
Is a Wiggling-Motion Modified Two-Step Impression Technique as Accurate as Conventional Techniques in Restorative Dentistry?


Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yamalik, N. Quality systems in dentistry. Part The increasing pressure for quality and implementation of quality assurance and improvement (QA/I) models in health care. Int. Dent. J. 2007, 57, 338–346. [Google Scholar] [CrossRef] [PubMed]
- Holm, C.; Tidehag, P.; Tillberg, A.; Molin, M. Longevity and quality of FPDs: A retrospective study of restorations 30, 20, and 10 years after insertion. Int. J. Prosthodont. 2003, 16, 283–289. [Google Scholar] [PubMed]
- Ahlholm, P.; Sipilä, K.; Vallittu, P.; Jakonen, M.; Kotiranta, U. Digital Versus Conventional Impressions in Fixed Prosthodontics: A Review. J. Prosthodont. 2018, 27, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Bandiaky, O.N.; Le Bars, P.; Gaudin, A.; Hardouin, J.B.; Cheraud-Carpentier, M.; Mbodj, E.B.; Soueidan, A. Comparative assessment of complete-coverage, fixed tooth-supported prostheses fabricated from digital scans or conventional impressions: A systematic review and meta-analysis. J. Prosthet. Dent. 2022, 127, 71–79. [Google Scholar] [CrossRef]
- Parize, H.; Dias Corpa Tardelli, J.; Bohner, L.; Sesma, N.; Muglia, V.A.; Cândido Dos Reis, A. Digital versus conventional workflow for the fabrication of physical casts for fixed prosthodontics: A systematic review of accuracy. J. Prosthet. Dent. 2022, 128, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Naumovski, B.; Kapushevska, B. Dimensional Stability and Acuracy of Silicone—Based Impression Materials Using Different Impression Techniques—A Literature Review. Prilozi 2017, 38, 131–138. [Google Scholar] [CrossRef]
- Varvara, G.; Sinjari, B.; Bernardi, S.; Turkyilmaz, I.; Malvezzi, V.; Piattelli, M.; Caputi, S. Comparative surface detail reproduction for elastomeric impression materials: Study on reproducibility performance. J. Biol. Regul Homeost. Agents 2021, 35, 161–169. [Google Scholar]
- Samet, N.; Shohat, M.; Livny, A.; Weiss, E.I. A clinical evaluation of fixed partial denture impressions. J. Prosthet. Dent. 2005, 94, 112–117. [Google Scholar] [CrossRef]
- Christensen, G.J. Ensuring accuracy and predictability with double-arch impressions. J. Am. Dent. Assoc. 2008, 139, 1123–1125. [Google Scholar] [CrossRef]
