
More than Ninety Percent of the Light Energy Emitted by Near-Infrared Laser Therapy Devices Used to Treat Musculoskeletal Disorders Is Absorbed within the First Ten Millimeters of Biological Tissue
Abstract
:1. Introduction
2. Materials and Methods
2.1. Biological Tissue Specimens
2.2. Instruments and Procedures
2.3. Penetration Depth Analysis
3. Results
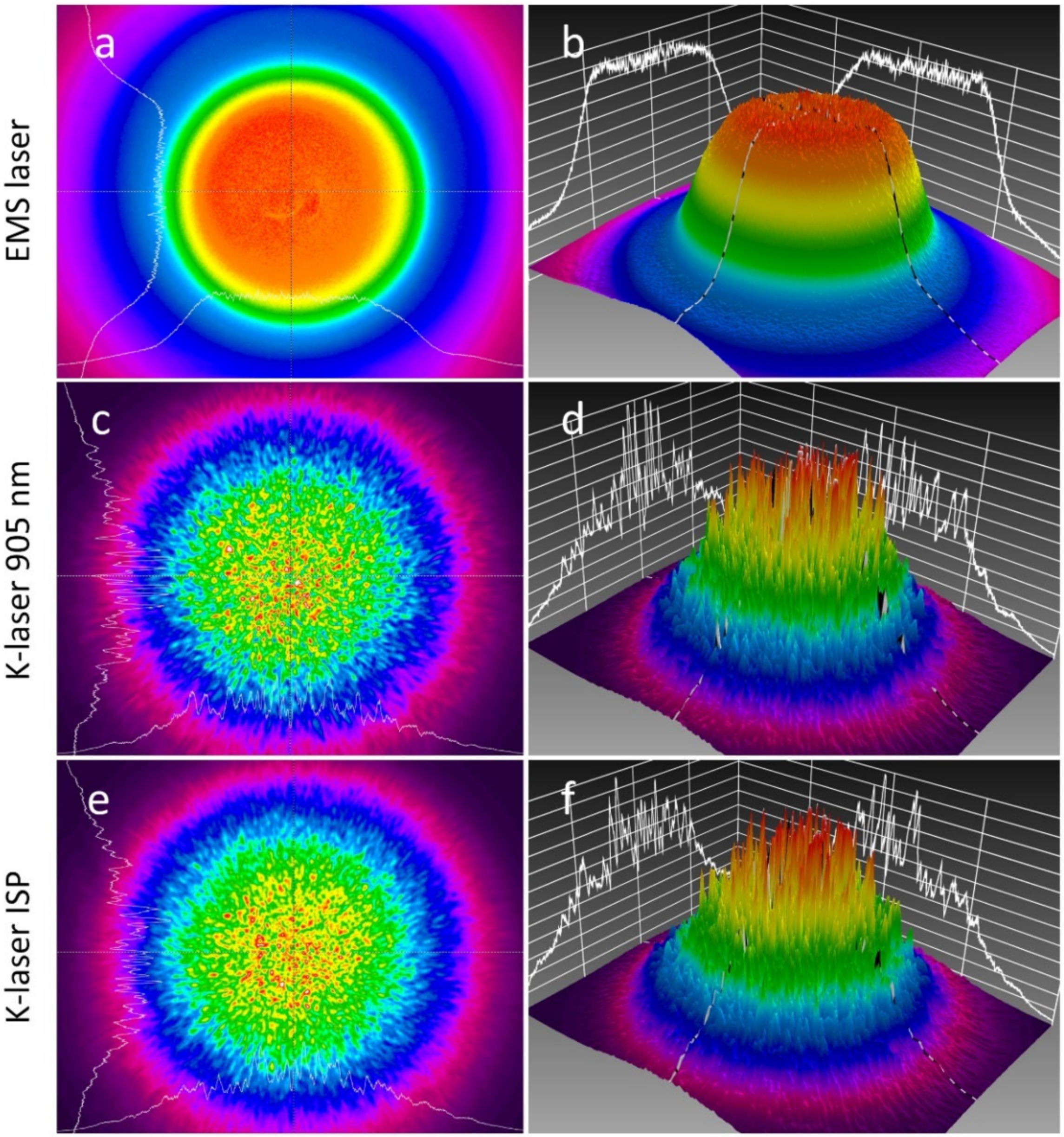
3.1. Laser Beam Characterization
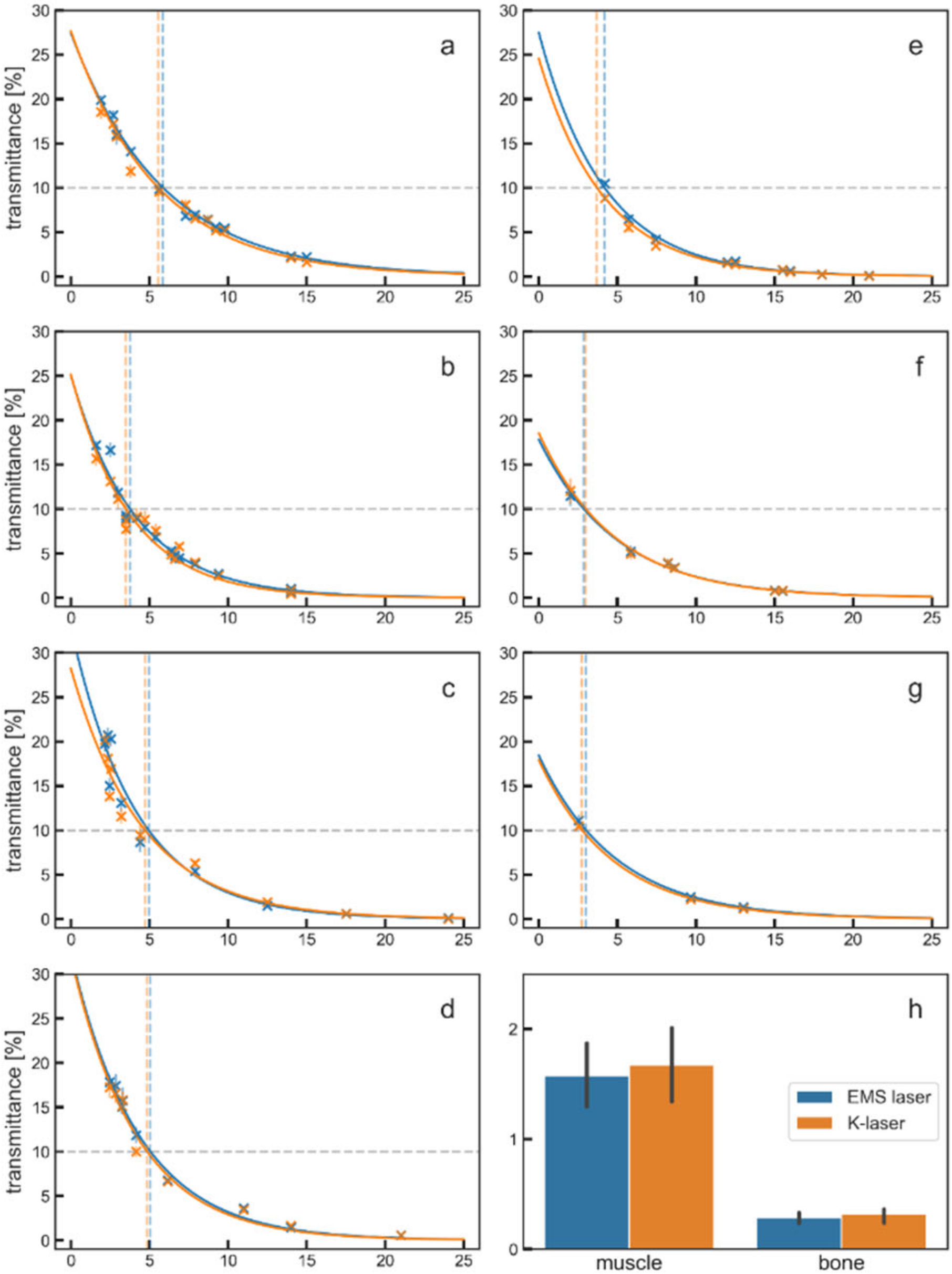
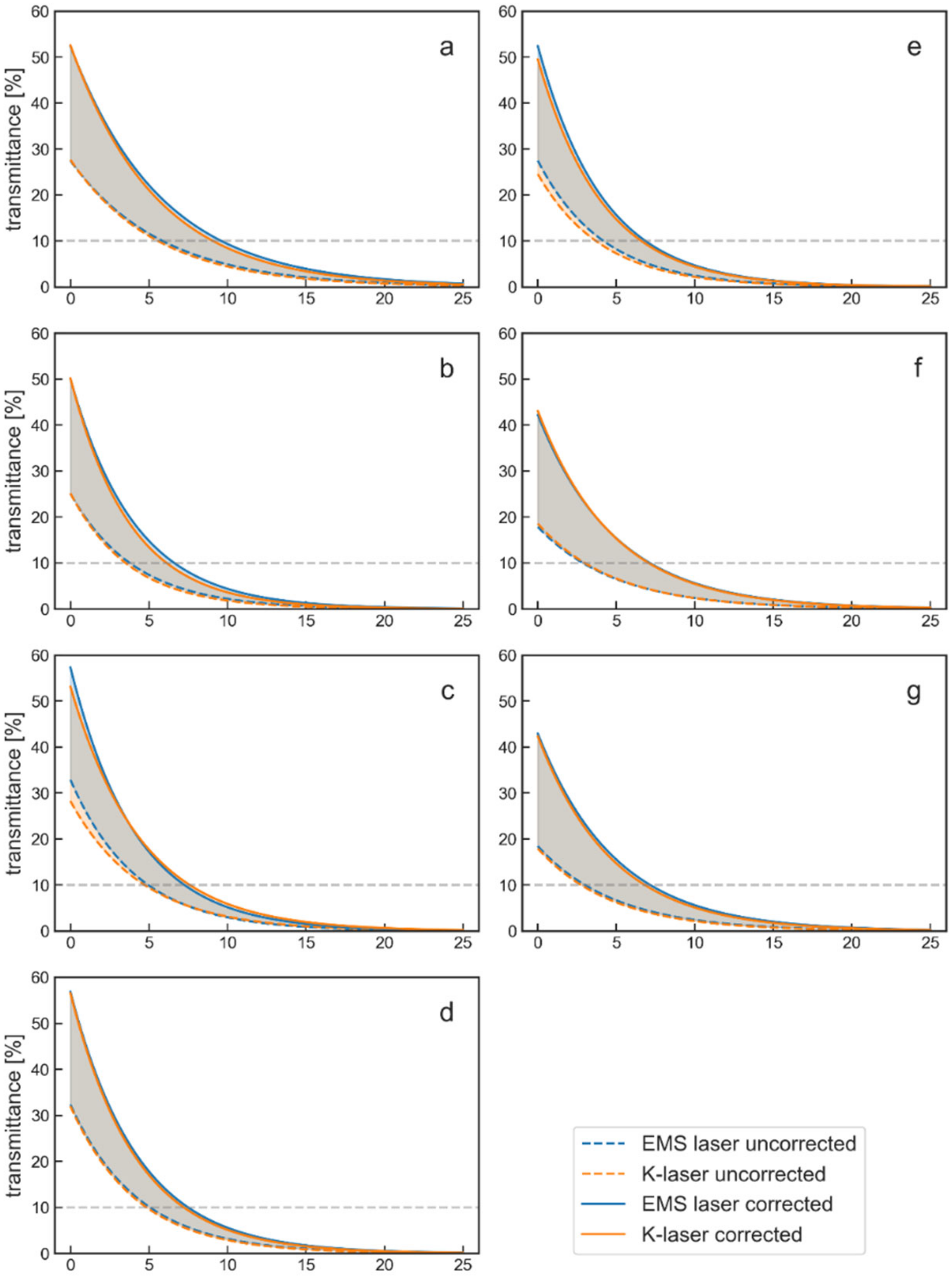
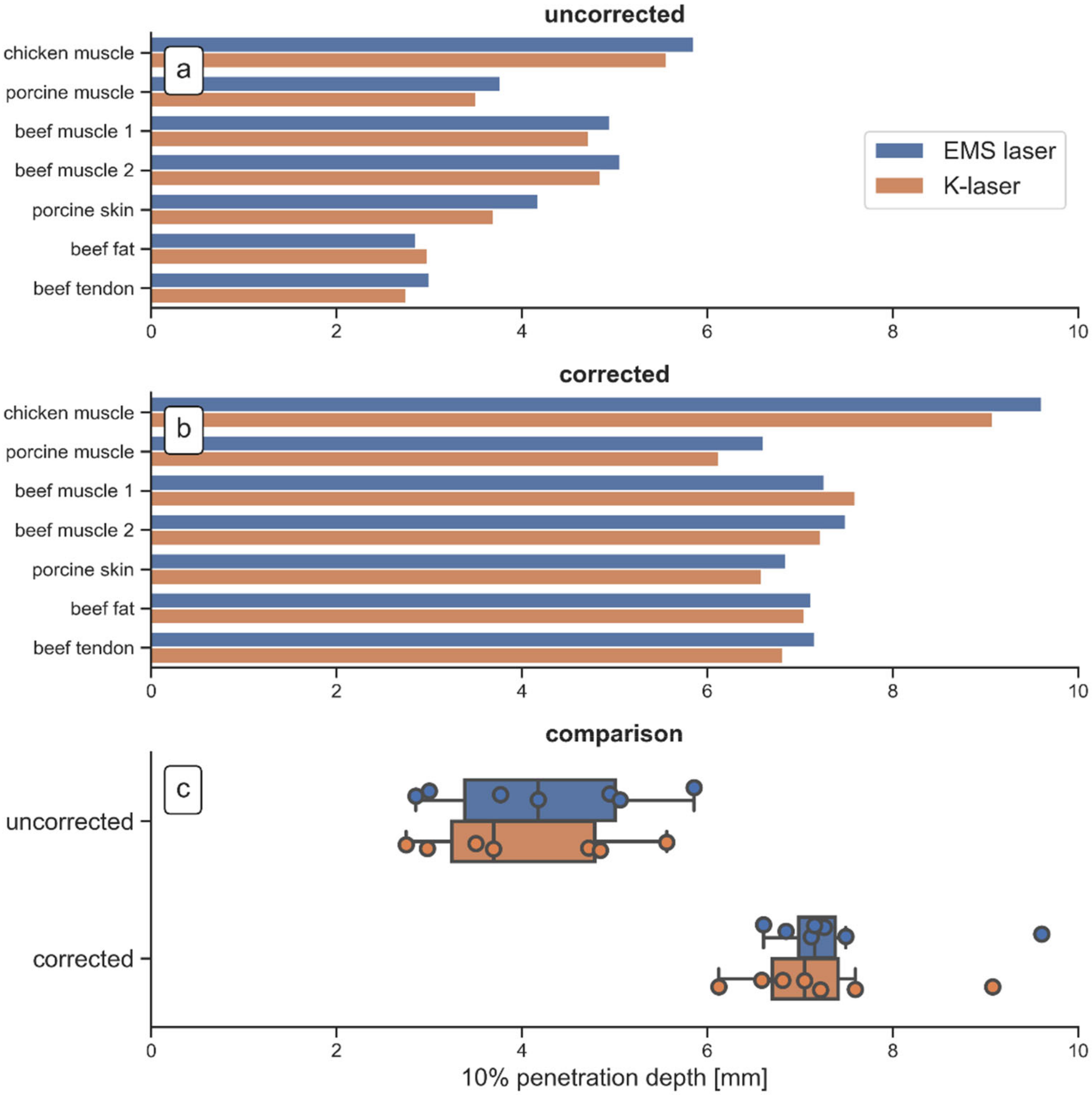
3.2. Penetration Depth of 905 nm Laser Light in Tissue
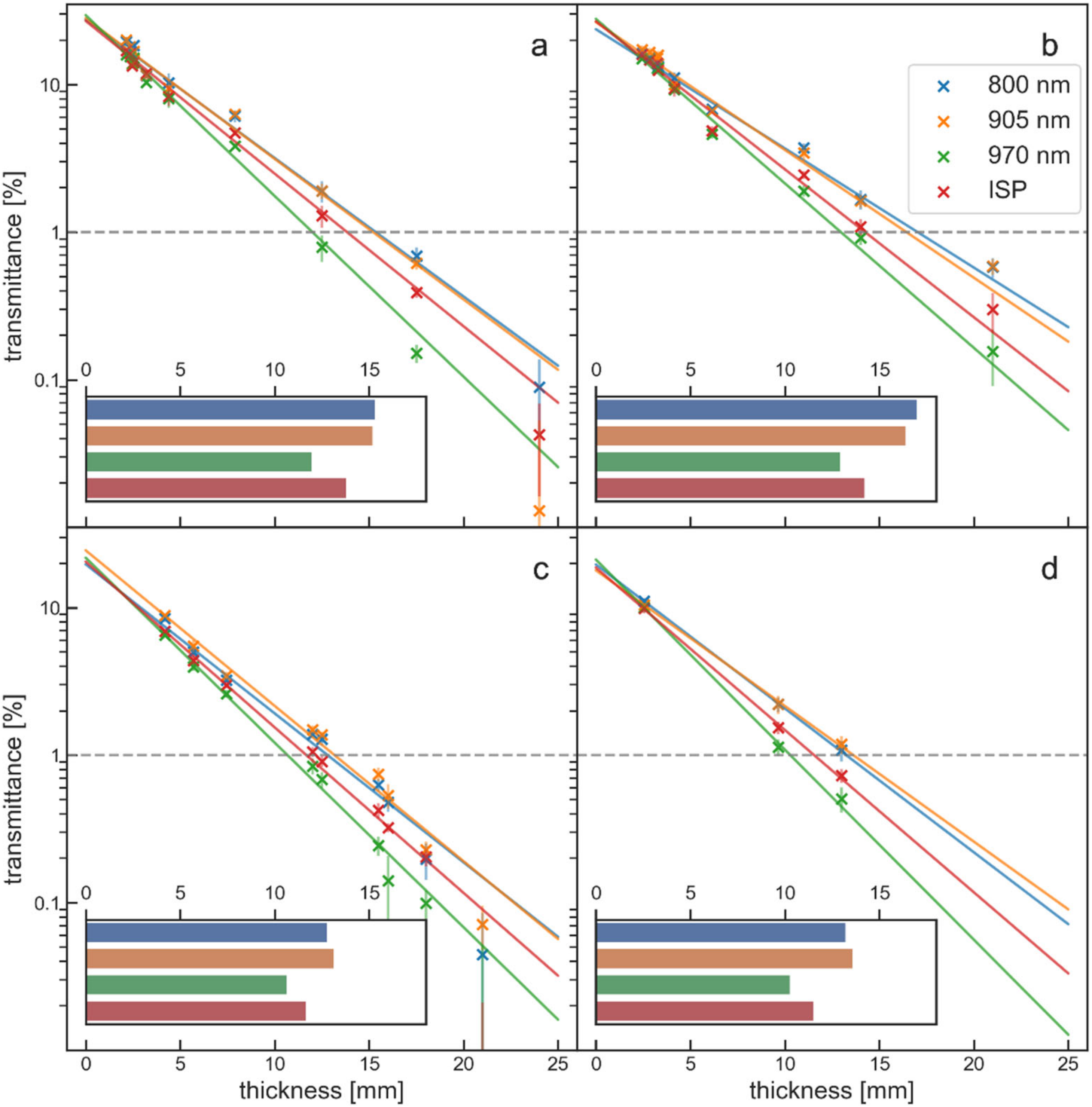
3.3. Effect of Wavelength on Penetration Depth
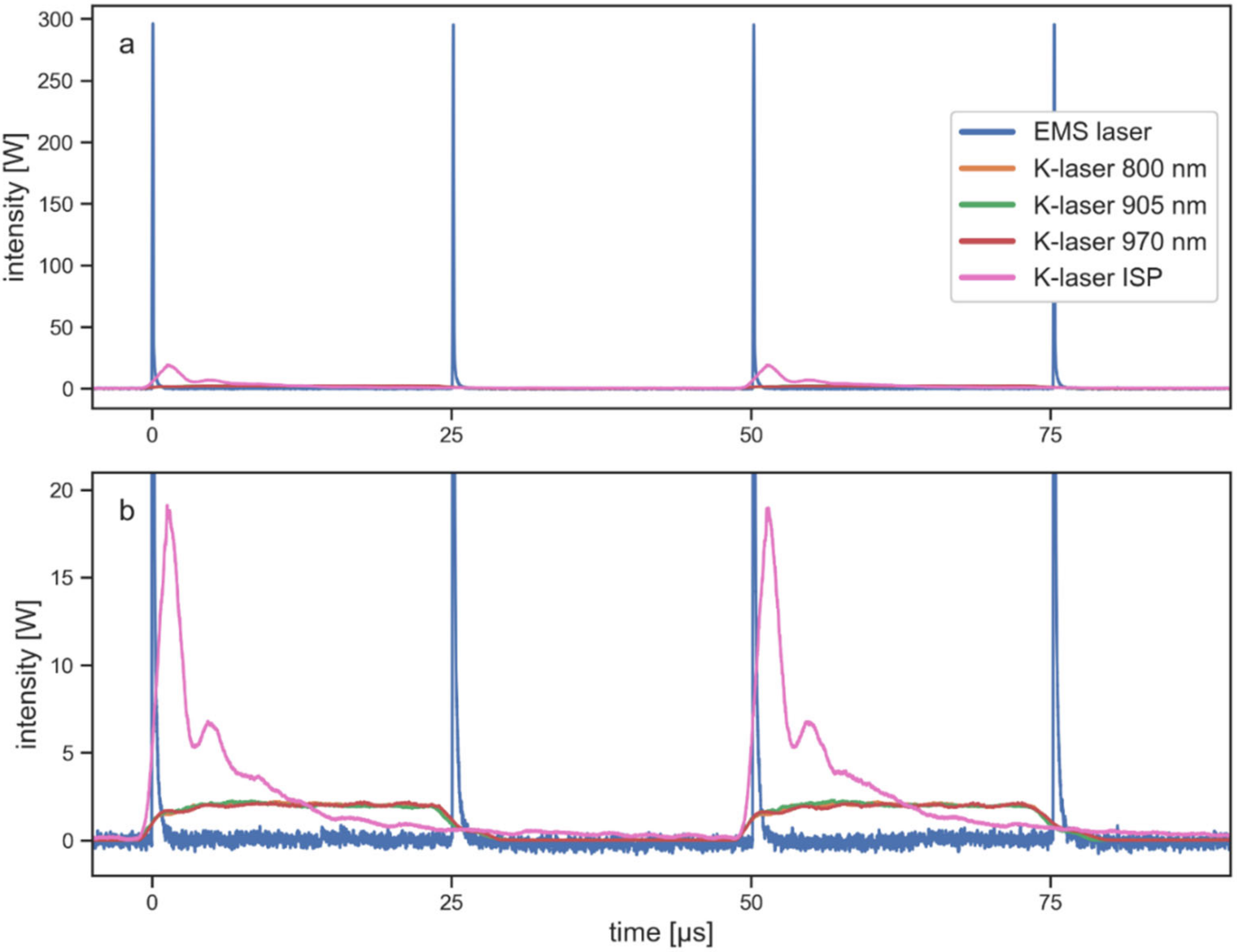
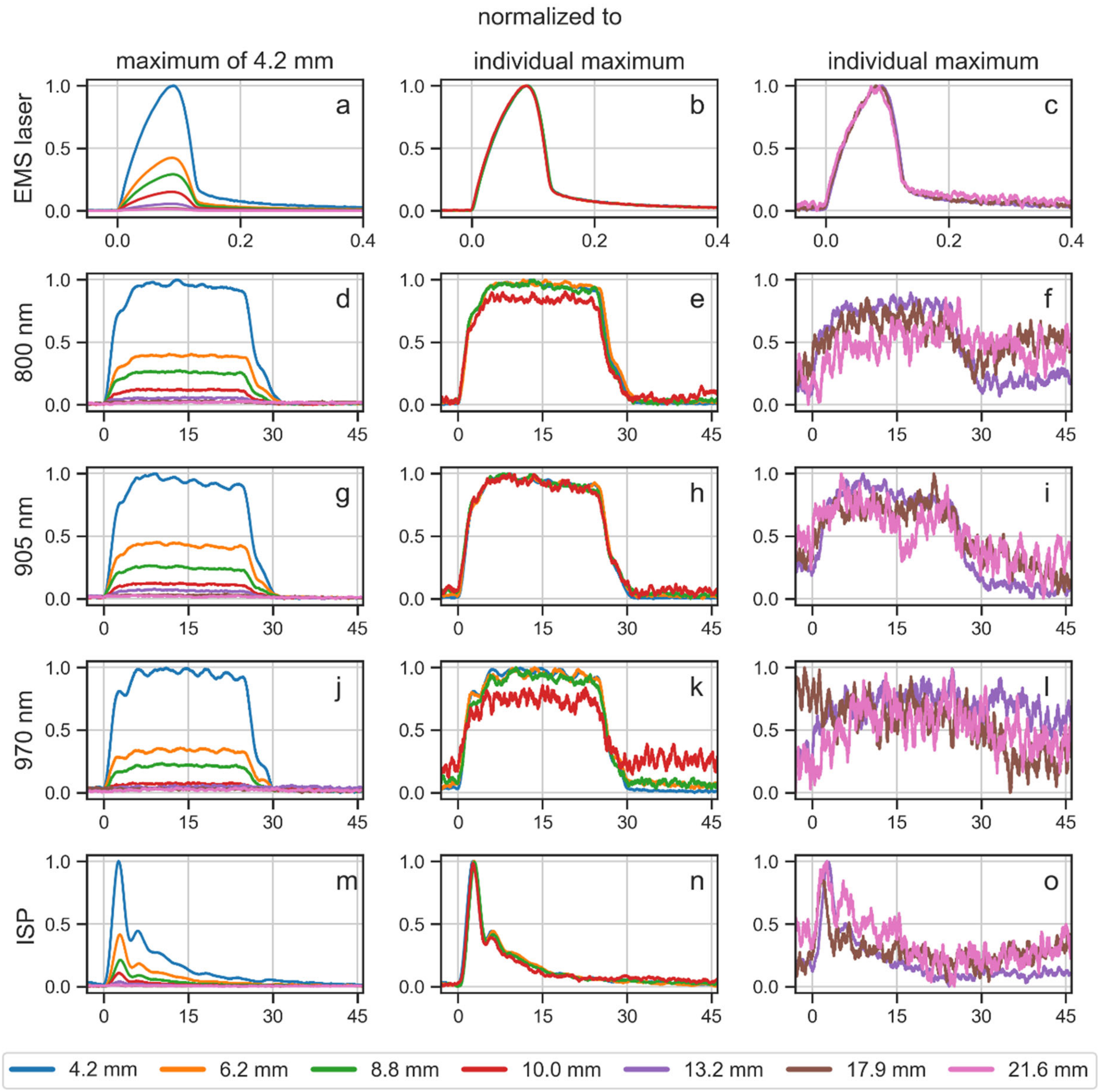
3.4. Laser Pulses Transmitted through Tissue
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Naterstad, I.F.; Joensen, J.; Bjordal, J.M.; Couppé, C.; Lopes-Martins, R.A.B.; Stausholm, M.B. Efficacy of low-level laser therapy in patients with lower extremity tendinopathy or plantar fasciitis: Systematic review and meta-analysis of randomised controlled trials. BMJ Open 2022, 12, e059479. [Google Scholar] [CrossRef]
- Mussttaf, R.A.; Jenkins, D.F.L.; Jha, A.N. Assessing the impact of low level laser therapy (LLLT) on biological systems: A review. Int. J. Radiat. Biol. 2019, 95, 120–143. [Google Scholar] [PubMed]
- Bjordal, J.M.; Lopes-Martins, R.A.B.; Joensen, J.; Iversen, V.V. The anti-inflammatory mechanism of low level laser therapy and its relevance for clinical use in physiotherapy. Phys. Ther. Rev. 2010, 15, 286–293. [Google Scholar]
