


Morphological and Ultrastructural Collagen Defects: Impact and Implications in Dentinogenesis Imperfecta


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Selection Criteria
- Human teeth, both of primary and permanent dentitions, of patients with DI ± OI. Patient age was not limited to a range;
- Teeth must exhibit collagen defects. Although this study focuses on the ultrastructural defects in dental collagen as cross-banding, other defects such as collagen size, shape and density have been included. Teeth could be examined with any assessment method;
- All study designs accepted;
- Publication date 1990 to 2021;
- Studies written in English.
- Animal studies;
- Non-DI dental pathology: Amelogenesis imperfecta, Dentin dysplasia, dens in dente;
- Studies of OI with no dental collagen examination;
- DI studies with no collagen examination;
- Dental pulp studies and regenerative studies;
- Papers published pre-1990;
- Papers with no English translation.
2.2. Data Extraction
3. Results
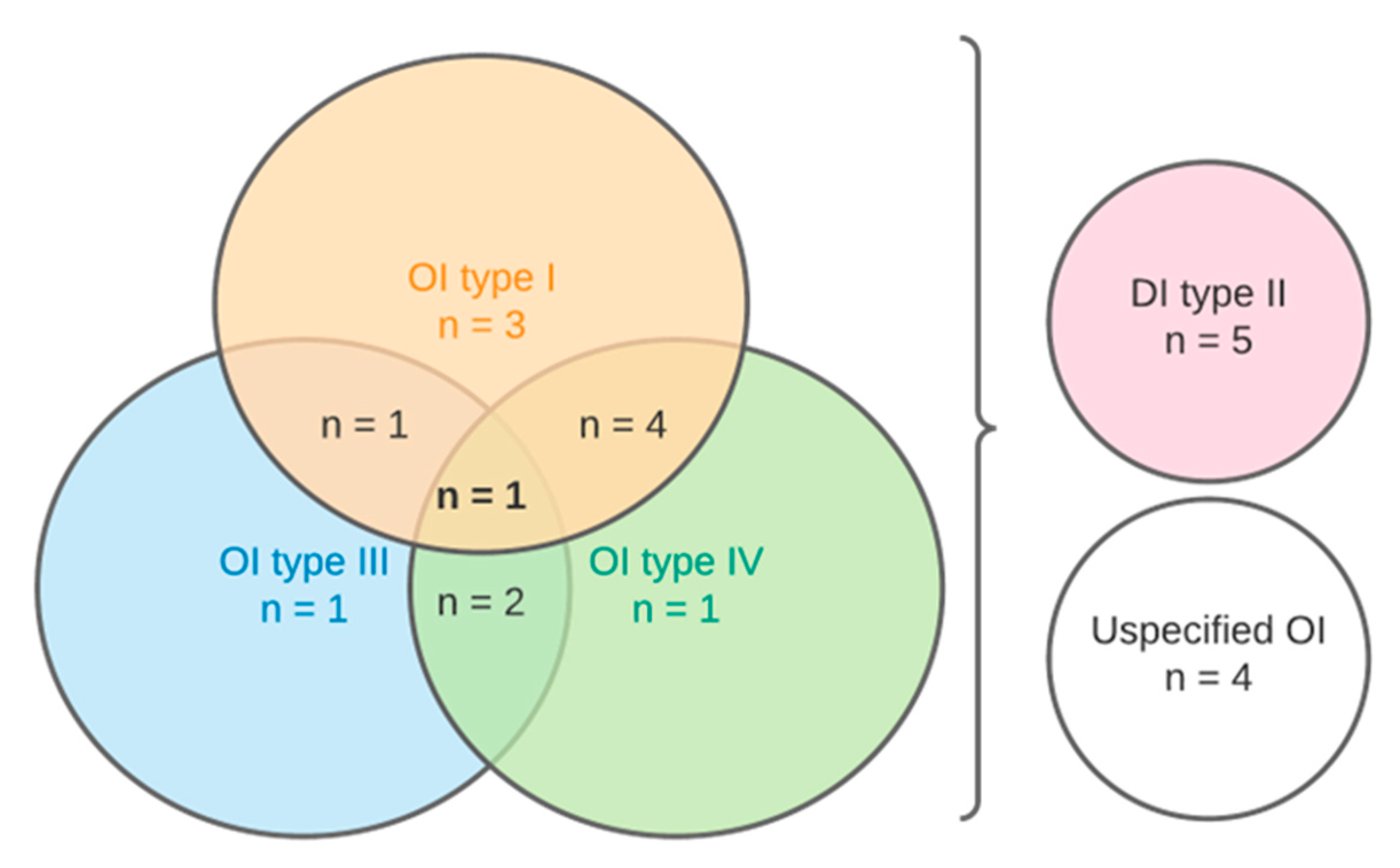
3.1. Study Selection
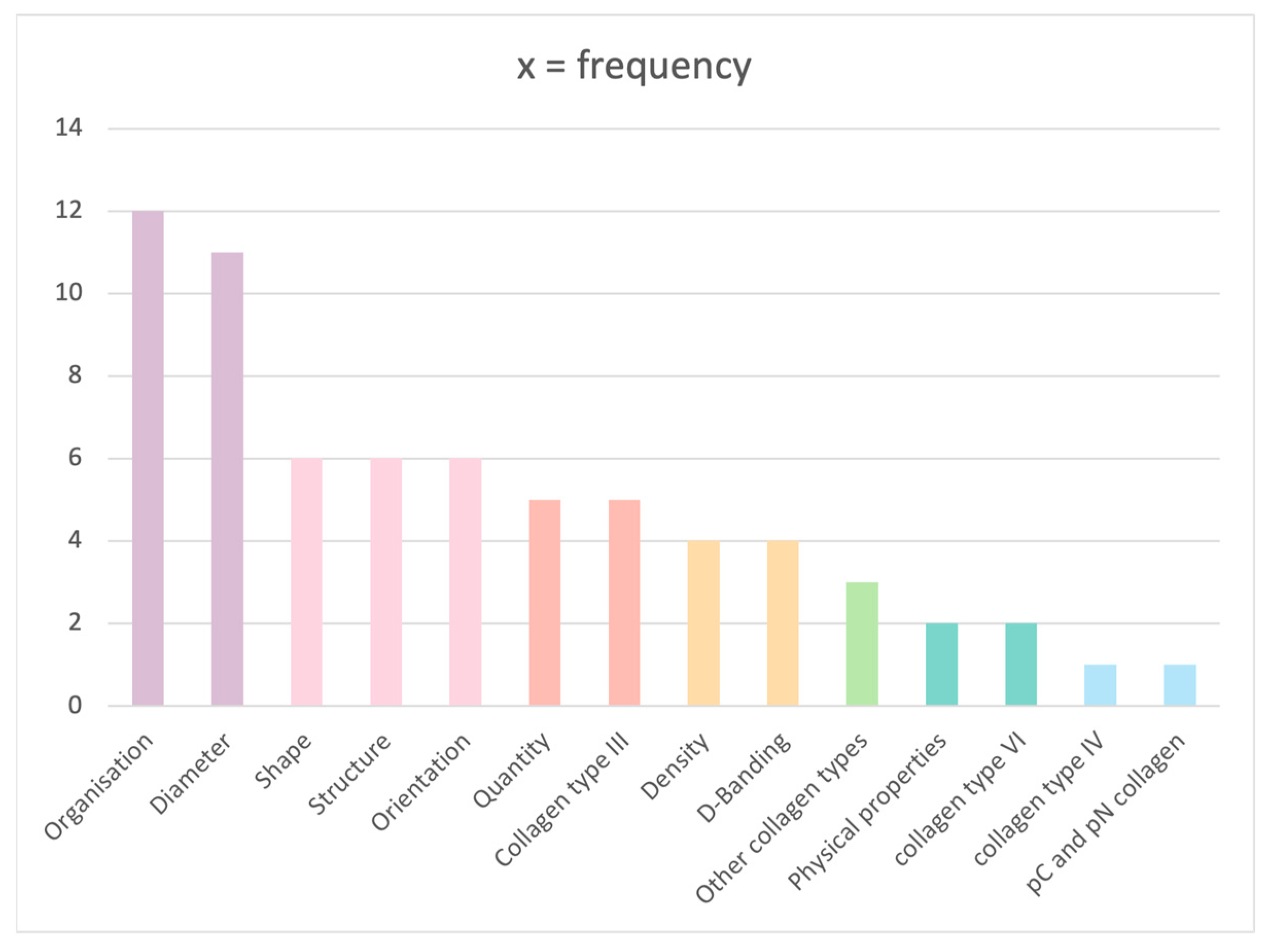
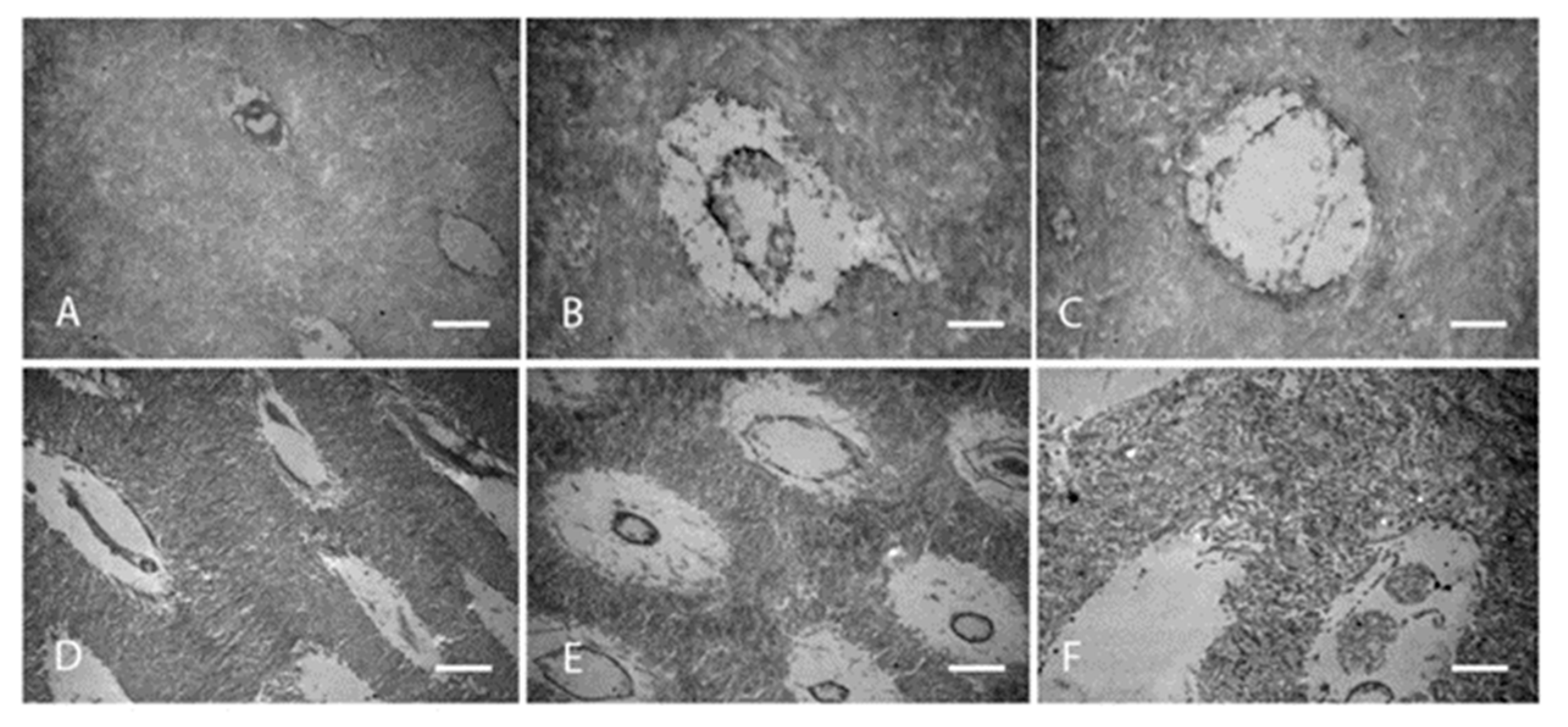
3.2. Collagen Characteristics
