
Oral Mucosal Lesions in Childhood

 , and
, and
Abstract
:1. Introduction
2. Physiological Structures
2.1. Linea Alba
2.2. Leukoedema
3. Congenital Anomalies
3.1. Ankyloglossia
3.2. Congenital Epulis
3.3. Melanocytic Nevus
- Compound nevus: the proliferation of melanocytes in both epithelium and the underlying connective tissue [24].
- Blue nevus: the proliferation of elongated melanocytes deep within the lamina propria, far from the epithelium. This lesion is typically found on the hard palate [1,24,25]. They can be further classified into atypical blue nevus, locally aggressive blue nevus and congenital giant melanocytic nevus with nodular growth [1,25].

{kind=link}
{kind=link}
| Type of Nevi | Prognosis and Treatment | Reference |
|---|---|---|
| Junctional nevus | Good prognosis. No treatment needed. May be surgical, cryotherapy, or laser therapy. | [28] |
| Compound nevus | Good prognosis. Surgical excision is treatment. | [29] |
| Intramucosal nevus | Good prognosis. Surgical excision is treatment. | [30] |
| Blue nevus | Possible malignancy. Pathohistological diagnosis is necessary. | [31] |
| Spitz nevus | Good prognosis in children. | [32] |
| The diagnosis of a Spitz nevus must be carefully distinguished from melanoma. Surgical excision is treatment. |
4. Developmental Anomalies
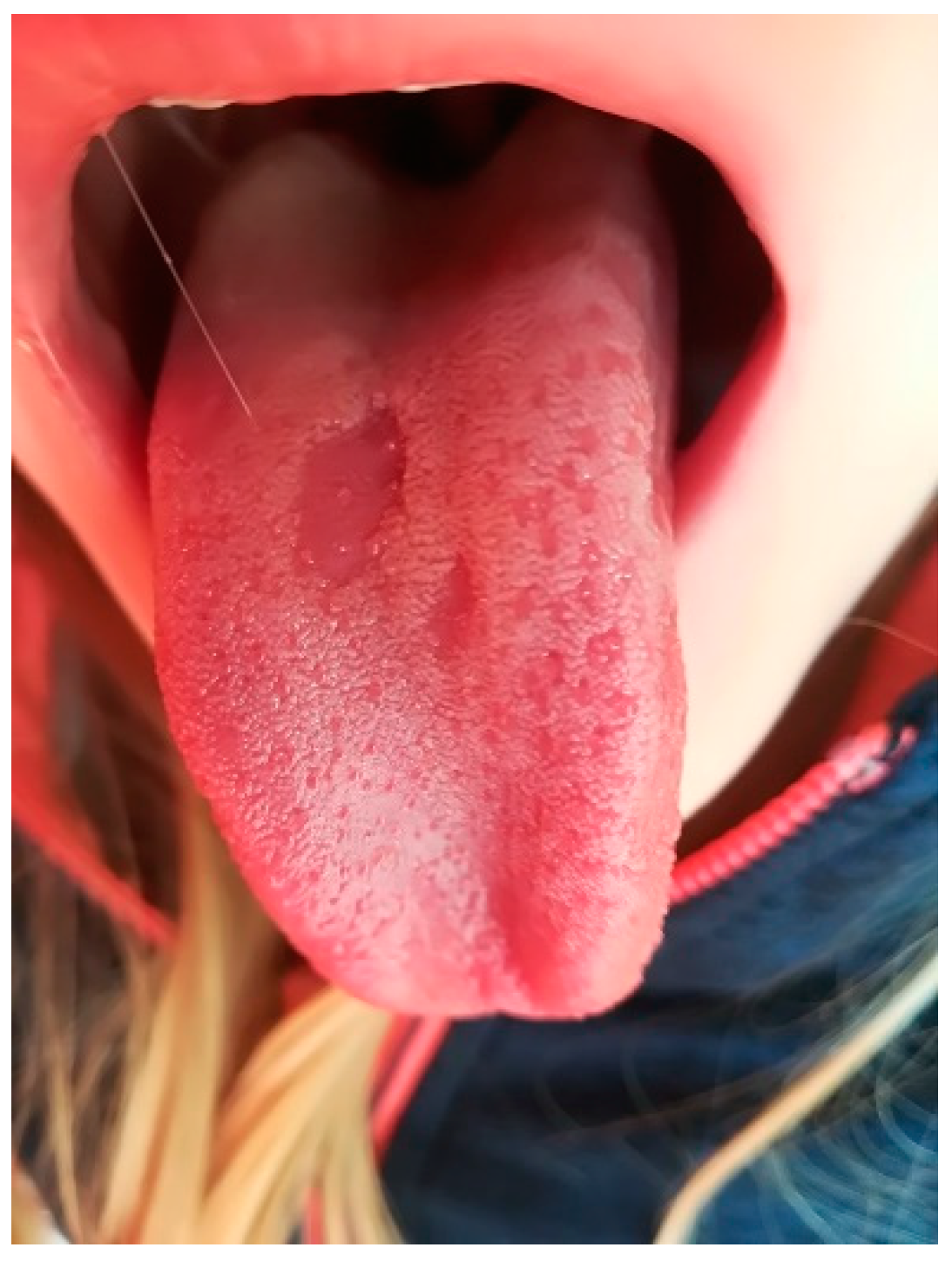
4.1. Geographic Tongue
4.2. Fissured Tongue
4.3. Retrocuspid Papilla
5. Hereditary Diseases
5.1. White Sponge Nevus
5.2. Peutz–Jeghers Syndrome
5.3. Neurofibromatosis Type 1
6. Benign Tumors
6.1. Fibroma
6.2. Hemangioma
6.3. Lymphangioma
7. Traumatic Lesions
7.1. Mucocele
7.2. Ranula
8. Injury to the Oral Mucosa
9. Recurrent Aphthous Lesions
- Minor aphthae: lesions are typically less than 1 cm in diameter; they heal without scarring within 10 days (Figure 2).
