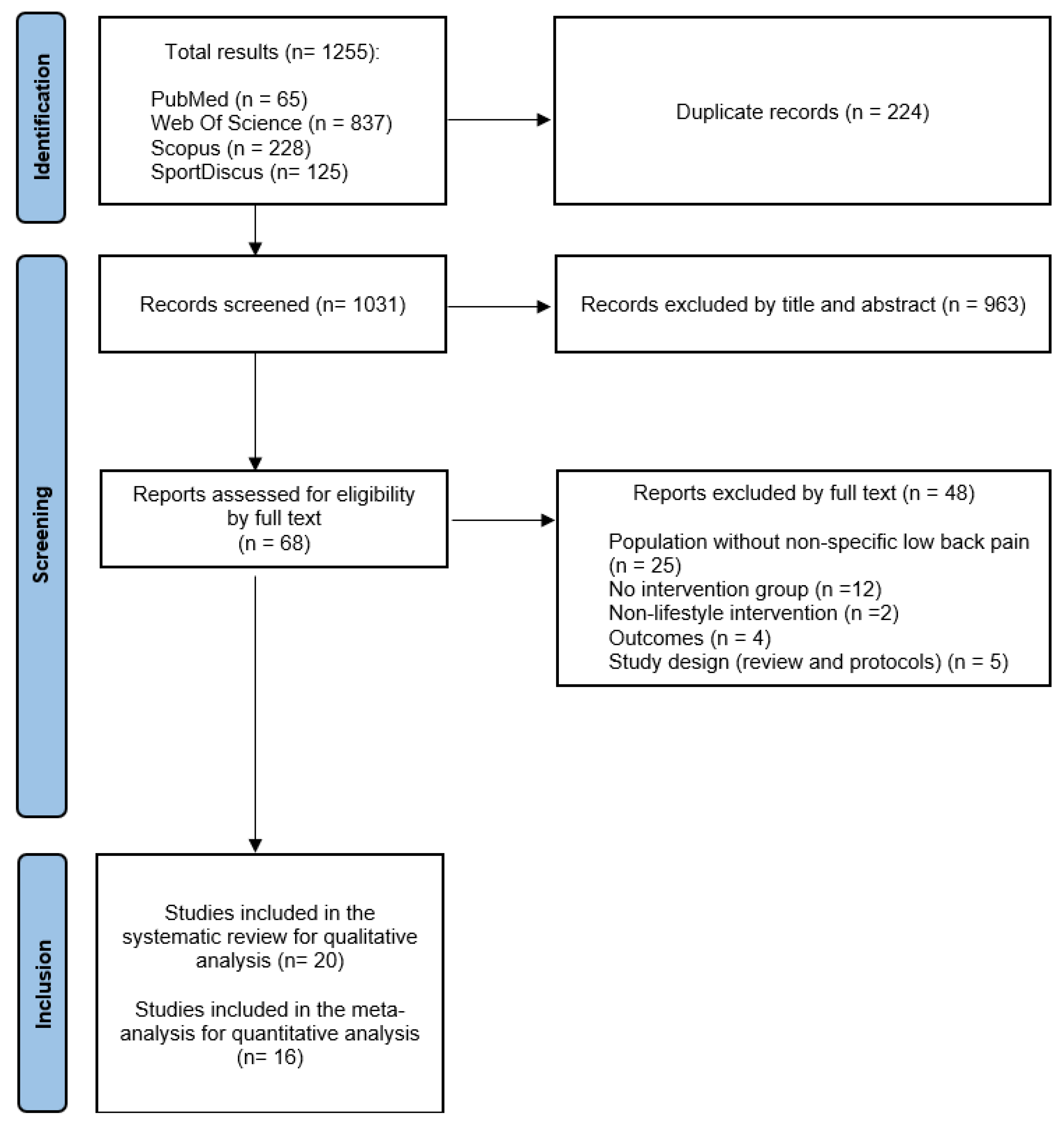
3.1. Study Selection
3.2. Study Characteristics
3.2.1. Sample
3.2.2. Intervention and Follow-Up
3.2.3. Outcomes
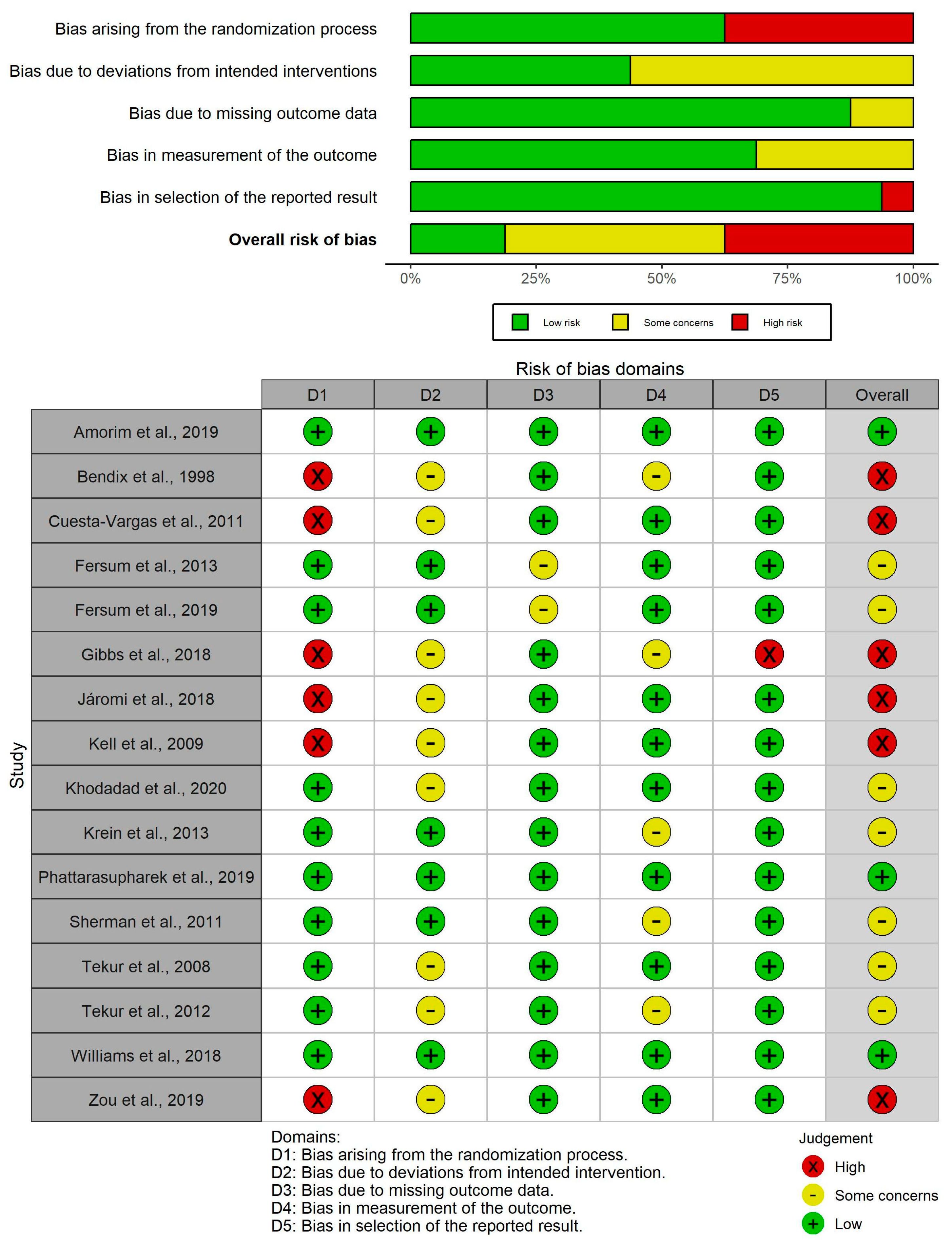
3.3. Methodological Quality and Risk of Bias

| Author and Year | Study Design | Sample Characteristics | Intervention | Comparator/ Control | Main Outcomes | Other Outcomes | Follow-Up | Main Results |
|---|---|---|---|---|---|---|---|---|
| Amorim et al., 2019 [53] | RCT | IG: n = 34 (15 F, 19 M); Age = 59.5 ± 11.9; BMI = 28.9 ± 6.0 CG: n = 34 (19 F, 15 M); Age = 57.1 ± 14.9; BMI = 27.2 ± 5.1 | Promotion of physical activity (information on sedentary behavior + personalized physical activity plan with coaching + motivational interviews + telephone calls) | Promotion of physical activity (information without follow-up) | Pain intensity (NRS) Disability (RMDQ) | Physical activity (IPAQ); fear avoidance (FABQ); depression and anxiety (DASS); sleep quality (PSQI) | Baseline and 6 months (follow-up every week) | Non-significant 1% weekly reduction in RMDQ (p = 0.66) No between-group SSD in NRS or RMDQ (p = 0.815 and p = 0.722, respectively) |
| Baena-Beato et al., 2013 [44] | Non-randomized controlled clinical trial | IG: n = 21 (12 F, 9 M); Age = 50.9 ± 9.6 GC: n = 17 (10 F, 7 M); Age = 46.2 ± 9.8 | Aquatic therapy (resistance + aerobic + mobility exercise) | Waiting list + recommendations on ergonomics, healthy lifestyle and exercise | Pain intensity (VAS) Disability (ODI) | Quality of life (SF-36); Functionality (functional tests) | Baseline and 2 months | Between-group SSD in favor of IG in VAS and ODI (p < 0.001) |
| Bendix et al., 1998 (Project A) [31] | RCT | IG (A1): n = 50 (35 F; 15 M); Age = 41 CG (A2): n = 49 (36 F; 13 M); Age = 41 | A1: Functional restoration (intensive physical exercise + psychological pain management + patient education) | A2: No intervention | Pain intensity (NRS) | Ability to work; ADLs; sports activity | Baseline, 3 weeks and 2 years | No between-group SSD in NRS (p = 0.5) |
| Bendix et al., 1998 (Project B) [31] | RCT | IG 1 (B2): n = 28 (21 F; 7 M); Age = 42.6 IG 2 (B3): n = 34 (25 F; 9 M); Age = 42.6 CG (B1): n = 40 (29 F; 11 M); Age = 38.9 | B2: Intensive physical training + patient education B3: Intensive physical training + psychological pain management | B1: Same as A1 | Same as Project A | Same as Project A | Baseline, 6 weeks and 2 years | Between-group SSD only when comparing B1 vs. B3 in favor of B1 (p = 0.003) |
| Cuesta-Vargas, 2011 [48] | RCT | IG: n = 25 (13 F, 12 M); Age = 39.8 ± 11.2; BMI = 26.2 ± 3.9; PD: 14.3 ± 9.4 weeks CG: n = 24 (14 F, 10 M); Age = 37.6 ± 13.2; BMI = 25.2 ± 4.5; PD: 16.9 ± 9.5 weeks | Multimodal program + Aquatic aerobic exercise | Multimodal program (therapeutic exercise + manual therapy + education) | Pain intensity (VAS) Disability (RMDQ) | Quality of life (SF-12); Functionality (functional tests) | Baseline and 15 weeks | Intragroup SSD for both groups in VAS and RMDQ (IG: p < 0.001 and p < 0.01, respectively; CG: p < 0.001) Between-groups SSD in favor of the IG in VAS (p < 0.05) |
| Fersum et al., 2013 [54] | RCT | IG: n = 51 (27 F, 24 M); Age = 41.0 ± 10.3; BMI = 25.6 ± 4.0 CG: n = 43 (21 F, 22 M); Age = 42.9 ± 12.5; BMI = 25.2 ± 3.5 | Cognitive–functional therapy (cognitive component, specific movement exercises, integration of ADLs and physical activity program) | Multimodal program (manual therapy + general therapeutic exercise) | Pain intensity (NRS) Disability (ODI) | Anxiety and depression (Hopkins Symptoms Checklist); fear-avoidance (FABQ) | Baseline and 3 and 12 months | Intragroup SSD for both groups in NRS and ODI (p < 0.05) Between-group SSD in favor of IG at 3 and 12 months in NRS and ODI (p < 0.001) |
