
A Rare Case of Mandibular Aspergillus Osteomyelitis in an Immunocompetent Patient

 , , ,
, , ,
Abstract
:1. Introduction
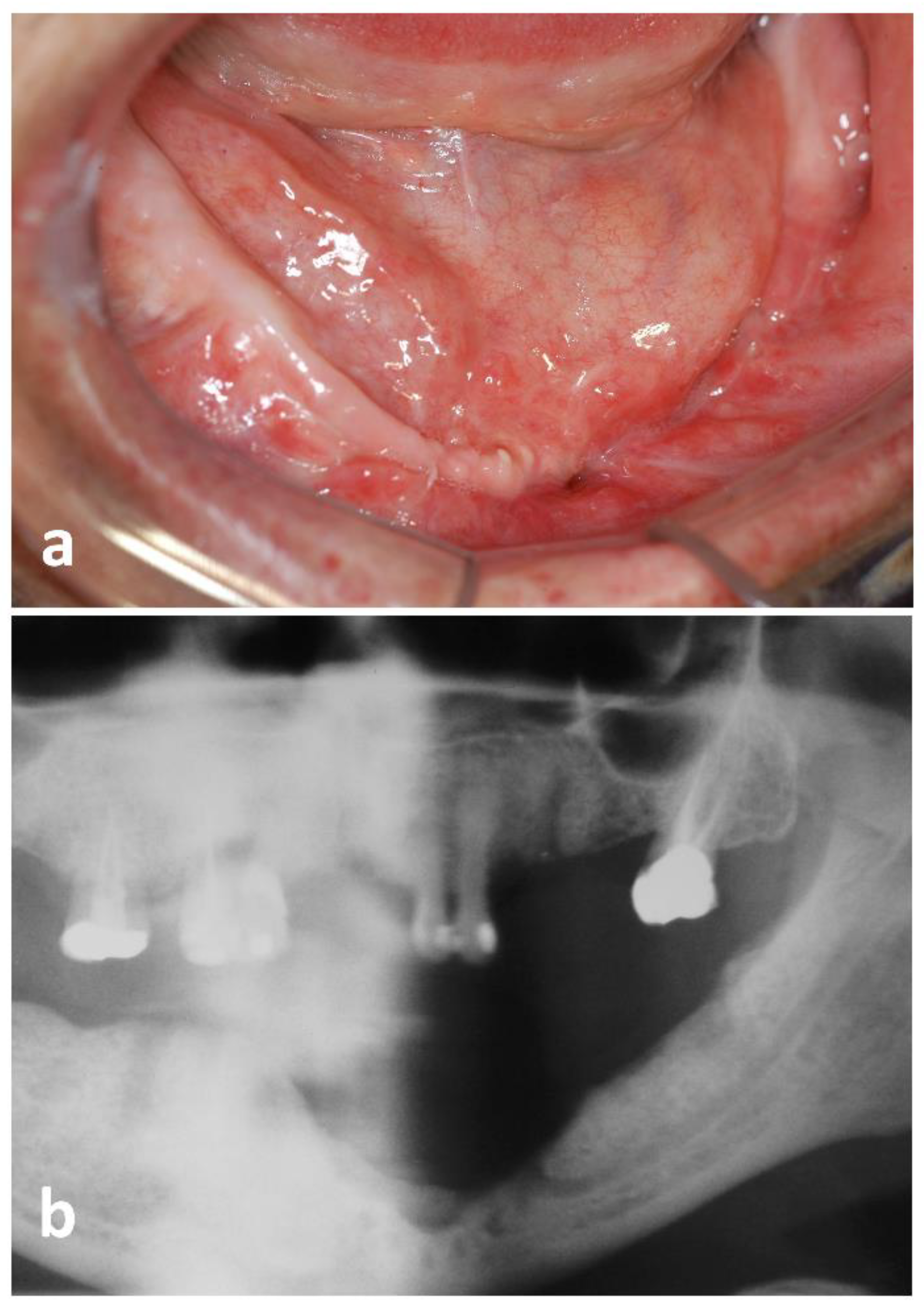
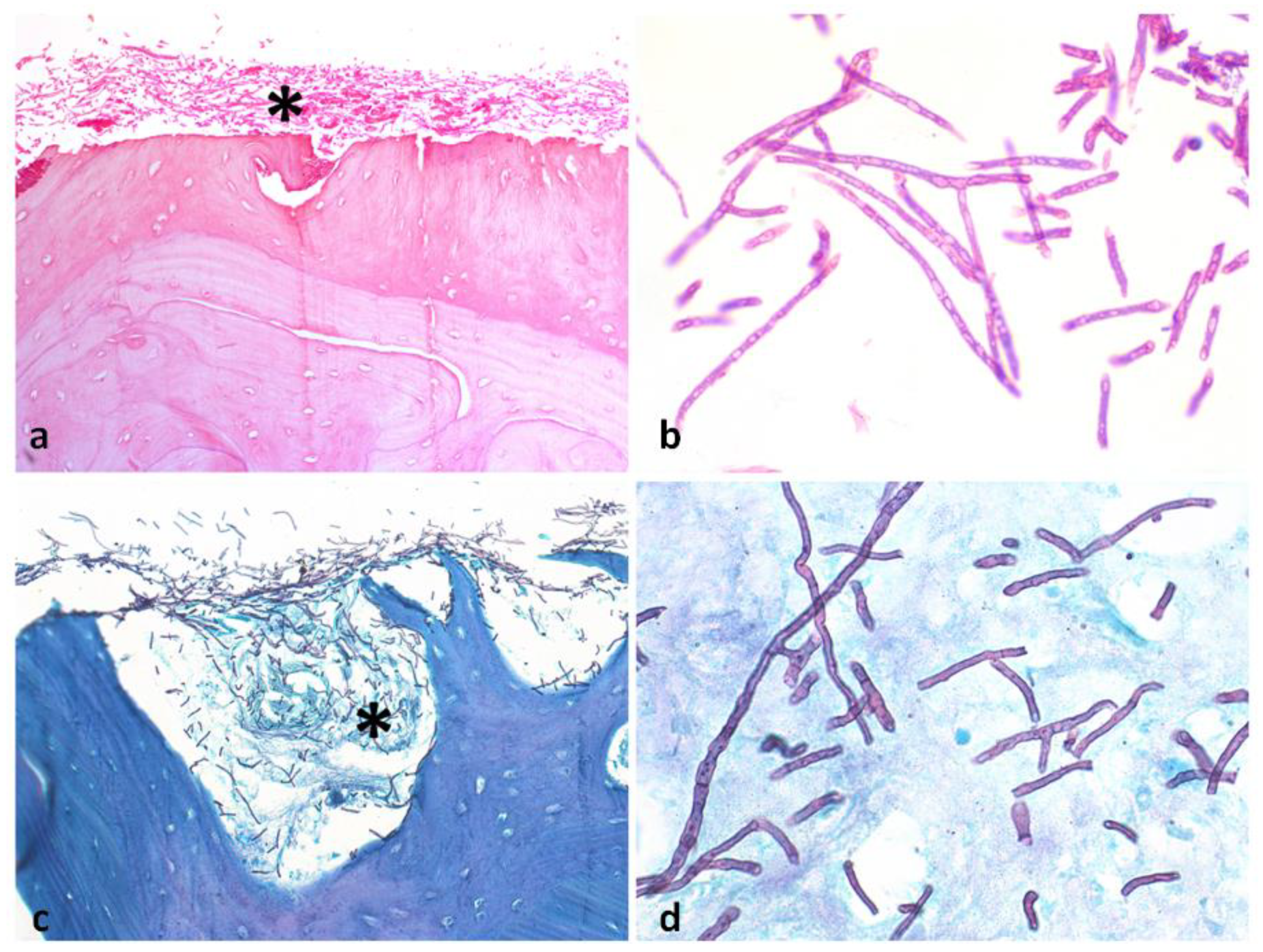
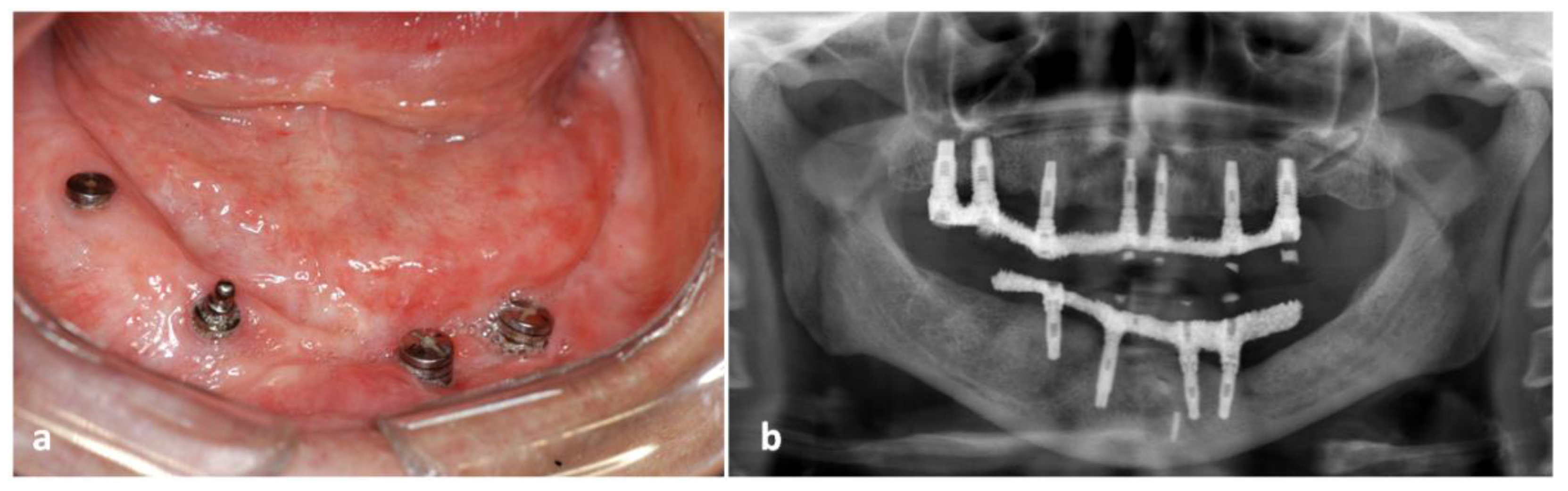
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Park, H.S.; Jun, S.C.; Han, K.H.; Hong, S.B.; Yu, J.H. Diversity, application, and synthetic biology of industrially important aspergillus fungi. Adv. Appl. Microbiol. 2017, 100, 161–202. [Google Scholar] [CrossRef] [PubMed]
- Filippi, A.; Dreyer, T.; Bohle, R.M.; Pohl, Y.; Rosseau, S. Sequestration of the alveolar bone by invasive aspergillosis in acute myeloid leukemia. J. Oral Pathol. Med. 1997, 26, 437–440. [Google Scholar] [CrossRef]
- Doub, J.B.; Mathur, P. Duration of posaconazole therapy for Aspergillus fumigatus osteomyelitis dictated by serial monitoring of 1,3-beta-D glucan. Infection 2020, 48, 959–963. [Google Scholar] [CrossRef] [PubMed]
- Cadena, J.; Thompson, G.R.; Patterson, T.F. Aspergillosis: Epidemiology, diagnosis, and treatment. Infect. Dis. Clin. N. Am. 2021, 35, 415–434. [Google Scholar] [CrossRef]
- Hovi, L.; Saarinen, U.M.; Donner, U.; Lindqvist, C. Opportunistic osteomyelitis in the jaws of children on immunosuppressive chemotherapy. J. Pediatr. Hematol. Oncol. 1996, 18, 90–94. [Google Scholar] [CrossRef] [PubMed]
- Khatri, M.L.; Stefanato, C.M.; Benghazeil, M.; Shafi, M.; Kubba, A.; Bhawan, J. Cutaneous and paranasal aspergillosis in an immunocompetent patient. Int. J. Dermatol. 2000, 39, 853–856. [Google Scholar] [CrossRef]
- Sandhu, S.; Kaur, T. Aspergillosis: A rare case of secondary delayed mandibular involvement. Quintessence Int. 2003, 34, 139–142. [Google Scholar]
- Karabulut, A.B.; Kabakas, F.; Berköz, O.; Karakas, Z.; Kesim, S.N. Hard palate perforation due to invasive aspergillosis in a patient with acute lymphoblastic leukemia. Int. J. Pediatr. Otorhinolaryngol. 2005, 69, 1395–1398. [Google Scholar] [CrossRef]