- Dompe, C.; Moncrieff, L.; Matys, J.; Grzech-Leśniak, K.; Kocherova, I.; Bryja, A.; Bruska, M.; Dominiak, M.; Mozdziak, P.; Skiba, T.H.I.; et al. Photobiomodulation-underlying mechanism and clinical applications. J. Clin. Med. 2020, 9, 1724. [Google Scholar]
- Chung, H.; Dai, T.; Sharma, S.K.; Huang, Y.-Y.; Carroll, J.D.; Hamblin, M.R. The nuts and bolts of low-level laser (light) therapy. Ann. Biomed. Eng. 2012, 40, 516–533. [Google Scholar] [CrossRef] [Green Version]
- Schmitz, C. Improving extracorporeal shock wave therapy with 904 or 905 nm pulsed, high power laser pretreatment. Preprints 2021, 2021010138. [Google Scholar] [CrossRef]
- De Freitas, L.F.; Hamblin, M.R. Proposed mechanisms of photobiomodulation or low-level light therapy. IEEE J. Sel. Top. Quantum Electron. 2016, 22, 7000417. [Google Scholar] [CrossRef] [Green Version]
- Moriyama, Y.; Nguyen, J.; Akens, M.; Moriyama, E.H.; Lilge, L. In vivo effects of low level laser therapy on inducible nitric oxide synthase. Lasers Surg. Med. 2009, 41, 227–231. [Google Scholar] [PubMed]
- Mezawa, S.; Iwata, K.; Naito, K.; Kamogawa, H. The possible analgesic effect of soft-laser irradiation on heat nociceptors in the cat tongue. Arch. Oral Biol. 1988, 33, 693–694. [Google Scholar] [PubMed]
- Bjordal, J.M.; Lopes-Martins, R.Á.B.; Iversen, V.V. A randomised, placebo controlled trial of low level laser therapy for activated Achilles tendinitis with microdialysis measurement of peritendinous prostaglandin E2 concentrations. Br. J. Sports Med. 2006, 40, 76–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Momin, A.; McNaughton, P.A. Regulation of firing frequency in nociceptive neurons by pro-inflammatory mediators. Exp. Brain Res. 2009, 196, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, C.; Császár, N.B.M.; Milz, S.; Schieker, M.; Maffulli, N.; Rompe, J.-D.; Furia, J.P. Efficacy and safety of extracorporeal shock wave therapy for orthopedic conditions: A systematic review on studies listed in the PEDro database. Br. Med. Bull. 2015, 116, 115–138. [Google Scholar] [CrossRef]
