The Rigid-Shield Technique: A New Contour and Clot Stabilizing Method for Ridge Preservation



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Presentation
2.1. Clinical Presentation
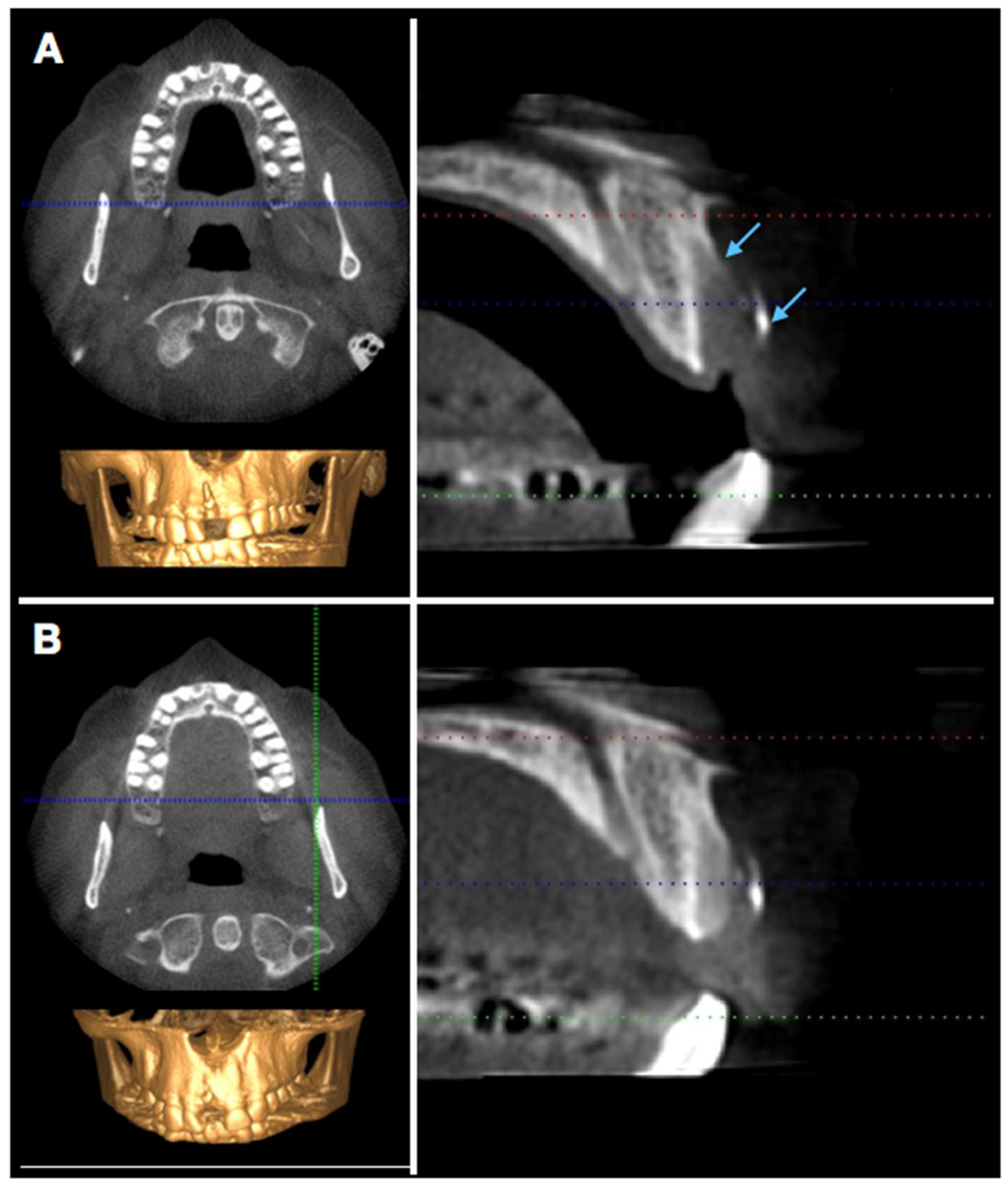
2.2. Radiographic Evaluation
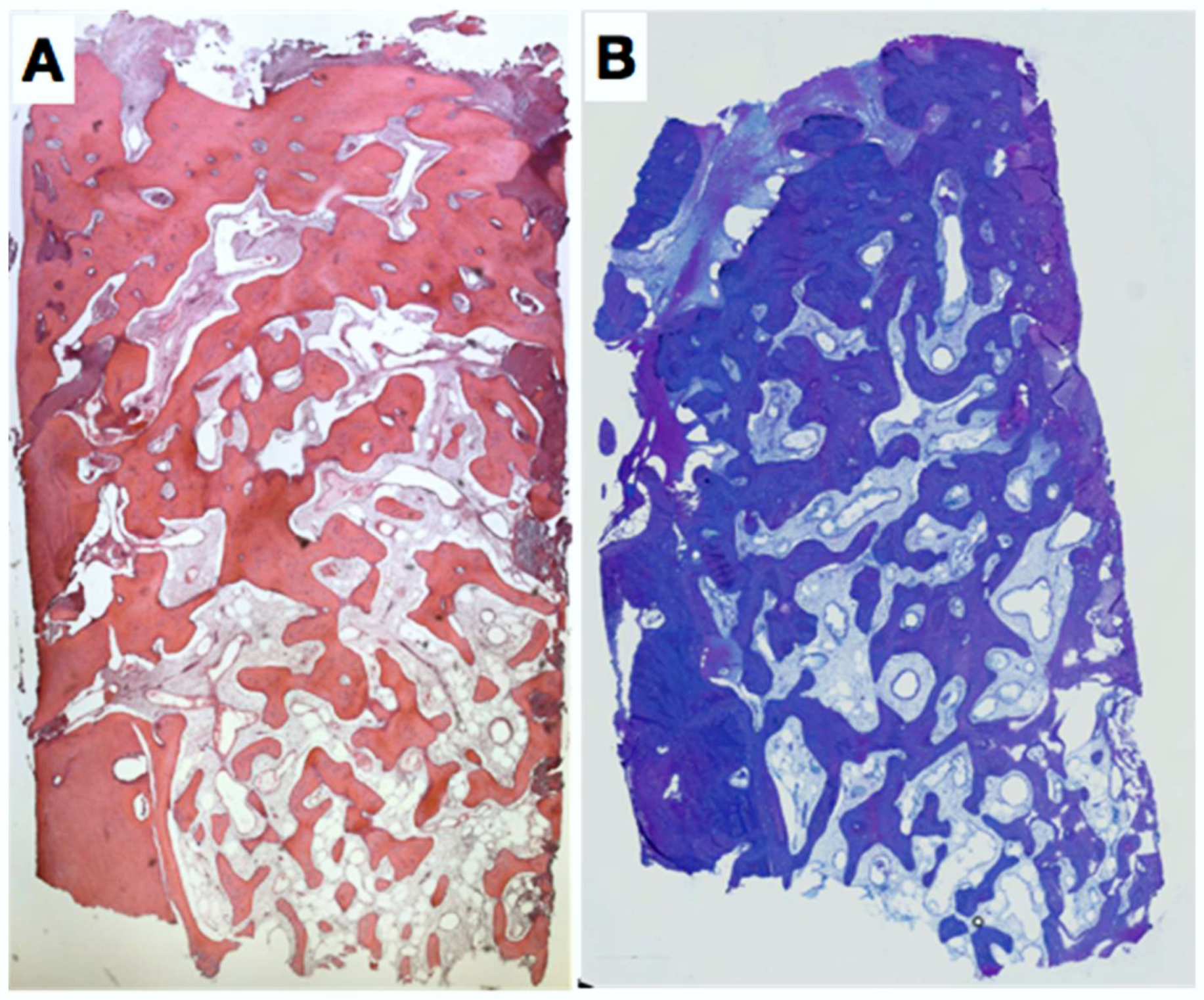
2.3. Histologic Evaluation
3. Discussion
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Schmidlin, P.R.; Jung, R.E.; Schug, J. Alveolarkammprävention nach Zahnextraktion-eine Literaturübersicht. Schweiz Monatsschr Zahnmed 2004, 114, 328–336. [Google Scholar] [PubMed]
- Tan, W.L.; Wong, T.L.T.; Wong, M.C.M.; Lang, N.P. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin. Oral. Implants Res. 2012, 23 (Suppl. 5), 1–21. [Google Scholar] [CrossRef] [PubMed]
- Chappuis, V.; Engel, O.; Reyes, M.; Shahim, K.; Nolte, L.P.; Buser, D. Ridge Alterations Post-extraction in the Esthetic site. J. Dent. Res. 2013, 92 (Suppl. 12), 195S–201S. [Google Scholar] [CrossRef] [PubMed]
- Lisowski, C.S. A comparative study of the resorption of alveolar ridge tissue under immediate dentures. Dent. Res. Grad. Study 1944, 45, 11–13. [Google Scholar] [PubMed]
- Von Wowern, N.; Winther, S. Submergence of roots for alveolar ridge preservation. A failure (4-year follow-up study. Int. J. Oral. Surg. 1981, 10, 247–250. [Google Scholar] [CrossRef]
- Block, M.S.; Kent, J.N. A comparison of particulate and solid root forms of hydroxylapatite in dog extraction sites. J. Oral. Maxillofac. Surg. 1986, 44, 89–93. [Google Scholar] [CrossRef]