- Chermetz, M.; Gobbo, M.; Rupel, K.; Ottaviani, G.; Tirelli, G.; Bussani, R.; Luzzati, R.; Di Lenarda, R.; Biasotto, M. Combined orofacial aspergillosis and mucormycosis: Fatal complication of a recurrent paediatric glioma-case report and review of literature. Mycopathologia 2016, 181, 723–733. [Google Scholar] [CrossRef]
- Sethi, P.; Saluja, R.; Jindal, N.; Singh, V. Invasive aspergillosis in an immunocompetent host. J. Oral Maxillofac. Pathol. 2012, 16, 297–300. [Google Scholar] [CrossRef] [Green Version]
- Ganesh, P.; Nagarjuna, M.; Shetty, S.; Kumar, P.; Bhat, V.; Salins, P.C. Invasive aspergillosis presenting as swelling of the buccal mucosa in an immunocompetent individual. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2015, 119, e60–e64. [Google Scholar] [CrossRef] [PubMed]
- Scully, C.; de Almeida, O.P. Orofacial manifestations of the systemic mycoses. J. Oral Pathol. Med. 1992, 21, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Panackal, A.A.; Li, H.; Kontoyiannis, D.P.; Mori, M.; Perego, C.A.; Boeckh, M.; Marr, K.A. Geoclimatic influences on invasive aspergillosis after hematopoietic stem cell transplantation. Clin. Infect. Dis. 2010, 15, 1588–1597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lador, N.; Polacheck, I.; Gural, A.; Sanatski, E.; Garfunkel, A. A trifungal infection of the mandible: Case report and literature review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, 451–456. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Reija, M.F.; Crespo-Pinilla, J.I.; Labayru-Echeverria, C.; Espeso-Ferrero, A.; Verrier-Hernandez, A. Invasive maxillary aspergillosis: Report of a case and review of the literature. Med. Oral 2002, 7, 200–205. [Google Scholar]
- Napoli, J.A.; Donegan, J.O. Aspergillosis and necrosis of the maxilla: A case report. J. Oral Maxillofac. Surg. 1991, 49, 532–534. [Google Scholar] [CrossRef]