- Major aphthous ulcerations: more than 1 cm in diameter, they can last for up to 30 days and may leave scars.
10. COVID-19 Infection
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pinto, A.; Haberland, C.M.; Baker, S. Pediatric Soft Tissue Oral Lesions. Dent. Clin. N. Am. 2014, 58, 437–453. [Google Scholar] [CrossRef] [PubMed]
- Delaney, J.E.; Keels, M.A. Pediatric Oral Pathology: Soft Tissue and Periodontal Conditions. Pediatr. Clin. N. Am. 2000, 47, 1125–1147. [Google Scholar] [CrossRef]
- Müller, S. Frictional Keratosis, Contact Keratosis and Smokeless Tobacco Keratosis: Features of Reactive White Lesions of the Oral Mucosa. Head Neck Pathol. 2019, 13, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Mills, N.; Pransky, S.M.; Geddes, D.T.; Mirjalili, S.A. What Is a Tongue Tie? Defining the Anatomy of the in-Situ Lingual Frenulum. Clin. Anat. 2019, 32, 749–761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savasta, S.; Rossi, A.; Foiadelli, T.; Licari, A.; Perini, A.M.E.; Farello, G.; Verrotti, A.; Marseglia, G.L. Melkersson–Rosenthal Syndrome in Childhood: Report of Three Paediatric Cases and a Review of the Literature. Int. J. Environ. Res. Public Health 2019, 16, 1289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nevozinskaya, Z.; Korsunskaya, I.; Sakaniya, L.; Perlamutrov, Y.; Sobolev, V. Peutz–Jeghers Syndrome in Dermatology. Acta Dermatovenerol. Alp. Pannonica Adriat 2019, 28, 135–137. [Google Scholar] [CrossRef]
- Patil, S.; Rao, R.S.; Majumdar, B.; Jafer, M.; Maralingannavar, M.; Sukumaran, A. Oral Lesions in Neonates. Int. J. Clin. Pediatr. Dent. 2016, 9, 131–138. [Google Scholar] [CrossRef]
- Kang, H.S.; Lee, H.E.; Ro, Y.S.; Lee, C.W. Three Cases of Morsicatio Labiorum. Ann. Dermatol. 2012, 24, 455–458. [Google Scholar] [CrossRef] [Green Version]
- Bardellini, E.; Veneri, F.; Amadori, F.; Conti, G.; Majorana, A. Photobiomodulation Therapy for the Management of Recurrent Aphthous Sto-Matitis in Children: Clinical Effectiveness and Parental Satisfaction. Med. Oral Patol. Oral y Cir. Bucal 2020, 25, e549–e553. [Google Scholar] [CrossRef]
- Madani, F.M.; Kuperstein, A.S. Normal Variations of Oral Anatomy and Common Oral Soft Tissue Lesions: Evaluation and Management. Med. Clin. N. Am. 2014, 98, 1281–1298. [Google Scholar] [CrossRef]
- Pinna, R.; Cocco, F.; Campus, G.; Conti, G.; Milia, E.; Sardella, A.; Cagetti, M.G. Genetic and Developmental Disorders of the Oral Mucosa: Epidemiology; Molecular Mechanisms; Diagnostic Criteria; Management. Periodontology 2000 2019, 80, 12–27. [Google Scholar] [CrossRef] [PubMed]
- Pompéia, L.E.; Ilinsky, R.S.; Ortolani, C.L.F.; Faltin, J.K. Ankyloglossia and Its Influence on Growth and Development of the Stomatognathic System. Rev. Paul Pediatr. 2017, 35, 216–221. [Google Scholar] [CrossRef] [Green Version]
- Walsh, J.; Tunkel, D. Diagnosis and Treatment of Ankyloglossia in Newborns and Infants: A Review. JAMA Otolaryngol. Head Neck Surg. 2017, 143, 1032–1039. [Google Scholar] [CrossRef] [PubMed]
- Solis-Pazmino, P.; Kim, G.S.; Lincango-Naranjo, E.; Prokop, L.; Ponce, O.J.; Truong, M.T. Major Complications after Tongue-Tie Release: A Case Report and Systematic Review. Int. J. Pediatr. Otorhinolaryngol. 2020, 138, 110356. [Google Scholar] [CrossRef]
