

Comprehensive Grading System for Experimental Autoimmune Uveitis in Mice


Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
2.2. EAU Induction
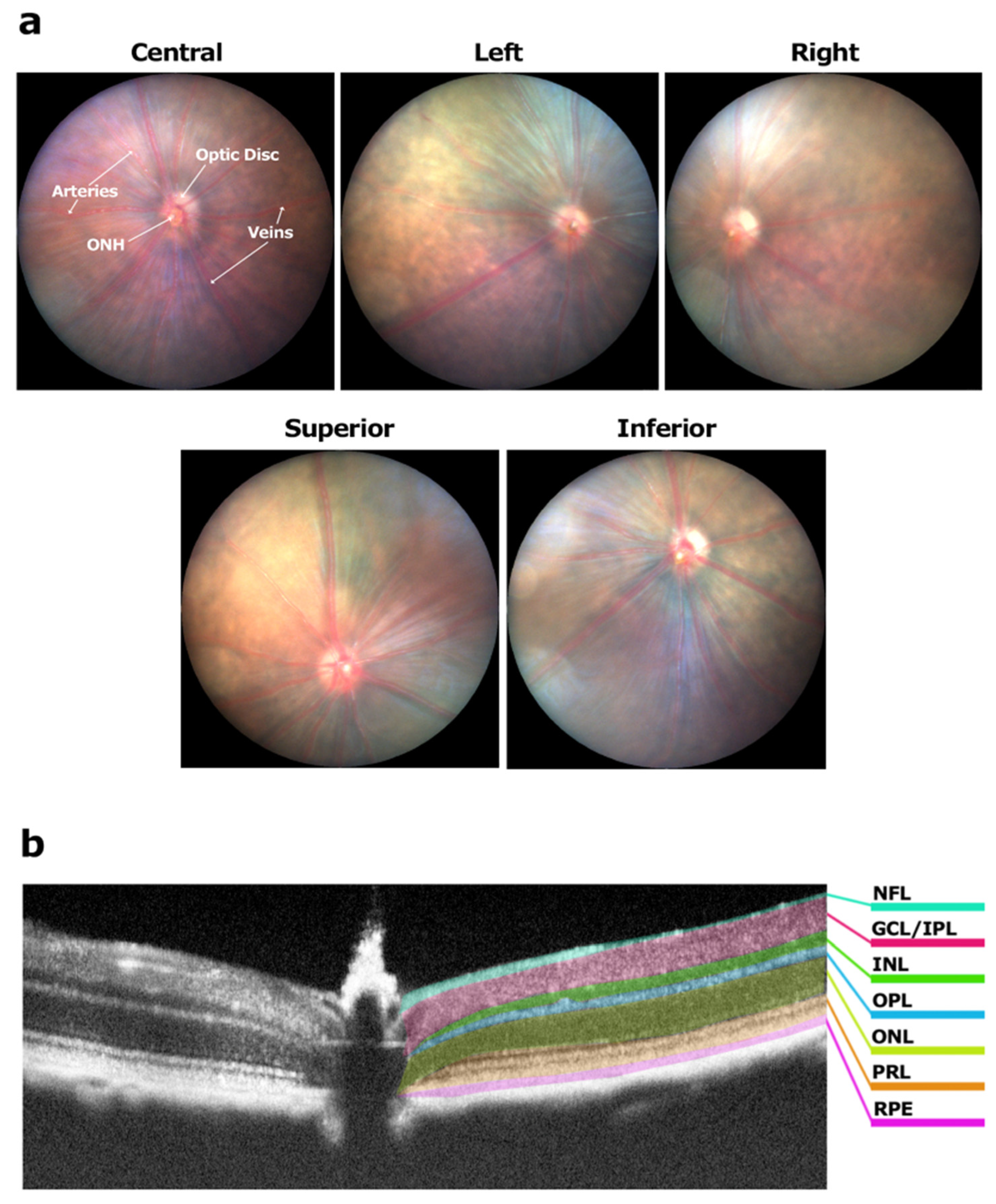
2.3. Fundus Imaging and Grading
2.3.1. Optic Disc
2.3.2. Retinal Blood Vessels
2.3.3. Retinal Tissue
2.3.4. Structural Damage
2.3.5. Grading
2.4. OCT Imaging and Grading
2.4.1. Vitreous
2.4.2. Retinal Layers
2.4.3. Grading
2.5. Statistical Analysis
3. Results
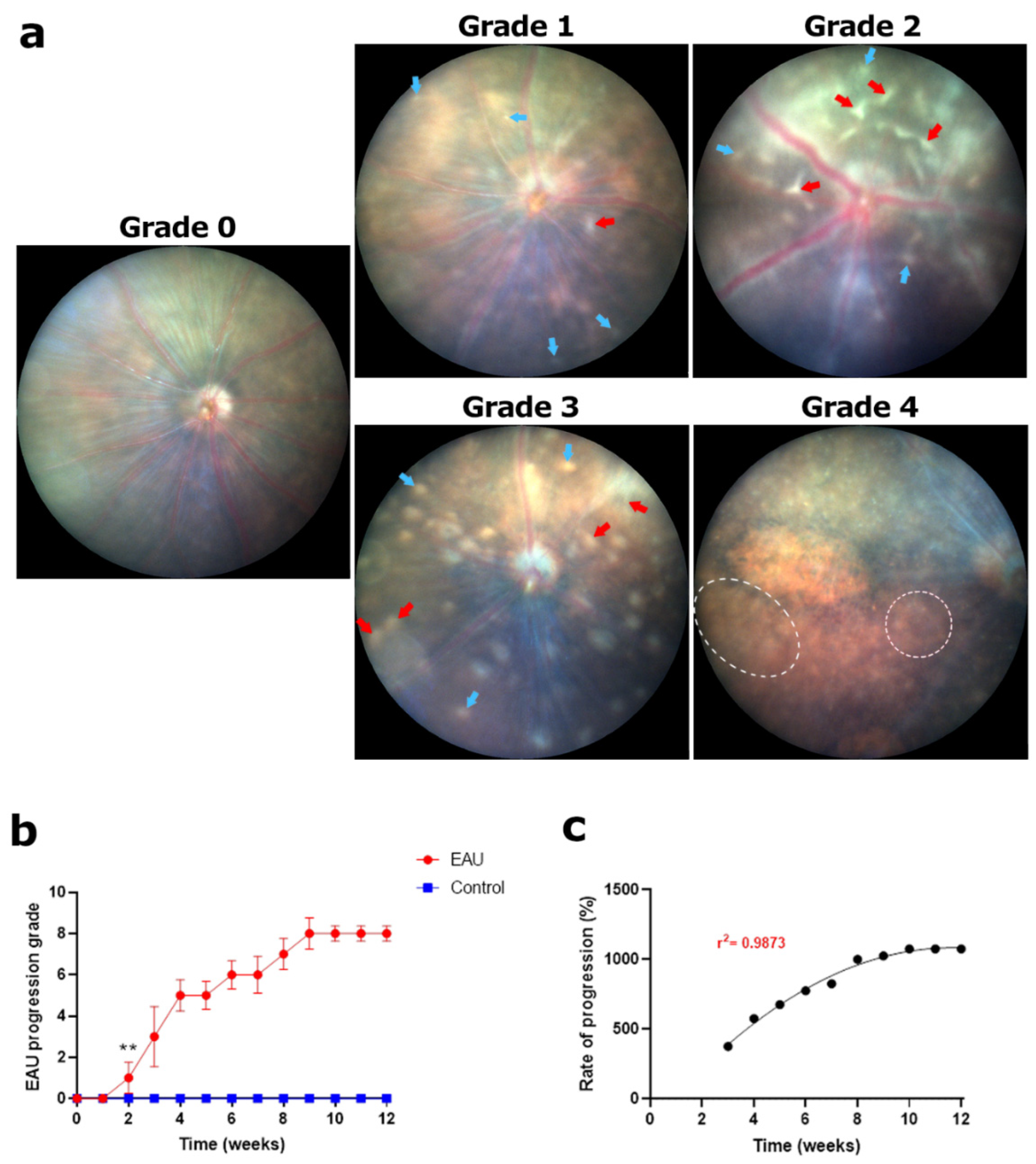
3.1. Fundus Imaging and Grading
3.1.1. Steady Rise in Swelling and Lesions in the Optic Disc Resulted in the Highest Clinical Score by Week 12
3.1.2. Rapid Progression of Cuffing in Retinal Blood Vessels Resulted in the Highest Clinical Score by Week 8
3.1.3. Increasing Retinal Tissue Lesions and Scarring Resulted in the Highest Clinical Scores by Week 9
3.1.4. Slowly Progressing Structural Damage in the Retina Resulted in Moderately High Clinical Scores by Week 12
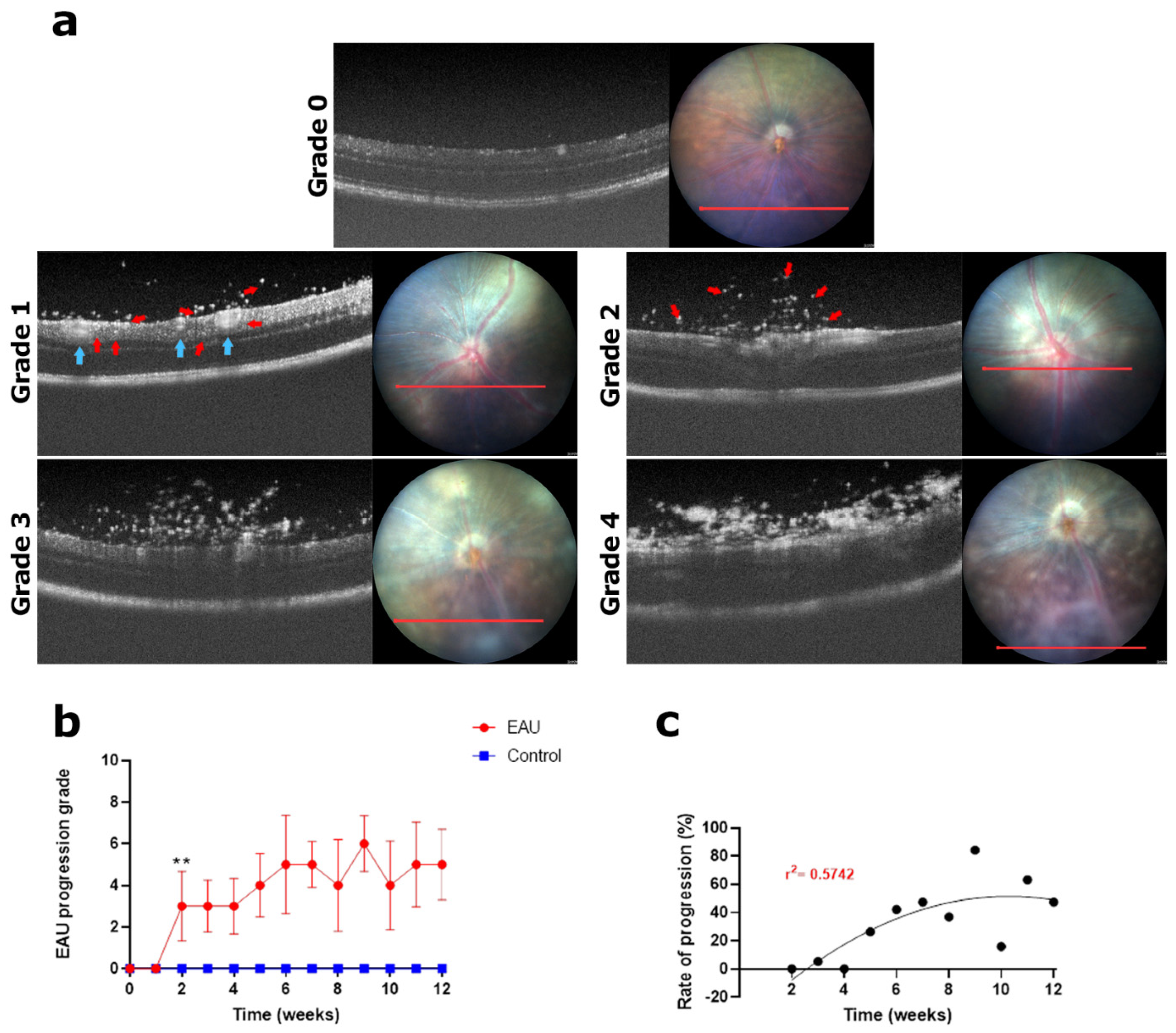
3.2. OCT Imaging and Grading
3.3. Slowly Progressing Structural Damage in the Retina Resulted in Moderately High Clinical Scores by Week 12
3.4. Large Areas of Subretinal Oedema and Granulomas in Retinal Layers Led to the Highest Clinical Score by Week 11
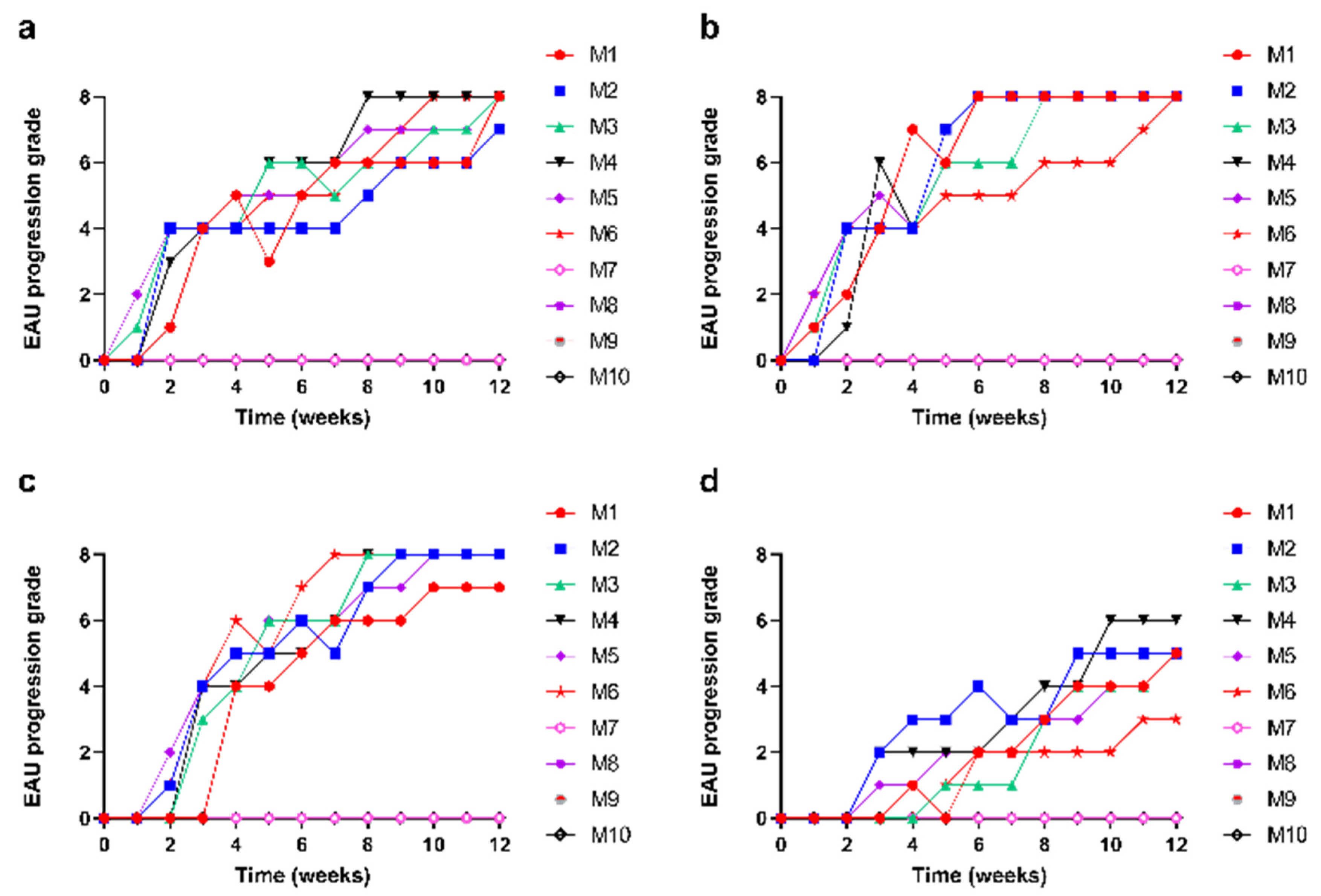
3.5. Slow and Steady Trajectory of EAU Signs over the 12-Week Study Period
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A




References
- Bansal, S.; Barathi, V.A.; Iwata, D.; Agrawal, R. Experimental autoimmune uveitis and other animal models of uveitis: An update. Indian J. Ophthalmol. 2015, 63, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Goldblum, D.; Fausch, K.; Frueh, B.E.; Theurillat, R.; Thormann, W.; Zimmerli, S. Ocular penetration of caspofungin in a rabbit uveitis model. Graefes Arch. Clin. Exp. Ophthalmol. 