| Fersum et al., 2019 [55] | RCT | IG: n = 30 (16 F, 14 M); Age = 42.9 ± 10.9; BMI = 25.6 ± 4.1 CG: n = 33 (17 F, 16 M); Age = 43.1 ± 12.8; BMI = 25.1 ± 3.7 | Same as Fersum et al., 2013 [54] | Same as Fersum et al., 2013 [54] | Same as Fersum et al., 2013 [54] | Same as Fersum et al., 2013 [54] | Baseline and 3 years | Between-group SSD in favor of the IG at 3 years in ODI (p < 0.001) |
| Gibbs et al., 2018 [50] | RCT | IG: n = 13 (11 F, 2 M); Age = 52 ± 9; BMI = 31.0 ± 7.5 CG: n = 14 (10 F, 4 M); Age = 51 ± 13; BMI = 29.0 ± 5.2 | Intervention on sedentary behavior (face-to-face counseling and by phone + education + use of sit-stand desk + cognitive–behavioral therapy) | No Intervention | Pain intensity (VAS) Disability (ODI) | Physical activity (Global Physical Activity Questionnaire); functionality (functional tests) | Baseline and 3 and 6 months | Intragroup SSD in both groups in ODI at 6 months (p < 0.05) Between-group SSD in favor of the IG in ODI at all follow-up moments (p < 0.001) |
| Járomi et al., 2018 [49] | RCT | IG: n = 67 (62 F, 5 M); Age = 41.73 ± 3.54; BMI = 24.7 ± 1.84; PD = 25.94 ± 9.36 weeks CG: n = 70 (66 F, 4 M); Age = 41.05 ± 3.8; BMI = 24.61 ± 1.78; PD = 27.22 ± 10.60 weeks | Back School education program + general therapeutic exercise | Lifestyle guidance | Pain intensity (VAS) | None | Baseline and 3 months | Intragroup SSD for IG in VAS (p < 0.001) Between-group SSD in favor of the IG in VAS (p < 0.001) |
| Kell et al., 2009 [46] | RCT | IG 1: n = 9 (3 F, 6 M); Age = 40.1 ± 8.7 IG 2: n = 9 (4 F, 5 M); Age = 36.7 ± 8.9 CG: n = 9 (4 F, 5 M); Age = 35.3 ± 7.3 Total PD = 27.6 (range 6–96) months | IG 1: Upper and lower limb resistance exercise IG 2: Aerobic exercise | No intervention | Pain intensity (VAS) Disability (ODI) | Quality of life (SF-36); functionality (functional tests) | Baseline and 4 months | Intragroup SSD for IG 1 in VAS and ODI (p < 0.05) Between-group SSD in favor of IG 1 vs. IG 2 and CG in ODI and VAS (p < 0.05) and IG 2 vs. CG in ODI (p < 0.05) |
| Khodadad et al., 2020 [47] | RCT | IG 1: n = 17; Age = 44.3 ± 1.43; BMI = 23.3 ± 1.17 IG 2: n = 17; Age = 42.2 ± 3.78; BMI = 24.8 ± 1.65 CG: n = 18; Age = 44.4 ± 2.17; BMI = 23.6 ± 1.32 | IG 1: Cognitive–functional therapy (education + exercise + mindfulness) IG 2: Lumbar stabilization exercise | Usual physical therapy | Pain intensity (VAS) Disability (ODI) | Behavioral risk factors (obesity, smoking, physical inactivity and risky alcohol consumption) | Baseline and 2 months | Intragroup SSD for IG 1 and IG 2 in VAS (p = 0.003) No between-group SSD |
| Krein et al., 2013 [56] | RCT | IG: n = 111 (12 F, 99 M); Age = 51.2 ± 12.5; BMI = 30.6 ± 5.7 CG: n = 118 (17 F, 101 M); Age = 51.9 ± 12.8; BMI = 31.6 ± 5.5 | Pedometer-based internet-mediated walking program (goal setting + feedback + e-community) | Pedometer-based walking program | Pain intensity (NRS) Disability (RMDQ) | Physical activity (pedometer); fear-avoidance (FABQ); self-efficacy for exercise (Exercise Regularly Scale) | Baseline and 6 and 12 months | Between-group in favor of IG only in RMDQ at 6 months (p = 0.02) |
| Ma et al., 2021 [43] | Non-randomized controlled clinical trial | IG: n = 73 (36 F, 37 M); Age = 36.3 ± 6.7; BMI = 23.52 ± 3.05 CG: n = 63 (29 F, 34 M); Age = 37.2 ± 7.5; BMI = 24.46 ± 4.72 | Maitland training (abdominal stabilization) + pain self-management | Pain self-management | Pain intensity (VAS) Disability (ODI + QLBPRS) | None | Baseline and 3 months | Between-group SSD in favor of the IG in VAS and ODI (p < 0.05) |