- Johnson, G.H.; Mancl, L.A.; Schwedhelm, E.R.; Verhoef, D.R.; Lepe, X. Clinical trial investigating success rates for polyether and vinyl polysiloxane impressions made with full-arch and dual-arch plastic trays. J. Prosthet. Dent. 2010, 103, 13–22. [Google Scholar] [CrossRef]
- Caputi, S.; Varvara, G. Dimensional accuracy of resultant casts made by a monophase, one-step and two-step, and a novel two-step putty/light-body impression technique: An in vitro study. J. Prosthet. Dent. 2008, 99, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Mishra, S.; Chowdhary, R. Linear dimensional accuracy of a polyvinyl siloxane of varying viscosities using different impression techniques. J. Investig. Clin. Dent. 2010, 1, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Manoj, S.S.; Cherian, K.P.; Chitre, V.; Aras, M. A Comparative Evaluation of the Linear Dimensional Accuracy of Four Impression Techniques using Polyether Impression Material. J. Indian Prosthodont. Soc. 2013, 13, 428–438. [Google Scholar] [CrossRef] [PubMed]
- Basapogu, S.; Pilla, A.; Pathipaka, S. Dimensional Accuracy of Hydrophilic and Hydrophobic VPS Impression Materials Using Different Impression Techniques—An In vitro Study. J. Clin. Diagn. Res. 2016, 10, ZC56–ZC59. [Google Scholar] [PubMed]
- Nissan, J.; Rosner, O.; Rosen, G.; Naishlos, S.; Zenziper, E.; Zelikman, H.; Lavi, D.; Chaushu, L. Influence of Vinyl Polysiloxane Impression Techniques on Marginal Fit of Metal Frameworks for Fixed Partial Dentures. Materials 2020, 13, 4684. [Google Scholar] [CrossRef]
- Nissan, J.; Laufer, B.Z.; Brosh, T.; Assif, D. Accuracy of three polyvinyl siloxane putty-wash impression techniques. J. Prosthet. Dent. 2000, 83, 161–165. [Google Scholar] [CrossRef]
- Dugal, R.; Railkar, B.; Musani, S. Comparative evaluation of dimensional accuracy of different polyvinyl siloxane putty-wash impression techniques-in vitro study. J. Int. Oral Health 2013, 5, 85–94. [Google Scholar]
- Nissan, J.; Rosner, O.; Bukhari, M.A.; Ghelfan, O.; Pilo, R. Effect of various putty-wash impression techniques on marginal fit of cast crowns. Int. J. Periodontics Restor. Dent. 2013, 33, e37–e42. [Google Scholar] [CrossRef]
- Levartovsky, S.; Zalis, M.; Pilo, R.; Harel, N.; Ganor, Y.; Brosh, T. The effect of one-step vs. two-step impression techniques on long-term accuracy and dimensional stability when the finish line is within the gingival sulcular area. J. Prosthodont. 2014, 23, 124–133. [Google Scholar] [CrossRef]