2007, 245, 825–833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agarwal, R.K.; Silver, P.B.; Caspi, R.R. Rodent models of experimental autoimmune uveitis. Methods Mol. Biol. 2012, 900, 443–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yadav, U.C.S.; Ramana, K.V. Endotoxin-Induced Uveitis in Rodents. In Mouse Models of Innate Immunity: Methods and Protocols; Allen, I.C., Ed.; Humana Press: Totowa, NJ, USA, 2013; pp. 155–162. [Google Scholar] [CrossRef]
- Chen, J.; Qian, H.; Horai, R.; Chan, C.C.; Caspi, R.R. Mouse Models of Experimental Autoimmune Uveitis: Comparative Analysis of Adjuvant-Induced vs Spontaneous Models of Uveitis. Curr. Mol. Med. 2015, 15, 550–557. [Google Scholar] [CrossRef]
- Shome, A.; Mugisho, O.O.; Niederer, R.L.; Rupenthal, I.D. Blocking the inflammasome: A novel approach to treat uveitis. Drug Discov. Today 2021, 26, 2839–2857. [Google Scholar] [CrossRef]
- Minos, E.; Barry, R.J.; Southworth, S.; Folkard, A.; Murray, P.I.; Duker, J.S.; Keane, P.A.; Denniston, A.K. Birdshot chorioretinopathy: Current knowledge and new concepts in pathophysiology, diagnosis, monitoring and treatment. Orphanet J. Rare Dis. 2016, 11, 61. [Google Scholar] [CrossRef] [Green Version]
- Durrani, O.M.; Meads, C.A.; Murray, P.I. Uveitis: A potentially blinding disease. Ophthalmologica 2004, 218, 223–236. [Google Scholar] [CrossRef]
- Wacker, W.B.; Kalsow, C.M. Autoimmune uveo-retinitis in the rat sensitized with retina photoreceptor cell antigen. Int. Arch. Allergy Appl. Immunol. 1973, 45, 582–592. [Google Scholar] [CrossRef]
- Caspi, R.R. Animal models of autoimmune and immune-mediated uveitis. Drug Discov. Today Dis. Models 2006, 3, 3–9. [Google Scholar] [CrossRef]