- Wuerfel, T.; Schmitz, C.; Jokinen, L.L.J. The effects of the exposure of musculoskeletal tissue to extracorporeal shock waves. Biomedicines 2022, 10, 1084. [Google Scholar] [CrossRef] [PubMed]
- Maier, M.; Averbeck, B.; Milz, S.; Refior, H.J.; Schmitz, C. Substance P and prostaglandin E2 release after shock wave application to the rabbit femur. Clin. Orthop. Relat. Res. 2003, 406, 237–245. [Google Scholar] [CrossRef]
- Gerdesmeyer, L.; Wagenpfeil, S.; Haake, M.; Maier, M.; Loew, M.; Wörtler, K.; Lampe, R.; Seil, R.; Handle, G.; Gassel, S.; et al. Extracorporeal shock wave therapy for the treatment of chronic calcifying tendonitis of the rotator cuff: A randomized controlled trial. JAMA 2003, 290, 2573–2580. [Google Scholar] [CrossRef]
- Zhang, Y.; Liu, Y.; Chou, S.; Weng, H. Dose-related effects of radial extracorporeal shock wave therapy for knee osteoarthritis: A randomized controlled trial. J. Rehabil. Med. 2021, 53, jrm00144. [Google Scholar] [PubMed]
- Klonschinski, T.; Ament, S.J.; Schlereth, T.; Rompe, J.D.; Birklein, F. Application of local anesthesia inhibits effects of low-energy extracorporeal shock wave treatment (ESWT) on nociceptors. Pain Med. 2011, 12, 1532–1537. [Google Scholar] [CrossRef]
- Rompe, J.D.; Meurer, A.; Nafe, B.; Hofmann, A.; Gerdesmeyer, L. Repetitive low-energy shock wave application without local anesthesia is more efficient than repetitive low-energy shock wave application with local anesthesia in the treatment of chronic plantar fasciitis. J. Orthop. Res. 2005, 23, 931–941. [Google Scholar] [PubMed]