- Ingram, J.; Copeland, M.; Johnson, D.; Emond, A. The Development and Evaluation of a Picture Tongue Assessment Tool for Tongue-Tie in Breastfed Babies (TABBY). Int. Breastfeed. J. 2019, 14, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Messner, A.H.; Walsh, J.; Rosenfeld, R.M.; Schwartz, S.R.; Ishman, S.L.; Baldassari, C.; Brietzke, S.E.; Darrow, D.H.; Goldstein, N.; Levi, J.; et al. Clinical Consensus Statement: Ankyloglossia in Children. Otolaryngol. Head Neck Surg. USA 2020, 162, 597–611. [Google Scholar] [CrossRef] [Green Version]
- Gessesse, M. Congenital Epulis. Ethiop. Med. J. 2007, 45, 395–397. [Google Scholar]
- Conrad, R.; Perez, M.C.N. Congenital Granular Cell Epulis. Arch. Pathol. Lab. Med. 2014, 138, 128–131. [Google Scholar] [CrossRef] [Green Version]
- Aparna, H.G.; Jayanth, B.S.; Shashidara, R.; Jaishankar, P. Congenital Epulis in a Newborn: A Case Report, Immunoprofiling and Review of Literature. Ethiop. J. Health Sci. 2014, 24, 359–362. [Google Scholar] [CrossRef] [Green Version]
- Mizutani, K.; Mukai, M.; Nagatsuka, H.; Yamada, S. Whitish-Yellow Tumor on Its Characteristic Cut Surface: A Case Report of Congenital Granular Cell Epulis. Clin. Pathol. 2019, 12, 1–2. [Google Scholar] [CrossRef] [Green Version]
- Kokubun, K.; Matsuzaka, K.; Akashi, Y.; Sumi, M.; Nakajima, K.; Murakami, S.; Narita, M.; Shibahara, T.; Inoue, T. Congenital Epulis: A Case and Review of the Literature. Bull. Tokyo Dent. Coll. 2018, 59, 127–132. [Google Scholar] [CrossRef]
- Kinsler, V.A.; O’Hare, P.; Bulstrode, N.; Calonje, J.E.; Chong, W.K.; Hargrave, D.; Jacques, T.; Lomas, D.; Sebire, N.J.; Slater, O. Melanoma in Congenital Melanocytic Naevi. Br. J. Dermatol. 2017, 176, 1131–1143. [Google Scholar] [CrossRef] [Green Version]
- Levy, R.; Lara-Corrales, I. Melanocytic Nevi in Children: A Review. Pediatr. Ann. 2016, 45, e293–e298. [Google Scholar] [CrossRef]
- Müller, S. Melanin-Associated Pigmented Lesions of the Oral Mucosa: Presentation, Differential Diagnosis, and Treatment. Dermatol. Ther. 2010, 23, 220–229. [Google Scholar] [CrossRef]
- Gondak, R.O.; da Silva-Jorge, R.; Jorge, J.; Lopes, M.A.; Vargas, P.A. Oral Pigmented Lesions: Clinicopathologic Features and Review of the Literature. Med. Oral Patol. Oral Cir. Bucal 2012, 17, e919–e924. [Google Scholar] [CrossRef]
- Li, C.C.; Harrist, T.J.; Noonan, V.L.; Woo, S. Bin Intraoral Spitz Nevus: Case Report and Literature Review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 117, 320–324. [Google Scholar] [CrossRef]
- Zayour, M.; Lazova, R. Congenital Melanocytic Nevi. Clin. Lab. Med. 2011, 31, 267–280. [Google Scholar] [CrossRef]
- Köse, O. Carbon Dioxide Ablative Laser Treatment of Acquired Junctional Melanocytic Nevi. J. Cosmet. Dermatol. 2021, 20, 491–496. [Google Scholar] [CrossRef]
- García de Oteyza, G.; Betancourt, J.; Benedetti Sandner, M.; Vázquez-Romo, K.A.; Hernández-Ayuso, I.; Ramos-Betancourt, N. Inflammatory Juvenile Compound Nevi: A Melanoma Is Not All That It Appears to Be. Arch. Soc. Esp. Oftalmol. 2019, 94, 90–94. [Google Scholar] [CrossRef]