- Caspi, R.R.; Roberge, F.G.; Chan, C.C.; Wiggert, B.; Chader, G.J.; Rozenszajn, L.A.; Lando, Z.; Nussenblatt, R.B. A new model of autoimmune disease. Experimental autoimmune uveoretinitis induced in mice with two different retinal antigens. J. Immunol. 1988, 140, 1490–1495. [Google Scholar] [CrossRef]
- Caspi, R.R.; Chan, C.-C.; Wiggert, B.; Chader, G.J. The mouse as a model of experimental autoimmune uveoretinitis (EAU). Curr. Eye Res. 1990, 9, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Paques, M.; Guyomard, J.-L.; Simonutti, M.; Roux, M.J.; Picaud, S.; LeGargasson, J.-F.o.; Sahel, J.-A. Panretinal, High-Resolution Color Photography of the Mouse Fundus. Investig. Ophthalmol. Vis. Sci. 2007, 48, 2769–2774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, H.; Koch, P.; Chen, M.; Lau, A.; Reid, D.M.; Forrester, J.V. A clinical grading system for retinal inflammation in the chronic model of experimental autoimmune uveoretinitis using digital fundus images. Exp. Eye Res. 2008, 87, 319–326. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, V.J.; Ko, T.H.; Wojtkowski, M.; Carvalho, M.; Clermont, A.; Bursell, S.-E.; Song, Q.H.; Lem, J.; Duker, J.S.; Schuman, J.S.; et al. Noninvasive Volumetric Imaging and Morphometry of the Rodent Retina with High-Speed, Ultrahigh-Resolution Optical Coherence Tomography. Investig. Ophthalmol. Vis. Sci. 2006, 47, 5522–5528. [Google Scholar] [CrossRef] [PubMed]
- Harimoto, K.; Ito, M.; Karasawa, Y.; Sakurai, Y.; Takeuchi, M. Evaluation of mouse experimental autoimmune uveoretinitis by spectral domain optical coherence tomography. Br. J. Ophthalmol. 2014, 98, 808–812. [Google Scholar] [CrossRef]
- Wigg, J.P.; Zhang, H.; Yang, D. A Quantitative and Standardized Method for the Evaluation of Choroidal Neovascularization Using MICRON III Fluorescein Angiograms in Rats. PLoS ONE 2015, 10, e0128418. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, A.; Boyd, R.F.; Yekkala, K. Correlations Between Retinal Optical Coherence Tomography and Histopathology in Preclinical Safety Assessment of Ocular Therapies. Toxicol. Pathol. 2021, 49, 528–536. [Google Scholar] [CrossRef]