- Urs, A.B.; Singh, H.; Nunia, K.; Mohanty, S.; Gupta, S. Post endodontic Aspergillosis in an immunocompetent individual. J. Clin. Exp. Dent. 2015, 7, e535–e539. [Google Scholar] [CrossRef]
- Matjaz, R.; Jernej, P.; Mirela, K.R. Sinus maxillaris mycetoma of odontogenic origin: Case report. Braz. Dent. J. 2004, 15, 248–250. [Google Scholar] [CrossRef]
- Sato, F.R.; Sawazaki, R.; Berretta, D.; Moreira, R.W.; Vargas, P.A.; de Almeida, O.P. Aspergillosis of the maxillary sinus associated with a zygomatic implant. J. Am. Dent. Assoc. 2010, 141, 1231–1235. [Google Scholar] [CrossRef]
- Telles, D.R.; Karki, N.; Marshall, M.W. Oral fungal infections: Diagnosis and management. Dent. Clin. N. Am. 2017, 61, 319–349. [Google Scholar] [CrossRef]
- Myoken, Y.; Sugata, T.; Kyo, T.I.; Fujihara, M. Pathological features of invasive oral aspergillosis in patients with hematological malignancies. J. Oral Maxillofac. Surg. 1996, 54, 263–270. [Google Scholar] [CrossRef]
- Park, M.S.; Eo, M.Y.; Myoung, H.; Kim, S.M.; Lee, J.H. Early diagnosis of jaw osteomyelitis by easy digitalized panoramic analysis. Maxillofac. Plast. Reconstr. Surg. 2019, 41, 6. [Google Scholar] [CrossRef] [PubMed]
- Gabrielli, E.; Fothergill, A.W.; Brescini, L.; Sutton, D.A.; Marchionni, E.; Orsetti, E.; Staffolani, S.; Castelli, P.; Gesuita, R.; Barchiesi, F. Osteomyelitis caused by Aspergillus species: A review of 310 reported cases. Clin. Microbiol. Infect. 2014, 20, 559–565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chugh, A.; Pandey, A.K.; Goyal, A.; Soni, K.; Jain, V.; Thirunavukkarasu, B.; Vedant, D.; Kumar, D.; Kumar, P. Atypical presentations of fungal osteomyelitis during post COVID-19 outbreak—Case series. J. Oral Maxillofac. Surg. Med. Pathol. 2022, 34, 622–627. [Google Scholar] [CrossRef]
- Correa, M.E.; Soares, A.B.; de Souza, C.A.; Cintra, M.L.; Jorge, J.; Almeida, O.P.; Vargas, P.A. Primary aspergillosis affecting the tongue of a leukemic patient. Oral Dis. 2003, 9, 49–53. [Google Scholar] [CrossRef]
