Acute Disseminated Encephalomyelitis: Current Perspectives

 , and
, and 
Abstract
:1. Brief Introduction and Historical Perspective
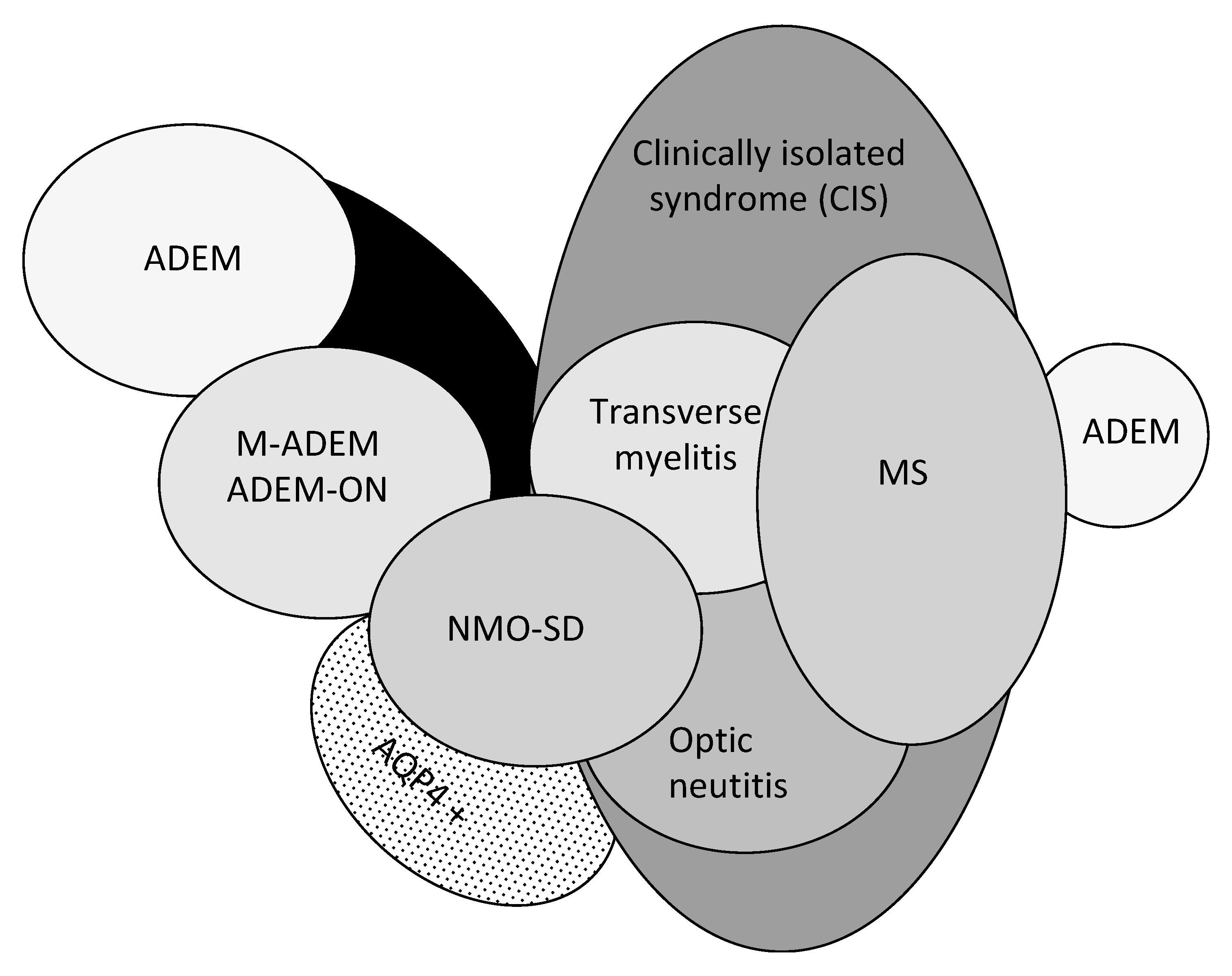
2. ADEM in the Context of ADS
3. Epidemiology
4. Clinical and Radiological Perspective
4.1. Diagnostic Criteria
4.2. Clinical Features
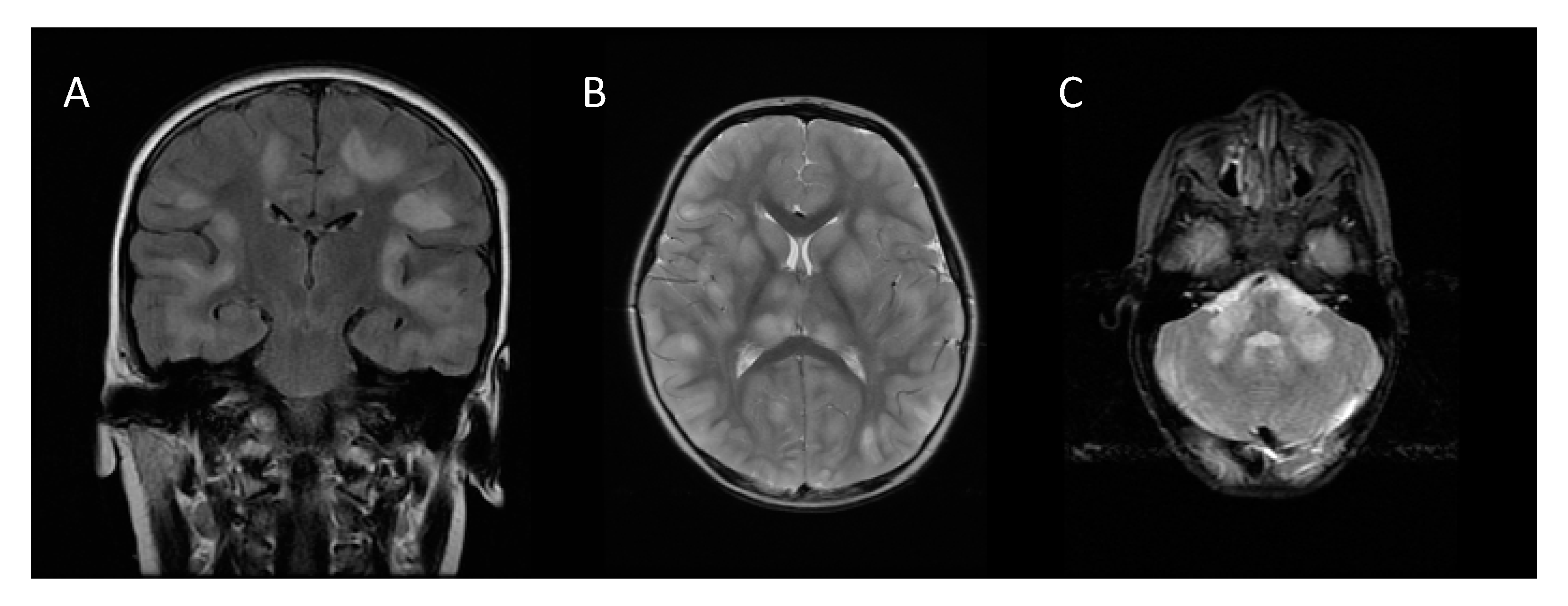
4.3. MRI Findings
4.4. Laboratory Findings
4.5. Differential Diagnosis
4.6. Comparison between Children and Adults
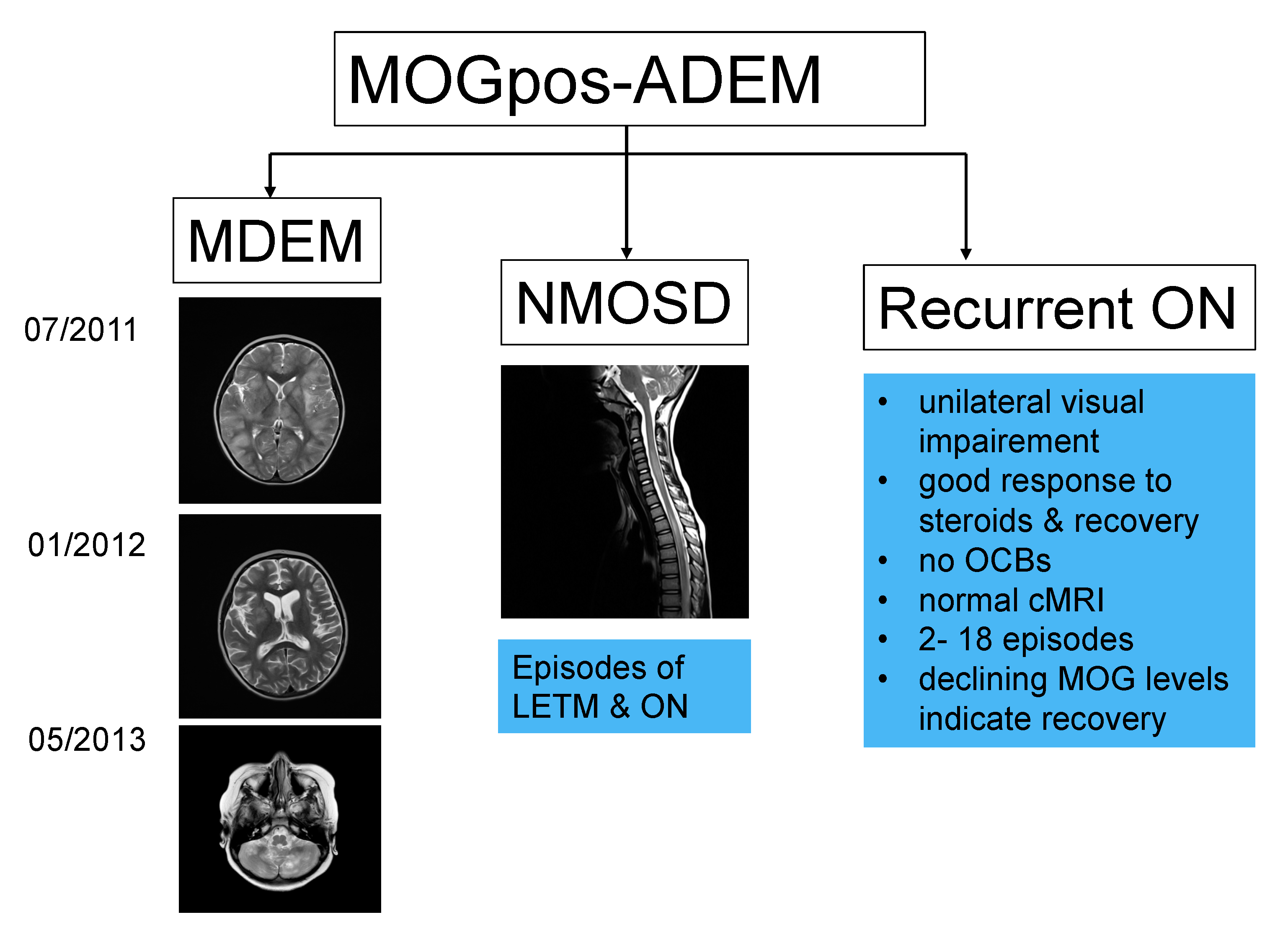
5. MOG in Monophasic and Relapsing Forms of ADEM
5.1. MDEM
5.2. ADEM-ON
5.3. ADEM-NMOSD
6. Pathology and Immunopathogenesis
7. Treatment and Outcome
7.1. Acute Phase Treatment
7.2. Relapsing Forms
7.3. Outcome
8. Future Directions
Author Contributions
Funding
Conflicts of Interest
References
- Pohl, D.; Alper, G.; Haren, K.V.; Kornberg, A.J.; Lucchinetti, C.F.; Tenembaum, S.; Belman, A.L. Acute disseminated encephalomyelitis. Updates on an inflammatory CNS syndrome. Neurology 2016, 87 (Suppl. 2), S38–S45. [Google Scholar] [CrossRef] [PubMed]
- Belman, A.L.; Hertz, D.; Hanefeld, F. Introduction: Historical perspective of pediatric multiple sclerosis and related disorders. In Demyelinating Disorders of the Central Nervous System in Childhood; Chabas, D., Waubant, E.L., Eds.; Cambridge University Press: New York, USA, 2011; pp. 1–9. [Google Scholar]
- Krupp, L.B.; Banwell, B.; Tenembaum, S. Consensus definitions proposed for pediatric multiple sclerosis and related disorders. Neurology 2007, 68 (Suppl. 2), S7–S12. [Google Scholar] [CrossRef]
- Krupp, L.B.; Tardieu, M.; Amato, M.P.; Banwell, B.; Chitnis, T.; Dale, R.C.; Ghezzi, A.; Hintzen, R.; Kornberg, A.; Pohl, D.; et al. International pediatric multiple sclerosis study group criteria for pediatric multiple sclerosis and immune-mediated central nervous system demyelinating disorders: Revisions to the 2007 definitions. Mult. Scler. 2013, 19, 1261–1267. [Google Scholar] [CrossRef] [PubMed]
- Granerod, J.; Davies, N.W.S.; Mukonoweshuro, W.; Mehta, A.; Das, K.; Lim, M.; Solomong, T.; Biswas, S.; Rosella, L.; Brown, D.W.G.; et al. Neuroimaging in encephalitis: Analysis of imaging findings and interobserver agreement. Clin. Radiol. 2016, 71, 1050–1058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hardy, T.A. How should we diagnose acute disseminated encephalomyelitis? Dev. Med. Child Neurol. 2018, 60, 1070. [Google Scholar] [CrossRef]
- Boesen, M.S.; Blinkenberg, M.; Koch-Henriksen, N.; Thygesen, L.C.; Uldall, P.V.; Magyari, M.; Born, A.P. Implications of the international paediatric multiple sclerosis study group consensus criteria for paediatric acute disseminated encephalomyelitis: A nationwide validation study. Dev. Med. Child Neurol. 2018, 60, 1123–1131. [Google Scholar] [CrossRef] [Green Version]
- Wong, Y.Y.M.; Hacohen, Y.; Armangue, T.; Wassmer, E.; Verhelst, H.; Hemingway, C.; van Pelt, E.D.; Catsman-Berrevoets, C.E.; Hintzen, P.Q.; Deiva, K.; et al. Paediatric acute disseminated encephalomyelitis followed by optic neuritis: Disease course, treatment response and outcome. Eur. J. Neurol. 2018, 25, 782–786. [Google Scholar] [CrossRef]