| Notarnicola et al., 2013 [45] | Prospective observational study | Total: n = 60 (33 F, 27 M); Age = 51.2 ± 9.8 | Pilates exercise program | No intervention | Disability (RMDQ + ODI) | Quality of life (SF-36); Ability to perform work tasks (Spinal Functional Sort) | Baseline and 6 months | Intragroup SSD for IG in RMDQ and ODI (p < 0.001) Between-group SSD in favor of IG in ODI (p = 0.006) |
| Phattharas-upharerk et al., 2019 [51] | RCT | IG: n = 36 (24 F, 12 M); Age = 35.7 ± 3.6 CG: n = 36 (22 F, 14 M); Age = 34.8 ± 4.3 | Qigong | Waiting list (general advice on pain self-management) | Pain intensity (VAS) Disability (RMDQ) | Mental status (Srithanya Stress Scale) | Baseline and 6 weeks (follow-up every week) | Intragroup SSD for IG in VAS (p < 0.001) Between-group SSD in favor of the IG in VAS and RMDQ (p < 0.001 and p = 0.022, respectively) |
| Sherman et al., 2011 [59] | RCT | IG 1: n = 92 (62 F, 30 M); Age = 46.6 ± 9.8 IG 2: n = 91 (57 F, 34 M); Age = 49 ± 9.91 CG: n = 45 (27 F, 18 M); Age = 50.8 ± 9.07 | IG 1: Yoga IG 2: General exercise | The Back Pain Helpbook | Pain intensity (NRS) Disability (RMDQ) | None | Baseline, 3 months and 26 weeks | Intragroup SSD for all groups in RMDQ at all follow-up times and in VAS at 12 weeks Between-group SSD in favor of IG 1 vs. CG in RMDQ and in VAS; between-group SSD in favor of IG 2 vs. CG only in RMDQ; without DES between both IG |
| Sofi et al., 2011 [42] | Non-randomized community trial | Total: n = 650 (560 F, 90 M); Age: 65 (range 23–87); BMI: 26.5 ± 4.2 | Empoli Adaptive Physical Activity | - | Pain intensity (VAS) | Functionality (Short Physical Performance Battery) | Baseline and 12-months | Between-group SSD between adherence and non-adherence for the VAS (p < 0.0001) |
| Tekur et al., 2008 [57] | RCT | IG: n = 40 (21 F, 19 M); Age = 49 ± 3.6 CG: n = 40 (15 F, 25 M); Age = 48 ± 4 | Yoga + pain self-management | Mobility exercise + pain self-management | Disability (ODI) | None | Baseline and 1 week | Intragroup SSD for IG in ODI (p = 0.001) Between-group SSD in favor of the GI in ODI (p < 0.001) |
| Tekur et al., 2012 [58] | RCT | Same as Tekur et al., 2008 [57] | Same as Tekur et al., 2008 [57] | Same as Tekur et al., 2008 [57] | Pain intensity (NRS) | Anxiety (State-Trait Anxiety Inventory); depression (Beck’s depression inventory); functionality (sit and reach) | Baseline and 1 week | Intragroup SSD for both groups in VAS (IG: p < 0.001 and CG: p = 0.005) Between-group SSD in favor of the IG in VAS (p < 0.001) |
| Williams et al., 2018 [52] | RCT | IG: n = 79 (48 F, 31 M); Age = 56.0 ± 13.3; BMI = 32.4 ± 3.5 CG: n = 80 (46 F, 34 M); Age = 57.4 ± 13.6; BMI = 32.1 ± 3.6 | Healthy lifestyle promotion (brief telephone advice + offer of a clinical consultation + referral to a telephone-based health coaching service) | Waiting list | Pain intensity (NRS) Disability (RMDQ) | Quality of life (SF-12); sleep quality (PSQI); physical activity (Active Australia Survey); depression and anxiety (DASS); fear-avoidance (FABQ); behavioral risk factors | Baseline and 6 months (follow-up every month) | Between-group SSD in favor of IG in NRS only at 10 and 18 weeks (p = 0.05 and p = 0.01, respectively) |
| Zou et al., 2019 [60] | RCT | IG 1: n = 15 (11 F, 4 M); Age = 58.13 ± 5.38 IG 2: n = 15 (11 F, 4 M); Age = 58.4 ± 5.08 CG: n = 13 (10 F, 3 M); Age = 60.67 ± 2.58 | IG 1: Tai Chi IG 2: Core stability training | No intervention | Pain intensity (VAS) | None | Baseline and 3 months | Between-group SSD in favor of IG 1 (p < 0.01) vs. CG and IG 2 vs. CG (p < 0.01) |
| Author and Year | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total | Quality |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Amorim et al., 2019 [53] | YES | YES | YES | YES | NO | NO | YES | NO | YES | YES | YES | 7 | High |