- Kang, W.S.; Choi, H.; Jang, G.; Lee, K.H.; Kim, E.; Kim, K.J.; Jeong, G.-Y.; Kim, J.S.; Na, C.-S.; Kim, S. Long-Term Exposure to Urban Particulate Matter on the Ocular Surface and the Incidence of Deleterious Changes in the Cornea, Conjunctiva and Retina in Rats. Int. J. Mol. Sci. 2020, 21, 4976. [Google Scholar] [CrossRef]
- Chen, J.; Qian, H.; Horai, R.; Chan, C.-C.; Caspi, R.R. Use of optical coherence tomography and electroretinography to evaluate retinal pathology in a mouse model of autoimmune uveitis. PLoS ONE 2013, 8, e63904. [Google Scholar] [CrossRef] [Green Version]
- Percie du Sert, N.; Ahluwalia, A.; Alam, S.; Avey, M.T.; Baker, M.; Browne, W.J.; Clark, A.; Cuthill, I.C.; Dirnagl, U.; Emerson, M.; et al. Reporting animal research: Explanation and elaboration for the ARRIVE guidelines 2.0. PLoS Biol. 2020, 18, e3000411. [Google Scholar] [CrossRef]
- Chen, X.; Kezic, J.M.; Forrester, J.V.; Goldberg, G.L.; Wicks, I.P.; Bernard, C.C.; McMenamin, P.G. In vivo multi-modal imaging of experimental autoimmune uveoretinitis in transgenic reporter mice reveals the dynamic nature of inflammatory changes during disease progression. J. Neuroinflammation 2015, 12, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.; Qian, H.; Horai, R.; Chan, C.-C.; Falick, Y.; Caspi, R. Comparative Analysis of Induced vs. Spontaneous Models of Autoimmune Uveitis Targeting the Interphotoreceptor Retinoid Binding Protein. PLoS ONE 2013, 8, e72161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mugisho, O.O.; Rupenthal, I.D.; Squirrell, D.M.; Bould, S.J.; Danesh-Meyer, H.V.; Zhang, J.; Green, C.R.; Acosta, M.L. Intravitreal pro-inflammatory cytokines in non-obese diabetic mice: Modelling signs of diabetic retinopathy. PLoS ONE 2018, 13, e0202156. [Google Scholar] [CrossRef]