- Zhao, Z.; Fairchild, P.W. Dependence of light transmission through human skin on incident beam diameter at different wavelengths. In Laser-Tissue Interaction IX, Proceedings of the SPIE 3254, BiOS ’98 International Biomedical Optics Symposium, San Jose, CA, USA, 13 May 1998; SPIE: Manchester, UK, 1998. [Google Scholar] [CrossRef]
- Ash, C.; Dubec, M.; Donne, K.; Bashford, T. Effect of wavelength and beam width on penetration in light-tissue interaction using computational methods. Lasers Med. Sci. 2017, 32, 1909–1918. [Google Scholar] [CrossRef]
- Liebert, A.; Waddington, G.; Bicknell, B.; Chow, R.; Adams, R. Quantification of the absorption of low-level 904 nm superpulsed laser, light as a function of skin colour. In Proceedings of the 9th WALT Congress, Surfers Paradise, Australia, 28–30 September 2012; Laakso, E.L., Young, C., Eds.; Medimond: Gold Coast, Australia, 2012; pp. 11–15. [Google Scholar]
- Hashmi, J.T.; Huang, Y.-Y.; Sharma, S.K.; Kurup, D.B.; Taboada, L.d.; Carroll, J.D.; Hamblin, M.R. Effect of pulsing in low-level light therapy. Lasers Surg. Med. 2010, 42, 450–466. [Google Scholar] [CrossRef] [Green Version]
- Hudson, D.E.; Hudson, D.O.; Wininger, J.M.; Richardson, B.D. Penetration of laser light at 808 and 980 nm in bovine tissue samples. Photomed. Laser Surg. 2013, 31, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Han, D.; Xu, J.; Wang, Z.; Yang, N.; Li, X.; Qian, Y.; Li, G.; Dai, R.; Xu, S. Penetrating effect of high-intensity infrared laser pulses through body tissue. RSC Adv. 2018, 8, 32344–32357. [Google Scholar] [PubMed]