- Singh, K.; Sahoo, S.; Prasad, K.D.; Goel, M.; Singh, A. Effect of different impression techniques on the dimensional accuracy of impressions using various elastomeric impression materials: An in vitro study. J. Contemp. Dent. Pract. 2012, 13, 98–106. [Google Scholar] [CrossRef]
- Mann, K.; Davids, A.; Range, U.; Richter, G.; Boening, K.; Reitemeier, B. Experimental study on the use of spacer foils in two-step putty and wash impression procedures using silicone impression materials. J. Prosthet. Dent. 2015, 113, 316–322. [Google Scholar] [CrossRef] [PubMed]
- Chugh, A.; Arora, A.; Singh, V.P. Accuracy of different putty-wash impression techniques with various spacer thickness. Int. J. Clin. Pediatr. Dent. 2012, 5, 33–38. [Google Scholar] [PubMed]
- Vitti, R.P.; da Silva, M.A.; Consani, R.L.; Sinhoreti, M.A. Dimensional accuracy of stone casts made from silicone-based impression materials and three impression techniques. Braz. Dent. J. 2013, 24, 498–502. [Google Scholar] [CrossRef]
- Nissan, J.; Gross, M.; Shifman, A.; Assif, D. Effect of wash bulk on the accuracy of polyvinyl siloxane putty-wash impressions. J. Oral Rehabil. 2002, 29, 357–361. [Google Scholar] [CrossRef] [PubMed]
- Gautam, N.; Ahmed, R.; Sharma, S.; Madineni, P.K.; Hasan, S. A Comparative Study to Evaluate the Accuracy of Various Spacer Thickness for Polyvinyl Siloxane Putty-wash Impression Techniques: An In Vitro Study. Int. J. Clin. Pediatr. Dent. 2020, 13, 536–542. [Google Scholar] [CrossRef] [PubMed]
- Hung, S.H.; Purk, J.H.; Tira, D.E.; Eick, J.D. Accuracy of one-step versus two-step putty wash addition silicone impression technique. J. Prosthet. Dent. 1992, 67, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Nimonkar, S.V.; Belkhode, V.M.; Godbole, S.R.; Nimonkar, P.V.; Dahane, T.; Sathe, S. Comparative Evaluation of the Effect of Chemical Disinfectants and Ultraviolet Disinfection on Dimensional Stability of the Polyvinyl Siloxane Impressions. J. Int. Soc. Prev. Community Dent. 2019, 9, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Idris, B.; Houston, F.; Claffey, N. Comparison of the dimensional accuracy of one- and two-step techniques with the use of putty/wash addition silicone impression materials. J. Prosthet. Dent. 1995, 74, 535–541. [Google Scholar] [CrossRef]
- Levartovsky, S.; Levy, G.; Brosh, T.; Harel, N.; Ganor, Y.; Pilo, R. Dimensional stability of polyvinyl siloxane impression material reproducing the sulcular area. Dent. Mater. J. 2013, 32, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Fenske, C. The influence of five impression techniques on the dimensional accuracy of master models. Braz. Dent. J. 2000, 11, 19–27. [Google Scholar]