- Mugisho, O.O.; Green, C.R.; Squirrell, D.M.; Bould, S.; Danesh-Meyer, H.V.; Zhang, J.; Acosta, M.L.; Rupenthal, I.D. Connexin43 hemichannel block protects against the development of diabetic retinopathy signs in a mouse model of the disease. J. Mol. Med. 2019, 97, 215–229. [Google Scholar] [CrossRef]
- Fan, N.W.; Li, J.; Mittal, S.K.; Foulsham, W.; Elbasiony, E.; Huckfeldt, R.M.; Chauhan, S.K.; Chen, Y. Characterization of Clinical and Immune Responses in an Experimental Chronic Autoimmune Uveitis Model. Am. J. Pathol. 2021, 191, 425–437. [Google Scholar] [CrossRef]
- Chen, J.; Caspi, R.R. Clinical and Functional Evaluation of Ocular Inflammatory Disease Using the Model of Experimental Autoimmune Uveitis. In Immunological Tolerance: Methods and Protocols; Boyd, A.S., Ed.; Springer: New York, NY, USA, 2019; pp. 211–227. [Google Scholar] [CrossRef]
- Meng, X.; Fang, S.; Zhang, Z.; Wang, Y.; You, C.; Zhang, J.; Yan, H. Preventive effect of chrysin on experimental autoimmune uveitis triggered by injection of human IRBP peptide 1–20 in mice. Cell. Mol. Immunol. 2017, 14, 702–711. [Google Scholar] [CrossRef] [Green Version]
- Xu, H.; Forrester, J.V.; Liversidge, J.; Crane, I.J. Leukocyte trafficking in experimental autoimmune uveitis: Breakdown of blood-retinal barrier and upregulation of cellular adhesion molecules. Investig. Ophthalmol. Vis. Sci. 2003, 44, 226–234. [Google Scholar] [CrossRef] [Green Version]
- Onal, S.; Tugal-Tutkun, I.; Neri, P.; Herbort, C.P. Optical coherence tomography imaging in uveitis. Int. Ophthalmol. 2014, 34, 401–435. [Google Scholar] [CrossRef] [PubMed]
- Ko, M.K.; Shao, H.; Kaplan, H.J.; Sun, D. Timing Effect of Adenosine-Directed Immunomodulation on Mouse Experimental Autoimmune Uveitis. J. Immunol. 2021, 207, 153–161. [Google Scholar] [CrossRef]