- Masaki, C.; Nakamoto, T.; Mukaibo, T.; Kondo, Y.; Hosowaka, R. Strategies for alveolar ridge reconstruction and preservation for implant therapy. J. Prosthodont. Res. 2015, 15, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Araújo, M.G.; Lindhe, J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J. Clin. Periodontol. 2005, 32, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Botticelli, D.; Berglundh, T.; Lindhe, J. Hard-tissue alterations following immediate implant placement in extraction sites. J. Clin. Periodontol. 2004, 31, 820–828. [Google Scholar] [CrossRef] [PubMed]
- Fickl, S.; Zuhr, O.; Wachtel, H.; Bolz, W.; Huerzeler, M.B. Hard tissue alterations after socket preservation: An experimental study in the beagle dog. Clin. Oral Implants Res. 2008, 19, 1111–1118. [Google Scholar] [CrossRef] [PubMed]
- Chappuis, V.; Mauricio, G.; Araújo, M.G.; Buser, D. Clinical relevance of dimensional bone and soft tissue alterations post-extraction in esthetic sites. Periodontol 2000 2017, 73, 73–83. [Google Scholar] [CrossRef] [PubMed]
- Jung, R.E.; Ioannidis, A.; Hämmerle, C.H.F.; Thoma, D.S. Alveolar ridge preservation in the esthetic zone. Periodontol 2000 2018, 77, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Lindhe, J.; Cecchinato, D.; Donati, M.; Tomasi, C.; Liljenberg, B. Ridge preservation with the use of deproteinized bovine bone mineral. Clin. Oral Implants Res. 2014, 25, 786–790. [Google Scholar] [CrossRef] [PubMed]
- Hürzeler, M.B.; Zuhr, O.; Schupbach, P.; Rebele, S.F.; Emmanouilidis, N.; Fickl, S. The socket-shield technique: A proof-of-principle report. J. Clin. Periodontol. 2010, 37, 855–862. [Google Scholar] [CrossRef] [PubMed]
