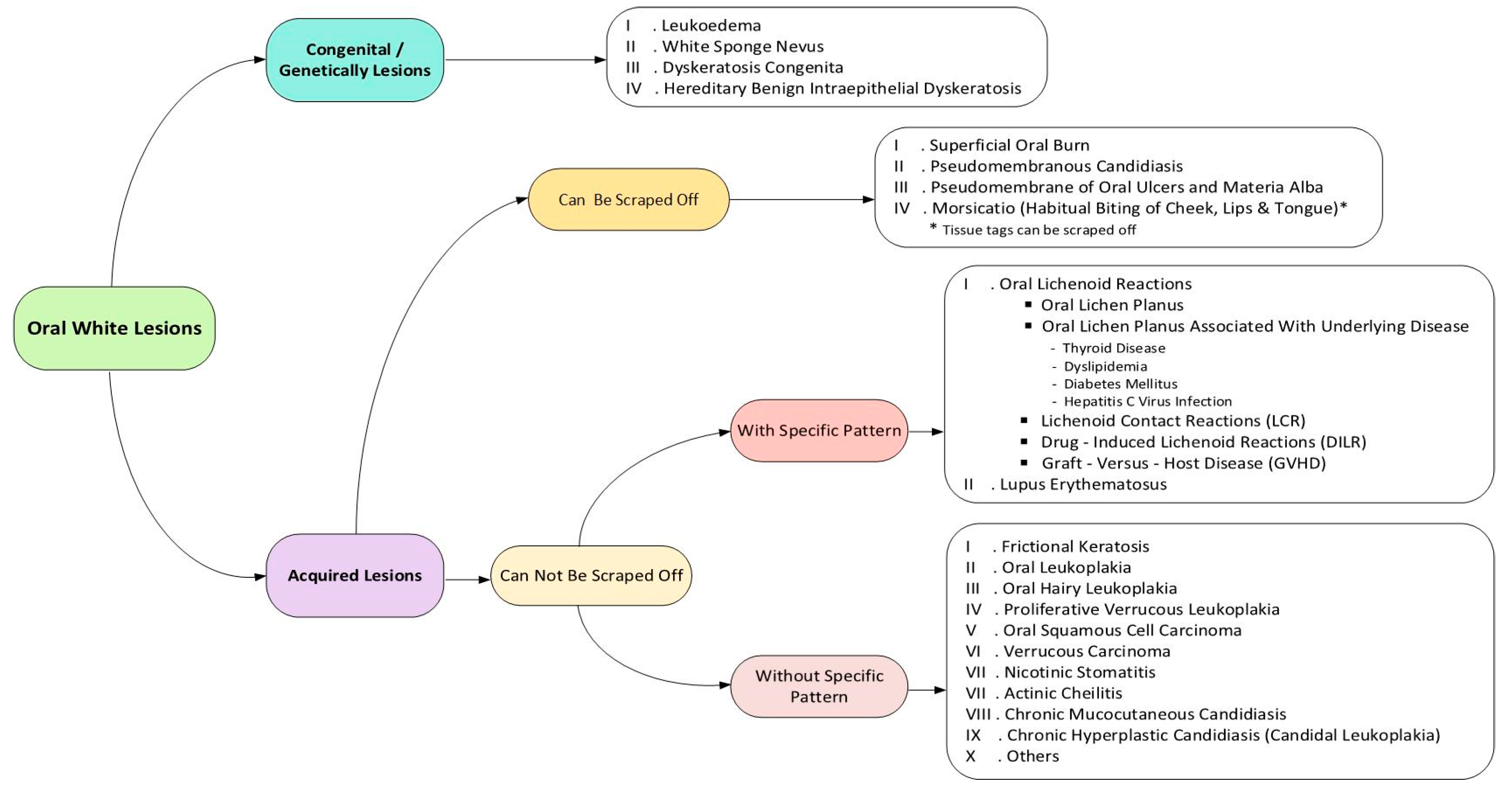
Oral White Lesions: An Updated Clinical Diagnostic Decision Tree

Abstract
:1. Introduction
2. Search Strategy
3. Congenital/Genetically Lesions
3.1. Leukoedema
3.2. White Sponge Nevus
3.3. Dyskeratosis Congenita
3.4. Hereditary Benign Intraepithelial Dyskeratosis
4. Acquired Lesions That Can Be Scraped Off
4.1. Superficial Oral Burn
4.2. Pseudomembranous Candidiasis
4.3. Pseudomembrane of Oral Ulcers and Materia Alba
4.4. Morsicatio
5. Acquired Lesions That Cannot Be Scraped Off (With Specific Pattern)
5.1. Lichenoid Reactions
5.2. Oral Lichen Planus
5.3. Oral Lichen Planus Associated with Underlying Diseases
5.4. Lichenoid Contact Reactions
5.5. Drug-Induced Lichenoid Reactions
5.6. Graft-Versus-Host Disease (GVHD)
5.7. Lupus Erythematosus
6. Acquired Lesions That Cannot Be Scraped Off (without Specific Pattern)
6.1. Frictional Keratosis
6.2. Oral Leukoplakia
6.3. Oral Hairy Leukoplakia
6.4. Proliferative Verrucous Leukoplakia
6.5. Oral Squamous Cell Carcinoma
6.6. Verrucous Carcinoma
6.7. Nicotinic Stomatitis
6.8. Actinic Cheilitis
6.9. Chronic Mucocutaneous Candidiasis
6.10. Chronic Hyperplastic Candidiasis (Candidal Leukoplakia)
7. Others
8. Discussions
9. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mortazavi, H.; Safi, Y.; Baharvand, M.; Rahmani, S. Diagnostic features of common oral ulcerative lesions: An updated decision tree. Int. J. Dent. 2016, 2016, 7278925. [Google Scholar] [CrossRef] [PubMed]
- Mortazavi, H.; Safi, Y.; Baharvand, M.; Rahmani, S.; Jafari, S. Peripheral Exophytic Oral Lesions: A Clinical Decision Tree. Int. J. Dent. 2017, 2017, 9193831. [Google Scholar] [CrossRef] [PubMed]
- Mohammad, A.; Bobby, J.; Devipriya, S. Prevalence of oral mucosal lesions in patients of the Kuwait University Dental Center. Saudi Dent. J. 2013, 25, 111–118. [Google Scholar]
- Glick, M. Burket’s Oral Medicine, 12th ed.; People’s Medical Publishing House: Shelton, CT, USA, 2015. [Google Scholar]
- Neville, B.; Damm, D.; Allen, C.; Chi, A. Oral and Maxillofacial Pathology, 4th ed.; Elsevier: Amsterdam, The Netherlands, 2016. [Google Scholar]
- Burket, L.; Greenberg, M.; Glick, M. Burket’s Oral Medicine Diagnosis and Treatment, 10th ed.; People’s Medical Publishing House: Hamilton, ON, Canada, 2003. [Google Scholar]
- Bhasin, M. Keratotic White Lesions of Oral Mucosa: An Oral Stomatologist Perspective. J. Periodontal. Med. Clin. Pract. 2016, 3, 33–40. [Google Scholar]
- Haseth, S.B.; Bakker, E.; Vermeer, M.H.; Idrissi, H.; Bosse, T.; Smit, V.T.; Terron-Kwiatkowski, A.; McLean, W.H.; Peters, A.A.; Hes, F.J. A novel keratin 13 variant in a four-generation family with white sponge nevus. Clin. Case Rep. 2017, 5, 1503–1509. [Google Scholar] [CrossRef] [PubMed]
- García, M.S.; Teruya-Feldstein, J. The diagnosis and treatment of dyskeratosiscongenita: A review. J. Blood Med. 2014, 5, 157. [Google Scholar]
- Babu, N.A.; Rajesh, E.; Krupaa, J.; Gnananandar, G. Genodermatoses. J. Pharm. Bioallied Sci. 2015, 7, S203–S206. [Google Scholar] [CrossRef] [PubMed]
