
Hyperalgesia, Increased Temporal Summation and Impaired Inhibitory Mechanisms in Episodic and Chronic Cluster Headache: An Observational Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
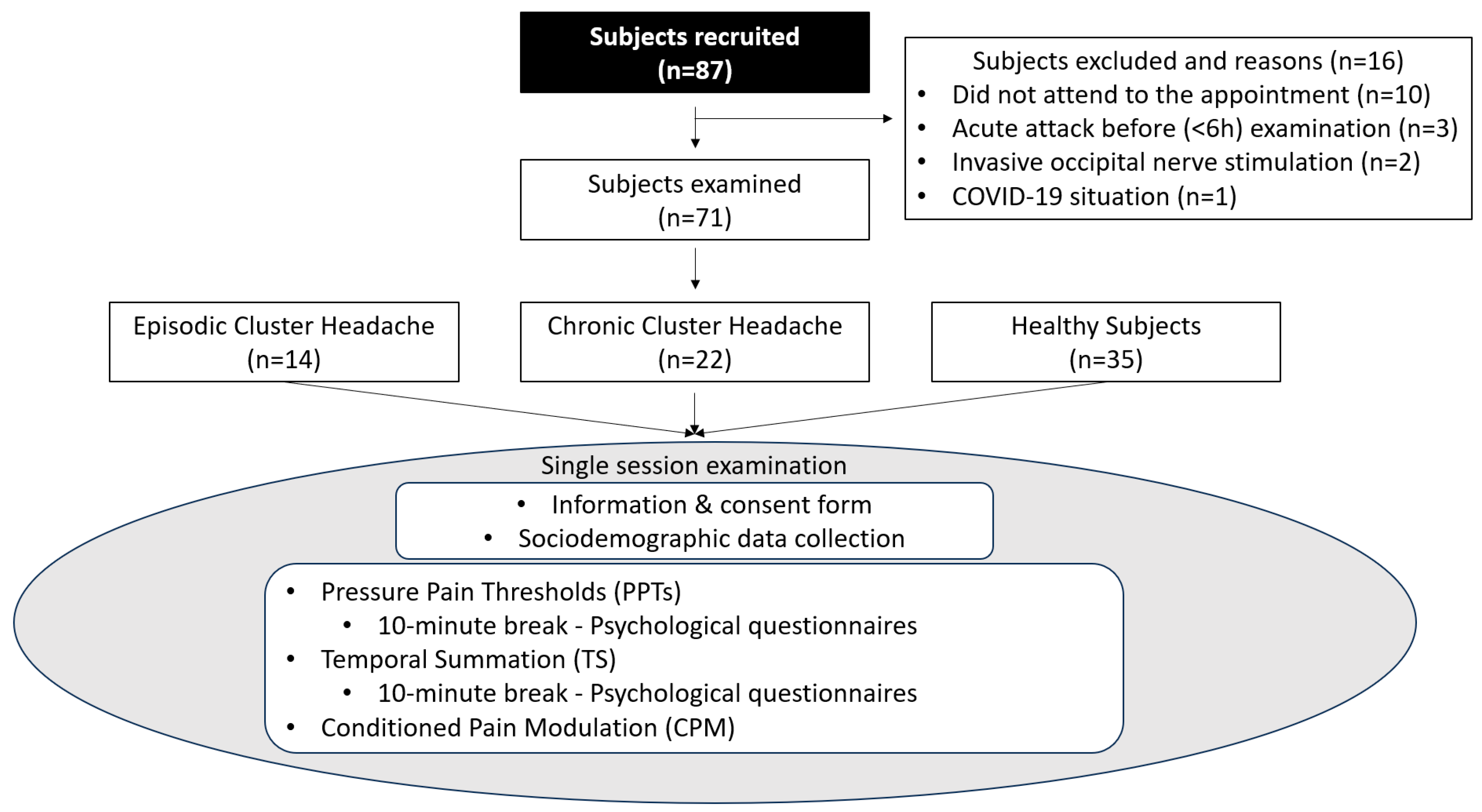
2.1. Participants
2.2. Procedures
2.2.1. Pressure Pain Thresholds (PPTs)
2.2.2. Temporal Summation (Wind-Up)
2.2.3. Conditioned Pain Modulation (CPM)
2.2.4. Psychosocial Questionnaires
2.3. Sample Size Calculation
2.4. Data Analysis
Comparison between Groups and Sides
3. Results
4. Discussion
4.1. Pressure Pain Thresholds
4.2. Temporal Summation
4.3. Conditioned Pain Modulation
4.4. Psychosocial Variables
4.5. Limitations
4.6. Future Directions
4.7. Clinical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Olesen, J. Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [Google Scholar]
- Fischera, M.; Marziniak, M.; Gralow, I.; Evers, S. The incidence and prevalence of cluster headache: A meta-analysis of population-based studies. Cephalalgia 2008, 28, 614–618. [Google Scholar] [CrossRef]
- Kim, S.A.; Choi, S.Y.; Youn, M.S.; Pozo-Rosich, P.; Lee, M.J. Epidemiology, burden and clinical spectrum of cluster headache: A global update. Cephalalgia 2023, 43, 3331024231201577. [Google Scholar] [CrossRef]
- Petersen, A.S.; Lund, N.; Snoer, A.; Jensen, R.H.; Barloese, M. The economic and personal burden of cluster headache: A controlled cross-sectional study. J. Headache Pain 2022, 23, 58. [Google Scholar] [CrossRef]
- May, A.; Schwedt, T.J.; Magis, D.; Pozo-Rosich, P.; Evers, S.; Wang, S.J. Cluster headache. Nat. Rev. Dis. Primers 2018, 4, 18006. [Google Scholar] [CrossRef]
- Schor, L.I.; Pearson, S.M.; Shapiro, R.E.; Zhang, W.; Miao, H.; Burish, M.J. Cluster headache epidemiology including pediatric onset, sex, and ICHD criteria: Results from the International Cluster Headache Questionnaire. Headache 2021, 61, 1511–1520. [Google Scholar] [CrossRef]
- Pringsheim, T. Cluster headache: Evidence for a disorder of circadian rhythm and hypothalamic function. Can. J. Neurol. Sci. 2002, 29, 33–40. [Google Scholar] [CrossRef]
- Strittmatter, M.; Hamann, G.F.; Grauer, M.; Fischer, C.; Blaes, F.; Hoffmann, K.H.; Schimrigk, K. Altered activity of the sympathetic nervous system and changes in the balance of hypophyseal, pituitary and adrenal hormones in patients with cluster headache. NeuroReport 1996, 7, 1229–1234. [Google Scholar] [CrossRef] [PubMed]
- Leone, M.; Bussone, G. A review of hormonal findings in cluster headache. Evid. Hypothal. Involv. Cephalalgia 1993, 13, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Holland, P.R. Modulation of trigeminovascular processing: Novel insights into primary headache disorders. Cephalalgia 2009, 29 (Suppl. S3), 1–6. [Google Scholar] [CrossRef] [PubMed]
- Malick, A.; Strassman, A.M.; Burstein, R. Trigeminohypothalamic and reticulohypothalamic tract neurons in the upper cervical spinal cord and caudal medulla of the rat. J. Neurophysiol. 2000, 84, 2078–2112. [Google Scholar] [CrossRef]