- Hacohen, Y.; Mankad, K.; Chong, W.K.; Barkhof, F.; Vincent, A.; Lim, M.; Wassmer, E.; Ciccarelli, O.; Hemingway, C. Diagnostic algorithm for relapsing acquired demyelinating syndromes in children. Neurology 2017, 89, 1–10. [Google Scholar] [CrossRef]
- Armangue, T.; Olivé-Cirera, G.; Martínez-Hernandez, E.; Sepulveda, M.; Ruiz-Garcia, R.; Muñoz-Batista, M.; Ariño, H.; González-Álvarez, V.; Felipe-Rucián, A.; Martínez-González, M.J.; et al. Associations of paediatric demyelinating and encephalitic syndromes with myelin oligodendrocyte glycoprotein antibodies: A multicentre observational study. Lancet Neurol. 2020, 19, 234–246. [Google Scholar] [CrossRef]
- Hacohen, Y.; Wong, Y.Y.; Lechner, C.; Jurynczyk, M.; Wright, S.; Konuskan, B.; Kalser, J.; Poulat, A.L.; Maurey, H.; Ganelin-Cohen, E.; et al. Disease course and treatment responses in children with relapsing myelin oligodendrocyte glycoprotein antibody–associated disease. JAMA Neurol. 2018, 75, 478–487. [Google Scholar] [CrossRef] [PubMed]
- Waters, P.; Fadda, G.; Woodhall, M.; O’Mahony, J.; Brown, R.A.; Castro, D.A.; Longoni, G.; Irani, S.R.; Sun, B.; Yeh, E.A.; et al. Serial anti–myelin oligodendrocyte glycoprotein antibody analyses and outcomes in children with demyelinating syndromes. JAMA Neurol. 2020, 77, 82–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, E.; Hacohen, Y.; Waldman, A.; Tillema, J.M.; Soldatos, A.; Ances, B.; Benseler, S.; Bielekova, B.; Dale, R.C.; Dalmau, J.; et al. Neuroimmune disorders of the central nervous system in children in the molecular era. Nat. Rev. Neurol. 2018, 14, 433–445. [Google Scholar] [CrossRef] [PubMed]
- Tenembaum, S.; Chamoles, N.; Fejerman, N. Acute disseminated encephalomyelitis. A long-term follow-up study of 84 pediatric patients. Neurology 2002, 59, 1224–1231. [Google Scholar] [CrossRef]
- Hahn, C.D.; Miles, B.S.; MacGregor, D.L.; Blaser, S.I.; Banwell, B.L.; Hetherington, C.R. Neurocognitive outcome after acute disseminated encephalomyelitis. Pediatric Neurol. 2003, 29, 117–123. [Google Scholar] [CrossRef]
- Neuteboom, R.; Wilbur, C.; Van Pelt, D.; Rodriguez, M.; Yeh, A. The spectrum of inflammatory acquired demyelinating syndromes in children. Semin. Pediatric Neurol. 2017, 24, 189–200. [Google Scholar] [CrossRef]
- Banwell, B.; Kennedy, J.; Sadovnick, D.; Arnold, D.L.; Magalhaes, S.; Wambera, K.; Connolly, M.B.; Yager, J.; Mah, J.K.; Shah, N.; et al. Incidence of acquired demyelination of the CNS in Canadian children. Neurology 2009, 72, 232–239. [Google Scholar] [CrossRef]
- Hintzen, R.Q.; Dale, R.C.; Neuteboom, R.F.; Mar, S.; Banwell, B. Pediatric acquired CNS demyelinating syndromes. Features associated with multiple sclerosis. Neurology 2016, 87 (Suppl. 2), S67–S73. [Google Scholar] [CrossRef] [Green Version]