- Odabasi, Z.; Mattiuzzi, G.; Estey, E.; Kantarjian, H.; Saeki, F.; Ridge, R.J.; Ketchum, P.A.; Finkelman, M.A.; Rex, J.H.; Ostrosky-Zeichner, L. Beta-D-glucan as a diagnostic adjunct for invasive fungal infections: Validation, cutoff development, and performance in patients with acute myelogenous leukemia and myelodysplastic syndrome. Clin. Infect. Dis. 2004, 15, 199–205. [Google Scholar] [CrossRef]
- Neofytos, D.; Horn, D.; Anaissie, E.; Steinbach, W.; Olyaei, A.; Fishman, J.; Pfaller, M.; Chang, C.; Webster, K.; Marr, K. Epidemiology and outcome of invasive fungal infection in adult hematopoietic stem cell transplant recipients: Analysis of Multicenter Prospective Antifungal Therapy (PATH) Alliance registry. Clin. Infect. Dis. 2009, 1, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Lat, A.; Bhadelia, N.; Miko, B.; Furuya, E.Y.; Thompson, G.R., III. Invasive aspergillosis after pandemic (H1N1) 2009. Emerg. Infect. Dis. 2010, 16, 971–973. [Google Scholar] [CrossRef]
- Thompson, G.R., III; Cornely, O.A.; Pappas, P.G.; Patterson, T.F.; Hoenigl, M.; Jenks, J.D.; Clancy, C.J.; Nguyen, M.H. Invasive aspergillosis as an under-recognized superinfection in COVID-19. Open Forum Infect. Dis. 2020, 19, ofaa242. [Google Scholar] [CrossRef]
- Zou, P.; Wang, C.; Zheng, S.; Guo, F.; Yang, L.; Zhang, Y.; Liu, P.; Shen, Y.; Wang, Y.; Zhang, X.; et al. Invasive pulmonary aspergillosis in adults with avian influenza A (H7N9) pneumonia in China: A retrospective study. J. Infect. Dis. 2020, 16 (Suppl. S2), S193–S197. [Google Scholar] [CrossRef]
- Suresh, A.; Joshi, A.; Desai, A.K.; Juturu, U.; Kurian, D.J.; Jain, P.; Kulkarni, R.D.; Kumar, N. COVID-19-associated fungal osteomyelitis of jaws and sinuses: An experience-driven management protocol. Med. Mycol. 2022, 2, myab082. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Author | Year | Sex | Age | Risk Factors | Oral Manifestation | Systemic Manifestation |