- Ferraro, S.; Nigri, A.; Demichelis, G.; Pinardi, C.; Chiapparini, L.; Giani, L.; Cecchini, A.P.; Leone, M. Understanding Cluster Headache Using Magnetic Resonance Imaging. Front. Neurol. 2020, 11, 535. [Google Scholar] [CrossRef]
- Loeser, J.D.; Treede, R.D. The Kyoto protocol of IASP Basic Pain Terminology. Pain 2008, 137, 473–477. [Google Scholar] [CrossRef]
- Gil-Martínez, A.; Navarro-Fernández, G.; Mangas-Guijarro, M.Á.; Diáz-De-Terán, J. Hyperalgesia and Central Sensitization Signs in Patients with Cluster Headache: A Cross-Sectional Study. Pain Med. 2019, 20, 2562–2570. [Google Scholar] [CrossRef]
- Fernández-de-las-Peñas, C.; Ortega-Santiago, R.; Cuadrado, M.L.; López-de-Silanes, C.; Pareja, J.A. Bilateral widespread mechanical pain hypersensitivity as sign of central sensitization in patients with cluster headache. Headache 2011, 51, 384–391. [Google Scholar] [CrossRef]
- Díaz-de-Terán, J.; Sastre-Real, M.; Lobato-Pérez, L.; Navarro-Fernández, G.; Elizagaray-García, I.; Gil-Martínez, A. Cluster headache, beyond the pain: A comparative cross-sectional study. Neurol. Sci. 2021, 42, 3673–3680. [Google Scholar] [CrossRef]
- Rolke, R.; Baron, R.; Maier, C.; Tölle, T.R.; Treede, R.D.; Beyer, A.; Binder, A.; Birbaumer, N.; Birklein, F.; Bötefür, I.C.; et al. Quantitative sensory testing in the German Research Network on Neuropathic Pain (DFNS): Standardized protocol and reference values. Pain 2006, 123, 231–243. [Google Scholar] [CrossRef]
- Quesada, C.; Kostenko, A.; Ho, I.; Leone, C.; Nochi, Z.; Stouffs, A.; Wittayer, M.; Caspani, O.; Finnerup, N.B.; Mouraux, A.; et al. Human surrogate models of central sensitization: A critical review and practical guide. Eur. J. Pain 2021, 25, 1389–1428. [Google Scholar] [CrossRef] [PubMed]
- Woolf, C.J. Central sensitization: Implications for the diagnosis and treatment of pain. Pain 2011, 152, S2–S15. [Google Scholar] [CrossRef] [PubMed]
- Palacios-Ceña, M.; Fuensalida-Novo, S.; Cuadrado, M.L.; Ordás-Bandera, C.; Madeleine, P.; Fernández-De-las-peñas, C.; Guerrero, L. Spatial Distribution of Temporalis Pressure Pain Sensitivity in Men with Episodic Cluster Headache. Int. J. Env. Res. Public Health 2019, 16, 4239. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Mayordomo, V.; Palacios-Ceña, M.; Guerrero-Peral, Á.; Fuensalida-Novo, S.; Fernández-de-las-Peñas, C.; Cuadrado, M.L. Widespread Hypersensitivity to Pressure Pain in Men With Cluster Headache During Prolonged Remission Is Not Related to the Levels of Depression and Anxiety. Pain Pract. 2020, 20, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Perrotta, A.; Serrao, M.; Ambrosini, A.; Bolla, M.; Coppola, G.; Sandrini, G.; Pierelli, F. Facilitated temporal processing of pain and defective supraspinal control of pain in cluster headache. Pain 2013, 154, 1325–1332. [Google Scholar] [CrossRef] [PubMed]
- Sandrini, G.; Antonaci, F.; Lanfranchi, S.; Milanov, I.; Danilov, A.; Nappi, G. Asymmetrical reduction of the nociceptive flexion reflex threshold in cluster headache. Cephalalgia 2000, 20, 647–652. [Google Scholar] [CrossRef] [PubMed]
- Ladda, J.; Straube, A.; Förderreuther, S.; Krause, P.; Eggert, T. Quantitative sensory testing in cluster headache: Increased sensory thresholds. Cephalalgia 2006, 26, 1043–1050. [Google Scholar] [CrossRef] [PubMed]
