
Clinical Effects of Oral Bacteriotherapy on Anal HPV Infection and Related Dysplasia in HIV-Positive MSM: Results from the “HPVinHIV” Trial

 ,
,  ,
,  , , , , , and
, , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
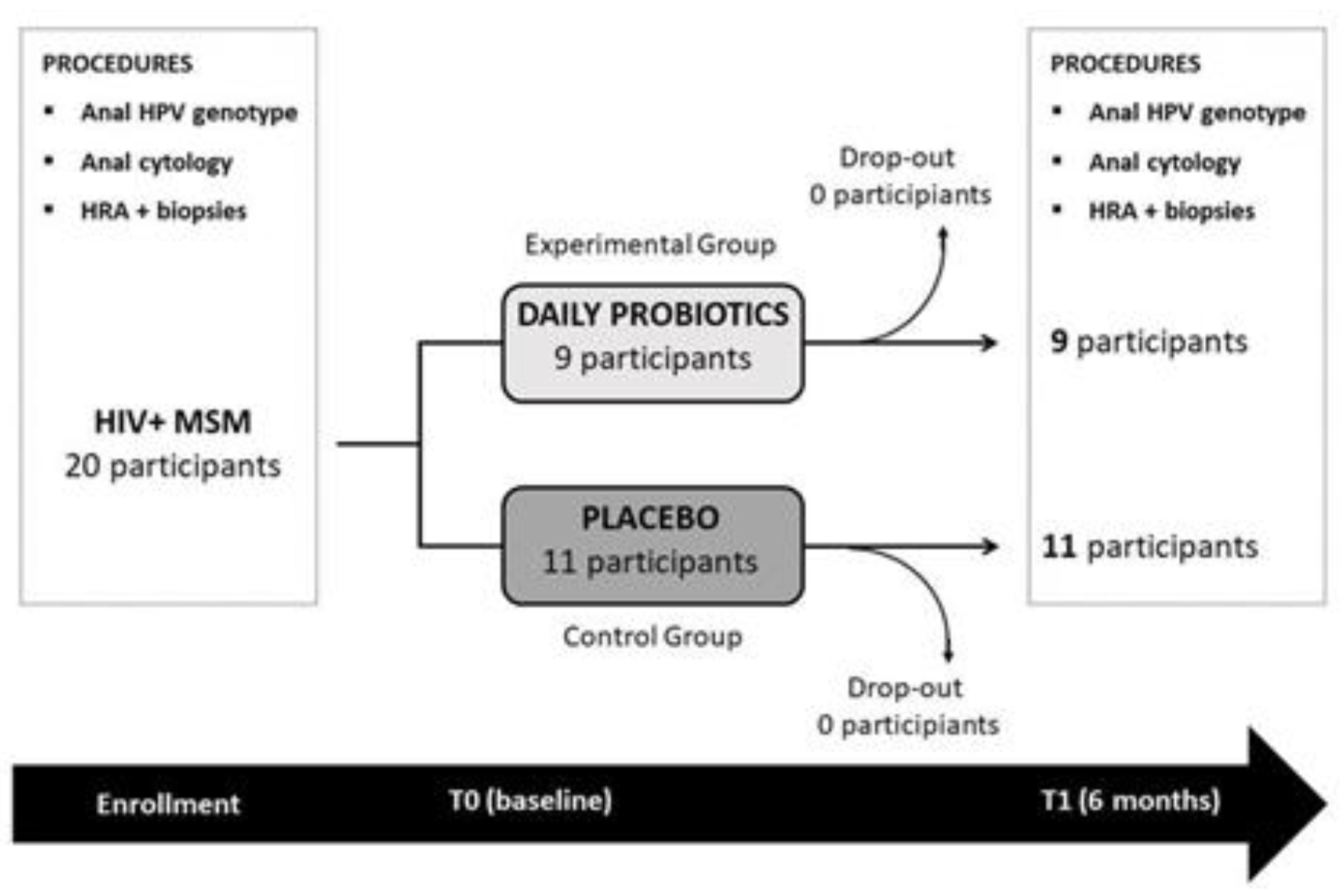
2.1. Study Design and Outcomes
2.2. Eligibility and Enrollment Criteria
2.3. Study Procedures
2.4. Probiotic Compound and Placebo
2.5. Statistical Analysis
2.6. Ethical Aspects
3. Results
3.1. Baseline Characteristics of Participants
3.2. End of Study Results (T1)
3.2.1. Effects of Modulation of Gut Flora on Anal HPV Infection in HIV-Positive MSM
3.2.2. Effects of Modulation of Gut Flora on Anal Dysplasia in HIV-Positive MSM Anal Cytology
3.2.3. HRA and Histology Results
3.2.4. Safety and Tolerability of Oral Bacteriotherapy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Squamous cell carcinoma of the anus | SCCA |
| Human Papilloma Virus | HPV |
| low grade squamous intraepithelial lesions | LSIL |
| high grade squamous intraepithelial lesions | HSIL |
| men having sex with men | MSM |
| randomized controlled trial | RCT |
| highly active anti-retroviral therapy | HAART |
| high resolution anoscopy | HRA |
| nucleoside reverse transcriptase inhibitors | NRTI |
| integrase strand transfer inhibitors | INSTI |
| non nucleoside reverse transcriptase inhibitors | NNRTI |
| protease inhibitors | PI |
References
- Kjaer, S.K.; van den Brule, A.J.; Bock, J.E.; Poll, P.A.; Engholm, G.; Sherman, M.E.; Walboomers, J.M.; Meijer, C.J. Human papillomavirus-the most significant risk determinant of cervical intraepithelial neoplasia. Int. J. Cancer 1996, 65, 601–606. [Google Scholar] [CrossRef]
- Schiffman, M.; Bauer, H.M.; Hoover, R.; Glass, A.G.; Cadell, D.M.; Rush, B.B.; Scott, D.R.; Sherman, M.; Kurman, R.; Wacholder, S.C.; et al. Epidemiologic evidence showing the HPV infection causes most cervical intraepithelial neoplasia. J. Natl. Cancer Inst. 1993, 85, 958–964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moscicki, A.B.; Ma, Y.; Farhat, S.; Jay, J.; Hanson, E.; Benningfield, S.; Jonte, J.; Godwin-Medina, C.; Wilson, R.; Shiboski, S. Natural history of anal Human Papillomavirus infection in heterosexual women and risks associated with persistence. Clin. Infect. Dis. 2014, 15, 804–811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellerbrock, T.V.; Chiasson, M.A.; Bush, T.J.; Sun, X.W.; Sawo, D.; Brudney, K.; Wright, T.C. Incidence of cervical squamous intraepithelial lesions in HIV-infected women. JAMA 2000, 23, 1031–1037. [Google Scholar] [CrossRef] [Green Version]