- Barbosa, R.I.; Guirro, E.C.d.O.; Bachmann, L.; Brandino, H.E.; Guirro, R.R.J. Analysis of low-level laser transmission at wavelengths 660, 830 and 904 nm in biological tissue samples. J. Photochem. Photobiol. B 2020, 209, 111914. [Google Scholar] [CrossRef] [PubMed]
- Barbora, A.; Bohar, O.; Sivan, A.A.; Magory, E.; Nause, A.; Minnes, R. Higher pulse frequency of near-infrared laser irradiation increases penetration depth for novel biomedical applications. PLoS ONE 2021, 16, e0245350. [Google Scholar] [CrossRef]
- Arslan, H.; Doluğan, Y.B. Optical penetration depths and fluence distributions in chicken breast and liver tissues. Opt. Spectrosc. 2019, 127, 763–768. [Google Scholar] [CrossRef]
- ISO 13694:2018; Optics and Photonics—Lasers and Laser-Related Equipment—Test Methods for Laser Beam Power (Energy) Density Distribution. International Organization for Standardization: Geneva, Switzerland, 2018. Available online: https://www.iso.org/standard/72945.html (accessed on 9 November 2022).
- Oshina, I.; Spigulis, J. Beer–Lambert law for optical tissue diagnostics: Current state of the art and the main limitations. J. Biomed. Opt. 2021, 26, 100901. [Google Scholar] [CrossRef]
- Stolik, S.; Delgado, J.A.; Perez, A.; Anasagasti, L. Measurement of the penetration depths of red and near infrared light in human “ex vivo” tissues. J. Photochem. Photobiol. B 2000, 57, 90–93. [Google Scholar]
- Bashkatov, A.N.; Genina, E.A.; Kochubey, V.I.; Tuchin, V.V. Optical properties of human skin, subcutaneous and mucous tissues in the wavelength range from 400 to 2000 nm. J. Phys. D App. Phys. 2005, 38, 2543. [Google Scholar] [CrossRef]
- Kolari, P.J.; Airaksinen, O. Poor penetration of infra-red and helium neon low power laser light into the dermal tissue. Acupunct. Electrother. Res. 1993, 18, 17–21. [Google Scholar] [CrossRef]