| Bendix et al., 1998 [31] | YES | YES | NO | YES | NO | NO | NO | YES | NO | YES | YES | 5 | Moderate |
| Cuesta-Vargas et al., 2011 [48] | YES | YES | NO | YES | NO | YES | YES | YES | NO | YES | YES | 7 | High |
| Fersum et al., 2013 [54] | YES | YES | YES | YES | NO | NO | YES | NO | YES | YES | YES | 7 | High |
| Fersum et al., 2019 [55] | YES | YES | YES | YES | NO | NO | YES | NO | YES | YES | YES | 7 | High |
| Gibbs et al., 2018 [50] | YES | YES | NO | YES | NO | NO | YES | YES | NO | YES | YES | 6 | High |
| Járomi et al., 2018 [49] | YES | YES | NO | YES | NO | NO | YES | YES | NO | YES | YES | 6 | High |
| Kell et al., 2009 [46] | YES | YES | NO | YES | NO | NO | NO | NO | NO | YES | YES | 4 | Moderate |
| Khodadad et al., 2020 [47] | YES | YES | YES | YES | NO | NO | YES | YES | NO | YES | YES | 7 | High |
| Krein et al., 2013 [56] | YES | YES | YES | YES | NO | NO | NO | YES | YES | YES | YES | 7 | High |
| Phattharasupharerk et al., 2019 [51] | YES | YES | YES | YES | NO | NO | YES | YES | YES | YES | YES | 8 | High |
| Sherman et al., 2011 [59] | YES | YES | YES | YES | NO | NO | NO | YES | YES | YES | YES | 7 | High |
| Tekur et al., 2008 [57] | YES | YES | YES | YES | NO | NO | YES | YES | NO | YES | YES | 7 | High |
| Tekur et al., 2012 [58] | YES | YES | YES | YES | NO | NO | NO | YES | NO | YES | YES | 6 | High |
| Williams et al., 2018 [52] | YES | YES | YES | YES | NO | NO | YES | YES | YES | YES | YES | 8 | High |
| Zou et al., 2019 [60] | YES | YES | NO | YES | NO | NO | YES | YES | NO | YES | YES | 6 | High |
3.4. Review Results
3.4.1. Pain Intensity
3.4.2. Functional Disability
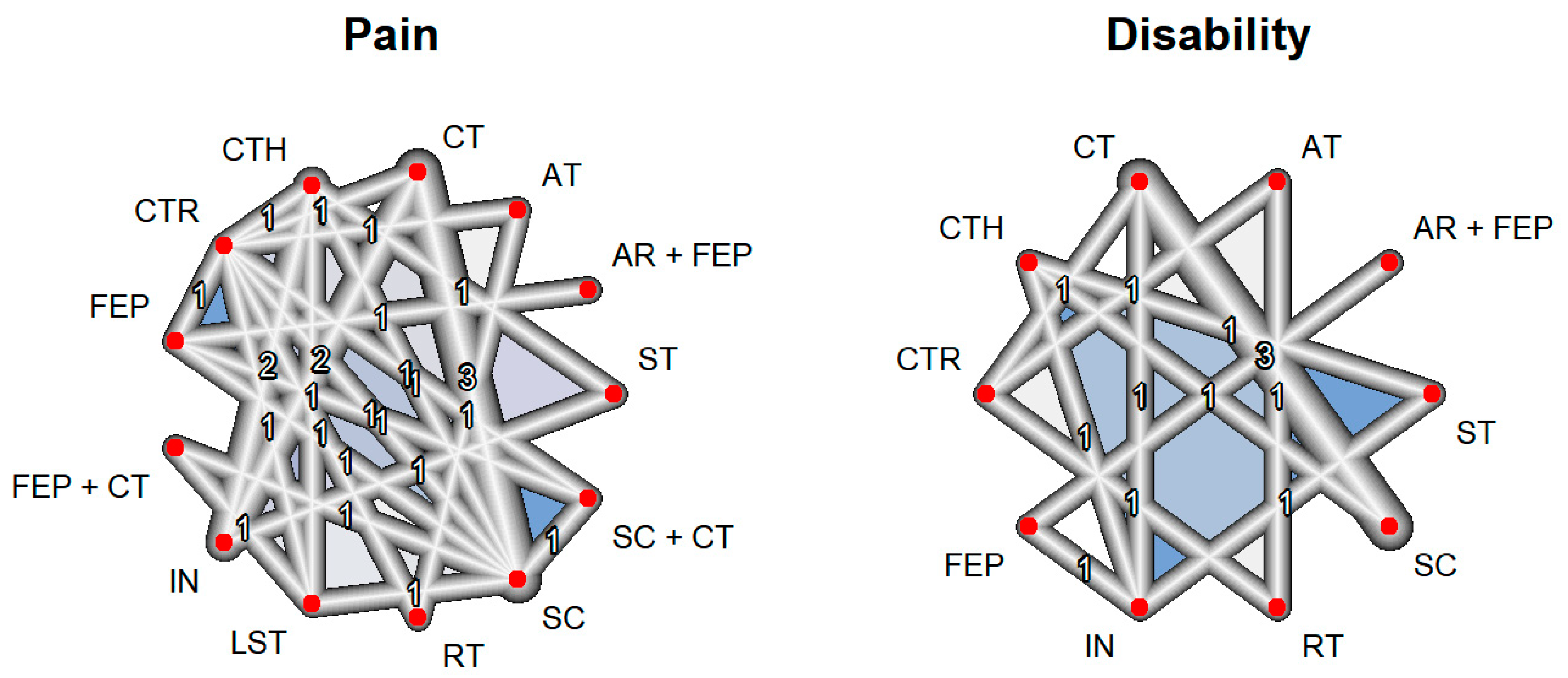
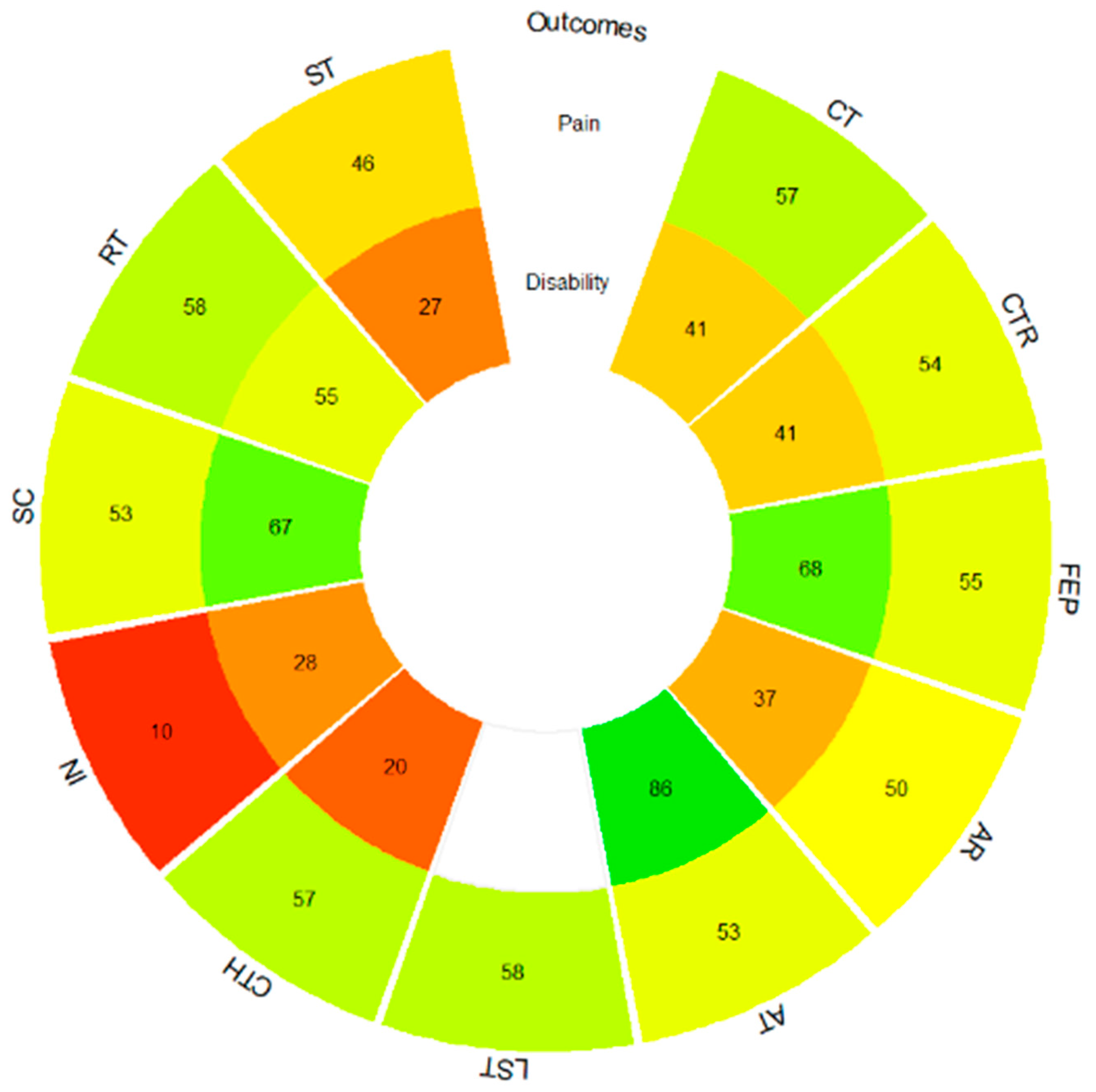
3.5. Meta-Analysis Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- James, S.L.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Briggs, A.M. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef]
- Wu, A.; March, L.; Zheng, X.; Huang, J.; Wang, X.; Zhao, J.; Blyth, F.M.; Smith, E.; Buchbinder, R.; Hoy, D. Global low back pain prevalence and years lived with disability from 1990 to 2017: Estimates from the Global Burden of Disease Study 2017. Ann. Transl. Med. 2020, 8, 299. [Google Scholar] [CrossRef] [PubMed]
- Cieza, A.; Causey, K.; Kamenov, K.; Hanson, S.W.; Chatterji, S.; Vos, T. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 2006–2017. [Google Scholar] [CrossRef] [PubMed]
- Buchbinder, R.; van Tulder, M.; Öberg, B.; Costa, L.M.; Woolf, A.; Schoene, M.; Croft, P.; Lancet Low Back Pain Series Working Group. Low back pain: A call for action. Lancet 2018, 391, 2384–2388. [Google Scholar] [CrossRef]
- Maher, C.; Underwood, M.; Buchbinder, R. Non-specific low back pain. Lancet 2017, 389, 736–747. [Google Scholar] [CrossRef] [PubMed]
- Bardin, L.D.; King, P.; Maher, C.G. Diagnostic triage for low back pain: A practical approach for primary care. Med. J. Aust. 2017, 206, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Costa, L.d.C.M.; Maher, C.G.; Hancock, M.J.; McAuley, J.H.; Herbert, R.D.; Costa, L.O. The prognosis of acute and persistent low-back pain: A meta-analysis. Can. Med. Assoc. J. 2012, 184, E613–E624. [Google Scholar] [CrossRef] [PubMed]
- Wallwork, S.B.; Braithwaite, F.A.; O’keeffe, M.; Travers, M.J.; Summers, S.J.; Lange, B.; Hince, D.A.; Costa, L.O.; Costa, L.d.C.M.; Chiera, B.; et al. The clinical course of acute, subacute and persistent low back pain: A systematic review and meta-analysis. Can. Med. Assoc. J. 2024, 196, E29–E46. [Google Scholar] [CrossRef] [PubMed]