- Ketelslegers, I.A.; Catsman-Berrevoets, C.E.; Neuteboom, R.F.; Boon, M.; van Dijk, K.G.; Eikelenboom, M.J.; Gooskens, R.H.; Niks, E.H.; Overweg-Plandsoen, W.C.; Peeters, E.A.; et al. Incidence of acquired demyelinating syndromes of the CNS in Dutch children: A nationwide study. J. Neurol. 2012, 259, 1929–1935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mikaeloff, Y.; Suissa, S.; Vallée, L.; Lubetzki, C.; Ponsot, G.; Confavreux, C.; Tardieu, M. First episode of acute CNS inflammatory demyelination in childhood: Prognostic factors for multiple sclerosis and disability. J. Pediatric 2004, 144, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Neuteboom, R.F.; Boon, M.; Catsman Berrevoets, C.E.; Vles, J.S.; Gooskens, R.H.; Stroink, H.; Vermeulen, R.J.; Rotteveel, J.J.; Ketelslegers, I.A.; Peeters, E.; et al. Prognostic factors after a first attack of inflammatory CNS demyelination in children. Neurology 2008, 71, 967–973. [Google Scholar] [CrossRef]
- Tardieu, M.; Mikaeloff, Y. What is acute disseminated encephalomyelitis (ADEM)? Eur. J. Paediatr. Neurol. 2004, 8, 239–242. [Google Scholar] [CrossRef]
- Ketelslegers, I.A.; Pelt, D.E.V.; Bryde, S.; Neuteboom, R.F.; Catsman-Berrevoets, C.E.; Hamann, D.; Hintzen, R.Q. Anti-MOG antibodies plead against MS diagnosis in an acquired demyelinating syndromes cohort. Mult. Scler. J. 2015, 21, 1513–1520. [Google Scholar] [CrossRef]
- Hacohen, Y.; Absoud, M.; Deiva, K.; Hemingway, C.; Nytrova, P.; Woodhall, M.; Palace, J.; Wassmer, E.; Tardieu, M.; Vincent, A.; et al. Myelin oligodendrocyte glycoprotein antibodies are associated with a non-MS course in children. Neurol. Neuroimmunol. Neuroinflamm. 2015, 2, e81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wingerchuk, D.M.; Banwell, B.; Bennett, J.L.; Cabre, P.; Carroll, W.; Chitnis, T.; de Seze, J.; Fujihara, K.; Greenberg, B.; Jacob, A.; et al. International consensus diagnostic criteria for neuromyelitis optica spectrum disorders. Neurology 2015, 89, 177–189. [Google Scholar] [CrossRef]
- Tenembaum, S.N. Acute disseminated encephalomyelitis. Pediatric neurology Part II. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2013; pp. 1253–1262. [Google Scholar]
- Parrish, J.B.; Yeh, E.A. Acute disseminated encephalomyelitis. In Neurodegenerative Diseases; Ahmad, S.I., Ed.; Springer: Berlin, Germany, 2012. [Google Scholar]
- Berzero, G.; Cortese, A.; Ravaglia, S.; Marchioni, E. Diagnosis and therapy of acute disseminated encephalomyelitis and its variants. Expert Rev. Neurother. 2015, 16, 83–101. [Google Scholar] [CrossRef]
- de Mol, C.L.; Wong, Y.Y.M.; van Pelt, E.D.; Ketelslegers, I.A.; Bakker, D.P.; Boon, M.; Braun, K.P.J.; van Dijk, K.G.J.; Eikelenboom, M.J.; Engelen, M.; et al. Incidence and outcome of acquired demyelinating syndromes in Dutch children: Update of a nationwide and prospective study. J. Neurol. 2018, 265, 1310–1319. [Google Scholar] [CrossRef] [Green Version]
- Absoud, M.; Lim, M.J.; Chong, W.K.; De Goede, C.G.; Foster, K.; Gunny, R.; Hemingway, C.; Jardine, P.E.; Kneen, R.; Likeman, M.; et al. Paediatric acquired demyelinating syndromes: Incidence, clinical and magnetic resonance imaging features. Mult. Scler. 2013, 19, 76–86. [Google Scholar] [CrossRef] [PubMed]
- Pellegrino, P.; Radice, S.; Clementi, E. Geoepidemiology of acute disseminated encephalomyelitis. Epidemiology 2014, 25, 928–929. [Google Scholar] [CrossRef]