- Bessler, M.; Wilson, D.B.; Mason, P.J. Dyskeratosiscongenita. FEBS Lett. 2010, 584, 3831–3838. [Google Scholar] [CrossRef] [PubMed]
- Bui, T.; Young, J.W.; Frausto, R.F.; Markello, T.C.; Glasgow, B.J.; Aldave, A.J. Hereditary benign intraepithelial dyskeratosis: Report of a case and re-examination of the evidence for locus heterogeneity. Ophthalmic Genet. 2016, 37, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Naganawa, T.; Murozumi, H.; Kumar, A.; Okuyama, A.; Okamoto, T.; Ando, T. Intraoral chemical burn in an elderly patient with dementia. Int. J. Burn. Trauma 2015, 5, 79. [Google Scholar]
- Anura, A. Traumatic oral mucosal lesions: A mini review and clinical update. Oral Health Dent. Manag. 2014, 13, 254–259. [Google Scholar] [PubMed]
- Kafas, P.; Stavrianos, C. Thermal burn of palate caused by microwave heated cheese-pie: A case report. Cases J. 2008, 1, 191. [Google Scholar] [CrossRef] [PubMed]
- Arun, S.; Renuka, V.; Aditi, M.; Ashutosh, A. Oral candidiasis: An overview. J. Oral Maxillofacpathol. 2014, 18, S81–S85. [Google Scholar]
- Scully, C.; Porter, S. ABC of oral health: Swellings and red, white, and pigmented lesions. Br. Med. J. 2000, 321, 225. [Google Scholar] [CrossRef]
- Wood, N.K.; Goaz, P.W. Differential Diagnosis of Oral Lesions; Mosby Elsevier Health Science: St. Louis, MO, USA, 1985. [Google Scholar]
- Scully, C. Oral and Maxillofacial Medicine-E-Book: The Basis of Diagnosis and Treatment, 3rd ed.; Elsevier Health Sciences: London, UK, 2013. [Google Scholar]
- Scully, C.; Felix, D.H. Oral Medicine—Update for the dental practitioner: Oral white patches. Br. Dent. J. 2005, 199, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.S.; Lee, H.E.; Ro, Y.S.; Lee, C.W. Three Cases of ‘MorsicatioLabiorum’. Ann. Dermatol. 2012, 24, 455–458. [Google Scholar] [CrossRef] [PubMed]
- Mortazavi, H.; Baharvand, M.; Mehdipour, M. Oral potentially malignant disorders: An overview of more than 20 entities. J. Dent. Res. Dent. Clin. Dent. Prospect. 2014, 8, 6–14. [Google Scholar]
- Bakhtiari, S.; Azari-Marhabi, S.; Mojahedi, S.M.; Namdari, M.; Elmi-Rankohi, Z.; Jafari, S. Comparing clinical effects of photodynamic therapy as a novel method with topical corticosteroid for treatment of Oral Lichen Planus. Photodiagnosis Photodyn. Ther. 2017, 20, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Shahidi, M.; Jafari, S.; Barati, M.; Mahdipour, M.; Gholami, M.S. Predictive value of salivary microRNA-320a, vascular endothelial growth factor receptor 2, CRP and IL-6 in Oral lichen planus progression. Inflammopharmacology 2017, 13, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Gheorghe, C.; Mihai, L.; Parlatescu, I.; Tovaru, S. Association of oral lichen planus with chronic C hepatitis. Review of the data in literature. Maedica 2014, 9, 98. [Google Scholar] [PubMed]
- Krishnamoorthy, B.; Suma, G.N.; Mamatha, N.S.; Sowbhagya, M.B.; Garlapati, K. Lipid Profile and Metabolic Syndrome Status in Patients with Oral Lichen Planus, Oral Lichenoid Reaction and Healthy Individuals Attending a Dental College in Northern India-A Descriptive Study. J. Clin. Diagn. Res. 2014, 8, ZC92. [Google Scholar] [CrossRef] [PubMed]
