
Dietary Supplements Use among Athletes in Lebanon: Knowledge, Attitudes, Practices, and Correlates

 , , ,
, , ,
Abstract
:1. Introduction
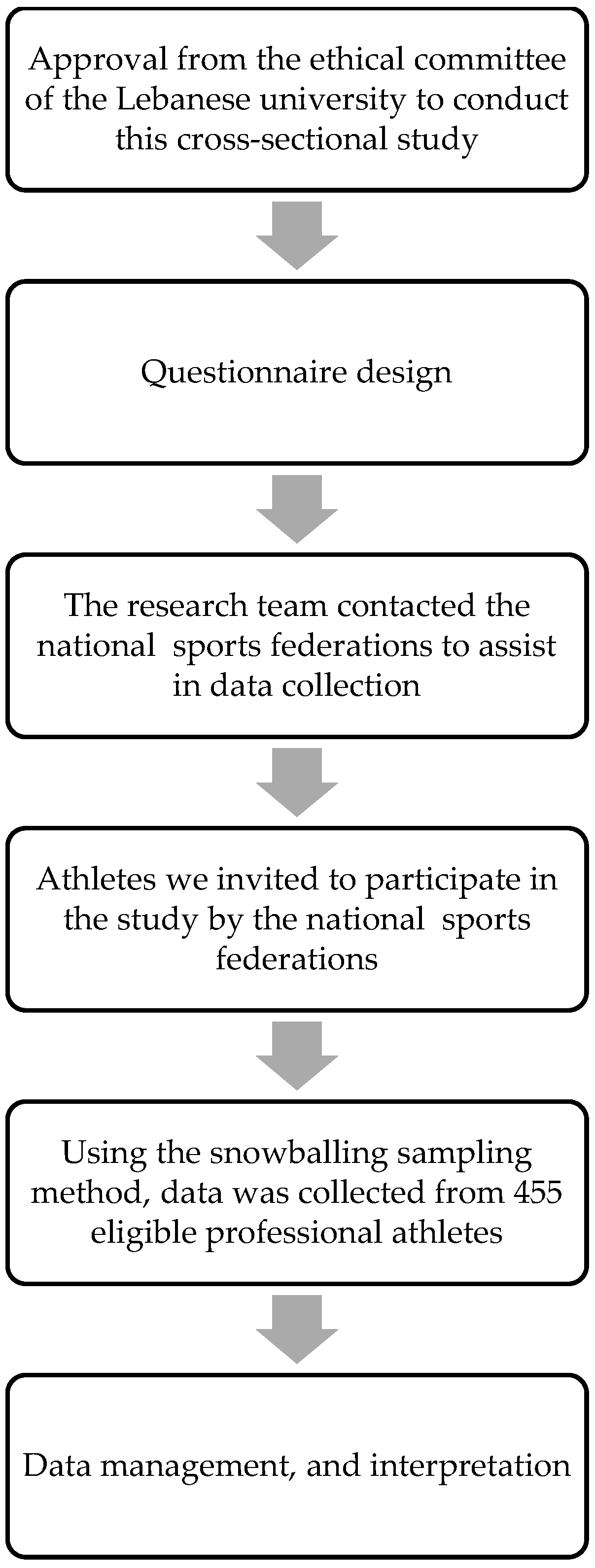
2. Materials and Methods
2.1. Study Design and Sampling Procedure
2.2. Participants
2.3. Study Instrument
2.4. Data Analysis
2.5. Ethical Considerations
3. Results
3.1. The Socio-Demographic and Personal Information of the Athletes
3.2. Sources of Information on Dietary Supplementation
3.3. DS-Related Knowledge of Athletes
3.4. DSs-Related Attitudes of Athletes
3.5. Prevalence of the DS Use and Supplementation Practices of Athletes
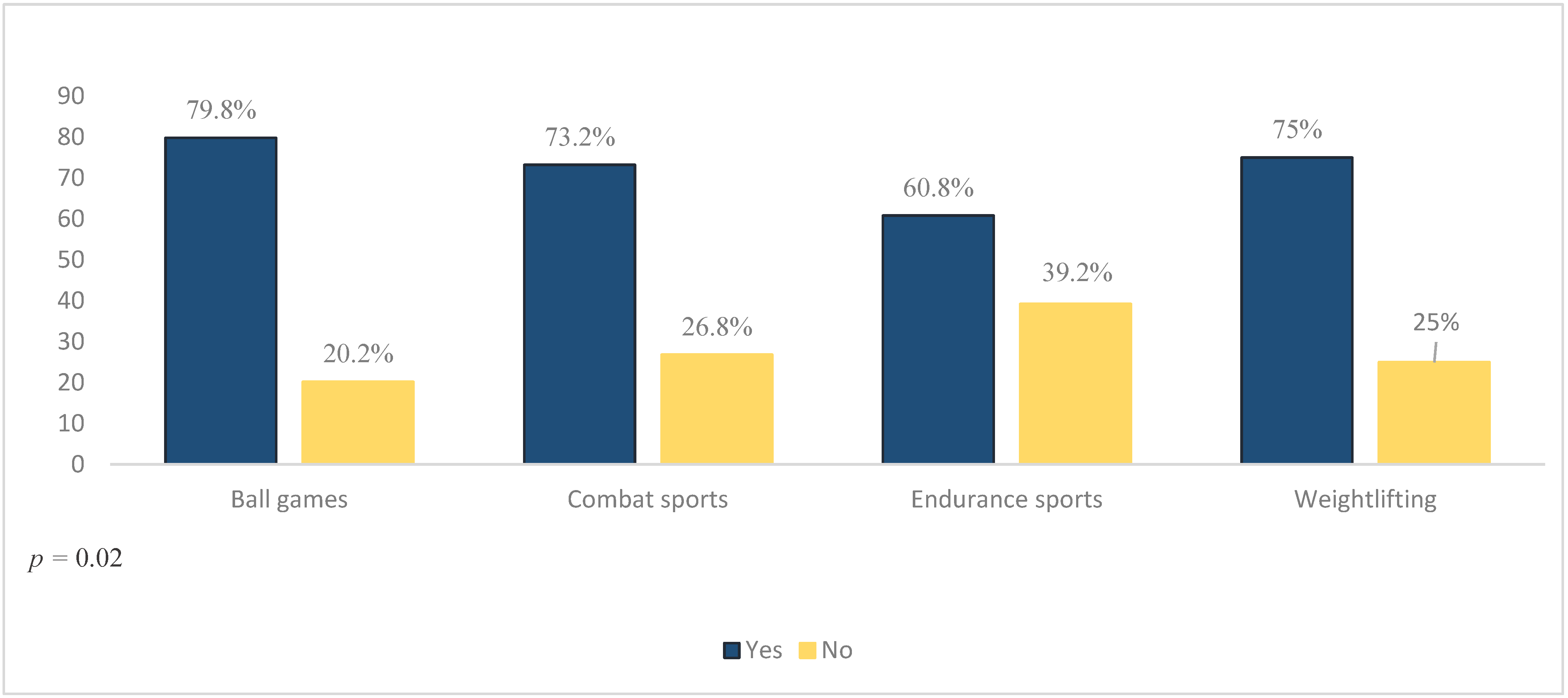
3.6. The Use of DSs According to Athletes’ Characteristics (Bivariate Analysis)
3.7. Determinants of DSs Use among Athletes (Logistic Regression Analysis)
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thomas, D.T.; Erdman, K.A.; Burke, L.M. Position of the Academy of Nutrition and Dietetics, Dietitians of Canada, and the American College of Sports Medicine: Nutrition and Athletic Performance. J. Acad. Nutr. Diet. 2016, 116, 501–528. [Google Scholar] [CrossRef] [PubMed]