- A Al Mulhim, F.; A Alalwan, H.; Alkhars, A.M.; Almutairi, A.; AlSaeed, M.N.; Althabit, F.M.; Al Mulhim, F.A.; Alalwan, H.A. Prevalence of Low Back Pain and Its Related Risk Factors and Disability Following Lumbar Discectomy: A Single-Center Study. Cureus 2023, 15, e49729. [Google Scholar] [CrossRef]
- Adelt, E.; Schoettker-Koeniger, T.; Luedtke, K.; Hall, T.; Schäfer, A. Lumbar movement control in non-specific chronic low back pain: Evaluation of a direction-specific battery of tests using item response theory. Musculoskelet. Sci. Pract. 2021, 55, 102406. [Google Scholar] [CrossRef]
- Stričević, J.; Papež, B.J. Non-specific low back pain: Occupational or lifestyle consequences? Wien. Klin. Wochenschr. 2015, 127, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Foster, N.E.; Anema, J.R.; Cherkin, D.; Chou, R.; Cohen, S.P.; Gross, D.P.; Ferreira, P.H.; Fritz, J.M.; Koes, B.W.; Peul, W.; et al. Prevention and treatment of low back pain: Evidence, challenges, and promising directions. Lancet 2018, 391, 2368–2383. [Google Scholar] [CrossRef] [PubMed]
- Hartvigsen, J.; Hancock, M.J.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J.; et al. What low back pain is and why we need to pay attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef] [PubMed]
- Zadro, J.; O’keeffe, M.; Maher, C. Do physical therapists follow evidence-based guidelines when managing musculoskeletal conditions? Systematic review. BMJ Open 2019, 9, e032329. [Google Scholar] [CrossRef] [PubMed]
- Dowell, D.; Haegerich, T.M.; Chou, R. CDC Guideline for Prescribing Opioids for Chronic Pain—United States, 2016. JAMA 2016, 315, 1624–1645. [Google Scholar] [CrossRef] [PubMed]
- Cashin, A.G.; Rizzo, R.R.; Wand, B.M.; E O’Connell, N.; Lee, H.; Bagg, M.K.; O’Hagan, E.; Maher, C.G.; Furlan, A.D.; van Tulder, M.W.; et al. Non-pharmacological and non-surgical treatments for low back pain in adults: An overview of Cochrane Reviews. Cochrane Database Syst. Rev. 2021, 2021, CD014691. [Google Scholar] [CrossRef]
- Qaseem, A.; Wilt, T.J.; McLean, R.M.; Forciea, M.A.; for the Clinical Guidelines Committee of the American College of Physicians. Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of Physicians. Ann. Intern. Med. 2017, 166, 514. [Google Scholar] [CrossRef] [PubMed]
- George, S.Z.; Fritz, J.M.; Silfies, S.P.; Schneider, M.J.; Beneciuk, J.M.; Lentz, T.A.; Gilliam, J.R.; Hendren, S.; Norman, K.S. Interventions for the Management of Acute and Chronic Low Back Pain: Revision 2021. J. Orthop. Sports Phys. Ther. 2021, 51, CPG1–CPG60. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro Scale for Rating Quality of Randomized Controlled Trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef]
- Albanese, E.; Bütikofer, L.; Armijo-Olivo, S.; Ha, C.; Egger, M. Construct validity of the Physiotherapy Evidence Database (PEDro) quality scale for randomized trials: Item response theory and factor analyses. Res. Synth. Methods 2020, 11, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Study Quality Assessment Tools|NHLBI, NIH. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 20 May 2022).
- Viechtbauer, W. Conducting Meta-Analyses in R with the metafor package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef]
- Balduzzi, S.; Rücker, G.; Nikolakopoulou, A.; Papakonstantinou, T.; Salanti, G.; Efthimiou, O.; Schwarzer, G. netmeta: An R Package for Network Meta-Analysis Using Frequentist Methods. J. Stat. Softw. 2023, 106, 1–40. [Google Scholar] [CrossRef]
- Luo, D.; Wan, X.; Liu, J.; Tong, T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med. Res. 2018, 27, 1785–1805. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration: London, UK, 2011; Available online: https://www.handbook.cochrane.org (accessed on 10 July 2023).