- López-Jornet, P.; Camacho-Alonso, F.; Rodríguez-Martínes, M.A. Alterations in serum lipid profile patterns in oral lichen planus: A cross-sectional study. Am. J. Clin. Dermatol. 2012, 13, 399–404. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Li, J.; Li, C.; Hua, H. The association of thyroid disease and oral lichen planus: A literature review and meta-analysis. Front. Endocrinol. 2017, 8, 310. [Google Scholar] [CrossRef] [PubMed]
- Mozaffari, H.R.; Sharifi, R.; Sadeghi, M. Prevalence of Oral Lichen Planus in Diabetes Mellitus: A Meta-Analysis Study. Acta Informatica Medica 2016, 24, 390. [Google Scholar] [CrossRef] [PubMed]
- Kamath, V.V.; Setlur, K.; Yerlagudda, K. Oral lichenoid lesions-A review and update. Indian J. Dermatol. 2015, 60, 102. [Google Scholar] [CrossRef] [PubMed]
- Treister, N.; Duncan, C.; Cutler, C.; Lehmann, L. How we treat oral chronic graft-versus-host disease. Blood 2012, 120, 3407–3418. [Google Scholar] [CrossRef] [PubMed]
- Rodsaward, P.; Prueksrisakul, T.; Deekajorndech, T.; Edwards, S.W.; Beresford, M.W.; Chiewchengchol, D. Oral Ulcers in Juvenile-Onset Systemic Lupus Erythematosus: A Review of the Literature. Am. J. Clin. Dermatol. 2017, 5, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Parlatescu, I.; Gheorghe, C.; Coculescu, E.; Tovaru, S. Oral Leukoplakia—An Update. Maedica 2014, 9, 88. [Google Scholar] [PubMed]
- Martorell-Calatayud, A.; Botella-Estrada, R.; Bagán-Sebastián, J.V.; Sanmartín-Jiménez, O.; Guillén-Barona, C. Oral leukoplakia: Clinical, histopathologic, and molecular features and therapeutic approach. Actasdermo-Sifiliográficas 2009, 100, 669–684. [Google Scholar] [CrossRef]
- Brasileiro, C.B.; Abreu, M.H.; Mesquita, R.A. Critical review of topical management of oral hairy leukoplakia. World J. Clin. Cases 2014, 2, 253. [Google Scholar] [CrossRef] [PubMed]
- Capella, D.L.; Gonçalves, J.M.; Abrantes, A.A.; Grando, L.J.; Daniel, F.I. Proliferative verrucous leukoplakia: Diagnosis, management and current advances. Braz. J. Otorhinolaryngol. 2017, 83, 585–593. [Google Scholar] [CrossRef] [PubMed]
- Munde, A.; Karle, R. Proliferative verrucous leukoplakia: An update. J. Cancer Res. Ther. 2016, 12, 469. [Google Scholar] [CrossRef] [PubMed]
- Alberto, C.A.; Alicia, D.F. Verrucous carcinoma of the oral mucosa: An epidemiological and follow-up study of patients treated with surgery in 5 last years. Med. Oral Patol. Oral Cir. Bucal. 2014, 19, e506–e511. [Google Scholar]
- Alper, A.; Emel, B.; Omer, G.; Bora, O. Oral Verrucous Carcinoma: A Study of 12 Cases. Eur. J. Dent. 2010, 4, 202–207. [Google Scholar]
- Zargaran, M.; Eshghyar, N.; Vaziri, P.B.; Mortazavi, H. Immunohistochemical evaluation of type IV collagen and laminin-332 γ2 chain expression in well-differentiated oral squamous cell carcinoma and oral verrucous carcinoma: A new recommended cut-off. J. Oral Pathol. Med. 2011, 40, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharyya, I.; Chehal, H.K. White lesions. Otolaryngol. Clin. North. Am. 2011, 44, 109–131. [Google Scholar] [CrossRef] [PubMed]
