
Novel Gene Polymorphisms for Stable Warfarin Dose in a Korean Population: Genome-Wide Association Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants and Data Collection
2.2. Genotyping and Sample Quality Control
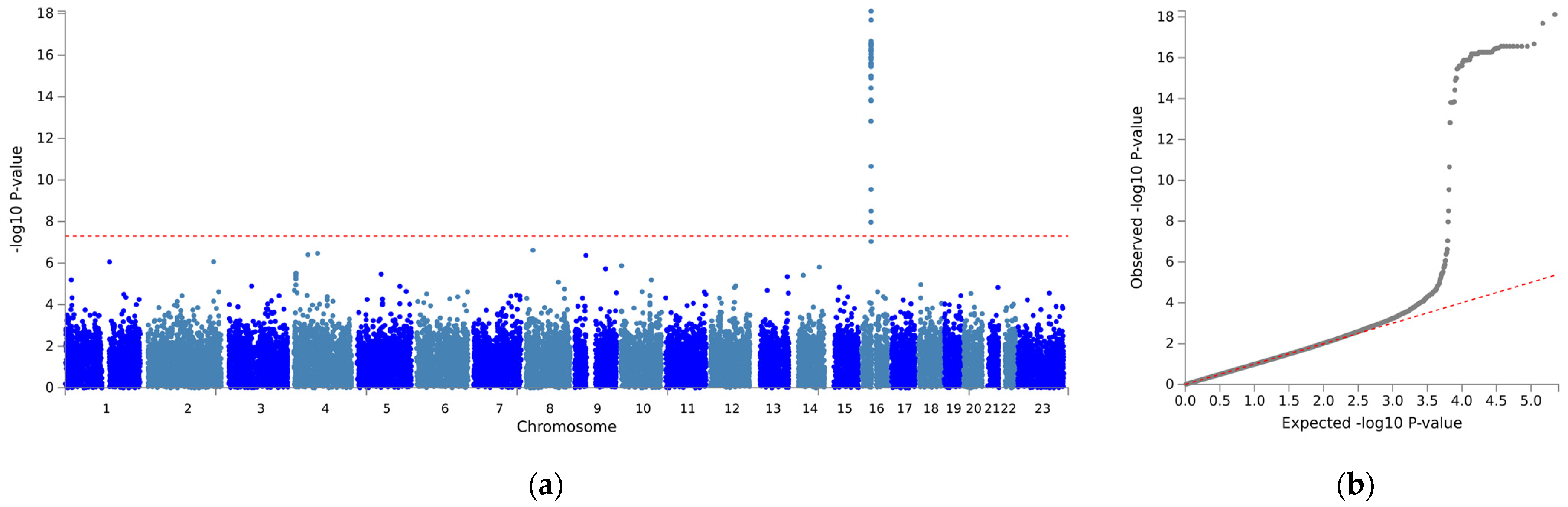
2.3. Genome-Wide Association Studies (GWAS)
2.4. Statistical Analysis
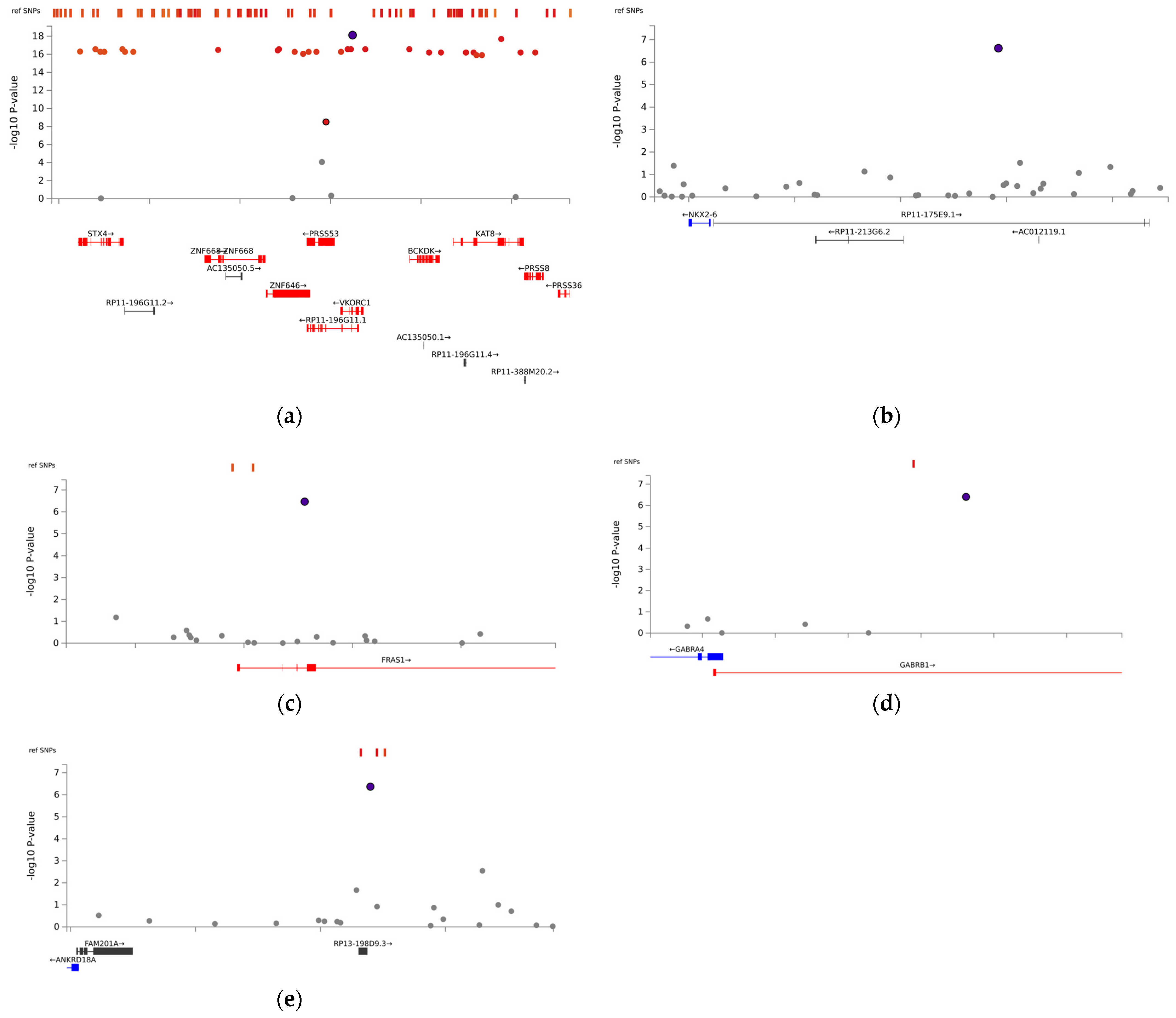
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roden, D.M.; Johnson, J.A.; Kimmel, S.E.; Krauss, R.M.; Medina, M.W.; Shuldiner, A.; Wilke, R.A. Cardiovascular pharmacogenomics. Circ. Res. 2011, 109, 807–820. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.A. Warfarin: An old drug but still interesting. Pharmacotherapy 2008, 28, 1081–1083. [Google Scholar] [CrossRef] [PubMed]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P.; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients with Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 143, e35–e71. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.A. Ethnic differences in cardiovascular drug response: Potential contribution of pharmacogenetics. Circulation 2008, 118, 1383–1393. [Google Scholar] [CrossRef] [PubMed]
- Holbrook, A.M.; Pereira, J.A.; Labiris, R.; McDonald, H.; Douketis, J.D.; Crowther, M.; Wells, P.S. Systematic overview of warfarin and its drug and food interactions. Arch. Intern. Med. 2005, 165, 1095–1106. [Google Scholar] [CrossRef]
- White, P.J. Patient factors that influence warfarin dose response. J. Pharm. Pract. 2010, 23, 194–204. [Google Scholar] [CrossRef]
- Franco, V.; Polanczyk, C.A.; Clausell, N.; Rohde, L.E. Role of dietary vitamin K intake in chronic oral anticoagulation: Prospective evidence from observational and randomized protocols. Am. J. Med. 2004, 116, 651–656. [Google Scholar]
- Miners, J.O.; Birkett, D.J. Cytochrome P4502C9: An enzyme of major importance in human drug metabolism. Br. J. Clin. Pharmacol. 1998, 45, 525–538. [Google Scholar]
- Limdi, N.A. Warfarin pharmacogenetics: Challenges and opportunities for clinical translation. Front. Pharmacol. 2012, 3, 183. [Google Scholar] [CrossRef]
- Kaye, J.B.; Schultz, L.E.; Steiner, H.E.; Kittles, R.A.; Cavallari, L.H.; Karnes, J.H. Warfarin Pharmacogenomics in Diverse Populations. Pharmacotherapy 2017, 37, 1150–1163. [Google Scholar] [CrossRef]
