Socioeconomic Inequalities in Oral Health-Related Quality of Life among Brazilians: A Cross-Sectional Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Outcome Measure
2.2. Socioeconomic Position Indicator and Other Covariates
2.3. Data Analysis
2.4. Ethical Considerations
3. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Elani, H.; Harper, S.; Allison, P.; Bedos, C.; Kaufman, J. Socio-economic inequalities and oral health in Canada and the United States. J. Dent. Res. 2012, 91, 865–870. [Google Scholar] [CrossRef]
- Petersen, P.E.; Bourgeois, D.; Ogawa, H.; Estupinan-Day, S.; Ndiaye, C. The global burden of oral diseases and risks to oral health. Bul. World Health Organ. 2005, 83, 661–669. [Google Scholar]
- Institute for Health Metrics Evaluation. The Global Burden of Disease: Generating Evidence, Guiding Policy; IHME: Seattle, WA, USA, 2013. [Google Scholar]
- Petersen, P.E.; Kwan, S. Equity, social determinants and public health programmes—The case of oral health. Community Dent. Oral Epidemiol. 2011, 39, 481–487. [Google Scholar] [CrossRef]
- Bernabé, E.; Sheiham, A. Tooth loss in the United Kingdom–trends in social inequalities: An age-period-and-cohort analysis. PLoS ONE 2014, 9, e104808. [Google Scholar] [CrossRef] [PubMed]
- Guarnizo-Herreño, C.C.; Tsakos, G.; Sheiham, A.; Marmot, M.G.; Kawachi, I.; Watt, R.G. Austin Powers bites back: A cross sectional comparison of US and English national oral health surveys. BMJ Br. Med. J. 2015, 351, h6543. [Google Scholar] [CrossRef] [PubMed]
- Tsakos, G.; Sheiham, A.; Iliffe, S.; Kharicha, K.; Harari, D.; Swift, C.G.; Stuck, A.E. The impact of educational level on oral health-related quality of life in older people in London. Eur. J. Oral Sci. 2009, 117, 286–292. [Google Scholar] [CrossRef]
- Prado, R.L.; Saliba, N.A.; Garbin, C.A.; Moimaz, S.A. Oral impacts on the daily performance of Brazilians assessed using a sociodental approach: Analyses of national data. Braz. Oral Res. 2015, 29, 1806–8324. [Google Scholar] [CrossRef] [PubMed]
- Slade, G.D.; Sanders, A.E. The paradox of better subjective oral health in older age. J. Dent. Res. 2011, 90, 1279–1285. [Google Scholar] [CrossRef]
- Souza, J.G.; Costa Oliveira, B.E.; Martins, A.M. Contextual and individual determinants of oral health-related quality of life in older Brazilians. Qual. Life Res. 2017, 26, 1295–1302. [Google Scholar] [CrossRef] [PubMed]
- Pereira, K.C.R.; Lacerda, J.; Traebert, J. The oral impact on daily performances and self-reported quality of life in elderly people in Florianópolis, Brazil. Oral Health Prev. Dent. 2009, 7, 163–172. [Google Scholar]
- Secretaria de Estado de Saúde de Minas Gerais. SB Minas Gerais. In Pesquisa das Condições de Saúde Bucal da População Mineira-Resultados Principais; Secretaria de Estado de Saúde de Minas Gerais: Belo Horizonte, Brazil, 2013. Available online: http://www.saude.mg.gov.br/images/documentos/SBMinas_Relatorio_Final.pdf (accessed on 1 November 2018).
- World Health Organization. Oral Health Assessment form, Oral Health Surveys, Basic Methods, 4th ed.; WHO: Geneva, Switzerland, 1997; pp. 26–29. [Google Scholar]
- Adulyanon, S.; Sheiham, A.; Slade, G. Oral impacts on daily performances. In Measuring Oral Health and Quality of Life; Slade, G.D., Ed.; Department of Dental Ecology, School of Dentistry, University of North Carolina: Chapel Hill, NC, USA, 1997; pp. 151–160. [Google Scholar]
- World Health Organization. Oral Health Surveys: Basic Methods; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Wagstaff, A.; Paci, P.; Van Doorslaer, E. On the measurement of inequalities in health. Soc. Sci. Med. 1991, 33, 545–557. [Google Scholar] [CrossRef] [Green Version]
- Mackenbach, J.P.; Stirbu, I.; Roskam, A.-J.R.; Schaap, M.M.; Menvielle, G.; Leinsalu, M.; Kunst, A.E. Socioeconomic Inequalities in Health in 22 European Countries. N. Engl. J. Med. 2008, 358, 2468–2481. [Google Scholar] [CrossRef] [Green Version]
- Ministério da Saúde, Secretaria de Atenção à Saúde, Secretaria de Vigilância em Saúde. Projeto SB Brasil 2010: Pesquisa Nacional de Saúde Bucal: Resultados Principais; Ministério da Saúde: Brasília, Brazil, 2011.