- Vieira, R.A.; Minicucci, E.M.; Marques, M.E.; Marques, S.A. Actinic cheilitis and squamous cell carcinoma of the lip: Clinical, histopathological and immunogenetic aspects. Anais Brasileiros de Dermatologia 2012, 87, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Okada, S.; Puel, A.; Casanova, J.L.; Kobayashi, M. Chronic mucocutaneous candidiasis disease associated with inborn errors of IL-17 immunity. Clin. Transl. Immunol. 2016, 5, e114. [Google Scholar] [CrossRef] [PubMed]
- ChambôFilho, A.; Souza-Filho, J.B.; Pignaton, C.C.; Zon, I.; Fernandes, A.S.; Cardoso, L.Q. Chronic mucocutaneous candidiasis: A case with exuberant cutaneous horns in nipples. Anais Brasileiros de Dermatologia 2014, 89, 641–644. [Google Scholar]
- Laura, C.C.; Yolanda, J.S. Clinical and microbiological diagnosis of oral candidiasis. J. Clin. Exp. Dent. 2013, 5, e279–e286. [Google Scholar]
- Sitheeque, M.A.; Samaranayake, L.P. Chronic hyperplastic candidosis/candidiasis [candidal leukoplakia]. Crit. Rev. Oral Biol. Med. 2003, 14, 253–267. [Google Scholar] [CrossRef] [PubMed]
- Scardina, G.A.; Ruggieri, A.; Messina, P. Chronic hyperplastic candidosis: A pilot study of the efficacy of 0.18% isotretinoin. J. Oral Sci. 2009, 51, 407–410. [Google Scholar] [CrossRef] [PubMed]
- Darling, M.R.; McCord, C.; Jackson-Boeters, L.; Copete, M. Markers of potential malignancy in chronic hyperplastic candidiasis. J. Investigclin Dent. 2012, 3, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Taheri, J.B.; Mortazavi, H.; Moshfeghi, M.; Bakhshi, M.; Bakhtiari, S.; Azari-Marhabi, S.; Alirezaei, S. Oro-facial manifestations of 100 leprosy patients. Med. Oralpatologia Oral Y Cirugiabucal 2012, 17, e728. [Google Scholar] [CrossRef]
- Jain, M. Leprosy in an Eight-Year-Old Child–An Exceptional Case with Unusual Oral Manifestation. J. Clin. Diagn. Res. 2017, 11, ZD19. [Google Scholar] [CrossRef] [PubMed]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Entity | Age | Gender | Common Location | Clinical Features | Treatment | Premalignant |
|---|---|---|---|---|---|---|
| Leukoedema | Not Assigned (NA) | M = F | buccal | mucosal folds, wrinkled white strerias | NA | NA |
| White sponge nevus | presents at birth | NA | buccal, ventral surface of the tongue, labial mucosa, soft palate, alveolar mucosa, floor of the mouth | symmetrical, thickened, white, corrugated or velvety, diffuse spongy plaques with an elevated, irregular and fissural surface | NA | NA |
| Dyskeratosis congenita | 5–12 years | NA | buccal, tongue, oropharynx | bullae formation, erosions, leukoplakic lesions, rapidly progressive periodontal disease, gingival inflammation and bleeding, gingival recession, bone loss, decreased root/crown ratio, mild taurodontism | bone marrow transplantation (BMT), androgens, oral and topical vitamin E | 30% malignant transformation in leukoplakia |
| Hereditary benign intra epithelial dyskeratosis | childhood | NA | buccal, labial | opalescent appearance mimicking leukoedema/thick, corrugated white plaques | NA | NA |