- Ward, L.D.; Kellis, M. HaploReg v4: Systematic mining of putative causal variants, cell types, regulators and target genes for human complex traits and disease. Nucleic Acids Res. 2016, 44, D877–D881. [Google Scholar] [CrossRef]
- Sayers, E.W.; Beck, J.; Bolton, E.E.; Bourexis, D.; Brister, J.R.; Canese, K.; Comeau, D.C.; Funk, K.; Kim, S.; Klimke, W.; et al. Database resources of the national center for biotechnology information. Nucleic Acids Res. 2021, 49, D10. [Google Scholar] [CrossRef]
- Tam, V.; Patel, N.; Turcotte, M.; Bossé, Y.; Paré, G.; Meyre, D. Benefits and limitations of genome-wide association studies. Nat. Rev. Genet. 2019, 20, 467–484. [Google Scholar] [CrossRef] [PubMed]
- El Rouby, N.; Shahin, M.H.; Bader, L.; Khalifa, S.I.; Elewa, H. Genomewide association analysis of warfarin dose requirements in Middle Eastern and North African populations. Clin. Transl. Sci. 2022, 15, 558–566. [Google Scholar] [CrossRef]
- Parra, E.J.; Botton, M.R.; A Perini, J.; Krithika, S.; Bourgeois, S.; A Johnson, T.; Tsunoda, T.; Pirmohamed, M.; Wadelius, M.; A Limdi, N.; et al. Genome-wide association study of warfarin maintenance dose in a Brazilian sample. Pharmacogenomics 2015, 16, 1253–1263. [Google Scholar] [CrossRef] [PubMed]
- Perera, M.A.; Cavallari, L.H.; Limdi, N.A.; Gamazon, E.R.; Konkashbaev, A.; Daneshjou, R.; Pluzhnikov, A.; Crawford, D.C.; Wang, J.; Liu, N.; et al. Genetic variants associated with warfarin dose in African-American individuals: A genome-wide association study. Lancet 2013, 382, 790–796. [Google Scholar] [CrossRef] [PubMed]
- Uffelmann, E.; Huang, Q.Q.; Munung, N.S.; De Vries, J.; Okada, Y.; Martin, A.R.; Martin, H.C.; Lappalainen, T.; Posthuma, D. Genome-wide association studies. Nat. Rev. Methods Primers 2021, 1, 59. [Google Scholar]
- Hoefele, J.; Wilhelm, C.; Schiesser, M.; Mack, R.; Heinrich, U.; Weber, L.T.; Biskup, S.; Daumer-Haas, C.; Klein, H.-G.; Rost, I. Expanding the mutation spectrum for Fraser syndrome: Identification of a novel heterozygous deletion in FRAS1. Gene 2013, 520, 194–197. [Google Scholar] [CrossRef]
- Asiimwe, I.G.; Blockman, M.; Cohen, K.; Cupido, C.; Hutchinson, C.; Jacobson, B.; Lamorde, M.; Morgan, J.; Mouton, J.P.; Nakagaayi, D.; et al. A genome-wide association study of plasma concentrations of warfarin enantiomers and metabolites in sub-Saharan black-African patients. Front. Pharmacol. 2022, 13, 967082. [Google Scholar] [CrossRef]