- Devildos, L.R.; Langlois, C.C. Intramucosal Cellular Nevi. Oral Surg. Oral Med. Oral Pathol. 1981, 52, 162–166. [Google Scholar] [CrossRef]
- Borgenvik, T.L.; Karlsvik, T.M.; Ray, S.; Fawzy, M.; James, N. Blue Nevus-like and Blue Nevus-Associated Melanoma: A Comprehensive Review of the Literature. ANZ J. Surg. 2017, 87, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.; Sawyer, J.D.; Neumeister, M.W. Spitz Nevus: Review and Update. Clin. Plast. Surg. 2021, 48, 677–686. [Google Scholar] [CrossRef] [PubMed]
- Gombra, V.; Kaur, M.; Sircar, K.; Popli, D.B. Pigmented Oral Compound Nevus of Retromolar Area—A Rare Case Report. Singapore Dent. J. 2016, 37, 33–35. [Google Scholar] [CrossRef] [PubMed]
- Lambertini, M.; Patrizi, A.; Fanti, P.A.; Melotti, B.; Caliceti, U.; Magnoni, C.; Misciali, C.; Baraldi, C.; Ravaioli, G.M.; Dika, E. Oral Melanoma and Other Pigmentations: When to Biopsy? J. Eur. Acad. Dermatology Venereol. 2018, 32, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Mangold, A.R.; Torgerson, R.R.; Rogers, R.S. Diseases of the Tongue. Clin. Dermatol. 2016, 34, 458–469. [Google Scholar] [CrossRef]
- Nandini, D.B.; Bhavana, S.B.; Deepak, B.S.; Ashwini, R. Paediatric Geographic Tongue: A Case Report, Review and Recent Updates. J. Clin. Diagnostic Res. 2016, 10, ZE05–ZE09. [Google Scholar] [CrossRef]
- Picciani, B.; Teixeira-Souza, T.; Santos, V.C.; Gonzaga, H.; Cardoso-Oliveira, J.; Gripp, A.; Dias, E.; Carneiro, S. Geographic Tongue and Psoriasis: Clinical, Histopathological, Inmunohistochemical and Genetic Correlation. Contin. Med. Educ. 2016, 91, 410–421. [Google Scholar]
- González-Álvarez, L.; García-Pola, M.J.; Garcia-Martin, J.M. Geographic Tongue: Predisposing Factors, Diagnosis and Treatment. A Systematic Review. Rev. Clin. Esp. 2018, 218, 481–488. [Google Scholar] [CrossRef]
- Dhawan, S.R.; Saini, A.G.; Singhi, P.D. Management Strategies of Melkersson-Rosenthal Syndrome: A Review. Int. J. Gen. Med. 2020, 13, 61–65. [Google Scholar] [CrossRef] [Green Version]
- Mainville, G.N. Non-HPV Papillary Lesions of the Oral Mucosa: Clinical and Histopathologic Features of Reactive and Neoplastic Conditions. Head Neck Pathol. 2019, 13, 71–79. [Google Scholar] [CrossRef]
- Benoit, S.; Schlipf, N.; Hausser, I.; Fischer, J.; Hamm, H. White Sponge Nevus—A Rare Autosomal Dominant Keratinopathy. Klin. Padiatr. 2014, 226, 375–376. [Google Scholar] [CrossRef]
- Burgmeier, C.; Schier, F.; Staatz, G. Gastric Outlet Obstruction in a Neonate Because of Peutz-Jeghers Syndrome. J. Pediatr. Surg. 2012, 47, e1. [Google Scholar] [CrossRef]
- Cunha, K.S.; Rozza-de-Menezes, R.E.; Andrade, R.M.; Almeida, L.; Janini, M.; Geller, M. Oral Manifestations of Neurofibromatosis Type 1 in Children with Facial Plexiform Neurofibroma: Report of Three Cases. J. Clin. Pediatr. Dent. 2015, 39, 168–171. [Google Scholar] [CrossRef]
- Bezerra, K.T.; Leite, T.C.; Roza, A.L.O.C.; Araújo, R.; Israel, M.S.; Canedo, N.H.S.; Agostini, M.; Benevenuto de Andrade, B.A.; Romañach, M.J. White Sponge Nevus: A Condition Not Always Clinically Suspected. J. Cutan. Pathol. 2020, 47, 22–26. [Google Scholar] [CrossRef]