| Entity | Age | Gender | Common Location | Clinical Features | Treatment | Premalignant |
|---|---|---|---|---|---|---|
| Superficial burn | NA | NA | palatal, posterior buccal, anterior tongue | sloughy yellow-white necrotic epithelium with the areas of erythema and ulceration | NSAIDs, antiseptics, antibiotics, analgesics | NA |
| psuedomembranous candidiasis | infants/elderly | F > M | buccal, tongue, palate | creamy white plaques, patches, or papules | antifungals | NA |
| Pseudomembrane of oral ulcers and materia alba | NA | NA | NA | a white, dirty yellow-white or grayish-white color | removal of the debris, oral rinses | NA |
| Morsicatio | >35 years | F > M | buccal, lips, lateral border of the tongue | shaggy and thickened macerated gray-white patches or plaques with keratin shreds, tissue tags or desquamated areas | cessation the habitual chewing | NA |
| Entity | Age | Gender | Common Location | Clinical Features | Treatment | Premalignant |
|---|---|---|---|---|---|---|
| Lichen planus | middle age, mean age of 55 | F > M | posterior buccal mucosa bilaterally | papular, reticular, plaque-like, bullous, erythematous and ulcerative features; white components might be seen as papules, plaques, and reticular areas | topical steroid, concurrent use of antifungal drugs | potentially malignant disorder |
| LCR | NA | F | restricted to sites that are regularly in contact with dental materials such as buccal mucosa and lateral borders of the tongue | same reaction patterns as seen in OLP, that is, reticulum, papules, plaque, erythema, and ulcers | replacement of dental materials | NA |
| DILR | NA | NA | NA | unilateral with an ulcerative reaction pattern | withdrawal of the drug and use of topical steroids | NA |
| GVHD | NA | NA | tongue and buccal mucosa | hyperkeratotic reticulations and plaques, erythematous changes, and ulcerations | systemic corticosteroids and/or other immunomodulatory agents | NA |
| SLE | mean age: 31 | F | palate, buccal mucosa, and gingivae | ulcerations, erythematous lesions, hyperkeratosis, honeycomb plaque and discoid lesions as whitish steriae generally radiating from the central erythematous area (brush border) | NSAIDs along with antimalarial agents, systemic corticosteroids in combination with other immunosuppressives and immune modulating agents | NA |
| Entity | Age | Gender | Common Location(s) | Clinical Features | Treatment | Premalignant |
|---|---|---|---|---|---|---|
| Frictional keratosis | NA | NA | NA | white plaque with rough and frayed surface | removal of irritants | NA |
| Oral leukoplakia | >50 years | M | buccal mucosa, lip vermilion and gingivae | white patch or plaque | NA | potentially malignant lesion |
| OHL | NA | M | borders of the tongue unilaterally or bilaterally | from slight, white vertical bands to thickened, furrowed areas with a shaggy surface | systemic anti-herpes virus drugs, topical retinoids or podophyllum resin, combination therapy with acyclovir cream and podophyllumresin, gentian violet, surgical excision or cryotherapy | no potential for malignant transformation |