- Åstrøm, A.; Haugejorden, O.; Skaret, E.; Trovik, T.; Klock, K. Oral Impacts on Daily Performance in Norwegian adults: The influence of age, number of missing teeth, and socio-demographic factors. Eur. J. Oral Sci. 2006, 114, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Maida, C.A.; Marcus, M.; Spolsky, V.W.; Wang, Y.; Liu, H. Socio-behavioral predictors of self-reported oral health-related quality of life. Qual. Life Res. 2013, 22, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Steele, J.G.; Sanders, A.E.; Slade, G.D.; Allen, P.F.; Lahti, S.; Nuttall, N.; Spencer, A.J. How do age and tooth loss affect oral health impacts and quality of life? A study comparing two national samples. Community Dent. Oral Epidemiol. 2004, 32, 107–114. [Google Scholar] [CrossRef]
- Carr, A.J.; Gibson, B.; Robinson, P.G. Is quality of life determined by expectations or experience? BMJ Br. Med. J. 2001, 322, 1240–1243. [Google Scholar] [CrossRef]
- Tsakos, G.; Demakakos, P.; Breeze, E.; Watt, R.G. Social gradients in oral health in older adults: Findings from the English longitudinal survey of aging. Am. J. Public Health 2011, 101, 1892–1899. [Google Scholar] [CrossRef]
- Fuentes-García, A.; Lera, L.; Sanchez, H.; Albala, C. Oral health-related quality of life of older people from three South American cities. Gerodontology 2013, 30, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Gülcan, F.; Ekbäck, G.; Ordell, S.; Lie, S.A.; Åstrøm, A.N. Inequality in oral health related to early and later life social conditions: A study of elderly in Norway and Sweden. BMC Oral Health 2015, 15, 20. [Google Scholar] [CrossRef] [PubMed]