- Koelman, D.L.; Mateen, F.J. Acute disseminated encephalomyelitis: Current controversies in diagnosis and outcome. J. Neurol. 2015, 262, 2013–2024. [Google Scholar] [CrossRef]
- Karussis, D.; Petrou, P. The spectrum of post-vaccination inflammatory CNS demyelinating syndromes. Autoimmun. Rev. 2014, 13, 215–224. [Google Scholar] [CrossRef]
- Langer-Gould, A.; Qian, L.; Tartof, S.Y.; Brara, S.M.; Jacobsen, S.J.; Beaber, B.E.; Sy, L.S.; Chao, C.; Hechter, R.; Tseng, H.F. Vaccines and the risk of multiple sclerosis and other central nervous system demyelinating diseases. JAMA Neurol. 2014, 71, 1506–1513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koelman, D.L.H.; Chahin, C.; Mar, S.S.; Venkatesan, A.; Hoganson, G.M.; Yeshokumar, A.K.; Barreras, P.; Majmudar, B.; Klein, J.P.; Chitnis, T.; et al. Acute disseminated encephalomyelitis in 228 patients. A retrospective, multicenter US study. Neurology 2016, 86, 1–9. [Google Scholar] [CrossRef]
- Dundar, N.O.; Anlar, B.; Guven, A.; Serdaroglu, A.; Yarar, C. Relapsing acute disseminated encephalomyelitis in children: Further evaluation of the diagnosis. J. Child Neurol. 2010, 25, 1491–1497. [Google Scholar] [CrossRef] [PubMed]
- Tenembaum, S.; Chitnis, T.; Ness, J.; Hahn, J.S. Acute disseminated encephalomyelitis. Neurology 2007, 68 (Suppl. 2), S23–S36. [Google Scholar] [CrossRef]
- Ketelslegers, I.A.; Visser, I.E.; Neuteboom, R.F.; Boon, M.; Catsman-Berrevoets, C.E.; Hintzen, R.Q. Disease course and outcome of acute disseminated encephalomyelitis is more severe in adults than in children. Mult. Scler. 2011, 17, 441–448. [Google Scholar] [CrossRef]
- Werner, K.M.; Dosh, M.P. Atypical ADEM and cardiogenic shock in a 14-year-old female. Pediatrics 2018, 142, 471. [Google Scholar] [CrossRef]
- Lademann, H.; Bertsche, A.; Petzold, A.; Zack, F.; Buttner, A.; Dabritz, J.; Hauenstein, C.; Bahn, E.; Spang, C.; Reuter, D.; et al. Acute disseminated encephalomyelitis with seizures and myocarditis: A fatal triad. Medicina 2020, 56, 277. [Google Scholar] [CrossRef]
- Dale, R.C.; Sousa, C.; Chong, W.K.; Cox, T.C.S.; Harding, B.; Neville, B.G.R. Acute disseminated encephalomyelitis, multiphasic disseminated encephalomyelitis and multiple sclerosis in children. Brain 2000, 123, 2407–2422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, Y.Y.M.; van Pelt, E.D.; Ketelslegers, I.A.; Catsman-Berrevoets, C.E.; Hintzen, R.Q.; Neuteboom, R.F. Evolution of MRI abnormalities in paediatric acute disseminated encephalomyelitis. Eur. J. Paediatr. Neurol. 2017, 21, 300–304. [Google Scholar] [CrossRef]
- Callen, D.J.; Shroff, M.M.; Branson, H.M.; Li, D.K.; Lotze, T.; Stephens, D.; Banwell, B.L. Role of MRI in the differentiation of ADEM from MS in children. Neurology 2009, 72, 968–973. [Google Scholar] [CrossRef]
- Ketelslegers, I.A.; Neuteboom, R.F.; Boon, M.; Catsman-Berrevoets, C.E.; Hintzen, R.Q. A comparison of MRI criteria for diagnosing pediatric ADEM and MS. Neurology 2010, 74, 1412–1415. [Google Scholar] [CrossRef]