- Fridley, B.L.; Ghosh, T.M.; Wang, A.; Raghavan, R.; Dai, J.; Goode, E.L.; Lamba, J.K. Genome-wide study of response to platinum, taxane, and combination therapy in ovarian cancer: In vitro phenotypes, inherited variation, and disease recurrence. Front. Genet. 2016, 7, 37. [Google Scholar] [CrossRef]
- Xie, Q.; Li, Y.; Liu, Z.; Mu, G.; Zhang, H.; Zhou, S.; Wang, Z.; Wang, Z.; Jiang, J.; Li, X.; et al. SLC4A4, FRAS1, and SULT1A1 genetic variations associated with dabigatran metabolism in a healthy Chinese population. Front. Genet. 2022, 13, 873031. [Google Scholar] [CrossRef] [PubMed]
- Pagani, F.; Baralle, F.E. Genomic variants in exons and introns: Identifying the splicing spoilers. Nat. Rev. Genet. 2004, 5, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Raponi, M.; Baralle, D. Alternative splicing: Good and bad effects of translationally silent substitutions. FEBS J. 2010, 277, 836–840. [Google Scholar] [CrossRef] [PubMed]
- Strehle, E.-M.; Yu, L.; Rosenfeld, J.A.; Donkervoort, S.; Zhou, Y.; Chen, T.-J.; Martinez, J.E.; Fan, Y.-S.; Barbouth, D.; Zhu, H.; et al. Genotype-phenotype analysis of 4q deletion syndrome: Proposal of a critical region. Am. J. Med. Genet. A 2012, 158A, 2139–2151. [Google Scholar] [CrossRef] [PubMed]
- Strehle, E.M.; Bantock, H.M. The phenotype of patients with 4q-syndrome. Genet. Couns. 2003, 14, 195–205. [Google Scholar] [PubMed]
- Wang, Y.; Cao, L.; Liang, D.; Meng, L.; Wu, Y.; Qiao, F.; Ji, X.; Luo, C.; Zhang, J.; Xu, T.; et al. Prenatal chromosomal microarray analysis in fetuses with congenital heart disease: A prospective cohort study. Am. J. Obstet. Gynecol. 2018, 218, 244.E1–244.E17. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Ahmad, A.; Dagenais, S.; Iyer, R.K.; Innis, J.W. Chromosome 4q deletion syndrome: Narrowing the cardiovascular critical region to 4q32.2-q34.3. Am. J. Med. Genet. A 2012, 158A, 635–640. [Google Scholar] [CrossRef] [PubMed]
- Leppert, M.; Poisson, S.N.; Carroll, J.D. Atrial Septal Defects and Cardioembolic Strokes. Cardiol. Clin. 2016, 34, 225–230. [Google Scholar] [CrossRef]
- Mandalenakis, Z.; Rosengren, A.; Lappas, G.; Eriksson, P.; Hansson, P.O.; Dellborg, M. Ischemic Stroke in Children and Young Adults with Congenital Heart Disease. J. Am. Heart Assoc. 2016, 5, e003071. [Google Scholar] [CrossRef]