- Ellrich, J.; Ristic, D.; Yekta, S.S. Impaired thermal perception in cluster headache. J. Neurol. 2006, 253, 1292–1299. [Google Scholar] [CrossRef]
- Nuwailati, R.; Bobos, P.; Drangsholt, M.; Curatolo, M. Reliability of conditioned pain modulation in healthy individuals and chronic pain patients: A systematic review and meta-analysis. Scand. J. Pain 2022, 22, 262–278. [Google Scholar] [CrossRef]
- Moana-Filho, E.J.; Babiloni, A.H.; Theis-Mahon, N.R. Endogenous pain modulation in chronic orofacial pain: A systematic review and meta-analysis. Pain 2018, 159, 1441–1455. [Google Scholar] [CrossRef]
- Williams, A.E.; Miller, M.M.; Bartley, E.J.; McCabe, K.M.; Kerr, K.L.; Rhudy, J.L. Impairment of Inhibition of Trigeminal Nociception via Conditioned Pain Modulation in Persons with Migraine Headaches. Pain Med. Off. J. Am. Acad. Pain Med. 2019, 20, 1600. [Google Scholar] [CrossRef]
- Lewis, G.N.; Rice, D.A.; McNair, P.J. Conditioned pain modulation in populations with chronic pain: A systematic review and meta-analysis. J. Pain 2012, 13, 936–944. [Google Scholar] [CrossRef]
- Den Bandt, H.L.; Paulis, W.D.; Beckweé, D.; Ickmans, K.; Nijs, J.; Voogt, L. Pain Mechanisms in Low Back Pain: A Systematic Review With Meta-analysis of Mechanical Quantitative Sensory Testing Outcomes in People With Nonspecific Low Back Pain. J. Orthop. Sports Phys. Ther. 2019, 49, 698–715. [Google Scholar] [CrossRef]
- O’Brien, A.T.; Deitos, A.; Triñanes Pego, Y.; Fregni, F.; Carrillo-de-la-Peña, M.T. Defective Endogenous Pain Modulation in Fibromyalgia: A Meta-Analysis of Temporal Summation and Conditioned Pain Modulation Paradigms. J. Pain 2018, 19, 819–836. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef]
- Granot, M.; Weissman-Fogel, I.; Crispel, Y.; Pud, D.; Granovsky, Y.; Sprecher, E.; Yarnitsky, D. Determinants of endogenous analgesia magnitude in a diffuse noxious inhibitory control (DNIC) paradigm: Do conditioning stimulus painfulness, gender and personality variables matter? Pain 2008, 136, 142–149. [Google Scholar] [CrossRef]
- Mertens, M.G.; Hermans, L.; Crombez, G.; Goudman, L.; Calders, P.; Van Oosterwijck, J.; Meeus, M. Comparison of five conditioned pain modulation paradigms and influencing personal factors in healthy adults. Eur. J. Pain 2021, 25, 243–256. [Google Scholar] [CrossRef]
- Kinser, A.M.; Sands, W.A.; Stone, M.H. Reliability and validity of a pressure algometer. J. Strength. Cond. Res. 2009, 23, 312–314. [Google Scholar] [CrossRef]
- Chesterton, L.S.; Sim, J.; Wright, C.C.; Foster, N.E. Interrater reliability of algometry in measuring pressure pain thresholds in healthy humans, using multiple raters. Clin. J. Pain 2007, 23, 760–766. [Google Scholar] [CrossRef]
- Yarnitsky, D.; Bouhassira, D.; Drewes, A.M.; Fillingim, R.B.; Granot, M.; Hansson, P.; Landau, R.; Marchand, S.; Matre, D.; Nilsen, K.; et al. Recommendations on practice of conditioned pain modulation (CPM) testing. Eur. J. Pain 2015, 19, 805–806. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, D.L.; Kemp, H.I.; Ridout, D.; Yarnitsky, D.; Rice, A.S.C. Reliability of conditioned pain modulation: A systematic review. Pain 2016, 157, 2410–2419. [Google Scholar] [CrossRef] [PubMed]