- Drevon, D.; Fursa, S.R.; Malcolm, A.L. Intercoder Reliability and Validity of WebPlotDigitizer in Extracting Graphed Data. Behav. Modif. 2016, 41, 323–339. [Google Scholar] [CrossRef]
- Bendix, A.F.; Bendix, T.; Labriola, M.; Bœkgaard, P. Functional Restoration for Chronic Low Back Pain: Two-year follow-up of two randomized clinical trials. Spine 1998, 23, 717–725. [Google Scholar] [CrossRef]
- Rosenthal, R. Meta-Analytic Procedures for Social Research; Sage Publications: Newbury Park, CA, USA, 1993. [Google Scholar]
- Berlim, M.T.; McGirr, A.; dos Santos, N.R.; Tremblay, S.; Martins, R. Efficacy of theta burst stimulation (TBS) for major depression: An exploratory meta-analysis of randomized and sham-controlled trials. J. Psychiatr. Res. 2017, 90, 102–109. [Google Scholar] [CrossRef]
- Kallapiran, K.; Koo, S.; Kirubakaran, R.; Hancock, K. Review: Effectiveness of mindfulness in improving mental health symptoms of children and adolescents: A meta-analysis. Child Adolesc. Ment. Health 2015, 20, 182–194. [Google Scholar] [CrossRef]
- McGirr, A.; Berlim, M.T.; Bond, D.J.; Neufeld, N.H.; Chan, P.Y.; Yatham, L.N.; Lam, R.W. A systematic review and meta-analysis of randomized controlled trials of adjunctive ketamine in electroconvulsive therapy: Efficacy and tolerability. J. Psychiatr. Res. 2015, 62, 23–30. [Google Scholar] [CrossRef]
- Papadopoulos, V.P.; Apergis, N.; Filippou, D.K. Nocturia in CPAP-Treated Obstructive Sleep Apnea Patients: A Systematic Review and Meta-Analysis. SN Compr. Clin. Med. 2020, 2, 2799–2807. [Google Scholar] [CrossRef]
- Yagiz, G.; Akaras, E.; Kubis, H.-P.; Owen, J.A. The Effects of Resistance Training on Architecture and Volume of the Upper Extremity Muscles: A Systematic Review of Randomised Controlled Trials and Meta-Analyses. Appl. Sci. 2022, 12, 1593. [Google Scholar] [CrossRef]
- Bielewicz, J.; Daniluk, B.; Kamieniak, P. VAS and NRS, Same or Different? Are Visual Analog Scale Values and Numerical Rating Scale Equally Viable Tools for Assessing Patients after Microdiscectomy? Pain Res. Manag. 2022, 2022, 5337483. [Google Scholar] [CrossRef]
- Kersten, R.; Fikkers, J.; Wolterbeek, N.; Öner, F.; van Gaalen, S. Are the Roland Morris Disability Questionnaire and Oswestry Disability Index interchangeable in patients after lumbar spinal fusion? J. Back Musculoskelet. Rehabil. 2021, 34, 605–611. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Jackson, D.; Barrett, J.K.; Lu, G.; Ades, A.E.; White, I.R. Consistency and inconsistency in network meta-analysis: Concepts and models for multi-arm studies. Res. Synth. Methods 2012, 3, 98–110. [Google Scholar] [CrossRef] [PubMed]
- Chaimani, A.; Higgins, J.P.T.; Mavridis, D.; Spyridonos, P.; Salanti, G. Graphical Tools for Network Meta-Analysis in STATA. PLoS ONE 2013, 8, e76654. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Lova, R.M.; Nucida, V.; Taviani, A.; Benvenuti, F.; Stuart, M.; Weinrich, M.; Cecchi, F.; Abbate, R.; Gensini, G.F.; et al. Adaptive physical activity and back pain: A non-randomised community-based intervention trial. Eur. J. Phys. Rehabil. Med. 2011, 47, 543–549. [Google Scholar] [PubMed]
- Ma, Q.; Song, D.; Ma, Y.; Zhang, L.; Mi, L. Study on the improvement of Maitland combined with self-management on sedentary people with low back pain. Acta Med. Mediterr. 2021, 37, 387–393. [Google Scholar] [CrossRef]
- Baena-Beato, P.; Artero, E.G.; Arroyo-Morales, M.; Robles-Fuentes, A.; Gatto-Cardia, M.C.; Delgado-Fernández, M. Aquatic therapy improves pain, disability, quality of life, body composition and fitness in sedentary adults with chronic low back pain. A controlled clinical trial. Clin. Rehabil. 2013, 28, 350–360. [Google Scholar] [CrossRef]
- Notarnicola, A.; Fischetti, F.; Maccagnano, G.; Comes, R.; Tafuri, S.; Moretti, B. Daily pilates exercise or inactivity for patients with low back pain: A clinical prospective observational study. Eur. J. Phys. Rehabil. Med. 2013, 50, 59–66. [Google Scholar]
- Kell, R.T.; Asmundson, G.J.G. A Comparison of Two Forms of Periodized Exercise Rehabilitation Programs in the Management of Chronic Nonspecific Low-Back Pain. J. Strength Cond. Res. 2009, 23, 513–523. [Google Scholar] [CrossRef]
- Khodadad, B.; Letafatkar, A.; Hadadnezhad, M.; Shojaedin, S. Comparing the Effectiveness of Cognitive Functional Treatment and Lumbar Stabilization Treatment on Pain and Movement Control in Patients With Low Back Pain. Sports Health 2019, 12, 289–295. [Google Scholar] [CrossRef]
- Cuesta-Vargas, A.I.; García-Romero, J.C.; Arroyo-Morales, M.; Diego-Acosta, M.; Daly, D.J. Exercise, Manual Therapy, and Education with or Without High-Intensity Deep-Water Running for Nonspecific Chronic Low Back Pain: A pragmatic randomized controlled trial. Am. J. Phys. Med. Rehabil. 2011, 90, 526–538. [Google Scholar] [CrossRef]
- Járomi, M.; Kukla, A.; Szilágyi, B.; Simon-Ugron, Á.; Bobály, V.K.; Makai, A.; Linek, P.; Ács, P.; Leidecker, E. Back School programme for nurses has reduced low back pain levels: A randomised controlled trial. J. Clin. Nurs. 2018, 27, E895–E902. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, B.B.; Hergenroeder, A.L.; Perdomo, S.J.; Kowalsky, R.J.; Delitto, A.; Jakicic, J.M. Reducing sedentary behaviour to decrease chronic low back pain: The stand back randomised trial. Occup. Environ. Med. 2018, 75, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Phattharasupharerk, S.; Purepong, N.; Eksakulkla, S.; Siriphorn, A. Effects of Qigong practice in office workers with chronic non-specific low back pain: A randomized control trial. J. Bodyw. Mov. Ther. 2019, 23, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.; Wiggers, J.; O’Brien, K.M.; Wolfenden, L.; Yoong, S.L.; Hodder, R.K.; Lee, H.; Robson, E.K.; McAuley, J.H.; Haskins, R.; et al. Effectiveness of a healthy lifestyle intervention for chronic low back pain: A randomised controlled trial. Pain 2018, 159, 1137–1146. [Google Scholar] [CrossRef] [PubMed]
- Amorim, A.B.; Pappas, E.; Simic, M.; Ferreira, M.L.; Jennings, M.; Tiedemann, A.; Carvalho-E-Silva, A.P.; Caputo, E.; Kongsted, A.; Ferreira, P.H. Integrating Mobile-health, health coaching, and physical activity to reduce the burden of chronic low back pain trial (IMPACT): A pilot randomised controlled trial. BMC Musculoskelet. Disord. 2019, 20, 71. [Google Scholar] [CrossRef]