- Sobhan, M.; Alirezaei, P.; Farshchian, M.; Eshghi, G.; Basir, H.R.G.; Khezrian, L. White Sponge Nevus: Report of a Case and Review of the Literature. Acta Med. Iran. 2017, 55, 533–535. [Google Scholar]
- Cai, W.; Jiang, B.; Yu, F.; Yang, J.; Chen, Z.; Liu, J.; Wei, R.; Zhao, S.; Wang, X.; Liu, S. Current Approaches to the Diagnosis and Treatment of White Sponge Nevus. Expert Rev. Mol. Med. 2015, 17, e9. [Google Scholar] [CrossRef]
- Songu, M.; Adibelli, H.; Diniz, G. White Sponge Nevus: Clinical Suspicion and Diagnosis. Pediatr. Dermatol. 2012, 29, 495–497. [Google Scholar] [CrossRef]
- Schwartz, Z.; Magro, C.; Nuovo, G. The Molecular-Based Differentiation of Heck’s Disease from Its Mimics Including Oral Condyloma and White Sponge Nevus. Ann. Diagn. Pathol. 2019, 43, 151402. [Google Scholar] [CrossRef]
- Bukhari, A.F.; Farag, A.M.; Treister, N.S. Chronic Oral Lesions. Dermatol. Clin. 2020, 38, 451–466. [Google Scholar] [CrossRef]
- Elfatoiki, F.Z.; Capatas, S.; Skali, H.D.; Hali, F.; Attar, H.; Chiheb, S. Oral White Sponge Nevus: An Exceptional Differential Diagnosis in Childhood. Case Rep. Dermatol. Med. 2020, 2020, 4–6. [Google Scholar] [CrossRef]
- Yamashita, K.; Samejima, M.; Oikawa, K.; Mizuno, K.; Ando, Y. White Sponge Nevus in a Three-Year-Old Boy: A Case Report. Pediatr. Int. 2020, 62, 882–883. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.J.; Su, Z.; Liu, X.; Wang, L.; Zhang, Q. Peutz-Jeghers Syndrome with Early Onset of Pre-Adolescent Gynecomastia: A Predigree Case Report and Clinical and Molecular Genetic Analysis. Am. J. Transl. Res. 2017, 9, 2639–2644. [Google Scholar] [PubMed]
- Duan, S.X.; Wang, G.H.; Zhong, J.; Ou, W.H.; Fu, M.X.; Wang, F.S.; Ma, S.H.; Li, J.H. Peutz-Jeghers Syndrome with Intermittent Upper Intestinal Obstruction. Medicine 2017, 96, e6538. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.O.; Melit, L.E. Early Onset Peutz—Jeghers Syndrome, the Importance of Appropriate Diagnosis and Follow-Up. Medicine USA 2019, 98, e16381. [Google Scholar]
- Zhao, Z.Y.; Jiang, Y.L.; Li, B.R.; Li, J.; Jin, X.W.; Yu, E.D.; Ning, S. Bin Close and Regular Surveillance Is Key to Prevent Severe Complications for Peutz-Jeghers Syndrome Patients without Gastrointestinal Polyps: Case Report of a Novel STK11 Mutation (c.471–472delCT) in a Chinese Girl. BMC Surg. 2018, 18, 24. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, L.d.S.; Calderipe, C.B.; Maass, J.B.; Carrard, V.C.; Martins, M.D.; Abreu, L.G.; Schuch, L.F.; Uchoa Vasconcelos, A.C. Oral Pigmented Lesions in Syndromic Individuals: A Systematic Review. Oral Dis. 2021, 28, 531–540. [Google Scholar] [CrossRef]
- Tolentino, E.d.S.; Souza Pinto, G.N.d.; Maciel, L.; Soares, C.T.; Lara, V.S.; Moreschi, A.R.C. Exuberant Manifestation of Neurofibromatosis Type 1 Affecting 3 Generations: Delayed Diagnosis and the Importance of the Multidisciplinary Approach. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2019, 128, e108–e112. [Google Scholar] [CrossRef]
- Javed, F.; Ramalingam, S.; Ahmed, H.B.; Gupta, B.; Sundar, C.; Qadri, T.; Al-Hezaimi, K.; Romanos, G.E. Oral Manifestations in Patients with Neurofibromatosis Type-1: A Comprehensive Literature Review. Crit. Rev. Oncol. Hematol. 2014, 91, 123–129. [Google Scholar] [CrossRef]