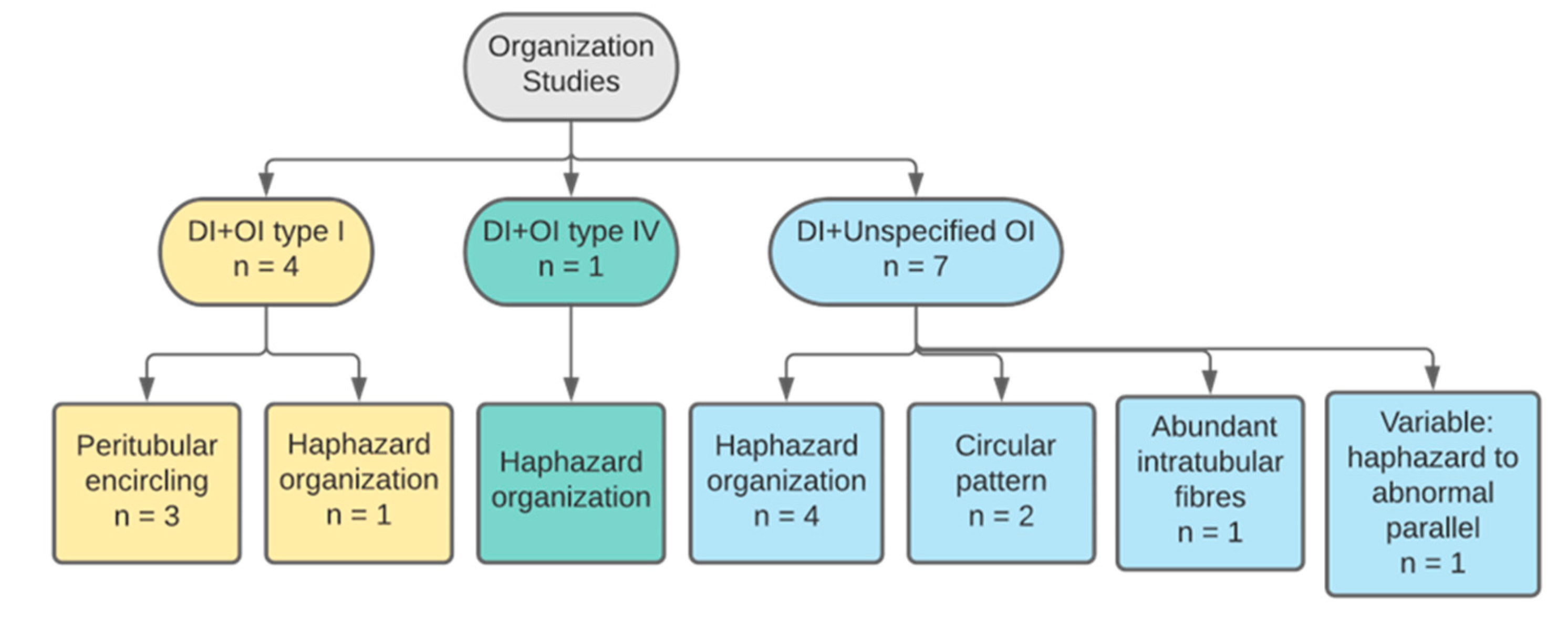
3.2.1. Collagen Organisation
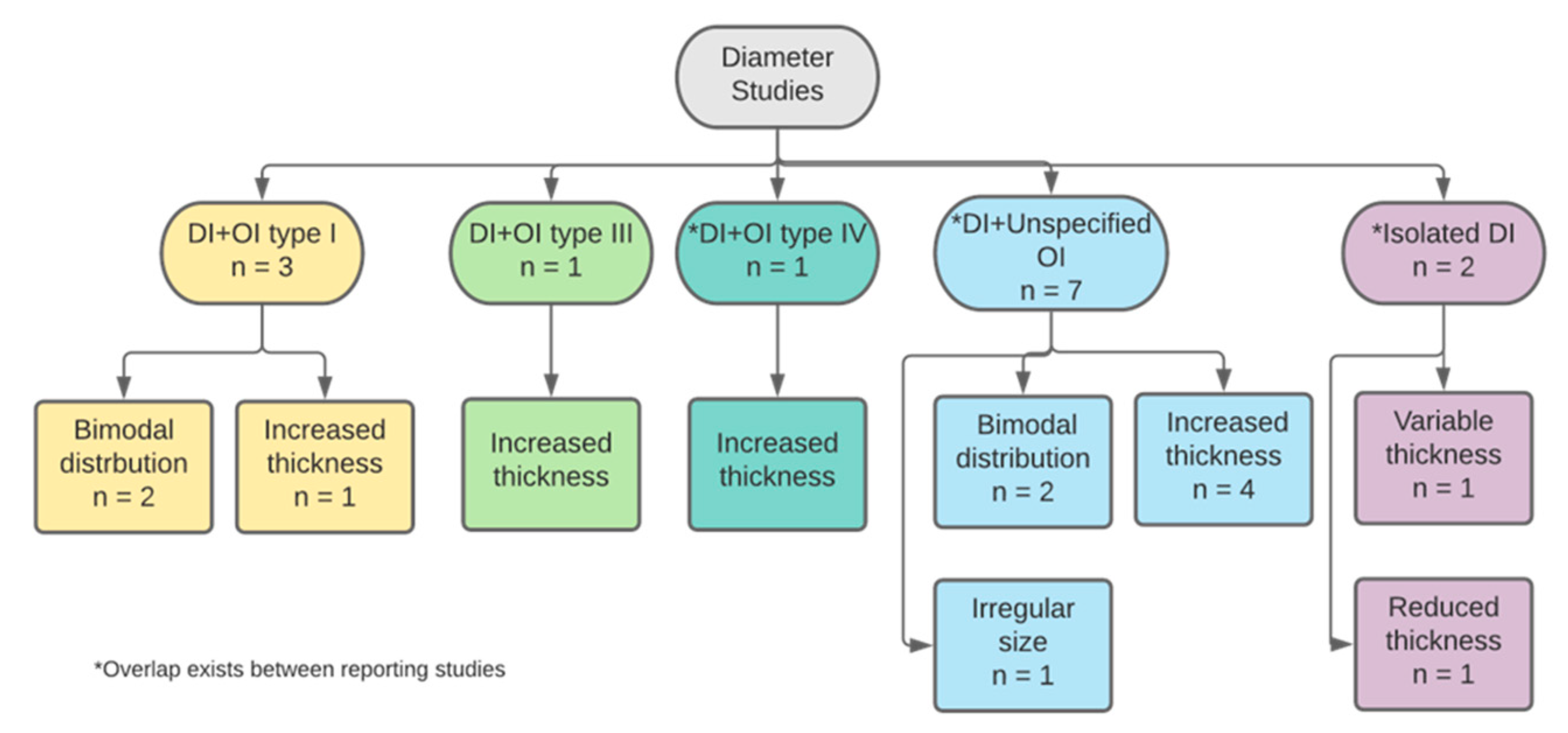
3.2.2. Collagen Diameter
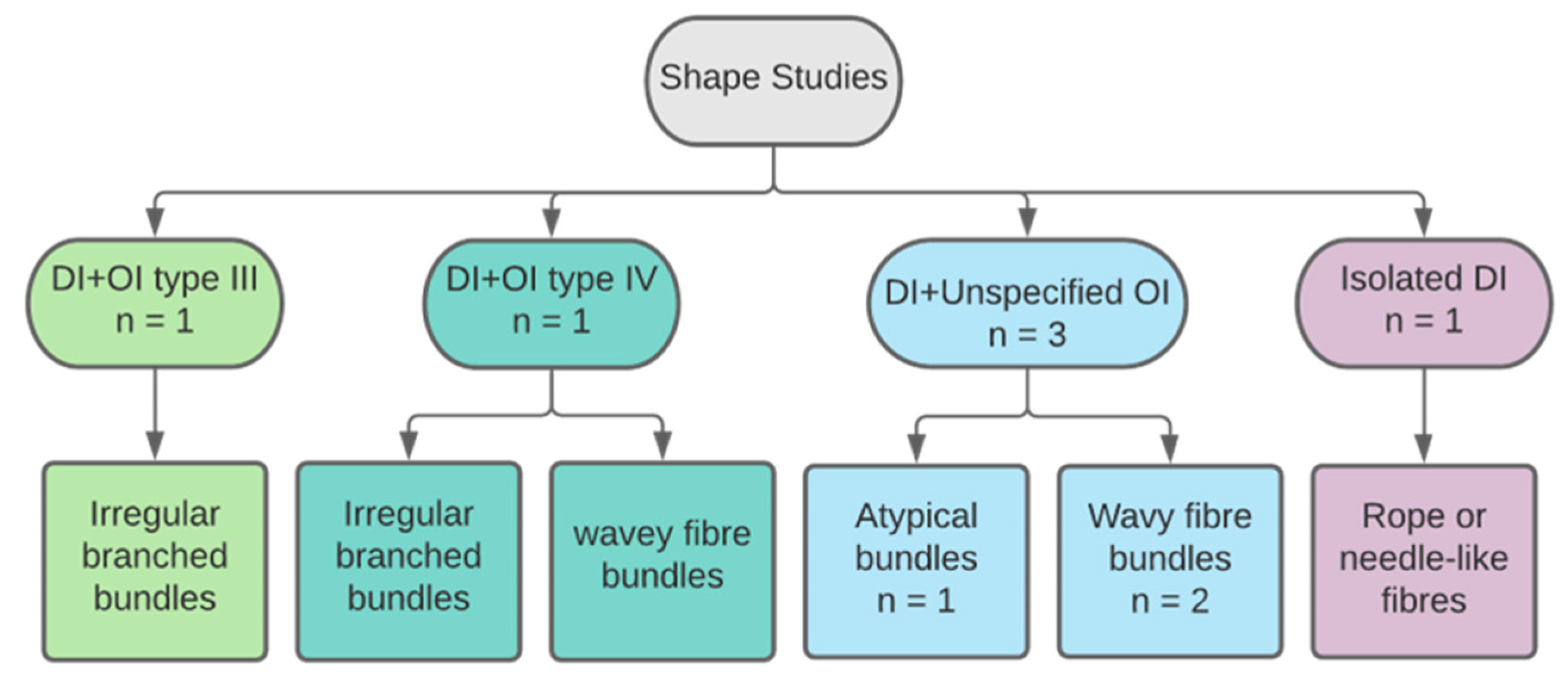
3.2.3. Collagen Shape
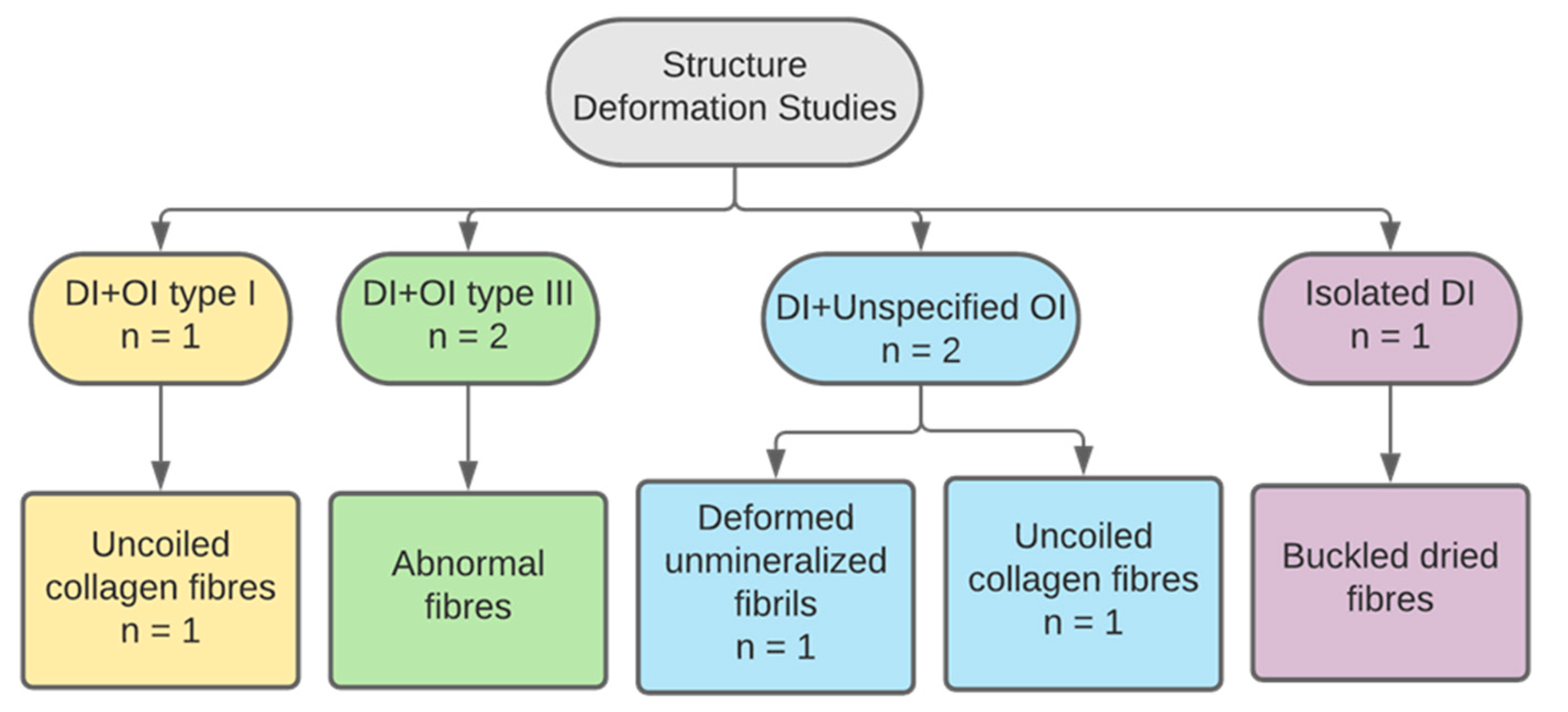
3.2.4. Collagen Structure
3.2.5. Collagen Quantity
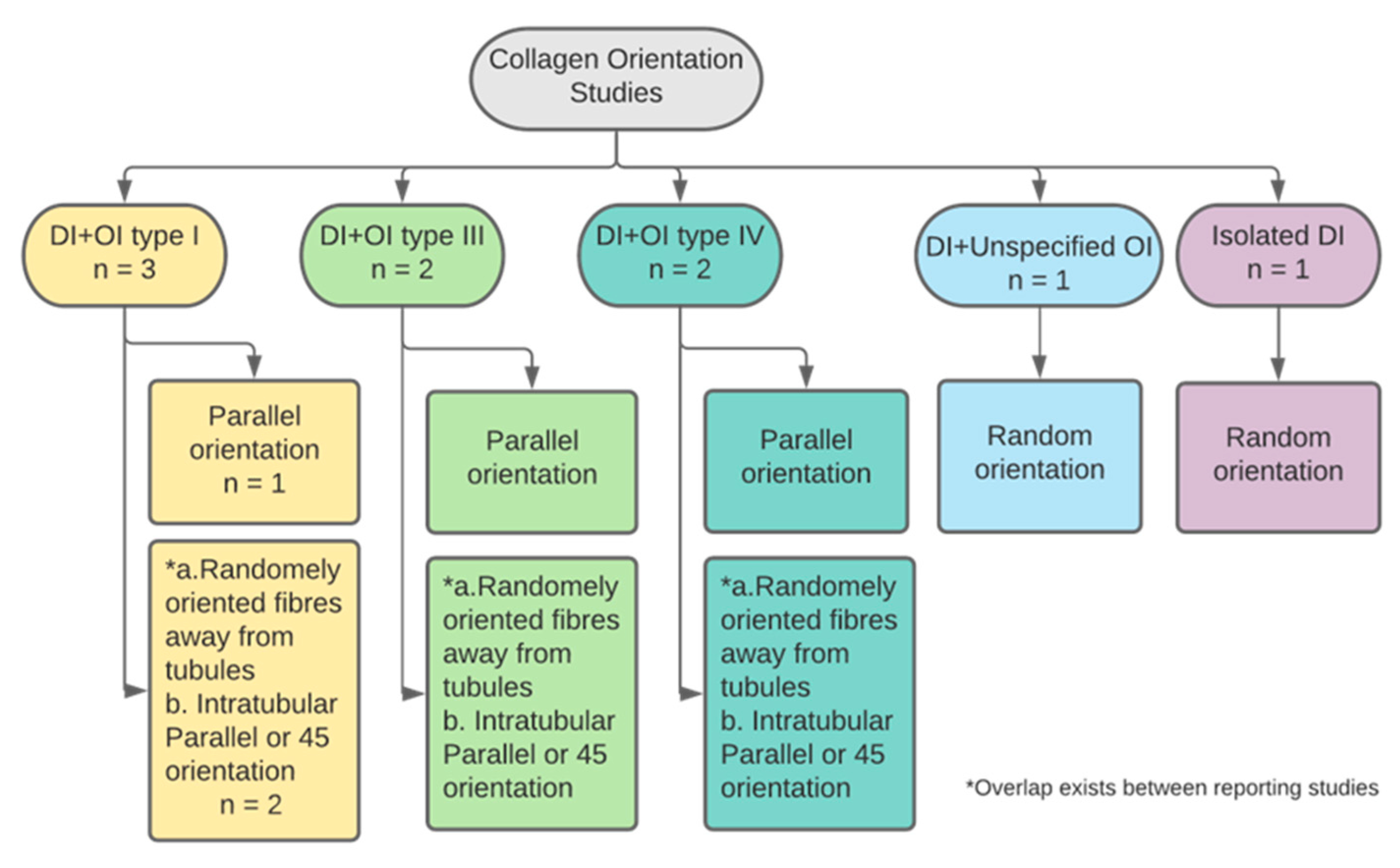
3.2.6. Collagen Orientation
3.2.7. Collagen Density
3.3. Collagen Types
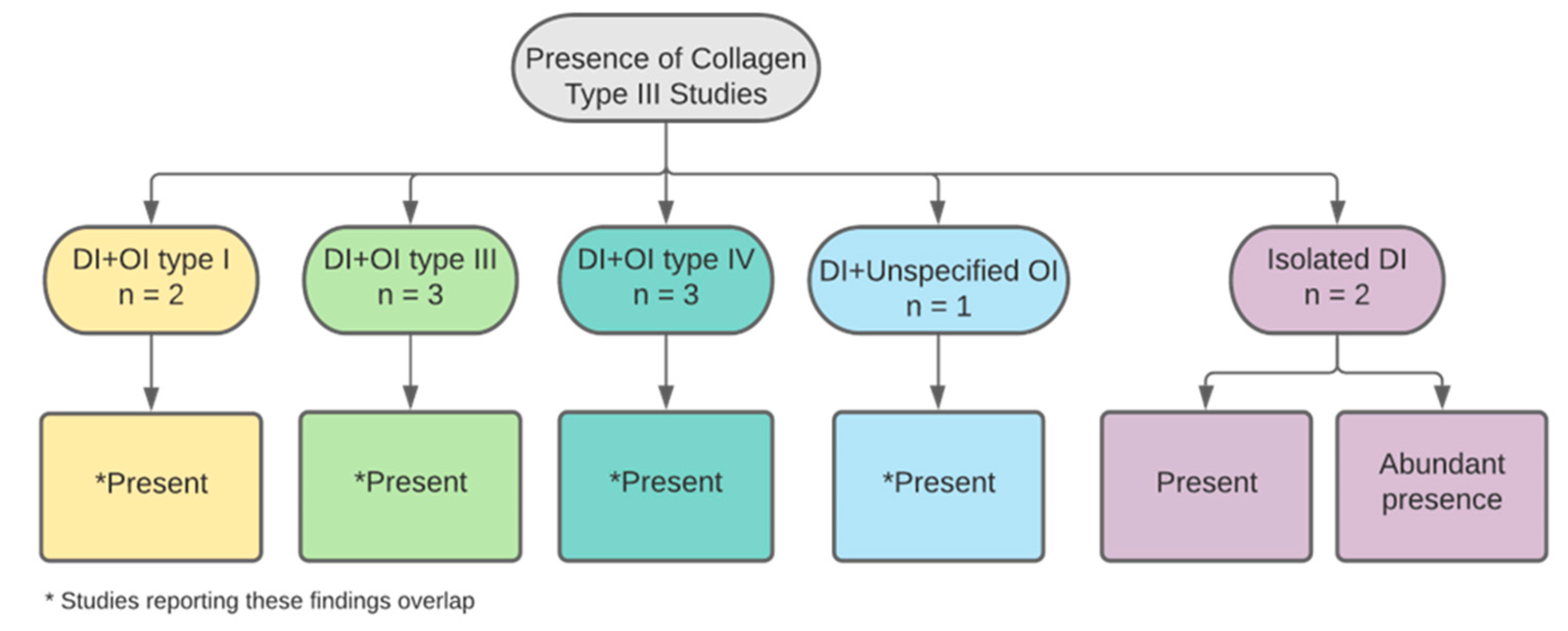
3.3.1. Collagen Type III
3.3.2. Collagen Types IV and VI
3.3.3. pC-Collagen and pN-Collagen
3.3.4. Other Types of Collagen
3.4. Physical Properties
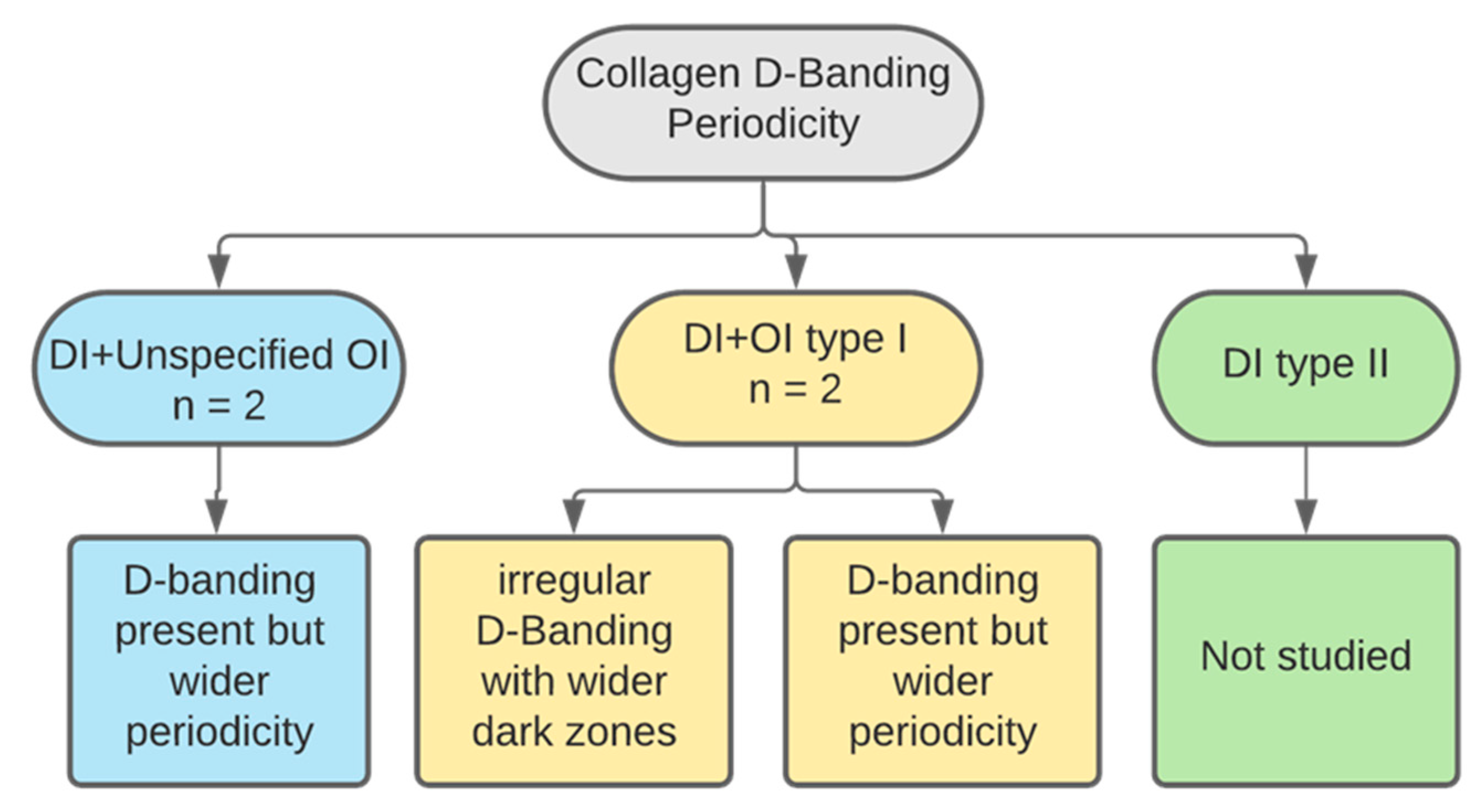
3.5. D-Banding Periodicity
3.6. Isolated DI versus OIDI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gadi, L. Morphological and Ultrstructural Collagen Defects: Impact and Implications in Dentinogenesis Imperfecta. Ph.D. Thesis, UCL (University College London), London, UK, 2022. [Google Scholar]
- Boskey, A.L. Bone composition: Relationship to bone fragility and antiosteoporotic drug effects. Bonekey Rep. 2013, 2, 447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breschi, L.; Maravic, T.; Cunha, S.R.; Comba, A.; Cadenaro, M.; Tjäderhane, L.; Pashley, D.H.; Tay, F.R.; Mazzoni, A. Dentin bonding systems: From dentin collagen structure to bond preservation and clinical applications. Dent. Mater. 