| PVL | mean age: 60 years | F | gingivae | non-homogeneous multifocal areas with speckled and rough surface in the form of exophytic, wart-like, verrucous, polypoid projections or erythematous components | surgery, carbon dioxide laser ablation, topical photodynamic therapy, oral retinoids, topical bleomycin solution, beta-carotene, methisoprinol (a synthetic antiviral agent), radiation, chemotherapy | malignant transformation |
| OSCC | >65 years | M | floor of the mouth, posterior lateral borders and ventral surface of the tongue | red, white, or combined red-and-white lesion; alteration of surface texture into granular, rough, fungating, papillary, and verruciform or crusted lesion; or existence of a mass or irregular ulceration with rolled border and induration on palpation. | radiation therapy or combined chemo radiation therapy with or without surgery | NA |
| Verrucous carcinoma | elderly | M | mandibular vestibule, buccal mucosa, gingivae, tongue, and hard palate | asymptomatic, diffuse, well demarcated, thick white plaque with papillary or verruciform projections | NA | NA |
| Nicotinic stomatitis | >45 | M | palate | diffuse leathery grayish-white palatal plaque with red points, “dried mud” appearance | regression after cessation of smoking | not a premalignant condition |
| Actinic cheilitis | old age | M | lower lip vermilion | dryness, swelling, cracks, atrophic regions, crusting regions, keratotic plaques, chronic ulceration | Surgery, cryotherapy, electrosurgery, topical retinoids, 5-flurouracil cream, photodynamic therapy, CO2 laser ablation and vermilionectomy | Premalignant condition |
| Chronic mucocutaneous candidiasis | begins during infancy | NA | nails, skin, oral and genital mucosae | chronic whitish plaques, along with crusts and ulcers | antifungal therapy | NA |
| chronic hyperplastic candidiasis (Candidal leukoplakia) | over 50 | NA | retro commisures bilaterally, tongue, palate and lips | white patches or plaques | antifungal therapy, topical retinoids, betacarotene, bleomyin, several surgical techniques | NA |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mortazavi, H.; Safi, Y.; Baharvand, M.; Jafari, S.; Anbari, F.; Rahmani, S. Oral White Lesions: An Updated Clinical Diagnostic Decision Tree. Dent. J. 2019, 7, 15. https://doi.org/10.3390/dj7010015
Mortazavi H, Safi Y, Baharvand M, Jafari S, Anbari F, Rahmani S. Oral White Lesions: An Updated Clinical Diagnostic Decision Tree. Dentistry Journal. 2019; 7(1):15. https://doi.org/10.3390/dj7010015
Chicago/Turabian StyleMortazavi, Hamed, Yaser Safi, Maryam Baharvand, Soudeh Jafari, Fahimeh Anbari, and Somayeh Rahmani. 2019. "Oral White Lesions: An Updated Clinical Diagnostic Decision Tree" Dentistry Journal 7, no. 1: 15. https://doi.org/10.3390/dj7010015
APA StyleMortazavi, H., Safi, Y., Baharvand, M., Jafari, S., Anbari, F., & Rahmani, S. (2019). Oral White Lesions: An Updated Clinical Diagnostic Decision Tree. Dentistry Journal, 7(1), 15. https://doi.org/10.3390/dj7010015