- Ritz, J.P.; Roggan, A.; Isbert, C.; Müller, G.; Buhr, H.J.; Germer, C.T. Optical properties of native and coagulated porcine liver tissue between 400 and 2400 nm. Lasers Surg. Med. 2001, 29, 205–212. [Google Scholar]
- Nussbaum, E.L.; van Zuylen, J.; Jing, F. Transmission of light through human skin folds during phototherapy: Effects of physical characteristics, irradiation wavelength, and skin-diode coupling. Physiother. Can. 2007, 59, 194–207. [Google Scholar] [CrossRef]
- Zhang, Z.; Monteiro-Riviere, N.A. Comparison of integrins in human skin, pig skin, and perfused skin: An in vitro skin toxicology model. J. Appl. Toxicol. 1997, 17, 247–253. [Google Scholar] [CrossRef]
- Arslan, H.; Doluğan, Y.B.; Ay, A.N. Measurement of the penetration depth in biological tissue for different optical powers. Sakarya Univ. J. Sci. 2018, 22, 1095–1100. [Google Scholar] [CrossRef]
- Ilic, S.; Leichliter, S.; Streeter, J.; Oron, A.; DeTaboada, L.; Oron, U. Effects of power densities, continuous and pulse frequencies, and number of sessions of low-level laser therapy on intact rat brain. Photomed. Laser Surg. 2006, 24, 458–466. [Google Scholar]
- Joensen, J.; Ovsthus, K.; Reed, R.K.; Hummelsund, S.; Iversen, V.V.; Lopes-Martins, R.Á.B.; Bjordal, J.M. Skin penetration time-profiles for continuous 810 nm and Superpulsed 904 nm lasers in a rat model. Photomed. Laser Surg. 2012, 30, 688–694. [Google Scholar]
- Anders, J.J.; Wu, X. Comparison of light penetration of continuous wave 810 nm and superpulsed 904 nm wavelength light in anesthetized rats. Photomed. Laser Surg. 2016, 34, 418–424. [Google Scholar] [CrossRef]