- Huang, J.; Yu, Q.; Zhou, Y.; Chu, Y.; Jiang, F.; Wang, Q. FAM201A knockdown inhibits proliferation and invasion of lung adenocarcinoma cells by regulating miR-7515/GLO1 axis. J. Cell. Physiol. 2021, 236, 5620–5632. [Google Scholar] [CrossRef]
- He, W.; Qiao, Z.-X.; Ma, B. Long noncoding RNA FAM201A mediates the metastasis of lung squamous cell cancer via regulating ABCE1 expression. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 10343–10353. [Google Scholar] [PubMed]
- Huang, G.; Zhao, G.; Xia, J.; Wei, Y.; Chen, F.; Chen, J.; Shi, J. FGF2 and FAM201A affect the development of osteonecrosis of the femoral head after femoral neck fracture. Gene 2018, 652, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; He, X.Y.; Dan, Q.; Li, Y. FAM201A, a long noncoding RNA potentially associated with atrial fibrillation identified by ceRNA network analyses and WGCNA. BMC Med. Genom. 2022, 15, 80. [Google Scholar] [CrossRef] [PubMed]
- Carithers, L.J.; Moore, H.M. The Genotype-Tissue Expression (GTEx) Project. Biopreserv. Biobank. 2015, 13, 307–308. [Google Scholar] [CrossRef]
- Zaidi, S.; Brueckner, M. Genetics and Genomics of Congenital Heart Disease. Circ. Res. 2017, 120, 923–940. [Google Scholar] [CrossRef] [PubMed]
- Biben, C.; Hatzistavrou, T.; Harvey, R. Expression of NK-2 class homeobox gene Nkx2–6 in foregut endoderm and heart. Mech. Dev. 1998, 73, 125–127. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Schinke, M.; Liao, H.-S.; Yamasaki, N.; Izumo, S. Nkx2. 5 and Nkx2. 6, homologs of Drosophila tinman, are required for development of the pharynx. Mol. Cell. Biol. 2001, 21, 4391–4398. [Google Scholar] [CrossRef]
- Fatkin, D.; Santiago, C.F.; Huttner, I.G.; Lubitz, S.A.; Ellinor, P.T. Genetics of Atrial Fibrillation: State of the Art in 2017. Heart Lung Circ. 2017, 26, 894–901. [Google Scholar] [CrossRef]
- Wang, J.; Zhang, D.-F.; Sun, Y.-M.; Li, R.-G.; Qiu, X.-B.; Qu, X.-K.; Liu, X.; Fang, W.-Y.; Yang, Y.-Q. NKX2-6 mutation predisposes to familial atrial fibrillation. Int. J. Mol. Med. 2014, 34, 1581–1590. [Google Scholar] [CrossRef]
- Boon, N.A.; Bloomfield, P. The medical management of valvar heart disease. Heart 2002, 87, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Park, H.J.; La, H.-O.; Gwak, H.S. Effects of Diuretics on Warfarin Responses in Patients with Atrial Fibrillation. Korean J. Clin. Pharm. 2013, 23, 151–157. [Google Scholar]