- Bradley, L.J.; Ward, A.; Hsue, M.C.Y.; Liu, J.; Copland, D.A.; Dick, A.D.; Nicholson, L.B. Quantitative Assessment of Experimental Ocular Inflammatory Disease. Front. Immunol. 2021, 12, 630022. [Google Scholar] [CrossRef]
- Chen, Y.; Chen, Z.; Chong, P.W.; Wu, S.; Wang, W.; Zhou, H.; Chen, J. Comparative Analysis of the Interphotoreceptor Retinoid Binding ProteinInduced Models of Experimental Autoimmune Uveitis in B10.RIII versus C57BL/6 Mice. Curr. Mol. Med. 2018, 18, 602–611. [Google Scholar] [CrossRef] [PubMed]
- Forrester, J.V.; Liversidge, J.; Dua, H.S.; Towler, H.; McMenamin, P.G. Comparison of clinical and experimental uveitis. Curr. Eye Res. 1990, 9, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Pichi, F.; Sarraf, D.; Arepalli, S.; Lowder, C.Y.; Cunningham, E.T.; Neri, P.; Albini, T.A.; Gupta, V.; Baynes, K.; Srivastava, S.K. The application of optical coherence tomography angiography in uveitis and inflammatory eye diseases. Prog. Retin. Eye Res. 2017, 59, 178–201. [Google Scholar] [CrossRef] [PubMed]
- Chu, C.J.; Herrmann, P.; Carvalho, L.S.; Liyanage, S.E.; Bainbridge, J.W.B.; Ali, R.R.; Dick, A.D.; Luhmann, U.F.O. Assessment and in vivo scoring of murine experimental autoimmune uveoretinitis using optical coherence tomography. PLoS ONE 2013, 8, e63002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Touhami, S.; Leclercq, M.; Stanescu-Segall, D.; Touitou, V.; Bodaghi, B. Differential Diagnosis of Vitritis in Adult Patients. Ocul. Immunol. Inflamm. 2021, 29, 786–795. [Google Scholar] [CrossRef]
- Choi, W.J.; Pepple, K.L.; Wang, R.K. Automated three-dimensional cell counting method for grading uveitis of rodent eye in vivo with optical coherence tomography. J. Biophotonics 2018, 11, e201800140. [Google Scholar] [CrossRef]