- Lindstedt, F.; Berrebi, J.; Greayer, E.; Lonsdorf, T.B.; Schalling, M.; Ingvar, M.; Kosek, E. Conditioned Pain Modulation Is Associated with Common Polymorphisms in the Serotonin Transporter Gene. PLoS ONE 2011, 6, E18252. [Google Scholar] [CrossRef] [PubMed]
- Lipton, R.B.; Bigal, M.E.; Ashina, S.; Burstein, R.; Silberstein, S.; Reed, M.L.; Serrano, D.; Stewart, W.F.; American Migraine Prevalence Prevention Advisory Group. Cutaneous allodynia in the migraine population. Ann. Neurol. 2008, 63, 148–158. [Google Scholar] [CrossRef] [PubMed]
- García Campayo, J.; Rodero, B.; Alda, M.; Sobradiel, N.; Montero, J.; Moreno, S. Validation of the Spanish version of the Pain Catastrophizing Scale in fibromyalgia. Med. Clin. 2008, 131, 487–492. [Google Scholar] [CrossRef]
- Andrade Ortega, J.A.; Delgado Martínez, A.D.; Ruiz, R.A. Validation of the Spanish version of the Neck Disability Index. Spine 2010, 35, E114–E118. [Google Scholar] [CrossRef]
- Hita-Contreras, F.; Martínez-López, E.; Latorre-Román, P.A.; Garrido, F.; Santos, M.A.; Martínez-Amat, A. Reliability and validity of the Spanish version of the Pittsburgh Sleep Quality Index (PSQI) in patients with fibromyalgia. Rheumatol. Int. 2014, 34, 929–936. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Vilagut, G.; Ferrer, M.; Rajmil, L.; Rebollo, P.; Permanyer-Miralda, G.; Quintana, J.M.; Santed, R.; Valderas, J.M.; Ribera, A.; Domingo-Salvany, A.; et al. The Spanish version of the Short Form 36 Health Survey: A decade of experience and new developments. Gac. Sanit. 2005, 19, 135–150. [Google Scholar] [CrossRef] [PubMed]
- Portney, L.G.; Watkins, M.P. Foundations of Clinical Research: Applications to Practice. Surv. Ophthalmol. 2002, 47, 598. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- Palacios-Ceña, M.; Gómez-Mayordomo, V.; García-Azorín, D.; González-García, N.; Cuadrado, M.L.; Fernández-De-las-peñas, C.; Arendt-Nielsen, L.; Guerrero, A.L. Dynamic Pressure Pain Hypersensitivity as Assessed by Roller Pressure Algometry in Episodic Cluster Headache. Pain Physician 2020, 23, 219–227. [Google Scholar] [PubMed]
- Arendt-Nielsen, L.; Morlion, B.; Perrot, S.; Dahan, A.; Dickenson, A.; Kress, H.G.; Wells, C.; Bouhassira, D.; Drewes, A.M. Assessment and manifestation of central sensitisation across different chronic pain conditions. Eur. J. Pain 2018, 22, 216–241. [Google Scholar] [CrossRef] [PubMed]
- Guerrero-Peral, Á.; Gómez-Mayordomo, V.; García-Azorín, D.; González-García, N.; Fernández-de-las-Peñas, C.; Arendt-Nielsen, L.; Cuadrado, M.L. Association of dynamic and widespread mechanical sensitivity in cluster headache. Acta Neurol. Belg. 2020, 120, 1265–1270. [Google Scholar] [CrossRef] [PubMed]
- Malo-Urriés, M.; Hidalgo-García, C.; Estébanez-Demiguel, E.; Tricás-Moreno, J.M.; Santos-Lasaosa, S.; Jahanshahi, M. Sensory function in cluster headache: An observational study comparing the symptomatic and asymptomatic sides. Neuropsychiatr. Dis. Treat. 2018, 14, 3363–3371. [Google Scholar] [CrossRef] [PubMed]