- Nasouri, B.; Murphy, T.E.; Berberoglu, H. Near infrared laser penetration and absorption in human skin. Proc. SPIE 2014, 8932, 893207. [Google Scholar]
- Simpson, C.R.; Kohl, M.; Essenpreis, M.; Cope, M. Near-infrared optical properties of ex vivo human skin and subcutaneous tissues measured using the Monte Carlo inversion technique. Phys. Med. Biol. 1998, 43, 2465–2478. [Google Scholar] [CrossRef]
- Jacques, S.L. Optical properties of biological tissues: A review. Phys. Med. Biol. 2013, 58, R37–R61. [Google Scholar]
- Taroni, P.; Pifferi, A.; Torricelli, A.; Comelli, D.; Cubeddu, R. In vivo absorption and scattering spectroscopy of biological tissues. Photochem. Photobiol. Sci. 2003, 2, 124–129. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Laser Therapy Device | EMS Laser | K-Laser |
|---|---|---|
| Wavelengths [nm] | 905 | 800/905/970 |
| Modes | PW | CW/PW/ISP |
| [W] | 1.2 | 12 |
| [W] | 300 | 20 |
| Pulse lengths | 100 ns | 25 µs–0.5 s |
| Repetition rates [Hz] | 5–40 k | 1–20 k |
| Corrected Penetration Depth [mm] for | Corrected Transmittance [%] at | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Laser | Tissue | 15% | 10% | 5% | 1% | 5 mm | 10 mm | 15 mm | 20 mm |
| EMS laser | Chicken muscle | 7.3 | 9.6 | 13.6 | 23.0 | 22.1 | 9.3 | 3.9 | 1.7 |
| Porcine muscle | 4.9 | 6.6 | 9.5 | 16.1 | 14.8 | 4.4 | 1.3 | 0.4 | |
| Beef muscle 1 | 5.6 | 7.3 | 10.1 | 16.8 | 17.2 | 5.2 | 1.6 | 0.5 | |
| Beef muscle 2 | 5.7 | 7.5 | 10.5 | 17.4 | 17.8 | 5.6 | 1.8 | 0.6 | |
| Porcine skin | 5.2 | 6.9 | 9.7 | 16.4 | 15.6 | 4.7 | 1.4 | 0.4 | |
| Beef fat | 5.1 | 7.1 | 10.6 | 18.5 | 15.4 | 5.6 | 2.0 | 0.7 | |
| Beef tendon | 5.2 | 7.2 | 10.6 | 18.5 | 15.5 | 5.6 | 2.0 | 0.7 | |
| K-laser | Chicken muscle | 6.9 | 9.1 | 12.9 | 21.7 | 21.1 | 8.5 | 3.4 | 1.4 |