- Fersum, K.V.; O’Sullivan, P.; Skouen, J.; Smith, A.; Kvåle, A. Efficacy of classification-based cognitive functional therapy in patients with non-specific chronic low back pain: A randomized controlled trial. Eur. J. Pain 2013, 17, 916–928. [Google Scholar] [CrossRef] [PubMed]
- Fersum, K.V.; Smith, A.; Kvåle, A.; Skouen, J.S.; O’Sullivan, P. Cognitive functional therapy in patients with non-specific chronic low back pain—A randomized controlled trial 3-year follow-up. Eur. J. Pain 2019, 23, 1416–1424. [Google Scholar] [CrossRef] [PubMed]
- Krein, S.L.; Kadri, R.; Hughes, M.; A Kerr, E.; Piette, J.D.; Holleman, R.; Kim, H.M.; Richardson, C.R. Pedometer-Based Internet-Mediated Intervention For Adults With Chronic Low Back Pain: Randomized Controlled Trial. J. Med. Internet Res. 2013, 15, e181. [Google Scholar] [CrossRef] [PubMed]
- Tekur, P.; Singphow, C.; Nagendra, H.R.; Raghuram, N. Effect of Short-Term Intensive Yoga Program on Pain, Functional Disability and Spinal Flexibility in Chronic Low Back Pain: A Randomized Control Study. J. Altern. Complement. Med. 2008, 14, 637–644. [Google Scholar] [CrossRef] [PubMed]
- Tekur, P.; Nagarathna, R.; Chametcha, S.; Hankey, A.; Nagendra, H. A comprehensive yoga programs improves pain, anxiety and depression in chronic low back pain patients more than exercise: An RCT. Complement. Ther. Med. 2012, 20, 107–118. [Google Scholar] [CrossRef] [PubMed]
- Sherman, K.J.; Cherkin, D.C.; Wellman, R.D.; Cook, A.J.; Hawkes, R.J.; Delaney, K.; Deyo, R.A. A Randomized Trial Comparing Yoga, Stretching, and a Self-care Book for Chronic Low Back Pain. Arch. Intern. Med. 2011, 171, 2019–2026. [Google Scholar] [CrossRef]
- Zou, L.; Zhang, Y.; Liu, Y.; Tian, X.; Xiao, T.; Liu, X.; Yeung, A.S.; Liu, J.; Wang, X.; Yang, Q. The Effects of Tai Chi Chuan Versus Core Stability Training on Lower-Limb Neuromuscular Function in Aging Individuals with Non-Specific Chronic Lower Back Pain. Medicina 2019, 55, 60. [Google Scholar] [CrossRef]
- Castarlenas, E.; Jensen, M.P.; Von Baeyer, C.L.; Miró, J. Psychometric Properties of the Numerical Rating Scale to Assess Self-Reported Pain Intensity in Children and Adolescents. Clin. J. Pain 2017, 33, 376–383. [Google Scholar] [CrossRef]
- Roland, M.; Fairbank, J. The Roland–Morris Disability Questionnaire and the Oswestry Disability Questionnaire. Spine 2000, 25, 3115–3124. [Google Scholar] [CrossRef] [PubMed]
- Melikoglu, M.A.; Kocabas, H.; Sezer, I.; Bilgilisoy, M.; Tuncer, T. Validation of the Turkish Version of the Quebec Back Pain Disability Scale for Patients With Low Back Pain. Spine 2009, 34, E219–E224. [Google Scholar] [CrossRef] [PubMed]
- Otero-Ketterer, E.; Peñacoba-Puente, C.; Pinheiro-Araujo, C.F.; Valera-Calero, J.A.; Ortega-Santiago, R. Biopsychosocial Factors for Chronicity in Individuals with Non-Specific Low Back Pain: An Umbrella Review. Int. J. Environ. Res. Public Health 2022, 19, 10145. [Google Scholar] [CrossRef]
- Pires, D.A.d.F.; Cruz, E.J.C.B.; Canhão, H.C.d.M.; Nunes, C.D.R.D. The role of pain and disability changes after physiotherapy treatment on global perception of improvement in patients with chronic low back pain. Musculoskelet. Sci. Pract. 2020, 47, 102139. [Google Scholar] [CrossRef]
- Owen, P.J.; Miller, C.T.; Mundell, N.L.; Verswijveren, S.J.J.M.; Tagliaferri, S.D.; Brisby, H.; Bowe, S.J.; Belavy, D.L. Which specific modes of exercise training are most effective for treating low back pain? Network meta-analysis. Br. J. Sports Med. 2020, 54, 1279–1287. [Google Scholar] [CrossRef]
- Fernández-Rodríguez, R.; Álvarez-Bueno, C.; Cavero-Redondo, I.; Torres-Costoso, A.; Pozuelo-Carrascosa, D.P.; Reina-Gutiérrez, S.; Pascual-Morena, C.; Martínez-Vizcaíno, V. Best Exercise Options for Reducing Pain and Disability in Adults With Chronic Low Back Pain: Pilates, Strength, Core-Based, and Mind-Body. A Network Meta-analysis. J. Orthop. Sports Phys. Ther. 2022, 52, 505–521. [Google Scholar] [CrossRef]
- Tian, S.; Zhao, D. Comparative effectiveness of exercise interventions for low back pain: A systematic review and network meta-analysis of 41 randomised controlled trials. Lancet 2018, 392, S21. [Google Scholar] [CrossRef]
- Shi, J.; Hu, Z.-Y.; Wen, Y.-R.; Wang, Y.-F.; Lin, Y.-Y.; Zhao, H.-Z.; Lin, Y.-T.; Wang, Y.-L. Optimal modes of mind-body exercise for treating chronic non-specific low back pain: Systematic review and network meta-analysis. Front. Neurosci. 2022, 16, 1046518. [Google Scholar] [CrossRef]
- Essman, M.; Lin, C.Y. The Role of Exercise in Treating Low Back Pain. Curr. Sports Med. Rep. 2022, 21, 267–271. [Google Scholar] [CrossRef] [PubMed]
- Ho, E.K.-Y.; Chen, L.; Simic, M.; Ashton-James, C.E.; Comachio, J.; Wang, D.X.M.; Hayden, J.A.; Ferreira, M.L.; Ferreira, P.H. Psychological interventions for chronic, non-specific low back pain: Systematic review with network meta-analysis. BMJ Open 2020, 10, e034996. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Zhang, H.; Lv, C.; Tang, L.; Tian, S. Comparative efficacy of 12 non-drug interventions on non-specific chronic low back pain in nurses: A systematic review and network meta-analysis. J. Back Musculoskelet. Rehabil. 2021, 34, 499–510. [Google Scholar] [CrossRef] [PubMed]
- Huang, R.; Ning, J.; Chuter, V.H.; Taylor, J.B.; Christophe, D.; Meng, Z.; Xu, Y.; Jiang, L. Exercise alone and exercise combined with education both prevent episodes of low back pain and related absenteeism: Systematic review and network meta-analysis of randomised controlled trials (RCTs) aiMed. at preventing back pain. Br. J. Sports Med. 2020, 54, 766–770. [Google Scholar] [CrossRef] [PubMed]
- Lancet, T. Rethinking chronic pain. Lancet 2021, 397, 2023. [Google Scholar] [CrossRef]
- Booth, J.; Moseley, G.L.; Schiltenwolf, M.; Cashin, A.; Davies, M.; Hübscher, M. Exercise for chronic musculoskeletal pain: A biopsychosocial approach. Musculoskelet. Care 2017, 15, 413–421. [Google Scholar] [CrossRef]
- Heuvel, C.v.D.; van der Horst, J.; Winkelhorst, E.; Roelofsen, E.; Hutting, N. Experiences, barriers and needs of physiotherapists with regard to providing self-management support to people with low back pain: A qualitative study. Musculoskelet. Sci. Pract. 2021, 56, 102462. [Google Scholar] [CrossRef] [PubMed]