- Pavone, P.; Pettoello-Mantovano, M.; Le Pira, A.; Giardino, I.; Pulvirenti, A.; Giugno, R.; Parano, E.; Polizzi, A.; Distefano, A.; Ferro, A.; et al. Acute disseminated encephalomyelitis: A long-term prospective study and meta-analysis. Neuropediatrics 2010, 41, 246–255. [Google Scholar] [CrossRef] [PubMed]
- Kahlmann, V.; Roodbol, J.; van Leeuwen, N.; Ramakers, C.R.B.; van Pelt, D.; Neuteboom, R.F.; Catsman-Berrevoets, C.E.; de Wit, M.C.Y.; Jacobs, B.C. Validated age-specific reference values for CSF total protein levels in children. Eur. J. Paediatr. Neurol. 2017, 21, 654–660. [Google Scholar] [CrossRef] [PubMed]
- Rostasy, K.; Bajer-Kornek, B.; Venkateswaran, S.; Hemingway, C.; Tardieu, M. Differential diagnosis and evaluation in pediatric inflammatory demyelinating disorders. Neurology 2016, 87 (Suppl. 2), S28–S37. [Google Scholar] [CrossRef] [Green Version]
- Hennes, E.; Baumann, M.; Schanda, K.; Anlar, B.; Bajer-Kornek, B.; Blaschek, A.; Brantner-Inthaler, S.; Diepold, K.; Eisenkölbl, A.; Gotwald, T.; et al. Prognostic relevance of MOG antibodies in children with an acquired demyelinating syndrome. Neurology 2017, 89, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Mader, S.; Gredler, V.; Schanda, K.; Rostasy, K.; Dujmovic, I.; Pfaller, K.; Lutterotti, A.; Jarius, S.; Di Pauli, F.; Kuenz, B.; et al. Complement activating antibodies to myelin oligodendrocyte glycoprotein in neuromyelitis optica and related disorders. J. Neuroinflamm. 2011, 8, 184. [Google Scholar] [CrossRef] [Green Version]
- Dale, R.C.; Tantsis, E.M.; Merheb, V.; Kumaran, R.Y.; Sinmaz, N.; Pathmanandavel, K.; Ramanathan, S.; Booth, D.R.; Wienholt, L.A.; Prelog, K.; et al. Antibodies to MOG have a demyelination phenotype and affect oligodendrocyte cytoskeleton. Neurol. Neuroimmunol. Neuroinflamm. 2014, 1, e12. [Google Scholar] [CrossRef] [Green Version]
- Baumann, M.; Hennes, E.; Schanda, K.; Karenfort, M.; Kornek, B.; Seidl, R.; Diepold, K.; Lauffer, H.; Marquardt, I.; Strautmanis, J.; et al. Children with multiphasic disseminated encephalomyelitis and antibodies to the myelin oligodendrocyte glycoprotein (MOG): Extending the spectrum of MOG antibody positive diseases. Mult. Scler. 2016, 22, 1821–1829. [Google Scholar] [CrossRef] [PubMed]
- Kariyawasam, S.; Singh, R.R.; Gadian, J.; Lumsden, D.E.; Lin, J.; Siddiqui, A.; Hacohen, Y.; Absoud, M.; Lim, M. Clinical and radiological features of recurrent demyelination following acute disseminated encephalomyelitis (ADEM). Mult. Scler. Relat. Disord. 2015, 4, 451–456. [Google Scholar] [CrossRef]
- Huppke, P.; Rostasy, K.; Karenfort, M.; Huppke, B.; Seidl, R.; Leiz, S.; Reindl, M.; Gartner, J. Acute disseminated encephalomyelitis followed by recurrent or monophasic optic neuritis in pediatric patients. Mult. Scler. 2013, 19, 941–946. [Google Scholar] [CrossRef]
- Rostasy, K.; Mader, S.; Schanda, K.; Huppke, P.; Gartner, J.; Kraus, V.; Karenfort, M.; Tibussek, D.; Blaschek, A.; Bajer-Kornek, B.; et al. Anti-myelin oligodendrocyte glycoprotein antibodies in pediatric patients with optic neuritis. Arch. Neurol. 2012, 69, 752–756. [Google Scholar] [CrossRef] [Green Version]