- Mandelblatt, J.S.; Fahs, M.; Garibaldi, K.; Senie, R.T.; Peterson, H.B. Association between HIV infection and cervical neoplasia: Implications for clinical care of women at risk for both conditions. AIDS 1992, 6, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Palefsky, J.M.; Minkoff, H.; Kalish, L.A.; Levine, A.; Sacks, H.S.; Garcia, P.; Young, M.; Melnick, S.; Miotti, P.; Burk, R. Cervicovaginal human papillomavirus infection in human immunodeficiency virus-1 (HIV)-positive and high-risk HIV-negative women. J. Natl. Cancer Inst. 1999, 3, 226–236. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.J.; Palefsky, J.M. HPV-Associated Anal Cancer in the HIV/AIDS Patient. Cancer Treat Res. 2019, 177, 183–209. [Google Scholar] [CrossRef]
- Wu, P.F.; Hang, J.F.; Strong, C.; Chen, S.J.; Lin, L.Y.; Chen, S.S.; Lai, C.R.; Ku, S.W.; Lee, M.H. Anal human papillomavirus and its associations with abnormal anal cytology among men who have sex with men. Sci Rep. 2020, 21, 3165. [Google Scholar] [CrossRef] [Green Version]
- Hanson, L.; Vande, V.L.; Jermé, M.; Abad, C.L.; Safdar, N. Probiotics for Treatment and Prevention of Urogenital Infections in Women: A Systematic Review. J. Midwifery Womens Health 2016, 61, 339–355. [Google Scholar] [CrossRef]
- MacPhee, R.A.; Hummelen, R.; Bisanz, J.E.; Miller, W.L.; Reid, G. Probiotic strategies for the treatment and prevention of bacterial vaginosis. Expert Opin. Pharmacother. 2010, 11, 2985–2995. [Google Scholar] [CrossRef]
- Reid, G.; Dols, J.; Miller, W. Targeting the vaginal microbiota with probiotics as a means to counteract infections. Curr. Opin. Clin. Nutr. Metab. Care 2009, 12, 583–587. [Google Scholar] [CrossRef]
- Spurbeck, R.; Arvidson, C.G. Lactobacilli at the front line of defence against vaginally acquired infections. Future Microbiol. 2011, 6, 567–582. [Google Scholar] [CrossRef] [PubMed]
- Bolton, M.; van der Straten, A.; Cohen, C.R. Probiotics: Potential to prevent HIV and sexually transmitted infections in women. Sex Transm. Dis. 2008, 35, 214–225. [Google Scholar] [CrossRef]
- Verhoeven, V.; Renard, N.; Makar, A.; Van Royen, P.; Bogers, J.P.; Lardon, F.; Baay, M. Probiotics enhance the clearance of human papillomavirus-related cervical lesions: A prospective controlled pilot study. Eur. J. Cancer Prev. 2013, 22, 46–51. [Google Scholar] [CrossRef]
- Palma, E.; Recine, N.; Domenici, L.; Giorgini, M.; Pierangeli, A.; Panici, P.B. Long-term Lactobacillus rhamnosus BMX 54 application to restore a balanced vaginal ecosystem: A promising solution against HPV-infection. BMC Infect Dis. 2018, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiong, Y.; Cui, L.; Bian, C.; Zhao, X.; Wang, X. Clearance of human papillomavirus infection in patients with cervical intraepithelial neoplasia: A systemic review and meta-analysis. Medicine 2020, 13, e23155. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.D.; Xu, D.J.; Wang, B.Y.; Yan, D.H.; Lv, Z.; Su, J.R. Inhibitory Effect of Vaginal Lactobacillus Supernatants on Cervical Cancer Cells. Probiotics Antimicrob. Proteins 2018, 10, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Abdolalipour, E.; Mahooti, M.; Salehzadeh, A.; Torabi, A.; Mohebbi, S.R.; Gorji, A.; Ghaemi, A. Evaluation of the antitumor immune responses of probiotic Bifidobacterium bifidum in human papillomavirus-induced tumor model. Microb. Pathog. 2020, 145, 104207. [Google Scholar] [CrossRef] [PubMed]
- Abdolalipour, E.; Mahooti, M.; Gorji, A.; Ghaemi, A. Synergistic Therapeutic Effects of Probiotic Lactobacillus casei TD-2 Consumption on GM-CSF-Induced Immune Responses in a Murine Model of Cervical Cancer. Nutr. Cancer. 2020, 26, 1–11. [Google Scholar] [CrossRef]
- Zevin, A.S.; McKinnon, L.; Burgener, A. Microbial translocation and microbiome dysbiosis in HIV-associated immune activation. Curr. Opin. HIV AIDS 2016, 11, 182–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vujkovic-Cvijin, I.; Dunham, R.M.; Iwai, S. Dysbiosis of the gut microbiota is associated with HIV disease progression and tryptophan catabolism. Sci. Transl. Med. 2013, 5, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dillon, S.M.; Lee, E.J.; Kotter, C.V. An altered intestinal mucosal microbiome in HIV-1 infection is associated with mucosal and systemic immune activation and endotoxemia. Mucosal Immunol. 2014, 7, 983–994. [Google Scholar] [CrossRef] [Green Version]
- Brenchley, J.M.; Price, D.A.; Schacker, T.W. Microbial translocation is a cause of systemic immune activation in chronic HIV infection. Nat. Med. 2006, 12, 1365–1371. [Google Scholar] [CrossRef] [Green Version]
- Ceccarelli, G.; Cavallari, E.N.; Savinelli, S.; Bianchi, L.; Pierangeli, A.; Vullo, F.; Ciardi, A.; D'ettorre, G. Clearance of human papillomavirus related anal condylomas after oral and endorectal multistrain probiotic supplementation in an HIV positive male: A case report. Medicine 2018, 97, e0329. [Google Scholar] [CrossRef] [PubMed]
- Verteramo, R.; Pierangeli, A.; Mancini, E.; Calzolari, E.; Bucci, M.; Osborn, J.; Nicosia, R.; Chiarini, F.; Antonelli, G.; Degener, A.M. Human papillomaviruses and genital co-infections in gynecological outpatients. BMC Infect. Dis. 2009, 9, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, S.; Bunge, E.; Bakker, M.; Castellsagué, X. The incidence, clearance and persistence of non-cervical human papillomavirus infections: A systematic review of the literature. BMC Infect Dis. 2016, 14, 293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darragh, T.M.; Colgan, T.J.; Cox, J.T.; Heller, D.S.; Henry, M.R.; Luff, R.D.; McCalmont, T.; Nayar, R.; Palefsky, J.M.; Stoler, M.H.; et al. Members of LAST Project Work Groups. The Lower Anogenital Squamous Terminology Standardization Project for HPV-Associated Lesions: Background and consensus recommendations from the College of American Pathologists and the American Society for Colposcopy and Cervical Pathology. Arch. Pathol. Lab. Med. 2012, 136, 1266–1297. [Google Scholar] [CrossRef] [PubMed]