- Briggs, A.M.; E Jordan, J.; O’Sullivan, P.B.; Buchbinder, R.; Burnett, A.F.; Osborne, R.H.; Straker, L.M. Individuals with chronic low back pain have greater difficulty in engaging in positive lifestyle behaviours than those without back pain: An assessment of health literacy. BMC Musculoskelet. Disord. 2011, 12, 161. [Google Scholar] [CrossRef] [PubMed]
- Fillingim, R.B.; King, C.D.; Ribeiro-Dasilva, M.C.; Rahim-Williams, B.; Riley, J.L., III. Sex, Gender, and Pain: A Review of Recent Clinical and Experimental Findings. J. Pain 2009, 10, 447–485. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}


| Author and Year | D1 | D2 | D3 | D4 | D5 | D6 | D7 | Overall Risk of Bias |
|---|---|---|---|---|---|---|---|---|
| Baena-Beato et al., 2013 [44] | Serious | Low | Low | Low | Moderate | Low | Low | Serious |
| Ma et al., 2021 [43] | Serious | Low | Serious | No information | No information | No information | Moderate | No information |
| Sofi et al., 2011 [42] | Moderate | Low | Low | Moderate | Moderate | Serious | Moderate | Serious |
| Author and Year | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | Q12 | Q13 | Q14 | Quality Rating |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Notarnicola et al., 2013 [45] | YES | YES | NR | YES | NO | YES | YES | NO | YES | NO | YES | YES | YES | YES | Fair |
| Pain Intensity Outcome | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CT | ||||||||||||
| −1.38 (−19.34, 16.59) | CTR | |||||||||||
| −0.88 (−28.36, 26.60) | 0.49 (−25.01, 25.99) | FEP | ||||||||||
| −2.78 (−42.83, 37.27) | −1.41 (−40.13, 37.31) | −1.90 (−31.04, 27.24) | AR + FEP | |||||||||
| −1.18 (−34.182, 31.83) | 0.20 (−27.49, 27.89) | −0.29 (−37.93, 37.35) | 1.61 (−45.99, 49.21) | AT | ||||||||
| 0.12 (−28.41, 28.65) | 1.50 (−27.78, 30.77) | 1.00 (−34.58, 36.59) | 2.90 (−43.09, 48.89) | 1.30 (−39.00, 41.59) | FEP + CT | |||||||
| 0.16 (−21.94, 22.27) | 1.54 (−19.95, 23.03) | 1.05 (−29.44, 31.53) | 2.95 (−39.22, 45.11) | 1.34 (−33.71, 36.39) | 0.04 (−25.92, 26.00) | LST | ||||||
| −0.57 (−18.58, 17.45) | 0.81 (−18.79, 20.41) | 0.31 (−28.72, 29.35) | 2.21 (−38.92, 43.35) | 0.61 (−33.32, 34.53) | −0.69 (−29.97, 28.60) | −0.73 (−22.23, 20.77) | CTH | |||||
| −19.42 (−35.96, −2.87) a | −18.04 (−39.64, 3.56) | −18.53 (−48.73, 11.67) | −16.63 (−58.60, 25.33) | −18.24 (−53.36, 16.88) | −19.54 (−50.34, 11.27) | −19.58 (−43.85, 4.69) | −18.85 (−35.52, −2.18) a | IN | ||||
| −1.72 (−15.37, 11.92) | −0.35 (−17.65, 16.95) | −0.84 (−26.34, 24.66) | 1.06 (−37.66, 39.78) | −0.55 (−33.20, 32.10) | −1.84 (−27.80, 24.12) | −1.89 (−21.76, 17.99) | −1.15 (−18.48, 16.17) | 17.69 (−1.17, 36.56) | SC | |||
| −1.65 (−29.14, 25.83) | −0.28 (−25.78, 25.22) | −0.77 (−28.47, 26.93) | 1.13 (−39.07, 41.33) | −0.48 (−38.12, 37.17) | −1.77 (−37.36, 33.81) | −1.82 (−32.30, 28.67) | −1.08 (−30.12, 27.95) | 17.76 (−12.44, 47.97) | 0.07 (−25.44, 25.58) | SC + CT | ||
| 0.62 (−32.38, 33.63) | 2.00 (−25.69, 29.69) | 1.51 (−36.13, 39.15) | 3.41 (−44.19, 51.01) | 1.80 (−25.89, 29.49) | 0.51 (−39.79, 40.80) | 0.46 (−34.59, 35.51) | 1.19 (−32.73, 35.12) | 20.04 (−15.08, 55.16) | 2.35 (−30.30, 35.00) | 2.28 (−35.37, 39.92) | RT | |
| −10.15 (−38.52, 18.21) | −8.78 (−39.29, 21.73) | −9.27 (−46.45, 27.92) | −7.37 (−54.61, 39.87) | −8.98 (−50.18, 32.23) | −10.27 (−47.80, 27.26) | −10.31 (−42.43, 21.80) | −9.58 (−34.97, 15.80) | 9.27 (−16.12, 34.65) | −8.43 (−37.30, 20.44) | −8.50 (−45.69, 28.69) | −10.78 (−51.98, 30.43) | ST |
| Functional disability outcome | ||||||||||||
| CT | ||||||||||||
| −1.52 (−22.28, 19.24) | AR + FEP | |||||||||||
| 16.40 (0.00, 32.80) a | 17.92 (−8.53, 44.37) | AT | ||||||||||
| 0.30 (−11.25, 11.85) | 1.82 (−21.93, 25.57) | −16.10 (−27.74, −4.46) a | CTR | |||||||||
| 32.88 (17.05, 48.72) a | 34.40 (20.98, 47.82) a | 16.48 (−6.32, 39.28) | 32.58 (12.98, 52.18) a | FEP | ||||||||
| −5.14 (−15.83, 5.55) | −3.62 (−24.36, 17.13) | −21.54 (−41.11, −1.96) a | −5.44 (−21.17, 10.30) | −38.02 (−53.84, −22.20) a | CTH | |||||||
| −3.22 (−13.00, 6.56) | −1.70 (−20.01, 16.61) | −19.62 (−38.71, −0.53) a | −3.52 (−18.65, 11.61) | −36.10 (−48.56, −23.64) a | 1.92 (−7.84, 11.67) | IN | ||||||
| 5.69 (−0.91, 12.30) | 7.21 (−13.92, 28.34) | −10.71 (−28.40, 6.97) | 5.39 (−7.91, 18.69) | −27.19 (−43.51, −10.87) a | 10.83 (0.72, 20.94) a | 8.91 (−1.64, 19.46) | SC | |||||
| 4.10 (−12.30, 20.50) | 5.62 (−20.84, 32.08) | −12.30 (−23.88, −0.72) a | 3.80 (−7.85, 15.45) | −28.78 (−51.58, −5.98) a | 9.24 (−10.34, 28.82) | 7.32 (−11.78, 26.42) | −1.59 (−19.28, 16.09) | RT | ||||
| −3.84 (−17.28, 9.59) | −2.32 (−23.74, 19.09) | −20.24 (−41.45, 0.96) | −4.14 (−21.86, 13.57) | −36.72 (−53.41, −20.03) a | 1.29 (−9.80, 12.38) | −0.62 (−11.73, 10.48) | −9.54 (−23.04, 3.97) | −7.94 (−29.15, 13.26) | ST | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herrero, P.; Val, P.; Lapuente-Hernández, D.; Cuenca-Zaldívar, J.N.; Calvo, S.; Gómez-Trullén, E.M. Effects of Lifestyle Interventions on the Improvement of Chronic Non-Specific Low Back Pain: A Systematic Review and Network Meta-Analysis. Healthcare 2024, 12, 505. https://doi.org/10.3390/healthcare12050505
Herrero P, Val P, Lapuente-Hernández D, Cuenca-Zaldívar JN, Calvo S, Gómez-Trullén EM. Effects of Lifestyle Interventions on the Improvement of Chronic Non-Specific Low Back Pain: A Systematic Review and Network Meta-Analysis. Healthcare. 2024; 12(5):505. https://doi.org/10.3390/healthcare12050505
Chicago/Turabian StyleHerrero, Pablo, Paula Val, Diego Lapuente-Hernández, Juan Nicolás Cuenca-Zaldívar, Sandra Calvo, and Eva María Gómez-Trullén. 2024. "Effects of Lifestyle Interventions on the Improvement of Chronic Non-Specific Low Back Pain: A Systematic Review and Network Meta-Analysis" Healthcare 12, no. 5: 505. https://doi.org/10.3390/healthcare12050505
APA StyleHerrero, P., Val, P., Lapuente-Hernández, D., Cuenca-Zaldívar, J. N., Calvo, S., & Gómez-Trullén, E. M. (2024). Effects of Lifestyle Interventions on the Improvement of Chronic Non-Specific Low Back Pain: A Systematic Review and Network Meta-Analysis. Healthcare, 12(5), 505. https://doi.org/10.3390/healthcare12050505