- Ramanathan, S.; Prelog, K.; Barnes, E.H.; Tantsis, E.M.; Reddel, S.W.; Henderson, A.P.D.; Vucic, S.; Gorman, M.P.; Benson, L.A.; Alper, G.; et al. Radiological differentiation of optic neuritis with myelin oligodendrocyte glycoprotein antibodies, aquaporin-4 antibodies, and multiple sclerosis. Mult. Scler. 2016, 22, 470–482. [Google Scholar] [CrossRef] [PubMed]
- Young, N.P.; Weinshenker, B.G.; Parisi, J.E.; Scheithauer, B.; Giannini, C.; Roemer, S.F.; Thomsen, K.M.; Mandrekar, J.N.; Erickson, B.J.; Lucchinetti, C.F. Perivenous demyelination: Association with clinically defined acute disseminated encephalomyelitis and comparison with pathologically confirmed multiple sclerosis. Brain 2010, 133 Pt 2, 333–348. [Google Scholar] [CrossRef] [Green Version]
- Ishizu, T.; Minohara, M.; Ichiyama, T.; Kira, R.; Tanaka, M.; Osoegawa, M.; Hara, T.; Furukawa, S.; Kira, J. CSF cytokine and chemokine profiles in acute disseminated encephalomyelitis. J. Neuroimmunol. 2006, 175, 52–58. [Google Scholar] [CrossRef]
- Dale, R.C.; Morovat, A. Interleukin-6 and oligoclonal igg synthesis in children with acute disseminated encephalomyelitis. Neuropediatrics 2003, 34, 141–145. [Google Scholar]
- Horellou, P.; Wang, M.; Keo, V.; Chretien, P.; Serguera, C.; Waters, P.; Deiva, K. Increased interleukin-6 correlates with myelin oligodendrocyte glycoprotein antibodies in pediatric monophasic demyelinating diseases and multiple sclerosis. J. Neuroimmunol. 2015, 289, 1–7. [Google Scholar] [CrossRef]
- Brilot, F.; Dale, R.C.; Selter, R.C.; Grummel, V.; Kalluri, S.R.; Aslam, M.; Busch, V.; Zhou, D.; Cepok, S.; Hemmer, B. Antibodies to native myelin oligodendrocyte glycoprotein in children with inflammatory demyelinating central nervous system disease. Ann. Neurol. 2009, 66, 833–842. [Google Scholar] [CrossRef]
- McLaughlin, K.A.; Chitnis, T.; Newcombe, J.; Franz, B.; Kennedy, J.; McArdel, S.; Kuhle, J.; Kappos, L.; Rostasy, K.; Pohl, D.; et al. Age-dependent B cell autoimmunity to a myelin surface antigen in pediatric multiple sclerosis. J. Immunol. 2009, 183, 4067–4076. [Google Scholar] [CrossRef]
- Peschl, P.; Schanda, K.; Zeka, B.; Given, K.; Bohm, D.; Ruprecht, K.; Saiz, A.; Lutterotti, A.; Rostasy, K.; Hoftberger, R.; et al. Human antibodies against the myelin oligodendrocyte glycoprotein can cause complement-dependent demyelination. J. Neuroinflamm. 2017, 14, 208. [Google Scholar] [CrossRef] [Green Version]
- Fovet, C.M.; Stimmer, L.; Contreras, V.; Horellou, P.; Hubert, A.; Seddiki, N.; Chapon, C.; Tricot, S.; Leroy, C.; Flament, J.; et al. Intradermal vaccination prevents anti-MOG autoimmune encephalomyelitis in macaques. EBioMedicine 2019, 47, 492–505. [Google Scholar] [CrossRef]
- Bhat, R.; Steinman, L. Innate and adaptive autoimmunity directed to the central nervous system. Neuron 2009, 64, 123–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, C.F.; Horwitz, M.S.; Hobbs, M.V.; Oldstone, M.B.A. Viral infection of transgenic mice expressing a viral protein in oligodendrocytes leads to chronic central nervous system autoimmune disease. J. Exp. Med. 1996, 184, 2371–2384. [Google Scholar] [CrossRef] [Green Version]