- Edwards, H.D.; Webb, R.D.; Conway, S.E. Effect of oral diuretics on chronic warfarin therapy: A retrospective study. Expert. Opin. Drug Saf. 2012, 11, 375–380. [Google Scholar] [CrossRef] [PubMed]
- Kamiyama, E.; Yoshigae, Y.; Kasuya, A.; Takei, M.; Kurihara, A.; Ikeda, T. Inhibitory effects of angiotensin receptor blockers on CYP2C9 activity in human liver microsomes. Drug Metab. Pharmacokinet. 2007, 22, 267–275. [Google Scholar] [CrossRef]
- Stangier, J.; Su CA, P.; Hendriks, M.G.; van Lier, J.J.; Sollie, F.A.; Oosterhuis, B.; Jonkman, J.H. Steady-state pharmacodynamics and pharmacokinetics of warfarin in the presence and absence of telmisartan in healthy male volunteers. J. Clin. Pharmacol. 2000, 40 Pt 1, 1331–1337. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, F.; McGinnis, R.; Bourgeois, S.; Barnes, C.; Eriksson, N.; Soranzo, N.; Whittaker, P.; Ranganath, V.; Kumanduri, V.; McLaren, W.; et al. A genome-wide association study confirms VKORC1, CYP2C9, and CYP4F2 as principal genetic determinants of warfarin dose. PLoS Genet. 2009, 5, e1000433. [Google Scholar] [CrossRef] [PubMed]
- Cooper, G.M.; Johnson, J.A.; Langaee, T.Y.; Feng, H.; Stanaway, I.B.; Schwarz, U.I.; Ritchie, M.D.; Stein, C.M.; Roden, D.M.; Smith, J.D.; et al. A genome-wide scan for common genetic variants with a large influence on warfarin maintenance dose. Blood 2008, 112, 1022–1027. [Google Scholar] [CrossRef]
- Limdi, N.A.; Beasley, T.M.; Crowley, M.R.; A Goldstein, J.; Rieder, M.J.; A Flockhart, D.; Arnett, D.K.; Acton, R.T.; Liu, N.; Shendre, A.; et al. VKORC1 polymorphisms, haplotypes and haplotype groups on warfarin dose among African-Americans and European-Americans. Pharmacogenomics 2008, 9, 1445–1458. [Google Scholar] [CrossRef] [PubMed]
- Cha, P.-C.; Mushiroda, T.; Takahashi, A.; Kubo, M.; Minami, S.; Kamatani, N.; Nakamura, Y. Genome-wide association study identifies genetic determinants of warfarin responsiveness for Japanese. Hum. Mol. Genet. 2010, 19, 4735–4744. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Number (%) (n = 214) | Stable Dose (mg/day) (mean ± SD) | p-Value |
|---|---|---|---|
| Age (year) | 58.3 ± 10.1 g | ||
| Age at operation (year) | 43.5 ± 11.2 g | ||
| Sex | 0.217 | ||
| Male | 71 (33.2) | 5.72 ± 1.95 | |
| Female | 143 (66.8) | 5.38 ± 1.92 | |
| Body mass index (kg/m2) | 0.480 | ||