2018, 34, 78–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myllyharju, J.; Kivirikko, K.I. Collagens and collagen-related diseases. Ann. Med. 2001, 33, 7–21. [Google Scholar] [CrossRef] [PubMed]
- Gelse, K.; Pöschl, E.; Aigner, T. Collagens—Structure, function, and biosynthesis. Adv. Drug Deliv. Rev. 2003, 55, 1531–1546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rauch, F.; Glorieux, F.H. Osteogenesis imperfecta. Lancet 2004, 363, 1377–1385. [Google Scholar] [CrossRef] [PubMed]
- Martin, E.; Shapiro, J.R. Osteogenesis imperfecta: Epidemiology and pathophysiology. Curr. Osteoporos. Rep. 2007, 5, 91–97. [Google Scholar] [CrossRef]
- Lindahl, K.; Åström, E.; Rubin, C.-J.; Grigelioniene, G.; Malmgren, B.; Ljunggren, Ö.; Kindmark, A. Genetic epidemiology, prevalence, and genotype–phenotype correlations in the Swedish population with osteogenesis imperfecta. Eur. J. Hum. Genet. 2015, 23, 1042–1050. [Google Scholar] [CrossRef] [Green Version]
- Sillence, D.O.; Senn, A.; Danks, D.M. Genetic heterogeneity in osteogenesis imperfecta. J. Med. Genet. 1979, 16, 101–116. [Google Scholar] [CrossRef] [Green Version]
- Marini, J.C.; Cabral, W.A. Chapter 23—Osteogenesis Imperfecta. In Genetics of Bone Biology and Skeletal Disease, 2nd ed.; Thakker, R.V., Whyte, M.P., Eisman, J.A., Igarashi, T., Eds.; Academic Press: Cambridge, MA, USA, 2018. [Google Scholar]
- Forlino, A.; Cabral, W.A.; Barnes, A.M.; Marini, J.C. New perspectives on osteogenesis imperfecta. Nat. Rev. Endocrinol. 2011, 7, 540–557. [Google Scholar] [CrossRef] [Green Version]
- Opsahl Vital, S.; Gaucher, C.; Bardet, C.; Rowe, P.S.; George, A.; Linglart, A.; Chaussain, C. Tooth dentin defects reflect genetic disorders affecting bone mineralization. Bone 2012, 50, 989–997. [Google Scholar] [CrossRef] [Green Version]
- Pallos, D.; Hart, P.S.; Cortelli, J.R.; Vian, S.; Wright, J.; Korkko, J.; Brunoni, D.; Hart, T.C. Novel COL1A1 mutation (G599C) associated with mild osteogenesis imperfecta and dentinogenesis imperfecta. Arch. Oral Biol. 2001, 46, 459–470. [Google Scholar] [CrossRef]