- Fahy, E.; Mulvihill, C.; O’Donoghue, G.; O’Regan, E.; Collins, M. Neurofibromatosis -1 Diagnosed from an Intraoral Swelling—A Case Series. Aust. Dent. J. 2021, 66, 205–211. [Google Scholar] [CrossRef]
- Thompson, L.D.R.; Koh, S.S.; Lau, S.K. Sporadic Neurofibroma of the Tongue Unassociated with Neurofibromatosis Type I: A Clinicopathologic Study of Ten Cases. Head Neck Pathol. 2020, 14, 374–380. [Google Scholar] [CrossRef]
- Luna, E.B.; Janini, M.E.R.; Lima, F.; Pontes, R.R.D.A.; Guedes, F.R.; Geller, M.; Da Silva, L.E.; Motta, A.T.; Cunha, K.S. Craniomaxillofacial Morphology Alterations in Children, Adolescents and Adults with Neurofibromatosis 1: A Cone Beam Computed Tomography Analysis of a Brazilian Sample. Med. Oral Patol. Oral y Cir. Bucal 2018, 23, e168–e179. [Google Scholar] [CrossRef]
- Sheejith, M.; Joseph, B.; Nath, S.G.; Sheejith, B. An Unusual Case of Multiple Intraoral Manifestations of Neurofbromatosis Type 1: Case Report with Literature Review. J. Clin. Diagn. Res. 2014, 8, ZD20–ZD22. [Google Scholar] [CrossRef]
- Kubota, S.; Imai, T.; Iwai, S.; Nakazawa, M.; Uzawa, N. Gingival Neurofibroma with Teardrop-Shaped Defects of the Interdental Alveolar Bone: An Unusual Oral Manifestation of Neurofibromatosis Type 1. J. Craniofac. Surg. 2019, 30, E205–E207. [Google Scholar] [CrossRef]
- Warhekar, A.M.; Wanjari, P.V.; Chaudhary, A.; Hada, D.S.; Gupta, R. A Rare Case Report of Neurofibromatosis I in HIV Positive Individual. J. Clin. Diagn. Res. 2015, 9, 20–22. [Google Scholar] [CrossRef]
- Valério, R.A.; de Queiroz, A.M.; Romualdo, P.C.; Brentegani, L.G.; de Paula-Silva, F.W.G. Mucocele and Fibroma: Treatment and Clinical Features for Differential Diagnosis. Braz. Dent. J. 2013, 24, 537–541. [Google Scholar] [CrossRef] [Green Version]
- Kilinc, A.; Saruhan, N.; Gundogdu, B.; Yalcin, E.; Ertas, U.; Urvasizoglu, G. Benign Tumors and Tumor-like Lesions of the Oral Cavity and Jaws: An Analysis of 709 Cases. Niger. J. Clin. Pract. 2017, 20, 1448–1454. [Google Scholar] [CrossRef]
- Dhanuthai, K.; Kintarak, S.; Subarnbhesaj, A.; Chamusri, N. A Multicenter Study of Tongue Lesions from Thailand. Eur. J. Dent. 2020, 14, 435–439. [Google Scholar] [CrossRef]
- Ogle, O.E.; Santosh, A.B.R. Medication Management of Jaw Lesions for Dental Patients. Dent. Clin. North Am. 2016, 60, 483–495. [Google Scholar] [CrossRef]
- Matsumoto, N.; Tsuchiya, M.; Nomoto, S.; Matsue, Y.; Nishikawa, Y.; Takamura, T.; Oki, H.; Komiyama, K. CD105 Expression in Oral Capillary Hemangiomas and Cavernous Hemangiomas. J. Oral Sci. 2015, 57, 45–53. [Google Scholar] [CrossRef] [Green Version]
- Barrón-Peña, A.; Martínez-Borras, M.A.; Benítez-Cárdenas, O.; Pozos-Guillén, A.; Garrocho-Rangel, A. Management of the Oral Hemangiomas in Infants and Children: Scoping Review. Med. Oral Patol. Oral y Cir. Bucal 2020, 25, e252–e261. [Google Scholar] [CrossRef]
- Dehart, A.; Richter, G. Hemangioma: Recent Advances. F1000Research 2019, 8, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Yuhan, B.T.; Svider, P.F.; Mutchnick, S.; Sheyn, A. Benign and Malignant Oral Lesions in Children and Adolescents: An Organized Approach to Diagnosis and Management. Pediatr. Clin. N. Am. 2018, 65, 1033–1050. [Google Scholar] [CrossRef]