| <25 | 160 (74.8) | 5.44 ± 1.83 | |
| ≥25 | 54 (25.2) | 5.65 ± 2.23 | |
| Valve position | 0.876 | ||
| Aortic | 47 (22.0) | 5.68 ± 1.60 | |
| Mitral | 106 (49.5) | 5.46 ± 2.03 | |
| Double a | 41 (19.2) | 5.38 ± 2.17 | |
| Tricuspid b | 16 (7.5) | 5.34 ± 1.77 | |
| Comorbidity | |||
| Hypertension | 0.174 | ||
| Yes | 18 (8.4) | 5.18 ± 1.70 | |
| No | 196 (91.6) | 5.59 ± 2.00 | |
| Diabetes mellitus | 0.940 | ||
| Yes | 18 (8.4) | 5.49 ± 1.94 | |
| No | 196 (91.6) | 5.49 ± 1.94 | |
| Congestive heart failure | 0.717 | ||
| Yes | 47 (22.0) | 5.40 ± 2.16 | |
| No | 167 (78.0) | 5.52 ± 1.87 | |
| Atrial fibrillation | 0.095 | ||
| Yes | 124 (57.9) | 5.30 ± 1.84 | |
| No | 90 (42.1) | 5.75 ± 2.03 | |
| Rheumatic disease | 0.650 | ||
| Yes | 122 (57.0) | 5.44 ± 1.90 | |
| No | 92 (43.0) | 5.56 ± 1.99 | |
| Myocardial infarction | 0.825 | ||
| Yes | 4 (1.90) | 5.70 ± 2.01 | |
| No | 210 (98.1) | 5.49 ± 1.94 | |
| Comedication | |||
| Antiplatelet drugs c | 0.582 | ||
| Yes | 8 (4.1) | 5.15 ± 1.10 | |
| No | 188 (95.9) | 5.53 ± 1.95 | |
| INR-increasing drugs d | 0.359 | ||
| Yes | 1 (0.5) | 3.75 | |
| No | 198 (99.5) | 5.52 ± 1.92 | |
| INR-decreasing drugs e | 0.353 | ||
| Yes | 2 (1.0) | 6.77 ± 2.50 | |
| No | 197 (99.0) | 5.50 ± 1.91 | |
| ARBs | 0.009 | ||
| Yes | 46 (21.9) | 4.81 ± 1.51 | |
| No | 164 (78.1) | 5.66 ± 2.00 | |
| ACEIs | 0.405 | ||
| Yes | 32 (15.2) | 5.21 ± 1.88 | |
| No | 178 (84.8) | 5.52 ± 1.94 | |
| Diuretics f | 0.001 | ||
| Yes | 90 (42.9) | 4.98 ± 1.89 | |
| No | 120 (57.1) | 5.84 ± 1.89 | |
| Calcium channel blockers | 0.389 | ||
| Yes | 31 (15.5) | 5.78 ± 2.01 | |
| No | 169 (84.5) | 5.46 ± 1.90 | |
| Statins | 0.455 | ||
| Yes | 8 (4.0) | 5.02 ± 1.43 | |
| No | 192 (96.0) | 5.53 ± 1.93 |
| CHR | Gene Polymorphism | Position | Allele Frequency | Grouped Genotypes | Number (%) | Stable Dose (mg/day) (mean ± SD) | p-Value |
|---|---|---|---|---|---|---|---|
| 16 | VKORC1 rs9934438 | 31104878 | G:A = 0.11:0.89 | GG | 4 (3.3) | 9.74 ± 2.18 | 6.23 × 10−6 |
| AG, AA | 209 (96.7) | 5.41 ± 1.84 | |||||
| 4 | FRAS1 rs4386623 | 78991190 | G:A = 0.99:0.01 | GG | 209 (95.9) | 5.39 ± 1.80 | 4.45 × 10−7 |
| GA, AA | 5 (4.1) | 9.70 ± 2.79 | |||||
| 9 | FAM201A rs1890109 | 38643996 | A:G = 0.98:0.02 | AA | 206 (94.6) | 5.39 ± 1.75 | 0.029 |
| AG, GG | 7 (5.4) | 9.04 ± 3.39 | |||||