- Andersen, S.; Petersen, M.W.; Svendsen, A.S.; Gazerani, P. Pressure pain thresholds assessed over temporalis, masseter, and frontalis muscles in healthy individuals, patients with tension-type headache, and those with migraine-a systematic review. Pain 2015, 156, 1409–1423. [Google Scholar] [CrossRef]
- Fernández-de-las-Peñas, C.; Plaza-Manzano, G.; Navarro-Santana, M.J.; Olesen, J.; Jensen, R.H.; Bendtsen, L. Evidence of localized and widespread pressure pain hypersensitivity in patients with tension-type headache: A systematic review and meta-analysis. Cephalalgia 2021, 41, 256–273. [Google Scholar] [CrossRef]
- Filatova, E.; Latysheva, N.; Kurenkov, A. Evidence of persistent central sensitization in chronic headaches: A multi-method study. J. Headache Pain 2008, 9, 295–300. [Google Scholar] [CrossRef]
- Harte, S.E.; Harris, R.E.; Clauw, D.J. The neurobiology of central sensitization. J. Appl. Biobehav. Res. 2018, 23, e12137. [Google Scholar] [CrossRef]
- Szikszay, T.M.; Lévénez, J.L.M.; Von Selle, J.; Adamczyk, W.M.; Luedtke, K. Investigation of Correlations Between Pain Modulation Paradigms. Pain Med. 2021, 22, 2028–2036. [Google Scholar] [CrossRef] [PubMed]
- Nahman-Averbuch, H.; Timmers, I. Neural mechanisms underlying the conditioned pain modulation response: A narrative review of neuroimaging studies. Pain 2023, 164, E25–E46. [Google Scholar] [CrossRef] [PubMed]
- Harrison, R.; Gandhi, W.; Van Reekum, C.M.; Salomons, T.V. Conditioned pain modulation is associated with heightened connectivity between the periaqueductal grey and cortical regions. Pain Rep. 2022, 7, E999. [Google Scholar] [CrossRef]
- Nahman-Averbuch, H.; Callahan, D.; Darken, R.; Haroutounian, S. Harnessing the conditioned pain modulation response in migraine diagnosis, outcome prediction, and treatment-A narrative review. Headache 2023, 63, 1167–1177. [Google Scholar] [CrossRef]
- Barloese, M.; Lund, N.; Petersen, A.; Rasmussen, M.; Jennum, P.; Jensen, R. Sleep and chronobiology in cluster headache. Cephalalgia 2015, 35, 969–978. [Google Scholar] [CrossRef]
- Pergolizzi, J.V.; Magnusson, P.; LeQuang, J.A.; Wollmuth, C.; Taylor, R.; Breve, F. Exploring the Connection Between Sleep and Cluster Headache: A Narrative Review. Pain Ther. 2020, 9, 359–371. [Google Scholar] [CrossRef]
- Lund, N.L.T.; Petersen, A.S.; Fronczek, R.; Tfelt-Hansen, J.; Belin, A.C.; Meisingset, T.; Tronvik, E.; Steinberg, A.; Gaul, C.; Jensen, R.H. Current treatment options for cluster headache: Limitations and the unmet need for better and specific treatments—A consensus article. J. Headache Pain 2023, 24, 121. [Google Scholar] [CrossRef]
- Stanyer, E.C.; Creeney, H.; Nesbitt, A.D.; Holland, P.R.; Hoffmann, J. Subjective Sleep Quality and Sleep Architecture in Patients With Migraine: A Meta-analysis. Neurology 2021, 97, E1620–E1631. [Google Scholar] [CrossRef] [PubMed]