- Andrade, F.B.; Lebrao, M.L.; Santos, J.L.F.; da Cruz Teixeira, D.S.; Oliveira Duarte, Y.A. Relationship between oral health–related quality of life, oral health, socioeconomic, and general health factors in elderly Brazilians. J. Am. Geriatr. Soc. 2012, 60, 1755–1760. [Google Scholar] [CrossRef] [PubMed]
- Allin, S.; Masseria, C.; Mossialos, E. Measuring socioeconomic differences in use of health care services by wealth versus by income. Am. J. Public Health 2009, 99, 1849–1855. [Google Scholar] [CrossRef] [PubMed]
- Avlund, K.; Holstein, B.E.; Osler, M.; Damsgaard, M.T.; Holm-Pedersen, P.; Rasmussen, N.K. Social position and health in old age: The relevance of different indicators of social position. Scand. J. Public Health 2003, 31, 126–136. [Google Scholar] [CrossRef]
- Grundy, E.; Holt, G. The socioeconomic status of older adults: How should we measure it in studies of health inequalities? J. Epidemiol. Community Health 2001, 55, 895–904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steele, J.; Shen, J.; Tsakos, G.; Fuller, E.; Morris, S.; Watt, R.; Wildman, J. The interplay between socioeconomic inequalities and clinical oral health. J. Dent. Res. 2015, 94, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Guarnizo-Herreño, C.C.; Watt, R.G.; Fuller, E.; Steele, J.G.; Shen, J.; Morris, S.; Tsakos, G. Socioeconomic position and subjective oral health: Findings for the adult population in England, Wales and Northern Ireland. BMC Public Health 2014, 14, 827. [Google Scholar] [CrossRef] [PubMed]
- Tsakos, G. Inequalities in Oral Health of the Elderly Rising to the Public Health Challenge? J. Dent. Res. 2011, 90, 689–690. [Google Scholar] [CrossRef]