- Calvo-Guirado, J.L.; Troiano, M.; López-López, P.J.; Ramírez-Fernandez, M.P.; de Val, J.E.M.S.; Marin, J.M.G.; Gehrke, S.A. Different configuration of socket shield technique in peri-implant bone preservation: An experimental study in dog mandible. Ann. Anat. 2016, 208, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Glocker Attin, T.; Schmidlin, P.R. Ridge Preservation with Modified “Socket-Shield” Technique: A Methodological Case Series. Dent. J. 2014, 2, 11–21. [Google Scholar] [CrossRef] [Green Version]
- Mardas, N.; Trullenque-Eriksson, A.; MacBeth, N.; Petrie, A.; Donos, N. Does ridge preservation following tooth extraction improve implant treatment outcomes: A systematic review: Group 4: Therapeutic concepts & methods. Clin. Oral Implants Res. 2015, 26 (Suppl. 11), 180–201. [Google Scholar] [CrossRef] [PubMed]
- Macbeth, N.; Trullenque-Eriksson, A.; Donos, N.; Mardas, N. Hard and soft tissue changes following alveolar ridge preservation: A systematic review. Clin. Oral Implants Res. 2017, 28, 982–1004. [Google Scholar] [CrossRef] [PubMed]
- Jambhekar, S.; Kernen, F.; Bidra, A.S. Clinical and histologic outcomes of socket grafting after flapless tooth extraction: A systematic review of randomized controlled clinical trials. J. Prosthet. Dent. 2015, 113, 371–382. [Google Scholar] [CrossRef] [PubMed]
- Iglhaut, G.; Schwarz, F.; Gründel, M.; Mihatovic, I.; Becker, J.; Schliephake, H. Shell technique using a rigid resorbable barrier system for localized alveolar ridge augmentation. Clin. Oral Implants Res. 2014, 25, e149-54. [Google Scholar] [CrossRef] [PubMed]
- Volkel, W.; Pabst, W.; Klemm, E. The use of resorbable osteosynthesis materials. Laryngorhinootologie 2011, 90, 23–25. [Google Scholar] [PubMed]