- Ademi Abdyli, R.; Abdyli, Y.; Perjuci, F.; Gashi, A.; Agani, Z.; Ahmedi, J. Sclerotherapy of Intraoral Superficial Hemangioma. Case Rep. Dent. 2016, 2016, 12–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maymone, M.B.C.; Greer, R.O.; Burdine, L.K.; Dao-Cheng, A.; Venkatesh, S.; Sahitya, P.C.; Maymone, A.C.; Kesecker, J.; Vashi, N.A. Benign Oral Mucosal Lesions: Clinical and Pathological Findings. J. Am. Acad. Dermatol. 2019, 81, 43–56. [Google Scholar] [CrossRef] [PubMed]
- Bharti, V.; Singh, J. Capillary Hemangioma of Palatal Mucosa. J. Indian Soc. Periodontol. 2012, 16, 475–478. [Google Scholar] [CrossRef]
- De Mesquita Netto, A.C.; De Oliveira, M.B.; Bernardes, V.F.; Gomes, C.C.; Gomez, R.S. Wilms Tumor 1 Protein Is Not Expressed in Oral Lymphangiomas. Braz. Dent. J. 2012, 23, 707–710. [Google Scholar] [CrossRef] [Green Version]
- Usha, V.; Sivasankari, T.; Jeelani, S.; Asokan, G.S.; Parthiban, J. Lymphangioma of the Tongue—A Case Report and Review of Literature. J. Clin. Diagn. Res. 2014, 8, ZD12–ZD14. [Google Scholar] [CrossRef]
- Bowers, E.M.R.; Schaitkin, B. Management of Mucoceles, Sialoceles, and Ranulas. Otolaryngol. Clin. N. Am. 2021, 54, 543–551. [Google Scholar] [CrossRef]
- Ayhan, E.; Toprak, S.F.; Kaya, Ş.; Akkaynak, Ş. Dermoscopy of Oral Mucocele: Three Types of Extravasation Mucoceles. Turkish J. Med. Sci. 2020, 50, 96–102. [Google Scholar] [CrossRef]
- Bhargava, N.; Agarwal, P.; Sharma, N.; Agrawal, M.; Sidiq, M.; Narain, P. An Unusual Presentation of Oral Mucocele in Infant and Its Review. Case Rep. Dent. 2014, 2014, 723130. [Google Scholar] [CrossRef] [Green Version]
- Joshi, S.R.; Pendyala, G.S.; Choudhari, S.; Kalburge, J. Mucocele of the Glands of Blandin-Nuhn in Children: A Clinical, Histopathologic, and Retrospective Study. N. Am. J. Med. Sci. 2012, 4, 379–383. [Google Scholar] [CrossRef]
- Choi, Y.J.; Byun, J.S.; Choi, J.K.; Jung, J.K. Identification of Predictive Variables for the Recurrence of Oral Mucocele. Med. Oral Patol. Oral y Cir. Bucal 2019, 24, e231–e235. [Google Scholar] [CrossRef]
- Abdel-Aziz, M.; Khalifa, B.; Nassar, A.; Kamel, A.; Naguib, N.; El-Tahan, A.R. Mucocele of the Hard Palate in Children. Int. J. Pediatr. Otorhinolaryngol. 2016, 85, 46–49. [Google Scholar] [CrossRef]
- Carlson, E.R.; Ord, R.A. Benign Pediatric Salivary Gland Lesions. Oral Maxillofac. Surg. Clin. N. Am. 2016, 28, 67–81. [Google Scholar] [CrossRef]
- Piazzetta, C.M.; Torres-Pereira, C.; Amenábar, J.M. Micro-Marsupialization as an Alternative Treatment for Mucocele in Pediatric Dentistry. Int. J. Paediatr. Dent. 2012, 22, 318–323. [Google Scholar] [CrossRef]
- Silva, D.F.B.; Neves, G.d.V.; Moura, R.Q.d.; Carvalho, S.H.G.d.; Pereira, J.V.; Gomes, D.Q.d.C. Modified Micromarsupialization as Treatment of Ranula in a Pediatric Patient. J. Craniofac. Surg. 2020, 31, e230–e232. [Google Scholar] [CrossRef]
- Saikaly, S.K.; Saikaly, T.S.; Saikaly, L.E. Recurrent Aphthous Ulceration: A Review of Potential Causes and Novel Treatments. J. Dermatolog. Treat. 2018, 29, 542–552. [Google Scholar] [CrossRef]
- Fitzpatrick, S.G.; Cohen, D.M.; Clark, A.N. Ulcerated Lesions of the Oral Mucosa: Clinical and Histologic Review. Head Neck Pathol. 2019, 13, 91–102. [Google Scholar] [CrossRef]