- Mengea, T.; Kieseiera, B.C.; Nesslera, S.; Hemmera, B.; Hartunga, H.; Stüve, O. Acute disseminated encephalomyelitis: An acute hit against the brain. Curr. Opin. Neurol. 2007, 20, 247–254. [Google Scholar] [CrossRef] [Green Version]
- Cole, J.; Evans, E.; Mwangi, M.; Mar, S. Acute disseminated encephalomyelitis in children: An updated review based on current diagnostic criteria. Pediatr. Neurol. 2019, 100, 26–34. [Google Scholar] [CrossRef]
- Anlar, B.; Basaran, C.; Kose, G.; Guven, A.; Haspolat, S.; Yakut, A.; Serdaroglu, A.; Senbil, N.; Tan, H.; Karaagaoglu, E.; et al. Acute disseminated encephalomyelitis in children: Outcome and prognosis. Neuropediatrics 2003, 34, 194–199. [Google Scholar]
- Pohl, D.; Tenembaum, S. Treatment of acute disseminated encephalomyelitis. Curr. Treat Options Neurol. 2012, 14, 264–275. [Google Scholar] [CrossRef] [PubMed]
- Chitnis, T. Pediatric demyelinating diseases. Contin. (Minneap Minn) 2013, 19, 1023–1045. [Google Scholar] [CrossRef] [PubMed]
- Iro, M.A.; Sadarangani, M.; Absoud, M.; Chong, W.K.; Clark, C.A.; Easton, A.; Gray, V.; Kneen, R.; Lim, M.; Pike, M.; et al. ImmunoglobuliN in the treatment of encephalitis (IgNiTE): Protocol for a multicentre randomised controlled trial. BMJ Open 2016, 6, e012356. [Google Scholar] [CrossRef] [Green Version]
- Eyre, M.; Hacohen, Y.; Barton, C.; Hemingway, C.; Lim, M. Therapeutic plasma exchange in paediatric neurology: A critical review and proposed treatment algorithm. Dev. Med. Child Neurol. 2018, 60, 765–779. [Google Scholar] [CrossRef] [Green Version]
- Weinshenker, B.G.; O’Brien, P.C.; Petterson, T.M.; Noseworthy, J.H.; Lucchinetti, C.F.; Dodick, D.W.; Pineda, A.A.; Stevens, L.N.; Rodriguez, M. A randomized trial of plasma exchange in acute central nervous system inflammatory demyelinating disease. Ann. Neurol. 1999, 46, 878–886. [Google Scholar] [CrossRef]
- Abboud, H.; Petrak, A.; Mealy, M.; Sasidharan, S.; Siddique, L.; Levy, M. Treatment of acute relapses in neuromyelitis optica: Steroids alone versus steroids plus plasma exchange. Mult. Scler. 2016, 22, 185–192. [Google Scholar] [CrossRef] [Green Version]
- Savransky, A.; Rubstein, A.; Rios, M.H.; Vergel, S.L.; Velasquez, M.C.; Sierra, S.P.; Marcarian, G.; Alba, R.; Pugliese, A.M.; Tenembaum, S. Prognostic indicators of improvement with therapeutic plasma exchange in pediatric demyelination. Neurology 2019, 93, e2065–e2073. [Google Scholar] [CrossRef]
- Kim, S.H.; Kim, W.; Huh, S.Y.; Lee, K.Y.; Jung, I.J.; Kim, H.J. Clinical efficacy of plasmapheresis in patients with neuromyelitis optica spectrum disorder and effects on circulating anti-aquaporin-4 antibody levels. J. Clin. Neurol. 2013, 9, 36–42. [Google Scholar] [CrossRef] [Green Version]
- Absoud, M.; Parslow, R.C.; Wassmer, E.; Hemingway, C.; Duncan, H.P.; Cummins, C.; Lim, M.J. Severe acute disseminated encephalomyelitis: A paediatric intensive care population-based study. Mult. Scler. 2010, 17, 1258–1261. [Google Scholar] [CrossRef]
