
UK Dietary Policy for the Prevention of Cardiovascular Disease

Abstract
:1. Introduction
2. UK Government Recommendations
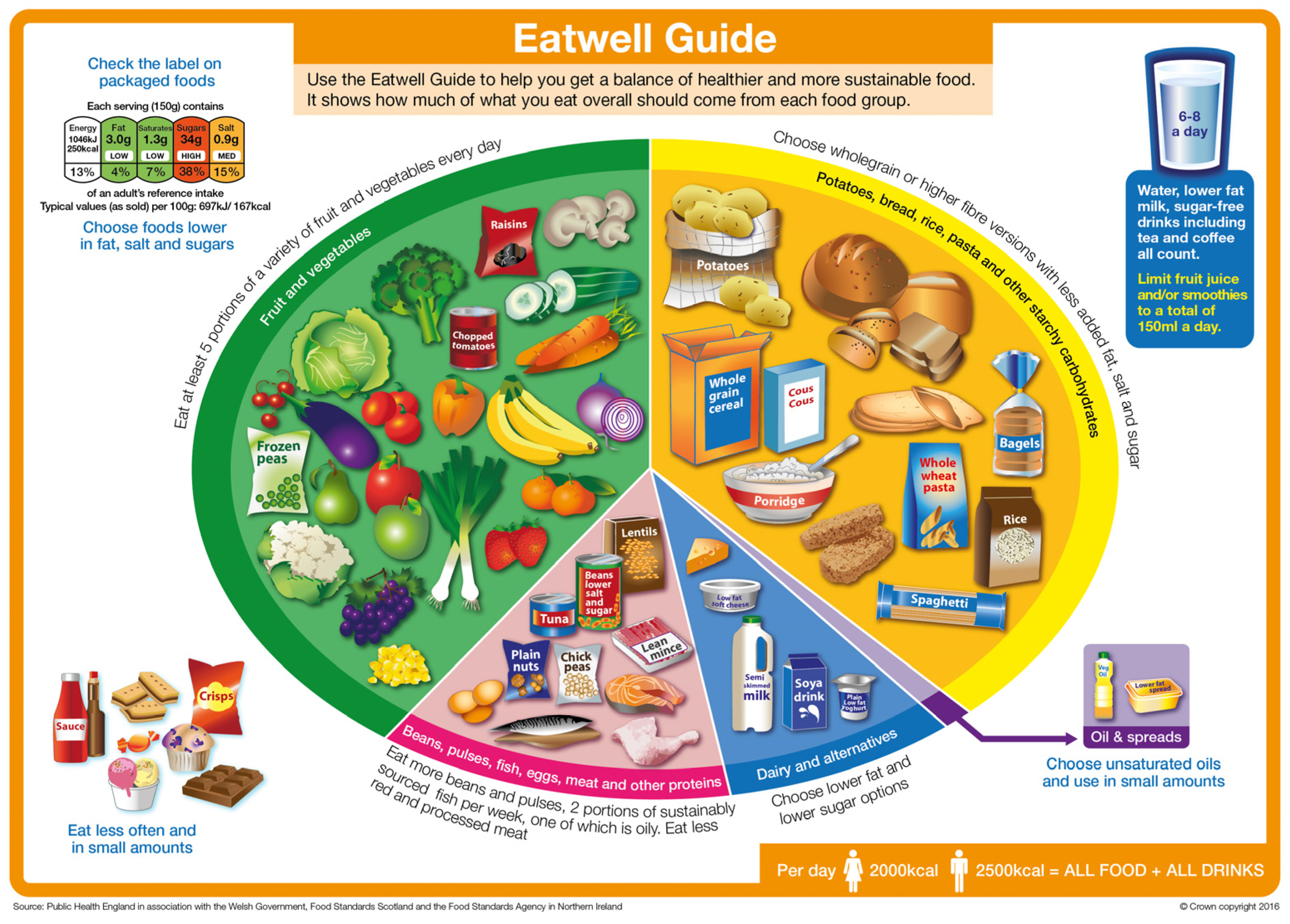
3. Eatwell Guide
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- British Heart Foundation. Cardiovascular Disease Statistics 2016. Available online: http://www.bhf.org.uk/research/heart-statistics (accessed on 2 November 2016).
- British Heart Foundation. Cardiovascular Disease Statistics 2015. Available online: http://www.bhf.org.uk/publications/statistics/cvd-stats-2015 (accessed on 2 November 2016).
- Forouzanfar, M.H.; Alexander, L.; Anderson, H.R.; Bachman, V.F.; Biryukov, S.; Brauer, M.; Burnett, R.; Casey, D.; Coates, M.M.; Cohen, A.; et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990–2013: A systematic analysis for the global burden of disease study 2013. Lancet 2015, 386, 2287–2323. [Google Scholar] [CrossRef]
- Marmot, M.G.; Allen, J.; Goldblatt, P.; Boyce, T.; McNeish, D.; Grady, M.; Geddes, I. Fair Society, Healthy Lives: Strategic Review of Health Inequalities in England Post-2010. Available online: http://www.instituteofhealthequity.org/projects/fair-society-healthy-lives-the-marmot-review (accessed on 2 November 2016).