- Ran, C.; Jennysdotter Olofsgård, F.; Steinberg, A.; Sjöstrand, C.; Waldenlind, E.; Dahlgren, A.; Belin, A.C. Patients with cluster headache show signs of insomnia and sleep related stress: Results from an actigraphy and self-assessed sleep study. J. Headache Pain 2023, 24, 114. [Google Scholar] [CrossRef] [PubMed]
- Ferraro, S.; Nigri, A.; Bruzzone, M.G.; Medina Carrion, J.P.; Fedeli, D.; Demichelis, G.; Chiapparini, L.; Ciullo, G.; Gonzalez, A.A.; Cecchini, A.P.; et al. Involvement of the ipsilateral-to-the-pain anterior-superior hypothalamic subunit in chronic cluster headache. J. Headache Pain 2024, 25, 7. [Google Scholar] [CrossRef] [PubMed]
- Raposio, G.; Raposio, E. Temporal surgery for chronic migraine treatment: A minimally-invasive perspective. Ann. Med. Surg. 2022, 76, 103578. [Google Scholar] [CrossRef]


{kind=link}
| ECH (n = 14) | CCH (n = 22) | Controls (n = 35) | |||
|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | Statistic | p-Value | |
| Age (years) | 50.14 (11.16) | 44.05 (11.88) | 46.31 (12.64) | F = 1.08 | 0.34 |
| BMI (kg/m2) | 25.73 (3.16) | 25.68 (3.22) | 24.96 (2.77) | F = 0.54 | 0.59 |
| Time since diagnosis (years) | 13.86 (8.48) | 9 (6.27) | - | t = 1.97 | 0.06 |
| Pain intensity of attacks (VAS) | 9.21 (1.53) | 8.98 (1.10) | - | t = 0.54 | 0.59 |
| Attack number in one day | 3.07 (1.53) | 2.40 (1.51) | - | t = 1.28 | 0.21 |
| Attack duration (minutes) | 49.07 (39.43) | 51.59 (39.26) | - | t = −0.19 | 0.85 |
| Time since last attack (days) | 165 (413) * | 9.5 (25) * | - | t = 3.66 | <0.01 |
| Pain intensity of last attack (VAS) | 8.93 (2.05) | 8.29 (2.06) | - | t = 0.9 | 0.38 |
| N (%) | N (%) | N (%) | |||
| Sex (males) | 12 (85.7%) | 21 (95.4%) | 32 (91.4%) | X2 = 1.05 | 0.59 |
| Side of attack (right) | 8 (57.1%) | 11 (50.0%) | - | X2 = 0.17 | 0.68 |
| Physical activity (% of sedentary) $ | 7 (20.0%) | 5 (22.7%) | 3 (21.4%) | X2 = 0.35 | 0.98 |
| ECH (n = 14) | CCH (n = 22) | Controls (n = 35) | Controls vs. ECH | Controls vs. CCH | ECH vs. CCH | ||
|---|---|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | Statistic (Effect Size) | Post hoc Analysis—Cohen’s d Effect Size | |||
| PPT (Symptomatic Side) $ | |||||||
| V1 (Ophthalmic Nerve) | 1.00 (0.19) | 0.93 (0.25) | 1.62 (0.36) | F = 44.06 ** (ηp2 = 0.56) | 1.92 ** | 2.14 ** | 0.31 |
| V2 (Maxillary Nerve) | 1.23 (0.22) | 1.21 (0.34) | 2.03 (0.44) | F† = 42.09 ** (ηp2 = 0.55) | 2.04 ** | 2.03 ** | 0.07 |
| MEDIAN NERVE | 6.82 (2.43) | 5.36 (2.17) | 8.08 (1.18) | F† = 14.96 ** (ηp2 = 0.31) | 0.78 | 1.67 ** | 0.64 |
| TIBIALIS ANTERIOR | 6.55 (2.08) | 5.76 (1.91) | 8.56 (1.64) | F = 17.59 ** (ηp2 = 0.34) | 1.13 * | 1.60 ** | 0.40 |
| PPT (Non-Symptomatic Side) # | |||||||
| V1 (Ophthalmic Nerve) | 1.43 (0.33) | 1.24 (0.26) | 1.62 (0.32) | F = 10.57 ** (ηp2 = 0.24) | 0.59 | 1.27 ** | 0.66 |
| V2 (Maxillary Nerve) | 1.56 (0.28) | 1.45 (0.40) | 2.04 (0.44) | F = 16.39 ** (ηp2 = 0.32) | 1.19 ** | 1.39 ** | 0.31 |
| MEDIAN NERVE | 6.65 (2.00) | 5.66 (1.80) | 8.05 (1.57) | F = 13.33 ** (ηp2 = 0.28) | 0.82 * | 1.44 ** | 0.53 |
| TIBIALIS ANTERIOR | 7.28 (1.45) | 6.35 (2.24) | 8.21 (1.40) | F† = 6.76 * (ηp2 = 0.19) | 0.66 | 1.05 ** | 0.47 |
| TSM (Symptomatic Side) $ | |||||||