- Jagger, D.C.; Sherriff, A.; Macpherson, L.M. Measuring socio-economic inequalities in edentate Scottish adults–cross-sectional analyses using Scottish Health Surveys 1995–2008/09. Community Dent. Oral Epidemiol. 2013, 41, 499–508. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Age Groups | |||
|---|---|---|---|
| Total (n = 2288) | 35–44 years (n = 1159) | 65–74 years (n = 1129) | |
| Sex | |||
| Male | 36.2 | 34.6 | 38.5 |
| Female | 63.8 | 65.4 | 61.5 |
| Schooling (in years) | |||
| 0–3 | 19.3 | 6.0 | 47.6 |
| 4–7 | 30.7 | 30.0 | 32.0 |
| 8–11 | 26.6 | 33.7 | 11.4 |
| 12+ | 23.5 | 30.2 | 9.1 |
| Family income (in reais) | |||
| ≤500 | 5.8 | 6.3 | 4.5 |
| 501–1500 | 52.5 | 48.4 | 61.3 |
| 1501–2500 | 25.5 | 27.6 | 20.9 |
| 2501–4500 | 11.8 | 12.9 | 9.4 |
| 4501+ | 4.4 | 4.7 | 4.0 |
| Negative Impact | |||
|---|---|---|---|
| Total | 35–44 years | 65–74 years | |
| (%) | (%) | (%) | |
| Sex | |||
| Male | 40.1 (34.6, 45.9) | 41.8 (34.7, 49.3) | 37.0 (30.3, 44.2) |
| Female | 43.8 (39.0, 48.8) | 46.5 (40.8, 52.4) | 37.7 (31.5, 44.4) |
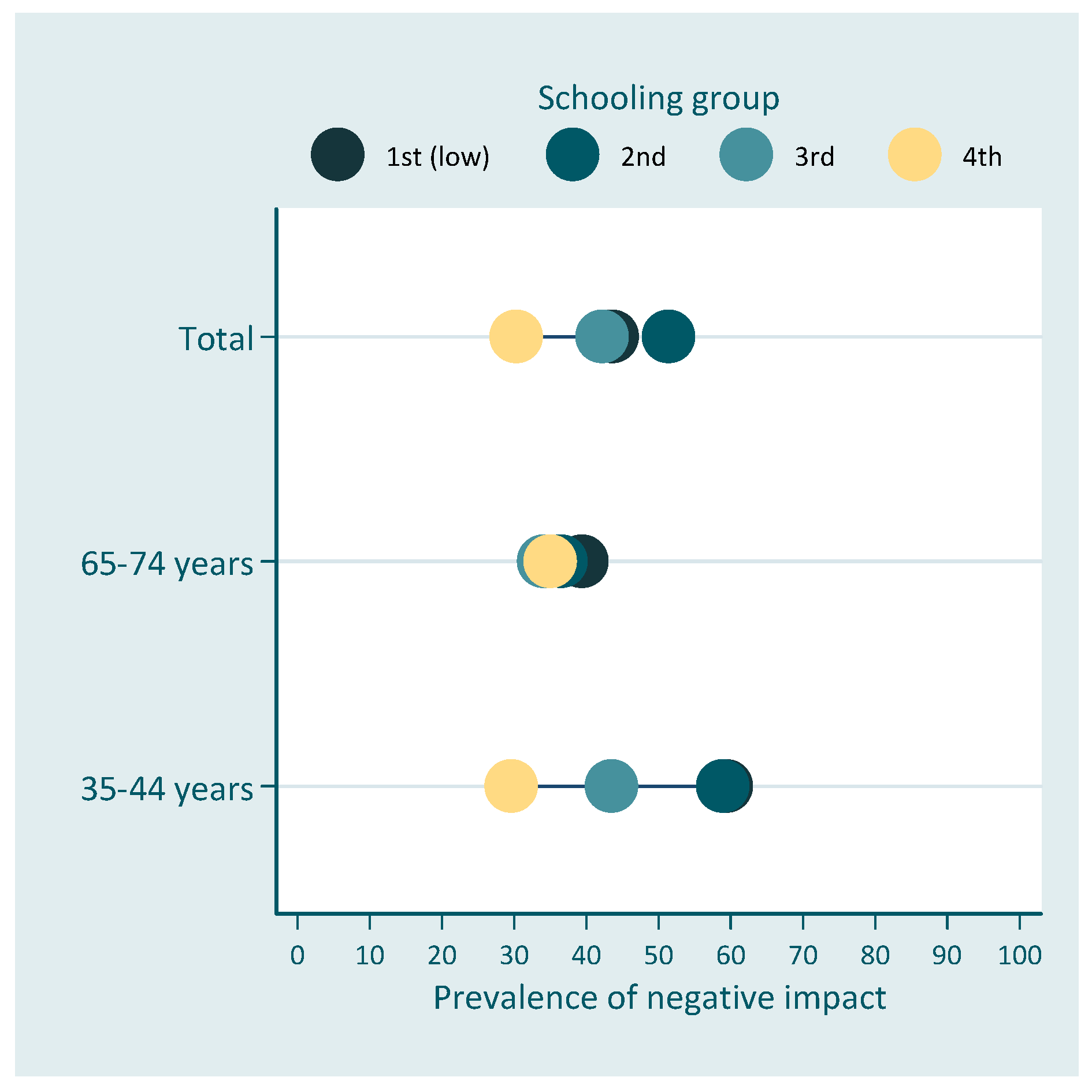
| Schooling | |||
| 0–3 years | 43.6 (37.6, 49.8) * | 59.4 (44.6, 72.7) * | 39.4 (33.2, 45.9) |
| 4–7 years | 51.4 (45.0, 57.8) | 58.9 (50.5, 66.8) | 36.5 (30.0, 43.4) |
| 8–11 years | 42.2 (36.5, 48.2) | 43.5 (37.3, 50.0) | 34.1 (21.3, 49.8) |
| 12+ years | 30.3 (24.5, 36.8) | 29.6 (23.4, 36.7) | 35.0 (23.8, 48.2) |
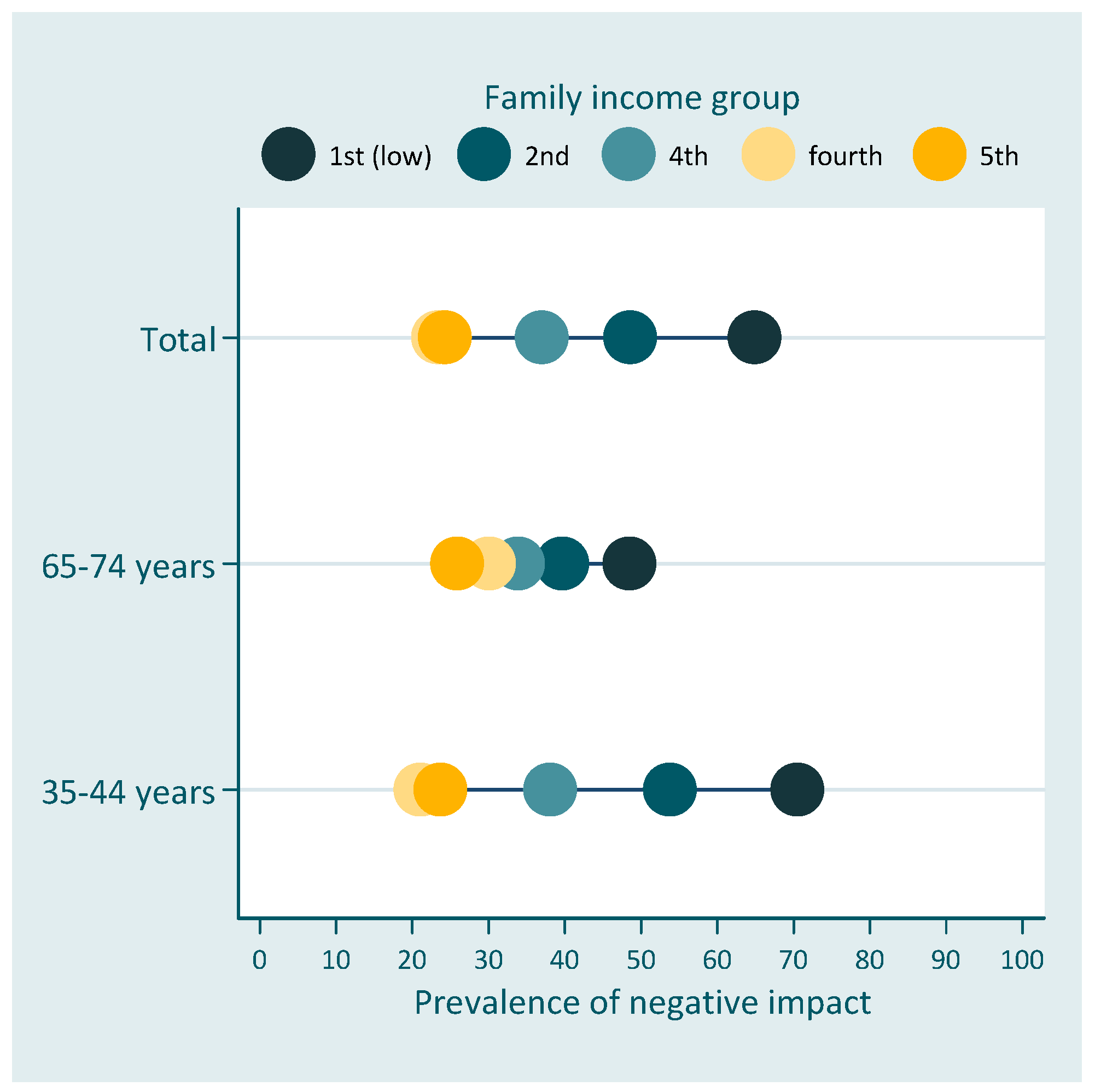
| Family income | |||
| ≤500 reais | 64.9 (55.0, 73.7) * | 70.5 (58.3, 80.3) * | 48.5 (31.4, 65.9) |
| 501–1500 reais | 48.6 (43.7, 53.5) | 53.8 (47.2, 60.4) | 39.7 (34.2, 45.5) |