- Silva, S.C.; Messias, A.M.; Abi-Rached, F.O.; de Souza, R.F.; Reis, J.M. Accuracy of Gypsum Casts after Different Impression Techniques and Double Pouring. PLoS ONE 2016, 11, e0164825. [Google Scholar] [CrossRef] [PubMed]
- Pande, N.A.; Parkhedkar, R.D. An evaluation of dimensional accuracy of one-step and two-step impression technique using addition silicone impression material: An in vitro study. J. Indian Prosthodont. Soc. 2013, 13, 254–259. [Google Scholar] [CrossRef] [PubMed]
- Pastoret, M.H.; Krastl, G.; Bühler, J.; Weiger, R.; Zitzmann, N.U. Accuracy of a separating foil impression using a novel polyolefin foil compared to a custom tray and a stock tray technique. J. Adv. Prosthodont. 2017, 9, 287–293. [Google Scholar] [CrossRef]
- Varvara, G.; Murmura, G.; Sinjari, B.; Cardelli, P.; Caputi, S. Evaluation of defects in surface detail for monophase, 2-phase, and 3-phase impression techniques: An in vitro study. J. Prosthet. Dent. 2015, 113, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.A.; Tushar Nezam, S.; Singh, P.; Kumari, N.; Singh, S.S. Comparison and Evaluation of Linear Dimensional Accuracy of Three Elastomeric Impression Materials at Different Time Intervals Using Vision Inspection System: An In Vitro Study. J. Int. Soc. Prev. Community Dent. 2020, 10, 736–742. [Google Scholar] [PubMed]
- Kamble, S.S.; Khandeparker, R.V.; Somasundaram, P.; Raghav, S.; Babaji, R.P.; Varghese, T.J. Comparative Evaluation of Dimensional Accuracy of Elastomeric Impression Materials when Treated with Autoclave, Microwave, and Chemical Disinfection. J. Int. Oral Health 2015, 7, 22–24. [Google Scholar]
- Soganci, G.; Cinar, D.; Caglar, A.; Yagiz, A. 3D evaluation of the effect of disinfectants on dimensional accuracy and stability of two elastomeric impression materials. Dent. Mater. J. 2018, 37, 675–684. [Google Scholar] [CrossRef]
- Pal, P.K.; Kamble, S.S.; Chaurasia, R.R.; Chaurasia, V.R.; Tiwari, S.; Bansal, D. Evaluation of Different Disinfactants on Dimensional Accuracy and Surface Quality of Type IV Gypsum Casts Retrieved from Elastomeric Impression Materials. J. Int. Oral Health 2014, 6, 77–81. [Google Scholar]
- Özdemir, H.; Pekince, K.A. Evaluation of the effect of storage time and disinfectant solutions on the dimensional accuracy of impression materials with digital radiography. Dent. Med. Probl. 2019, 56, 67–74. [Google Scholar] [CrossRef]