- Barron, M.J.; Mcdonnell, S.T.; Mackie, I.; Dixon, M.J. Hereditary dentine disorders: Dentinogenesis imperfecta and dentine dysplasia. Orphanet J. Rare Dis. 2008, 3, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shields, E.; Bixler, D.; El-Kafrawy, A. A proposed classification for heritable human dentine defects with a description of a new entity. Arch. Oral Biol. 1973, 18, 543–553. [Google Scholar] [CrossRef] [PubMed]
- Witkop, C.J. Hereditary defects of dentin. Dent. Clin. N. Am. 1975, 19, 25–45. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.K.; Saxena, P.; Jain, S.; Jain, D. Prevalence and distribution of selected developmental dental anomalies in an Indian population. J. Oral Sci. 2011, 53, 231–238. [Google Scholar] [CrossRef] [Green Version]
- Cassia, A.; Aoun, G.; El-Outa, A.; Pasquet, G.; Cavézian, R. Prevalence of Dentinogenesis imperfecta in a French population. J. Int. Soc. Prev. Community Dent. 2017, 7, 116. [Google Scholar]
- Witkop, C.J., Jr. Amelogenesis imperfecta, dentinogenesis imperfecta and dentin dysplasia revisited: Problems in classification. J. Oral Pathol. Med. 1988, 17, 547–553. [Google Scholar] [CrossRef]
- De La Dure-Molla, M.; Philippe Fournier, B.; Berdal, A. Isolated dentinogenesis imperfecta and dentin dysplasia: Revision of the classification. Eur. J. Hum. Genet. 2015, 23, 445–451. [Google Scholar] [CrossRef] [Green Version]