| V1 (Ophthalmic Nerve) | 2.21 (1.86) | 2.44 (1.25) | 1.52 (0.91) | F† = 4.74 * (ηp2 = 0.11) | 0.55 | 0.87 * | 0.15 |
| V2 (Maxillary Nerve) | 2.97 (1.99) | 2.82 (1.61) | 1.81 (1.01) | F† = 4.93 * (ηp2 = 0.13) | 0.86 * | 0.79 * | 0.08 |
| MEDIAN NERVE | 2.06 (1.51) | 1.68 (1.31) | 1.15 (0.71) | F† = 3.36 * (ηp2 = 0.10) | 0.91 * | 0.54 | 0.27 |
| TIBIALIS ANTERIOR | 1.49 (1.92) | 0.63 (0.54) | 0.46 (0.59) | F† = 2.29 * (ηp2 = 0.14) | 0.91 * | 0.30 | 0.68 * |
| TSM (Non-Symptomatic Side) # | |||||||
| V1 (Ophthalmic Nerve) | 2.24 (1.68) | 1.94 (1.25) | 1.29 (0.77) | F† = 3.88 * (ηp2 = 0.11) | 0.86 * | 0.66 | 0.21 |
| V2 (Maxillary Nerve) | 3.06 (2.28) | 2.48 (1.82) | 1.64 (0.98) | F† = 3.96 * (ηp2 = 0.12) | 0.97 * | 0.62 | 0.29 |
| MEDIAN NERVE | 1.84 (1.38) | 1.54 (1.24) | 0.95 (0.76) | F† = 3.94 * (ηp2 = 0.11) | 0.92 * | 0.61 | 0.23 |
| TIBIALIS ANTERIOR | 0.86 (1.13) | 0.60 (0.64) | 0.55 (0.62) | F† = 0.47 (ηp2 = 0.02) | 0.39 | 0.08 | 0.30 |
| CPM Effect (Symptomatic Side) $ | |||||||
| V1 (Ophthalmic Nerve) | 0.04 (0.10) | 0.06 (0.08) | 0.25 (0.13) | F† = 26.76 ** (ηp2 = 0.44) | 1.64 ** | 1.67 ** | 0.15 |
| TIBIALIS ANTERIOR | 0.35 (1.18) | 0.43 (0.67) | 0.74 (0.69) | F = 1.65 (ηp2 = 0.05) | 0.46 | 0.46 | 0.08 |
| CPM Effect (Non-Symptomatic Side) # | |||||||
| V1 (Ophthalmic Nerve) | 0.23 (0.13) | 0.10 (0.11) | 0.24 (0.18) | F† = 7.42 * (ηp2 = 0.14) | 0.05 | 0.86 * | 1.03 |
| TIBIALIS ANTERIOR | 0.84 (1.5) | 0.29 (0.51) | 0.98 (0.94) | F† = 6.56 * (ηp2 = 0.09) | 0.12 | 0.85 * | 0.54 |
| CPM % of change (Symptomatic Side) $ | |||||||
| V1 (Ophthalmic Nerve) | 0.05 (0.10) | 0.07 (0.10) | 0.15 (0.09) | F = 8.59 ** (ηp2 = 0.20) | 1.16 * | 0.87 * | 0.25 |
| TIBIALIS ANTERIOR | 0.08 (0.22) | 0.09 (0.14) | 0.08 (0.08) | F† = 0.04 (ηp2 < 0.01) | 0.02 | 0.08 | 0.07 |
| CPM % of change (Non-Symptomatic Side) # | |||||||
| V1 (Ophthalmic Nerve) | 0.16 (0.09) | 0.09 (0.09) | 0.14 (0.09) | F = 2.80 (ηp2 = 0.08) | 0.23 | 0.50 | 0.77 |
| TIBIALIS ANTERIOR | 0.14 (0.21) | 0.07 (0.09) | 0.11 (0.10) | F† = 1.58 (ηp2 = 0.04) | 0.14 | 0.44 | 0.44 |
| ECH (n = 14) (S) Side | ECH (n = 14) (NS) Side | Statistic | |||
|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | t Student | Effect Size | ||
| PPT | V1 (Ophthalmic Nerve) | 1 (0.19) | 1.43 (0.33) | 5.84 ** | d = 1.6 |
| V2 (Maxillary Nerve) | 1.23 (0.22) | 1.57 (0.28) | 3.62 * | d = 1.35 | |
| MEDIAN NERVE | 6.82 (2.43) | 6.65 (2.00) | 0.39 | d = 0.08 | |
| TIBIALIS ANTERIOR | 6.55 (2.08) | 7.28 (1.45) | 1.88 | d = 0.41 | |
| TSM | V1 (Ophthalmic Nerve) | 2.21 (1.86) | 2.24 (1.69) | 0.09 | d = 0.02 |
| V2 (Maxillary Nerve) | 2.97 (1.99) | 3.06 (2.28) | 0.3 | d = 0.04 | |
| MEDIAN NERVE | 2.06 (1.51) | 1.84 (1.38) | 1.11 | d = 0.15 | |
| TIBIALIS ANTERIOR | 1.49 (1.92) | 0.86 (1.13) | 1.41 | d = 0.4 | |
| CPM EFFECT | V1 (Ophthalmic Nerve) | 0.04 (0.10) | 0.23 (0.13) | 5.27 ** | d = 1.55 |
| TIBIALIS ANTERIOR | 0.354 (1.17) | 0.84 (1.49) | 1.25 | d = 0.36 | |
| CPM % OF CHANGE | V1 (Ophthalmic Nerve) | 0.09 (0.10) | 0.16 (0.09) | 4.08 ** | d = 1.23 |
| TIBIALIS ANTERIOR | 0.08 (0.22) | 0.14 (0.21) | 0.91 | d = 0.25 | |