- Bakshi, S.S.; Bakshi, S. Recurrent Aphthous Stomatitis. Arch. Med. Health Sci. 2019, 7, 317–318. [Google Scholar] [CrossRef]
- Ślebioda, Z.; Szponar, E.; Kowalska, A. Etiopathogenesis of Recurrent Aphthous Stomatitis and the Role of Immunologic Aspects: Literature Review. Arch. Immunol. Ther. Exp. (Warsz.) 2014, 62, 205–215. [Google Scholar] [CrossRef] [Green Version]
- Giannetti, L.; Murri Dello Diago, A.; Lo Muzio, L. Recurrent Aphtous Stomatitis. Minerva Stomatol. 2018, 67, 125–128. [Google Scholar] [CrossRef] [PubMed]
- Shah, K.; Guarderas, J.; Krishnaswamy, G. Aphthous Stomatitis. Ann. Allergy Asthma Immunol. 2016, 117, 341–343. [Google Scholar] [CrossRef] [PubMed]
- Chiang, C.P.; Yu-Fong Chang, J.; Wang, Y.P.; Wu, Y.H.; Wu, Y.C.; Sun, A. Recurrent Aphthous Stomatitis—Etiology, Serum Autoantibodies, Anemia, Hematinic Deficiencies, and Management. J. Formos. Med. Assoc. 2019, 118, 1279–1289. [Google Scholar] [CrossRef] [PubMed]
- Alrashdan, M.S.; Alkhader, M. Psychological Factors in Oral Mucosal and Orofacial Pain Conditions. Eur. J. Dent. 2017, 11, 548–552. [Google Scholar] [CrossRef] [PubMed]
- Mujayanto, R. Aphtous Stomatitis Following Ageusia in SARS-CoV-2 Reinfection: A Case Report. Eur. J. Dent. 2021, 15, 817–819. [Google Scholar] [CrossRef]
- Altenburg, A.; El-Haj, N.; Micheli, C.; Puttkammer, M.; Abdel-Naser, M.B.; Zouboulis, C.C. The Treatment of Chronic Recurrent Oral Aphthous Ulcers. Dtsch. Arztebl. Int. 2014, 111, 665–673. [Google Scholar] [CrossRef] [Green Version]
- Cui, R.Z.; Bruce, A.J.; Rogers, R.S. Recurrent Aphthous Stomatitis. Clin. Dermatol. 2016, 34, 475–481. [Google Scholar] [CrossRef]
- Paradowska-Stolarz, A.M. Oral Manifestations of COVID-19: Brief Review. Dent. Med. Probl. 2021, 58, 123–126. [Google Scholar] [CrossRef]
- Amorim dos Santos, J.; Normando, A.G.C.; Carvalho da Silva, R.L.; De Paula, R.M.; Cembranel, A.C.; Santos-Silva, A.R.; Guerra, E.N.S. Oral Mucosal Lesions in a COVID-19 Patient: New Signs or Secondary Manifestations? Int. J. Infect. Dis. 2020, 97, 326–328. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Horvat Aleksijević, L.; Prpić, J.; Muhvić Urek, M.; Pezelj-Ribarić, S.; Ivančić-Jokić, N.; Peršić Bukmir, R.; Aleksijević, M.; Glažar, I. Oral Mucosal Lesions in Childhood. Dent. J. 2022, 10, 214. https://doi.org/10.3390/dj10110214
Horvat Aleksijević L, Prpić J, Muhvić Urek M, Pezelj-Ribarić S, Ivančić-Jokić N, Peršić Bukmir R, Aleksijević M, Glažar I. Oral Mucosal Lesions in Childhood. Dentistry Journal. 2022; 10(11):214. https://doi.org/10.3390/dj10110214
Chicago/Turabian StyleHorvat Aleksijević, Lorena, Jelena Prpić, Miranda Muhvić Urek, Sonja Pezelj-Ribarić, Nataša Ivančić-Jokić, Romana Peršić Bukmir, Marko Aleksijević, and Irena Glažar. 2022. "Oral Mucosal Lesions in Childhood" Dentistry Journal 10, no. 11: 214. https://doi.org/10.3390/dj10110214
APA StyleHorvat Aleksijević, L., Prpić, J., Muhvić Urek, M., Pezelj-Ribarić, S., Ivančić-Jokić, N., Peršić Bukmir, R., Aleksijević, M., & Glažar, I. (2022). Oral Mucosal Lesions in Childhood. Dentistry Journal, 10(11), 214. https://doi.org/10.3390/dj10110214