- Holderegger, C.; Schmidlin, P.R.; Weber, F.E.; Mohn, D. Preclinical in vivo Performance of Novel Biodegradable, Electrospun Poly (lactic acid) and Poly (lactic-co-glycolic acid) Nanocomposites: A Review. Materials 2015, 8, 4912–4931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rothamel, D.; Schwarz, F.; Sager, M.; Herten, M.; Sculean, A.; Becker, J. Biodegradation of differently cross-linked collagen membranes: An experimental study in the rat. Clin. Oral Implants Res. 2005, 16, 369–378. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Rothamel, D.; Herten, M.; Sager, M.; Becker, J. Angiogenesis pattern of native and cross-linked collagen membranes: An immunohistochemical study in the rat. Clin. Oral Implants Res. 2006, 17, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Rosen, P.S.; Rosen, A.D. Purposeful exposure of a polylactic acid barrier to achieve socket preservation for placement of dental implants: Case series report. Compend. Cont. Educ. Dent. 2013, 34, 34–38. [Google Scholar]







© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mattiola, A.; Bosshardt, D.; Schmidlin, P.R. The Rigid-Shield Technique: A New Contour and Clot Stabilizing Method for Ridge Preservation. Dent. J. 2018, 6, 21. https://doi.org/10.3390/dj6020021
Mattiola A, Bosshardt D, Schmidlin PR. The Rigid-Shield Technique: A New Contour and Clot Stabilizing Method for Ridge Preservation. Dentistry Journal. 2018; 6(2):21. https://doi.org/10.3390/dj6020021
Chicago/Turabian StyleMattiola, Alessandro, Dieter Bosshardt, and Patrick R. Schmidlin. 2018. "The Rigid-Shield Technique: A New Contour and Clot Stabilizing Method for Ridge Preservation" Dentistry Journal 6, no. 2: 21. https://doi.org/10.3390/dj6020021
APA StyleMattiola, A., Bosshardt, D., & Schmidlin, P. R. (2018). The Rigid-Shield Technique: A New Contour and Clot Stabilizing Method for Ridge Preservation. Dentistry Journal, 6(2), 21. https://doi.org/10.3390/dj6020021