- Intarak, N.; Budsamongkol, T.; Theerapanon, T.; Chanamuangkon, T.; Srijunbarl, A.; Boonprakong, L.; Porntaveetus, T.; Shotelersuk, V. Tooth ultrastructure of a novel COL1A2 mutation expanding its genotypic and phenotypic spectra. Oral Dis. 2020, 27, 1257–1267. [Google Scholar] [CrossRef]
- Macdougall, M.; Dong, J.; Acevedo, A.C. Molecular basis of human dentin diseases. Am. J. Med. Genet. Part A 2006, 140, 2536–2546. [Google Scholar] [CrossRef]
- Ranta, H.; Lukinmaa, P.L.; Waltimo, J. Heritable dentin defects: Nosology, pathology, and treatment. Am. J. Med. Genet. 1993, 45, 193–200. [Google Scholar] [CrossRef]
- Orsini, G.; Majorana, A.; Mazzoni, A.; Putignano, A.; Falconi, M.; Polimeni, A.; Breschi, L. Immunocytochemical detection of dentin matrix proteins in primary teeth from patients with dentinogenesis imperfecta associated with osteogenesis imperfecta. Eur. J. Histochem. 2014, 58, 2405. [Google Scholar] [CrossRef]
- Hall, R.K.; Manière, M.C.; Palamara, J.; Hemmerlé, J. Odontoblast dysfunction in osteogenesis imperfecta: An LM, SEM, and ultrastructural study. Connect. Tissue Res. 2002, 43, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Majorana, A.; Bardellini, E.; Brunelli, P.C.; Lacaita, M.; Cazzolla, A.P.; Favia, G. Dentinogenesis imperfecta in children with osteogenesis imperfecta: A clinical and ultrastructural study. Int. J. Paediatr. Dent. 2010, 20, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Budsamongkol, T.; Intarak, N.; Theerapanon, T.; Yodsanga, S.; Porntaveetus, T.; Shotelersuk, V. A novel mutation in COL1A2 leads to osteogenesis imperfecta/Ehlers-Danlos overlap syndrome with brachydactyly. Genes Dis. 2019, 6, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Nutchoey, O.; Intarak, N.; Theerapanon, T.; Thaweesapphithak, S.; Boonprakong, L.; Srijunbarl, A.; Porntaveetus, T.; Shotelersuk, V. Phenotypic features of dentinogenesis imperfecta associated with osteogenesis imperfecta and COL1A2 mutations. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2021, 131, 694–701. [Google Scholar] [CrossRef]
- Cochrane Effective Practice and Organisation of Care (EPOC). Data Collection Form. EPOC Resources for Review Authors, 2013. Available online: epoc.cochrane.org/resources/epoc-specific-resources-review-authors (accessed on 1 December 2020).