- Public Health England. Public Health Outcomes Framework. Indicator 4.04i: Age Standardised Rate of Mortality from All Cardiovascular Diseases (Including Heart Disease and Stroke) in Persons Less than 75 Years of Age per 100,000 Population. Available online: http://www.phoutcomes.info/search/cardiovascular%20disease (accessed on 2 November 2016).
- Scientific Advisory Committee on Nutrition. A Framework for Evaluation of Evidence that Relates Food and Nutrients to Health. Available online: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/480493/SACN_Framework_for_the_Evaluation_of_Evidence.pdf (accessed on 2 November 2016).
- Levy, L.B. Dietary strategies, policy and cardiovascular disease risk reduction in England. Proc. Nutr. Soc. 2013, 72, 386–389. [Google Scholar] [CrossRef] [PubMed]
- Committee on Medical Aspects of Food Policy. Nutritional Aspects of Cardiovascular Disease; HMSO: London, UK, 1994. [Google Scholar]
- Shaw, D.I.; Thompson, A.K.; Minihane, A.M.; Williams, C.M. Update on Trans Fatty Acids and Health: Position Statement the Scientific Advisory Committee on Nutrition. Available online: https://ueaeprints.uea.ac.uk/36650/ (accessed on 2 November 2016).
- Scientific Advisory Committee on Nutrition. Salt and Health. Available online: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/338782/SACN_Salt_and_Health_report.pdf (accessed on 2 November 2016).
- Scientific Advisory Committee on Nutrition/Committee on Toxicity. Advice on Fish Consumption: Benefits & Risks. Available online: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/338801/SACN_Advice_on_Fish_Consumption.pdf (accessed on 2 November 2016).
- World Health Organization. Diet, Nutrition, and the Prevention of Chronic Diseases; World Health Organization: Geneva, Switzerland, 1990. [Google Scholar]
- Scientific Advisory Committee on Nutrition. Carbohydrates and Health. Available online: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/445503/SACN_Carbohydrates_and_Health.pdf (accessed on 2 November 2016).
- Bates, B.; Cox, L.; Nicholson, S.; Page, P.; Prentice, A.; Steer, T.; Swan, G. National Diet and Nutrition Survey: Results from Years 5 and 6 (Combined) of the Rolling Programme (2012/2013–2013/2014); Public Health England: London, UK, 2016.
- Bates, B.; Cox, L.; Maplethorpe, N.; Mazumder, A.; Nicholson, S.; Page, P.; Prentice, A.; Rooney, K.; Ziauddeen, N.; Swan, G. National Diet and Nutrition Survey: Assessment of Dietary Sodium Adults (19 to 64 Years) in England, 2011. Available online: https://www.gov.uk/government/publications/assessment-of-dietary-sodium-levels-among-adults-aged-19-64-in-england-2011 (accessed on 2 November 2016).
- Craig, R.; Fuller, E.; Mindell, J. Health Survey for England 2014. Available online: http://content.digital.nhs.uk/catalogue/PUB19295/HSE2014-Ch1-Intro.pdf (accessed on 2 November 2016).
- Department of Health. Salt Reduction—Onward and Downwards. Available online: https://responsibilitydeal.dh.gov.uk/salt-reduction-onwards-and-downwards/ (accessed on 2 November 2016).
- Bates, B.; Lennox, A.; Prentice, A.; Bates, C.; Swan, G. National Diet and Nutrition Survey: Headline Results from Years 1, 2 and 3 (Combined) of the Rolling Programme (2008/2009–2010/11). Available online: http://transparency.dh.gov.uk/2012/07/25/ndns-3-years-report/ (accessed on 2 November 2016).
- Department of Health. New Saturated Fat Pledge. Available online: https://responsibilitydeal.dh.gov.uk/new-saturated-fat-pledge/ (accessed on 2 November 2016).
- Chowdhury, R.; Warnakula, S.; Kunutsor, S.; Crowe, F.; Ward, H.A.; Johnson, L.; Franco, O.H.; Butterworth, A.S.; Forouhi, N.G.; Thompson, S.G.; et al. Association of dietary, circulating, and supplement fatty acids with coronary risk: A systematic review and meta-analysis. Ann. Intern. Med. 2014, 160, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Harcombe, Z.; Baker, J.S.; Cooper, S.M.; Davies, B.; Sculthorpe, N.; DiNicolantonio, J.J.; Grace, F. Evidence from randomised controlled trials did not support the introduction of dietary fat guidelines in 1977 and 1983: A systematic review and meta-analysis. Open Heart 2015, 2, e000196. [Google Scholar] [CrossRef] [PubMed]
- Crowe, F.L.; Roddam, A.W.; Key, T.J.; Appleby, P.N.; Overvad, K.; Jakobsen, M.U.; Tjønneland, A.; Hansen, L.; Boeing, H.; Weikert, C.; et al. Fruit and vegetable intake and mortality from ischaemic heart disease: Results from the European Prospective Investigation into Cancer and Nutrition (EPIC)-Heart study. Eur. Heart J. 2011, 32, 1235–1243. [Google Scholar] [CrossRef] [PubMed]
- Public Health England. Government Recommendations for Food Energy and Nutrients for Males and Females Aged 1–18 Years and 19+ Years. Available online: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/547050/government__dietary_recommendations.pdf (accessed on 2 November 2016).