- Bowers, C.E.; Calder, V.L.; Greenwood, J.; Eskandarpour, M.J.J.o.v.e.J. Experimental Autoimmune Uveitis: An Intraocular Inflammatory Mouse Model. J. Vis. Exp. 2022, 179, e61832. [Google Scholar] [CrossRef]
- Li, H.; Zhu, L.; Wang, R.; Xie, L.; Ren, J.; Ma, S.; Zhang, W.; Liu, X.; Huang, Z.; Chen, B.; et al. Aging weakens Th17 cell pathogenicity and ameliorates experimental autoimmune uveitis in mice. Protein Cell 2022, 13, 422–445. [Google Scholar] [CrossRef]
- Fukushima, A.; Yamaguchi, T.; Ishida, W.; Fukata, K.; Udaka, K.; Ueno, H. Mice lacking the IFN-gamma receptor or fyn develop severe experimental autoimmune uveoretinitis characterized by different immune responses. Immunogenetics 2005, 57, 337–343. [Google Scholar] [CrossRef]
- Cortes, L.M.; Mattapallil, M.J.; Silver, P.B.; Donoso, L.A.; Liou, G.I.; Zhu, W.; Chan, C.-C.; Caspi, R.R. Repertoire Analysis and New Pathogenic Epitopes of IRBP in C57BL/6 (H-2b) and B10.RIII (H-2r) Mice. Investig. Ophthalmol. Vis. Sci. 2008, 49, 1946–1956. [Google Scholar] [CrossRef] [Green Version]
- Mattapallil, M.J.; Silver, P.B.; Cortes, L.M.; St. Leger, A.J.; Jittayasothorn, Y.; Kielczewski, J.L.; Moon, J.J.; Chan, C.-C.; Caspi, R.R. Characterization of a New Epitope of IRBP That Induces Moderate to Severe Uveoretinitis in Mice With H-2b Haplotype. Investig. Ophthalmol. Vis. Sci. 2015, 56, 5439–5449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, S.-M.; Yang, C.-H.; Tsai, H.-Y.; Lin, C.-J.; Fang, Y.-H.; Shieh, C.-C.; Chen, S.-H. Chitosan Oligosaccharides Suppress Nuclear Factor-Kappa B Activation and Ameliorate Experimental Autoimmune Uveoretinitis in Mice. Int. J. Mol. Sci. 2020, 21, 8326. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.-R.; Lumsden, L.; Forrester, J.V. Macrophages and Dendritic Cells in IRBP-Induced Experimental Autoimmune Uveoretinitis in B10RIII Mice. Investig. Ophthalmol. Vis. Sci. 1999, 40, 3177–3185. [Google Scholar]