- Waltimo, J.; Ojanotko-Harri, A.; Lukinmaa, P.L. Mild forms of dentinogenesis imperfecta in association with osteogenesis imperfecta as characterized by light and transmission electron microscopy. J. Oral Pathol. Med. 1996, 25, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, S.; Strange, A.P.; Aguayo, S.; Shinawi, A.; Harith, N.; Mohamed-Ibrahim, N.; Siddiqui, S.; Parekh, S.; Bozec, L. Phenotypic Properties of Collagen in Dentinogenesis Imperfecta Associated with Osteogenesis Imperfecta. Int. J. Nanomed. 2019, 14, 9423–9435. [Google Scholar] [CrossRef] [Green Version]
- Kinney, J.H.; Pople, J.A.; Driessen, C.H.; Breunig, T.M.; Marshall, G.W.; Marshall, S.J. Intrafibrillar mineral may be absent in dentinogenesis imperfecta type II (DI-II). J. Dent. Res. 2001, 80, 1555–1559. [Google Scholar] [CrossRef] [Green Version]
- Duan, X.; Liu, Z.; Gan, Y.; Xia, D.; Li, Q.; Li, Y.; Yang, J.; Gao, S.; Dong, M. Mutations in COL1A1 gene change dentin nanostructure. Anat. Rec. 2016, 299, 511–519. [Google Scholar] [CrossRef] [Green Version]
- Josic, U.; Maravic, T.; Bossù, M.; Cadenaro, M.; Comba, A.; Ierardo, G.; Polimeni, A.; Florenzano, F.; Breschi, L.; Mazzoni, A. Morphological Characterization of Deciduous Enamel and Dentin in Patients Affected by Osteogenesis Imperfecta. Appl. Sci. 2020, 10, 7835. [Google Scholar] [CrossRef]
- Waltimo, J.; Ranta, H.; Lukinmaa, P.L. Ultrastructure of dentin matrix in heritable dentin defects. Scanning Microsc. 1995, 9, 185–197; discussion 197–198. [Google Scholar]
- Waltimo, J.; Risteli, L.; Risteli, J.; Lukinmaa, P.L. Altered collagen expression in human dentin: Increased reactivity of type III and presence of type VI in dentinogenesis imperfecta, as revealed by immunoelectron microscopy. J. Histochem. Cytochem. 1994, 42, 1593–1601. [Google Scholar] [CrossRef] [Green Version]
- Waltimo, J. Hyperfibers and vesicles in dentin matrix in dentinogenesis imperfecta (DI) associated with osteogenesis imperfecta (OI). J. Oral Pathol. Med. 1994, 23, 389–393. [Google Scholar] [CrossRef] [PubMed]
- De Coster, P.J.; Cornelissen, M.; De Paepe, A.; Martens, L.C.; Vral, A. Abnormal dentin structure in two novel gene mutations [COL1A1, Arg134Cys] and [ADAMTS2, Trp795-to-ter] causing rare type I collagen disorders. Arch. Oral Biol. 2007, 52, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Waltimo, J. Unusual forms of collagen in human dentin. Matrix Biol. 1996, 15, 53–56. [Google Scholar] [CrossRef]
- Council, O. Guideline on dental management of heritable dental developmental anomalies. Pediatr. Dent. 2013, 35, 179–184. [Google Scholar]
- Frassetto, A.; Breschi, L.; Turco, G.; Marchesi, G.; Di Lenarda, R.; Tay, F.R.; Pashley, D.H.; Cadenaro, M. Mechanisms of degradation of the hybrid layer in adhesive dentistry and therapeutic agents to improve bond durability—A literature review. Dent. Mater. 2016, 32, e41–e53. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, M.; Kulkarni, A.B.; Young, M.; Boskey, A. Dentin: Structure, composition and mineralization. Front. Biosci. Elite Ed. 2011, 3, 711–735. [Google Scholar] [CrossRef]
- Holbrook, K.A.; Byers, P.H. Diseases of the extracellular matrix: Structural alterations of collagen fibrils in skin. In Connective Tissue Disease Molecular Pathology of the Extracellular Matrix; CRC Press: Boca Raton, FL, USA, 1987; pp. 101–140. [Google Scholar]
- Nudelman, F.; Pieterse, K.; George, A.; Bomans, P.H.; Friedrich, H.; Brylka, L.J.; Hilbers, P.A.; De With, G.; Sommerdijk, N.A. The role of collagen in bone apatite formation in the presence of hydroxyapatite nucleation inhibitors. Nat. Mater. 2010, 9, 1004–1009. [Google Scholar] [CrossRef] [Green Version]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| OI Type | Gene Mutation | Severity | Clinical Presentation |
|---|---|---|---|
| Defects in collagen synthesis and structure | |||
| I | COL1A1 | Mild |
|
| II | COL1A1–COL1A2 | Lethal |
|
| III | COL1A1–COL1A2 | Progress with age |
|
| IV | COL1A1–COL1A2 | Moderately severe |
|
| Shields 1973 [15] | Witkop 1988 [19] | Barron et al. 2008 [14] | De La Dure-Molla M et al. 2015 [20] | Clinical Presentation | Associated Gene |
| Type I DI/DI associated with OI/syndromic DI | Dentinogenesis Imperfecta | DGI-I | - |
| COL1A1 COL1A2 |
| Type II DI | Hereditary opalescent dentin | DGI-II | Moderate isolated DI |
| DSPP |
| Type III DI | Brandywine isolate | DGI-III | Severe isolated DI |
| DSPP |
| Author(s) | Date | Study Design | Dentition | DI Type | OI Type | Parameter Studied |
|---|---|---|---|---|---|---|
| Intarak et al. [21] | 2020 | Cross sectional | 1 primary and 1 permanent teeth | Type I | Type IV |
|
| Ranta et al. [23] | 1993 | Review | Unspecified | Types I and II | Types I and III |
|
| Orsini et al. [24] | 2014 | Cross sectional | Primaryunspecified number | Type I | Type I |
|
| Hall et al. [25] | 2002 | Cross sectional | Primary and permanentunspecified number | Types I and II | Types I, III and IV |
|
| Majorana et al. [26] | 2010 | Cross sectional | 7 Primary teeth | Type I | Types I, III and IV |
|
| Budsamongkol et al. [27] | 2019 | Cross sectional | 1 primary tooth | Type I | Type III |
|
| Nutchoey et al. [28] | 2021 | Cross sectional | 3 primary teeth | Type I | unspecified |
|
| Waltimo et al. [30] | 1996 | Cross sectional | Primary and permanentunspecified number | Type I | Type I |
|
| Ibrahim et al. [31] | 2019 | Cross sectional | 8 Primary teeth | Type I | Type I |
|
| Kinney et al. [32] | 2001 | Cross sectional | 3 permanent teeth | Type II | unclear |
|
| Duan et al. [33] | 2016 | Cross sectional | 28 Permanent teeth | Type I | unspecified |
|
| Josic et al. [34] | 2020 | Cross sectional | Primaryunspecified number | Type I | Unspecified |
|
| Waltimo et al. [35] | 1995 | Cross sectional | Primaryunspecified number | Types I and II | Types I and IV |
|
| Waltimo et al. [36] | 1994 | Review | Primary and permanentunspecified number | Types I and II | Types I and IV |
|
| Waltimo [37] | 1994 | Case series | 8 primary teeth | Type I | Types I and IV |
|
| De Coster et al. [38] | 2006 | Cross sectional | Primary and permanentunspecified number | Type I | Types III and IV |
|
| Waltimo [39] | 1996 | Cross sectional | 2 primary teeth | Type I | Types I and IV |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gadi, L.S.A.; Chau, D.Y.S.; Parekh, S. Morphological and Ultrastructural Collagen Defects: Impact and Implications in Dentinogenesis Imperfecta. Dent. J. 2023, 11, 95. https://doi.org/10.3390/dj11040095
Gadi LSA, Chau DYS, Parekh S. Morphological and Ultrastructural Collagen Defects: Impact and Implications in Dentinogenesis Imperfecta. Dentistry Journal. 2023; 11(4):95. https://doi.org/10.3390/dj11040095
Chicago/Turabian StyleGadi, Lubabah S. A., David Y. S. Chau, and Susan Parekh. 2023. "Morphological and Ultrastructural Collagen Defects: Impact and Implications in Dentinogenesis Imperfecta" Dentistry Journal 11, no. 4: 95. https://doi.org/10.3390/dj11040095
APA StyleGadi, L. S. A., Chau, D. Y. S., & Parekh, S. (2023). Morphological and Ultrastructural Collagen Defects: Impact and Implications in Dentinogenesis Imperfecta. Dentistry Journal, 11(4), 95. https://doi.org/10.3390/dj11040095