| CCH (n = 22) (S) Side | CCH (n = 22) (NS) Side | Statistic | |||
|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | t Student | Effect Size | ||
| PPT | V1 (Ophthalmic Nerve) | 0.93 (0.25) | 1.24 (0.26) | 8.57 ** | d = 1.22 |
| V2 (Maxillary Nerve) | 1.21 (0.34) | 1.45(0.4) | 3.25 * | d = 0.65 | |
| MEDIAN NERVE | 5.36 (2.17) | 5.66 (1.8) | 1.13 | d = 0.15 | |
| TIBIALIS ANTERIOR | 5.76 (1.91) | 6.35 (2.24) | 2.77 * | d = 0.28 | |
| TSM | V1 (Ophthalmic Nerve) | 2.44 (1.25) | 1.94 (1.25) | 2.22* | d = 0.4 |
| V2 (Maxillary Nerve) | 2.82 (1.61) | 2.48 (1.82) | 1.28 | d = 0.2 | |
| MEDIAN NERVE | 1.68 (1.31) | 1.54 (1.24) | 0.59 | d = 0.11 | |
| TIBIALIS ANTERIOR | 0.63 (0.54) | 0.60 (0.64) | 0.25 | d = 0.05 | |
| CPM EFFECT | V1 (Ophthalmic Nerve) | 0.06 (0.08) | 0.10 (0.11) | 1.79 | d = 0.47 |
| TIBIALIS ANTERIOR | 0.43 (0.67) | 0.29 (0.51) | 0.97 | d = 0.23 | |
| CPM % OF CHANGE | V1 (Ophthalmic Nerve) | 0.07 (0.10) | 0.09 (0.09) | 0.78 | d = 0.2 |
| TIBIALIS ANTERIOR | 0.09 (0.14) | 0.07 (0.10) | 0.78 | d = 0.19 | |
| ECH (n = 14) | CCH (n = 22) | Controls (n = 35) | Controls vs. ECH | Controls vs. CCH | ECH vs. CCH | ||
|---|---|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | Statistic (Effect Size) | Post hoc Analysis—Cohen’s d Effect Size | |||
| ASC | 4.29 (3.79) | 4.55 (3.49) | - | t = −0.21 (d = 0.07) | - | - | - |
| PCS | 35.57 (9.85) | 31.32 (8.36) | - | t = 1.39 (d = 0.47) | - | - | - |
| NDI | 6.07 (7.24) | 9.64 (7.59) | - | t = −1.4 (d = 0.48) | - | - | - |
| PSQI | 6.86 (3.92) | 9.45 (4.94) | 4.34 (2.15) | F† = 11.79 ** (ηp2 = 0.29) | 0.91 | 1.46 ** | 0.57 |
| PCS-12 | 47.94 (9.36) | 40.53 (10.86) | 52.81 (4.13) | F† = 13.62 ** (ηp2 = 0.33) | 0.81 | 1.65 ** | 0.72 * |
| MCS-12 | 52.01 (8.57) | 47.10 (11.86) | 51.92 (4.02) | F† = 1.66 (ηp2 = 0.07) | 0.02 | 0.6 | 0.46 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bertotti, G.; Elizagaray-García, J.I.; Rodríguez-Vico, J.; Gil-Martínez, A. Hyperalgesia, Increased Temporal Summation and Impaired Inhibitory Mechanisms in Episodic and Chronic Cluster Headache: An Observational Study. Biomedicines 2024, 12, 374. https://doi.org/10.3390/biomedicines12020374
Bertotti G, Elizagaray-García JI, Rodríguez-Vico J, Gil-Martínez A. Hyperalgesia, Increased Temporal Summation and Impaired Inhibitory Mechanisms in Episodic and Chronic Cluster Headache: An Observational Study. Biomedicines. 2024; 12(2):374. https://doi.org/10.3390/biomedicines12020374
Chicago/Turabian StyleBertotti, Gabriele, Juan Ignacio Elizagaray-García, Jaime Rodríguez-Vico, and Alfonso Gil-Martínez. 2024. "Hyperalgesia, Increased Temporal Summation and Impaired Inhibitory Mechanisms in Episodic and Chronic Cluster Headache: An Observational Study" Biomedicines 12, no. 2: 374. https://doi.org/10.3390/biomedicines12020374
APA StyleBertotti, G., Elizagaray-García, J. I., Rodríguez-Vico, J., & Gil-Martínez, A. (2024). Hyperalgesia, Increased Temporal Summation and Impaired Inhibitory Mechanisms in Episodic and Chronic Cluster Headache: An Observational Study. Biomedicines, 12(2), 374. https://doi.org/10.3390/biomedicines12020374