- Hillman, R.J.; Cuming, T.; Darragh, T.; Nathan, M.; Berry-Lawthorn, M.; Goldstone, S.; Law, C.; Palefsky, J.; Barroso, L.F.; Stier, E.A.; et al. 2016 IANS International Guidelines for Practice Standards in the Detection of Anal Cancer Precursors. J. Low Genit. Tract. Dis. 2016, 20, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Clifford, G.M.; Georges, D.; Shiels, M.S.; Engels, E.A.; Albuquerque, A.; Poynten, I.M.; de Pokomandy, A.; Stier, E.A. A meta-analysis of anal cancer incidence by risk group: Toward a unified anal cancer risk scale. Int. J. Cancer. 2021, 148, 38–47. [Google Scholar] [CrossRef]
- Palefsky, J.M.; Lensing, S.Y.; Belzer, M.; Lee, J.; Gaur, A.H.; Mayer, K.; Futterman, D.; Stier, A.; Paul, M.E.; Chiao, E.Y.; et al. High Prevalence of Anal High-Grade Squamous Intraepithelial Lesions, and Prevention Through Human Papillomavirus Vaccination, in Young Men Who Have Sex With Men Living With Human Immunodeficiency Virus. Clin. Infect. Dis. 2021, 15, 434. [Google Scholar] [CrossRef]
- Wieland, U.; Kreuter, A. One step towards standardized management of anal dysplasia. Lancet Oncol. 2013, 14, 273–274. [Google Scholar] [CrossRef]
- Liu, J.; Williams, B.; Frank, D.; Dillon, S.M.; Wilson, C.C.; Landay, A.L. Inside Out: HIV, the Gut Microbiome, and the Mucosal Immune System. J. Immunol. 2017, 198, 605–614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceccarelli, G.; Statzu, M.; Santinelli, L.; Pinacchio, C.; Bitossi, C.; Cavallari, E.N.; Vullo, V.; Scagnolari, C.; d’Ettorre, G. Challenges in the management of HIV infection: Update on the role of probiotic supplementation as a possible complementary therapeutic strategy for cART treated people living with HIV/AIDS. Expert Opin. Biol. Ther. 2019, 19, 949–965. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Experimental Group | Control Group | p-Value | |
|---|---|---|---|
| Participants | 9 | 11 | |
| Age | 44 (35–49.5) | 55 (50–58) | 0.010 |
| Diabetes | 0 | 1 (9%) | 0.341 |
| Cigarette smokers | 3 (33%) | 6 (55%) | 0.367 |
| Anal receptive intercourse | 9 (100%) | 11 (100%) | 1 |
| Lifetime sexual partners | 100 (100–150) | 50 (40–250) | 0.341 |
| HPV vaccination | 0 | 0 | 1.000 |
| Years from HIV diagnosis | 12 (10–14) | 18 (10.5–25.5) | 0.081 |
| T CD4 nadir (cells/μL) | 460 (350–532) | 262 (113–406) | 0.387 |