- Hsu, K.L.; Balhaddad, A.A.; Martini Garcia, I.; Collares, F.M.; Dhar, V.; DePaola, L.; Melo, M.A. 3D cone-beam C.T. imaging used to determine the effect of disinfection protocols on the dimensional stability of full arch impressions. Saudi Dent. J. 2021, 33, 453–461. [Google Scholar] [CrossRef]
- Guntupalli, Y.; Ganesh, S.B.; Jayalakshmi, S. Effect of disinfectants on the tear strength of addition silicone impression material—An in vitro study. J. Adv. Pharm. Technol. Res. 2022, 13 (Suppl. S2), S458–S461. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
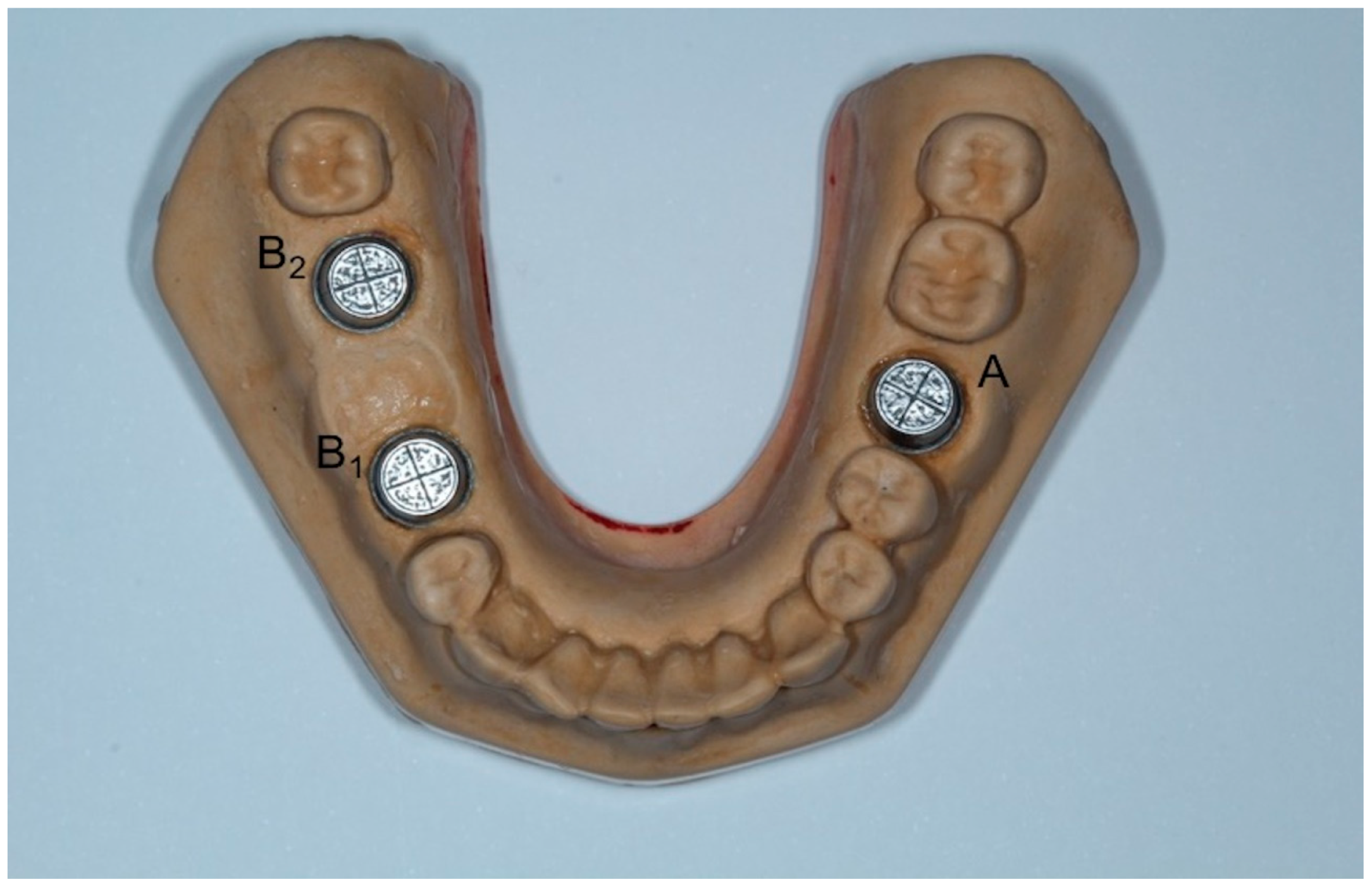
| Distance (μm) | DM | CO | ME | WI | MM |
|---|---|---|---|---|---|
| MD | 6064 a (59.49) | 6067 a (84.75) | 6080 a (44.59) | 6070 a (27.34) | 6029 b (37.50) |
| BL | 6073 a (55.00) | 6049 ab (81.58) | 6068 a (67.25) | 6042 ab (37.00) | 6026 b (20.84) |
| H | 6017 b (95.58) | 6001 ab (72.67) | 6029 ab (78.83) | 6023 ab (72.92) | 6052 a (44.67) |
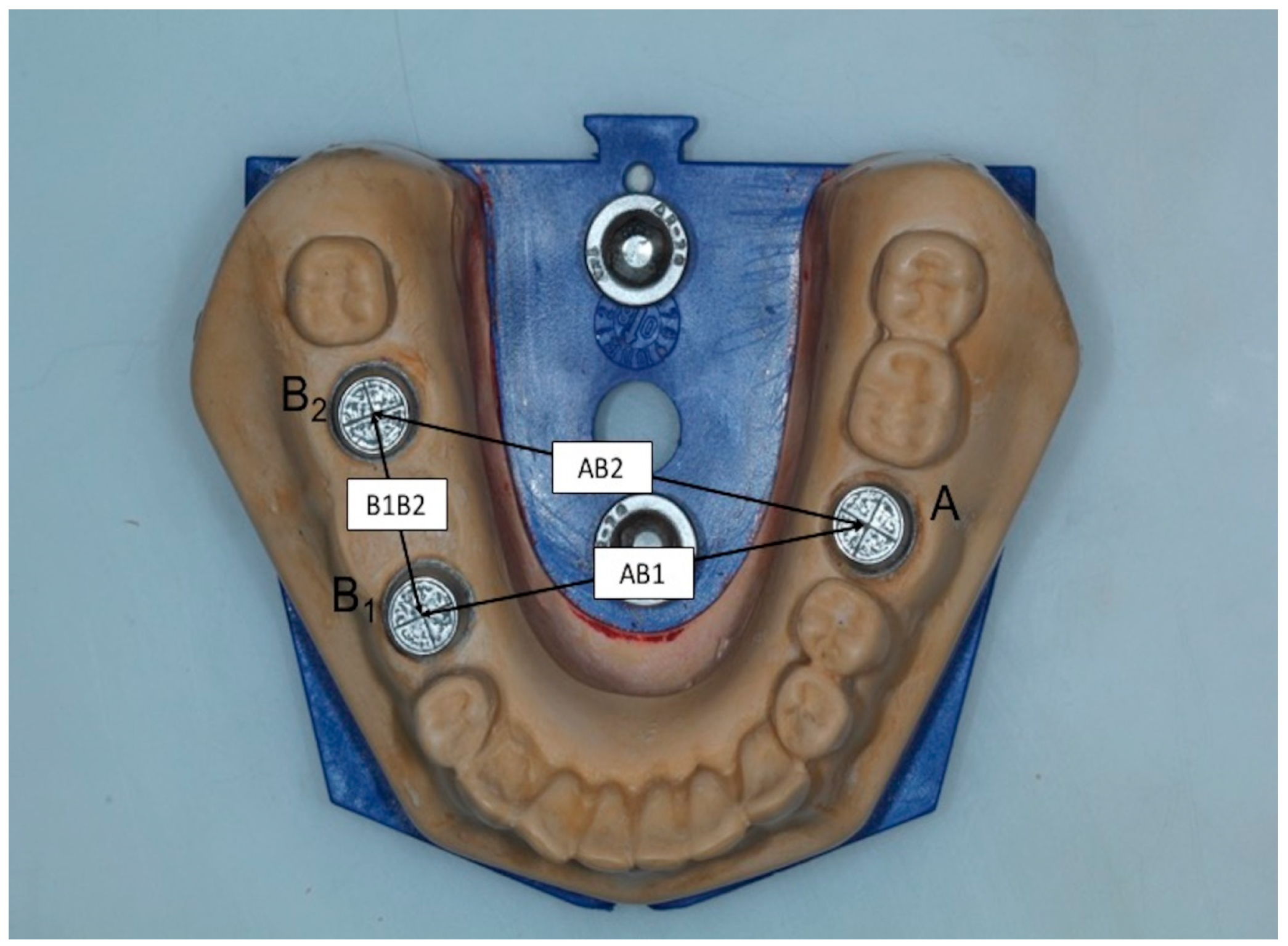
| Distance (μm) | DM | CO | ME | WI | MM |
|---|---|---|---|---|---|
| AB1 | 40,109 a (41.02) | 40,104 a (69.79) | 40,122 a (64.62) | 40,108 a (52.98) | 40,046 a (54.43) |
| AB2 | 44,676 a (29.88) | 44,718 ab (36.06) | 44,734 ab (69.10) | 44,748 b (52.60) | 44,720 ab (48.20) |
| B1B2 | 16,847 a (57.00) | 16,861 a (71.06) | 16,857 a (91.49) | 16,795 a (50.77) | 16,806 a (64.56) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zappi, A.; Papazoglou, E.; Anagnostou, M. Is a Wiggling-Motion Modified Two-Step Impression Technique as Accurate as Conventional Techniques in Restorative Dentistry? Dent. J. 2023, 11, 139. https://doi.org/10.3390/dj11050139
Zappi A, Papazoglou E, Anagnostou M. Is a Wiggling-Motion Modified Two-Step Impression Technique as Accurate as Conventional Techniques in Restorative Dentistry? Dentistry Journal. 2023; 11(5):139. https://doi.org/10.3390/dj11050139
Chicago/Turabian StyleZappi, Anastasia, Efstratios Papazoglou, and Maria Anagnostou. 2023. "Is a Wiggling-Motion Modified Two-Step Impression Technique as Accurate as Conventional Techniques in Restorative Dentistry?" Dentistry Journal 11, no. 5: 139. https://doi.org/10.3390/dj11050139
APA StyleZappi, A., Papazoglou, E., & Anagnostou, M. (2023). Is a Wiggling-Motion Modified Two-Step Impression Technique as Accurate as Conventional Techniques in Restorative Dentistry? Dentistry Journal, 11(5), 139. https://doi.org/10.3390/dj11050139