- Hunt, P.; Rayner, M.; Gatenby, S. A national food guide for the UK? Background and development. J. Hum. Nutr. Diet. 1995, 8, 315–322. [Google Scholar] [CrossRef]
- Gatenby, S.; Hunt, P.; Rayner, M. The national food guide: Development of dietetic criteria and nutritional characteristics. J. Hum. Nutr. Diet. 1995, 8, 323–334. [Google Scholar] [CrossRef]
- Hunt, P.; Gatenby, S.; Rayner, M. The format for the national food guide: Performance and preference studies. J. Hum. Nutr. Diet. 1995, 8, 335–351. [Google Scholar] [CrossRef]
- Food Standards Agency. The Answer to Healthy Eating—On a Plate. Available online: http://tna.europarchive.org/20120209120540/http://www.food.gov.uk/news/newsarchive/2007/sep/plate (accessed on 2 November 2016).
- Public Health England. The Eatwell Plate: External Reference Group Review. Available online: https://www.gov.uk/government/publications/the-Eatwell-plate-external-reference-group-review (accessed on 2 November 2016).
- Public Health England. From Plate to Guide: What, Why and How for the Eatwell Model. Available online: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/579388/Eatwell_model_guide_report.pdf (accessed on 23 January 2017).
- Cobiac, L.J.; Scarborough, P.; Kaur, A.; Rayner, M. The Eatwell guide: Modelling the health implications of incorporating new sugar and fibre guidelines. PLoS ONE 2016, 11, e0167859. [Google Scholar] [CrossRef] [PubMed]
- Public Health England. Composition of Foods Integrated Dataset (CoFID). Available online: https://www.gov.uk/government/publications/composition-of-foods-integrated-dataset-cofid (accessed on 2 November 2016).
- Public Health England. Sugar Reduction the Evidence for Action. Available online: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/470179/Sugar_reduction_The_evidence_for_action.pdf (accessed on 2 November 2016).
- Department of Health. Childhood Obesity: A Plan for Action. Available online: https://www.gov.uk/government/publications/childhood-obesity-a-plan-for-action (accessed on 2 November 2016).
- Public Health England. Action on Cardiovascular Disease: Getting Serious on Prevention. Available online: https://www.gov.uk/government/publications/cardiovascular-disease-getting-serious-about-prevention (accessed on 23 January 2017).


{kind=link}
| Dietary Recommendation | |
|---|---|
| Nutrients | |
| Energy | 2000 kcal (8.4 MJ) for women; 2500 kcal (10.4 MJ) for men |
| Carbohydrates | ≥50% of total energy |
| Free Sugars | ≤5% food energy |
| Fat | ≤35% food energy |
| Saturated Fat | ≤11% food energy |
| Salt | ≤6 g/2363 mg sodium |
| Fibre (AOAC) | 30 g |
| Foods | |
| Fruits and Vegetables | At least 5 portions of a variety each day |
| Fish | At least 2 portions a week, one of which should be oily |
| Dietary Recommendation | Constraint Factors Used in Linear Programming Model (Exclusing Alcohol) | |
|---|---|---|
| Nutrients | ||
| Energy | 2250 kcal (9414 MJ) 1 | No increase 4 |
| Carbohydrates | ≥50% of total energy | ≥50% of food energy |
| Free sugars | ≤5% food energy | ≤5% food energy |
| Fat | ≤35% food energy | ≤35% food energy |
| Saturated fat | ≤11% food energy | ≤11% food energy |
| Protein | Approx. 15% food energy | ≥14.5 & ≤15.5% of energy |
| Salt | ≤6 g/2363 mg sodium | ≤6 g/2363 mg sodium |
| Fibre (AOAC) 2 | 30 g | ≥30 g |
| Foods | ||
| Fruits and vegetables 3 | At least 5 portions of a variety each day | ≥5 portions a day |
| Fish | At least 2 portions a week, one of which should be oily | ≥2 portions (2 × 140 g) a week, one of which should be oily |
| Red and processed meat | High consumers should reduce their intake to the average of the population (70 g) | ≤70 g/day |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Levy, L.; Tedstone, A. UK Dietary Policy for the Prevention of Cardiovascular Disease. Healthcare 2017, 5, 9. https://doi.org/10.3390/healthcare5010009
Levy L, Tedstone A. UK Dietary Policy for the Prevention of Cardiovascular Disease. Healthcare. 2017; 5(1):9. https://doi.org/10.3390/healthcare5010009
Chicago/Turabian StyleLevy, Louis, and Alison Tedstone. 2017. "UK Dietary Policy for the Prevention of Cardiovascular Disease" Healthcare 5, no. 1: 9. https://doi.org/10.3390/healthcare5010009
APA StyleLevy, L., & Tedstone, A. (2017). UK Dietary Policy for the Prevention of Cardiovascular Disease. Healthcare, 5(1), 9. https://doi.org/10.3390/healthcare5010009