| T CD4 baseline (cells/μL) | 877 (700–936) | 700 (540–897) | 0.606 |
| Treatment with NRTI | 8 (89%) | 9 (82%) | 0.673 |
| Treatment with INSTI | 4 (44%) | 8 (73%) | 0.227 |
| Treatment with NNRTI | 5 (56%) | 3 (27%) | 0.227 |
| Treatment with PI | 1 (11%) | 2 (18%) | 0.673 |
| High risk HPV | 6 (67%) | 5 (45%) | 0.367 |
| Anal condyloma | 2 (22%) | 1 (9%) | 0.656 |
| Number of SIL (histology) | 1 (1–2) | 2 (1–3) | 0.714 |
| Participants with HSIL (histology) | 1 (11%) | 0 | 0.317 |
| Experimental Group | Control Group | p-Value | |
|---|---|---|---|
| HPV clearance | 6 (67%) | 2 (18%) | 0.067 |
| High risk HPV T1 | 3 (33%) | 6 (55%) | 0.367 |
| Number of SIL (histology) | 1 (0–1) | 2 (2–4) | 0.053 |
| Participants with normal HRA | 3 (33%) | 0 | 0.230 |
| Participants with regression of at least 1 SIL | 8 (88%) | 1 (9%) | 0.002 |
| Participants with persistent and worsened SIL | 1 (11%) | 7 (78%) | 0.004 |
| Participants with onset of new SIL | 2 (22%) | 8 (73%) | 0.023 |
| Participants with HSIL (histology) | 0 | 3 (27%) | 0.083 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cavallari, E.N.; Ceccarelli, G.; Santinelli, L.; Innocenti, G.P.; De Girolamo, G.; Borrazzo, C.; Spagnolello, O.; Scagnolari, C.; Arcieri, S.; Ciardi, A.; et al. Clinical Effects of Oral Bacteriotherapy on Anal HPV Infection and Related Dysplasia in HIV-Positive MSM: Results from the “HPVinHIV” Trial. Biomedicines 2021, 9, 1738. https://doi.org/10.3390/biomedicines9111738
Cavallari EN, Ceccarelli G, Santinelli L, Innocenti GP, De Girolamo G, Borrazzo C, Spagnolello O, Scagnolari C, Arcieri S, Ciardi A, et al. Clinical Effects of Oral Bacteriotherapy on Anal HPV Infection and Related Dysplasia in HIV-Positive MSM: Results from the “HPVinHIV” Trial. Biomedicines. 2021; 9(11):1738. https://doi.org/10.3390/biomedicines9111738
Chicago/Turabian StyleCavallari, Eugenio Nelson, Giancarlo Ceccarelli, Letizia Santinelli, Giuseppe Pietro Innocenti, Gabriella De Girolamo, Cristian Borrazzo, Ornella Spagnolello, Carolina Scagnolari, Stefano Arcieri, Antonio Ciardi, and et al. 2021. "Clinical Effects of Oral Bacteriotherapy on Anal HPV Infection and Related Dysplasia in HIV-Positive MSM: Results from the “HPVinHIV” Trial" Biomedicines 9, no. 11: 1738. https://doi.org/10.3390/biomedicines9111738
APA StyleCavallari, E. N., Ceccarelli, G., Santinelli, L., Innocenti, G. P., De Girolamo, G., Borrazzo, C., Spagnolello, O., Scagnolari, C., Arcieri, S., Ciardi, A., Pierangeli, A., Mastroianni, C. M., & d’Ettorre, G. (2021). Clinical Effects of Oral Bacteriotherapy on Anal HPV Infection and Related Dysplasia in HIV-Positive MSM: Results from the “HPVinHIV” Trial. Biomedicines, 9(11), 1738. https://doi.org/10.3390/biomedicines9111738