- Zhou, J.; Lu, X.; Zhang, Y.; Ji, T.; Jin, Y.; Xu, M.; Bao, X.; Zhang, Y.; Xiong, H.; Chang, X.; et al. Follow-up study on Chinese children with relapsing MOG-IgG-associated central nervous system demyelination. Mult. Scler. Relat. Disord. 2019, 28, 4–10. [Google Scholar] [CrossRef]
- Deiva, K.; Cobo-Calvo, A.; Maurey, H.; De Chalus, A.; Yazbeck, E.; Husson, B.; Vukusic, S.; Serguerra, C.; Horellou, P.; Marignier, R.; et al. Risk factors for academic difficulties in children with myelin oligodendrocyte glycoprotein antibody-associated acute demyelinating syndromes. Dev. Med. Child Neurol. 2020, 62, 1075–1081. [Google Scholar] [CrossRef]
- Aubert-Broche, B.; Weier, K.; Longoni, G.; Fonov, V.S.; Bar-Or, A.; Marrie, R.A.; Yeh, E.A.; Narayanan, S.; Arnold, D.L.; Verhey, L.H.; et al. Monophasic demyelination reduces brain growth in children. Neurology 2017, 88, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Spadaro, M.; Winklmeier, S.; Beltran, E.; Macrini, C.; Hoftberger, R.; Schuh, E.; Thaler, F.S.; Gerdes, L.A.; Laurent, S.; Gerhards, R.; et al. Pathogenicity of human antibodies against myelin oligodendrocyte glycoprotein. Ann. Neurol. 2018, 84, 315–328. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| ADEM | Single polyfocal clinical CNS event with presumed inflammatory cause Encephalopathy that cannot be explained by fever MRI typically shows diffuse, poorly demarcated, large >1–2 cm lesions predominantly involving cerebral white matter; T1 hypointense white matter lesions are rare; deep gray matter lesions (e.g., thalamus or basal ganglia) can be present No new symptoms, signs or MRI findings after three months of initial ADEM |
| Multiphasic ADEM | New event of ADEM three months or more after initial event that can be associated with new or re-emergence of prior clinical and MRI findings |
| ADEM-ON | At least one subsequent attack of optic neuritis, without encephalopathy, at least three months after initial ADEM |
| ADEM-MS | ADEM followed three months later by a non-encephalopathic clinical event with new lesions on brain MRI consistent with MS |
| ADEM-NMOSD | ADEM followed three months later by ON, myelitis or area postrema syndrome, fulfilling NMOSD diagnostic criteria |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paolilo, R.B.; Deiva, K.; Neuteboom, R.; Rostásy, K.; Lim, M. Acute Disseminated Encephalomyelitis: Current Perspectives. Children 2020, 7, 210. https://doi.org/10.3390/children7110210
Paolilo RB, Deiva K, Neuteboom R, Rostásy K, Lim M. Acute Disseminated Encephalomyelitis: Current Perspectives. Children. 2020; 7(11):210. https://doi.org/10.3390/children7110210
Chicago/Turabian StylePaolilo, Renata Barbosa, Kumaran Deiva, Rinze Neuteboom, Kevin Rostásy, and Ming Lim. 2020. "Acute Disseminated Encephalomyelitis: Current Perspectives" Children 7, no. 11: 210. https://doi.org/10.3390/children7110210
APA StylePaolilo, R. B., Deiva, K., Neuteboom, R., Rostásy, K., & Lim, M. (2020). Acute Disseminated Encephalomyelitis: Current Perspectives. Children, 7(11), 210. https://doi.org/10.3390/children7110210