| Porcine muscle | 4.6 | 6.1 | 8.8 | 14.9 | 13.5 | 3.6 | 1.0 | 0.3 | |
| Beef muscle 1 | 5.8 | 7.6 | 10.8 | 18.1 | 17.7 | 5.9 | 2.0 | 0.7 | |
| Beef muscle 2 | 5.5 | 7.2 | 10.1 | 16.8 | 17.0 | 5.1 | 1.5 | 0.5 | |
| Porcine skin | 4.9 | 6.6 | 9.4 | 16.1 | 14.7 | 4.4 | 1.3 | 0.4 | |
| Beef fat | 5.1 | 7.1 | 10.4 | 18.2 | 15.3 | 5.4 | 1.9 | 0.7 | |
| Beef tendon | 4.9 | 6.8 | 10.1 | 17.7 | 14.7 | 5.1 | 1.8 | 0.6 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaub, L.; Schmitz, C. More than Ninety Percent of the Light Energy Emitted by Near-Infrared Laser Therapy Devices Used to Treat Musculoskeletal Disorders Is Absorbed within the First Ten Millimeters of Biological Tissue. Biomedicines 2022, 10, 3204. https://doi.org/10.3390/biomedicines10123204
Kaub L, Schmitz C. More than Ninety Percent of the Light Energy Emitted by Near-Infrared Laser Therapy Devices Used to Treat Musculoskeletal Disorders Is Absorbed within the First Ten Millimeters of Biological Tissue. Biomedicines. 2022; 10(12):3204. https://doi.org/10.3390/biomedicines10123204
Chicago/Turabian StyleKaub, Leon, and Christoph Schmitz. 2022. "More than Ninety Percent of the Light Energy Emitted by Near-Infrared Laser Therapy Devices Used to Treat Musculoskeletal Disorders Is Absorbed within the First Ten Millimeters of Biological Tissue" Biomedicines 10, no. 12: 3204. https://doi.org/10.3390/biomedicines10123204
APA StyleKaub, L., & Schmitz, C. (2022). More than Ninety Percent of the Light Energy Emitted by Near-Infrared Laser Therapy Devices Used to Treat Musculoskeletal Disorders Is Absorbed within the First Ten Millimeters of Biological Tissue. Biomedicines, 10(12), 3204. https://doi.org/10.3390/biomedicines10123204