- Maatta, J.; Nygardas, P.T.; Hinkkanen, A. Enhancement of Experimental Autoimmune Encephalomyelitis Severity by Ultrasound Emulsification of Antigen/Adjuvant in Distinct Strains of Mice. Scand. J. Immunol. 2000, 51, 87–90. [Google Scholar] [CrossRef]
- Taha, A.; Ahmed, E.; Ismaiel, A.; Ashokkumar, M.; Xu, X.Y.; Pan, S.Y.; Hu, H. Ultrasonic emulsification: An overview on the preparation of different emulsifiers-stabilized emulsions. Trends Food Sci. Technol. 2020, 105, 363–377. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Grade | Optic Disc | Retinal Blood Vessels | Retinal Tissue | Structural Damage |
|---|---|---|---|---|
| 0 |
|
|
|
|
| 1 |
|
|
|
|
| 2 |
|
|
|
|
| 3 |
|
|
|
|
| 4 |
|
|
|
|
| Grade | Vitreous | Retinal Layers |
|---|---|---|
| 0 |
|
|
| 1 |
|
|
| 2 |
|
|
| 3 |
|
|
| 4 |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shome, A.; Mugisho, O.O.; Niederer, R.L.; Rupenthal, I.D. Comprehensive Grading System for Experimental Autoimmune Uveitis in Mice. Biomedicines 2023, 11, 2022. https://doi.org/10.3390/biomedicines11072022
Shome A, Mugisho OO, Niederer RL, Rupenthal ID. Comprehensive Grading System for Experimental Autoimmune Uveitis in Mice. Biomedicines. 2023; 11(7):2022. https://doi.org/10.3390/biomedicines11072022
Chicago/Turabian StyleShome, Avik, Odunayo O. Mugisho, Rachael L. Niederer, and Ilva D. Rupenthal. 2023. "Comprehensive Grading System for Experimental Autoimmune Uveitis in Mice" Biomedicines 11, no. 7: 2022. https://doi.org/10.3390/biomedicines11072022
APA StyleShome, A., Mugisho, O. O., Niederer, R. L., & Rupenthal, I. D. (2023). Comprehensive Grading System for Experimental Autoimmune Uveitis in Mice. Biomedicines, 11(7), 2022. https://doi.org/10.3390/biomedicines11072022