| 1501–2500 reais | 37.0 (30.5, 44.0) | 38.1 (30.6, 46.2) | 33.9 (25.3, 43.6) |
| 2501–4500 reais | 23.4 (16.9, 31.5) | 21.1 (13.9, 30.7) | 30.1 (9.4, 43.6) |
| 4501+ reais | 24.3 (13.9, 39.0) | 23.7 (10.3, 45.8) | 25.9 (11.5, 48.3) |
| SII (95% CI) | RII (95% CI) | |
|---|---|---|
| Schooling | ||
| Total | −7.6 (−20.7; 5.6) | 0.84 (0.61; 1.14) |
| 35–44 years | −13.9 (−28.6; 0.7) | 0.73 (0.53; 1.02) |
| 65–74 years | 3.0 (−13.4; 19.5) | 1.14 (0.73; 1.77) |
| Family income | ||
| Total | −27.8 (−39.2; −0.165) ** | 0.52 (0.39; 0.69) ** |
| 35–44 years | −32.4 (−47.4; −0.174) ** | 0.49 (0.34; 0.69) ** |
| 65–74 years | −18.3 (−34.5; −0.022) * | 0.63 (0.40; 0.99) * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bof de Andrade, F.; Drumond Andrade, F.C. Socioeconomic Inequalities in Oral Health-Related Quality of Life among Brazilians: A Cross-Sectional Study. Dent. J. 2019, 7, 39. https://doi.org/10.3390/dj7020039
Bof de Andrade F, Drumond Andrade FC. Socioeconomic Inequalities in Oral Health-Related Quality of Life among Brazilians: A Cross-Sectional Study. Dentistry Journal. 2019; 7(2):39. https://doi.org/10.3390/dj7020039
Chicago/Turabian StyleBof de Andrade, Fabíola, and Flavia Cristina Drumond Andrade. 2019. "Socioeconomic Inequalities in Oral Health-Related Quality of Life among Brazilians: A Cross-Sectional Study" Dentistry Journal 7, no. 2: 39. https://doi.org/10.3390/dj7020039
APA StyleBof de Andrade, F., & Drumond Andrade, F. C. (2019). Socioeconomic Inequalities in Oral Health-Related Quality of Life among Brazilians: A Cross-Sectional Study. Dentistry Journal, 7(2), 39. https://doi.org/10.3390/dj7020039