|---|---|---|---|---|---|---|
| Hovi et al. [5] | 1996 | F | 5 | Leukemia | Gingival necrosis and swelling | Fever |
| Filippi et al. [2] | 1997 | M | 36 | Leukemia | Gingival necrosis, bone sequestration | Pulmonary aspergillosis |
| Sandhu and Kaur [7] | 2003 | F | 35 | None | Gingival necrosis | Pulmonary aspergillosis |
| Lador et al. [14] | 2006 | F | 42 | Leukemia | Gingival and alveolar mucosa necrosis | Fever |
| Chugh et al. [24] | 2022 | M | 64 | Post-COVID-19 | Alveolar mucosa and bone necrosis | None |
| Current | 2022 | F | 57 | None | Swelling and fistula | None |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faustino, I.S.P.; Ramos, J.C.; Mariz, B.A.L.A.; Papadopoulou, E.; Georgaki, M.; Nikitakis, N.G.; Vargas, P.A.; Santos-Silva, A.R.; Lopes, M.A. A Rare Case of Mandibular Aspergillus Osteomyelitis in an Immunocompetent Patient. Dent. J. 2022, 10, 213. https://doi.org/10.3390/dj10110213
Faustino ISP, Ramos JC, Mariz BALA, Papadopoulou E, Georgaki M, Nikitakis NG, Vargas PA, Santos-Silva AR, Lopes MA. A Rare Case of Mandibular Aspergillus Osteomyelitis in an Immunocompetent Patient. Dentistry Journal. 2022; 10(11):213. https://doi.org/10.3390/dj10110213
Chicago/Turabian StyleFaustino, Isabel Schausltz Pereira, Joab Cabral Ramos, Bruno Augusto Linhares Almeida Mariz, Erofili Papadopoulou, Maria Georgaki, Nikolaos G. Nikitakis, Pablo Agustin Vargas, Alan Roger Santos-Silva, and Marcio Ajudarte Lopes. 2022. "A Rare Case of Mandibular Aspergillus Osteomyelitis in an Immunocompetent Patient" Dentistry Journal 10, no. 11: 213. https://doi.org/10.3390/dj10110213
APA StyleFaustino, I. S. P., Ramos, J. C., Mariz, B. A. L. A., Papadopoulou, E., Georgaki, M., Nikitakis, N. G., Vargas, P. A., Santos-Silva, A. R., & Lopes, M. A. (2022). A Rare Case of Mandibular Aspergillus Osteomyelitis in an Immunocompetent Patient. Dentistry Journal, 10(11), 213. https://doi.org/10.3390/dj10110213