| 8 | NKX2-6 rs310279 | 23618463 | A:G = 0.98:0.02 | AA | 205 (94.0) | 5.36 ± 1.78 | 9.30 × 10−3 |
| AG, GG | 8 (6.0) | 8.84 ± 2.78 | |||||
| 4 | GABRB1 rs117496075 | 47013091 | G:A = 0.98:0.02 | GG | 208 (95.4) | 5.39 ± 1.78 | 0.055 |
| GA, AA | 6 (4.6) | 8.99 ± 3.54 |
| Predictors | Model I | Model II | ||||
|---|---|---|---|---|---|---|
| β (95% CI) | R2 | p-Value | β (95% CI) | R2 | p-Value | |
| Age at operation (year) | −0.02 (−0.04, −0.01) | 0.011 | 0.027 | −0.02 (−0.04, −0.01) | 0.030 | 0.013 |
| ARBs | −0.54 (−1.00, −0.09) | 0.021 | 0.019 | −0.56 (−0.99, −0.14) | 0.015 | 0.010 |
| Diuretics | −0.46 (−0.85, −0.06) | 0.032 | 0.024 | −0.39 (−0.76, −0.02) | 0.009 | 0.040 |
| VKORC1 rs9934438 per A allele | −2.04 (−2.44, −1.64) | 0.330 | <2.0 × 10−16 | −1.98 (−2.44, −1.64) | 0.330 | <2.0 × 10−16 |
| FRAS1 rs4386623 (0 = GG, 1 = GA,AA) | 3.25 (2.04, 4.45) | 0.099 | 3.07 × 10−7 | 3.10 (2.04, 4.45) | 0.099 | 1.91 × 10−7 |
| FAM201A rs1890109 (0 = AA, 1 = AG,GG) | 1.71 (0.65, 2.76) | 0.040 | 0.002 | 1.91 (0.91, 2.90) | 0.047 | 2.00 × 10−4 |
| NKX2-6 rs310279 (0 = AA, 1 = AG,GG) | 1.43 (0.41, 2.44) | 0.013 | 0.006 | 1.32 (0.36, 2.28) | 0.020 | 0.007 |
| CYP2C9 rs1057910 per C allele | −1.75 (−2.41, −1.08) | 0.052 | 6.87 × 10−7 | |||
| Adjusted R2 | 0.531 | 0.585 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.S.; Lee, S.; Yee, J.; Park, K.; Jang, E.J.; Chang, B.C.; Gwak, H.S. Novel Gene Polymorphisms for Stable Warfarin Dose in a Korean Population: Genome-Wide Association Study. Biomedicines 2023, 11, 2308. https://doi.org/10.3390/biomedicines11082308
Kim JS, Lee S, Yee J, Park K, Jang EJ, Chang BC, Gwak HS. Novel Gene Polymorphisms for Stable Warfarin Dose in a Korean Population: Genome-Wide Association Study. Biomedicines. 2023; 11(8):2308. https://doi.org/10.3390/biomedicines11082308
Chicago/Turabian StyleKim, Jung Sun, Sak Lee, Jeong Yee, Kyemyung Park, Eun Jeong Jang, Byung Chul Chang, and Hye Sun Gwak. 2023. "Novel Gene Polymorphisms for Stable Warfarin Dose in a Korean Population: Genome-Wide Association Study" Biomedicines 11, no. 8: 2308. https://doi.org/10.3390/biomedicines11082308
APA StyleKim, J. S., Lee, S., Yee, J., Park, K., Jang, E. J., Chang, B. C., & Gwak, H. S. (2023). Novel Gene Polymorphisms for Stable Warfarin Dose in a Korean Population: Genome-Wide Association Study. Biomedicines, 11(8), 2308. https://doi.org/10.3390/biomedicines11082308