- Hurst, P.; Kavussanu, M.; Boardley, I.; Ring, C. Sport supplement use predicts doping attitudes and likelihood via sport supplement beliefs. J. Sports Sci. 2019, 37, 1734–1740. [Google Scholar] [CrossRef] [PubMed]
- Parnell, J.A.; Wiens, K.; Erdman, K.A. Evaluation of congruence among dietary supplement use and motivation for supplementation in Young, Canadian athletes. J. Int. Soc. Sports Nutr. 2015, 12, 49. [Google Scholar] [CrossRef] [Green Version]
- Jonnalagadda, S.S.; Ziegler, P.J.; Nelson, J.A. Food preferences, dieting behaviors, and body image perceptions of elite figure skaters. Int. J. Sport Nutr. Exerc. Metab. 2004, 14, 594–606. [Google Scholar] [CrossRef]
- Shephard, R.J. American College of Sports Medicine Position Stand: Exercise and Fluid Replacement. Yearb. Sports Med. 2007, 2007, 254–255. [Google Scholar] [CrossRef]
- Maughan, R.J.; King, D.S.; Lea, T. Dietary supplements. J. Sports Sci. 2004, 22, 95–113. [Google Scholar] [CrossRef]
- Eichner, A.; Tygart, T. Adulterated dietary supplements threaten the health and sporting career of up-and-Coming Young Athletes. Drug Test. Anal. 2015, 8, 304–306. [Google Scholar] [CrossRef] [Green Version]
- Baylis, A.; Cameron-Smith, D.; Burke, L.M. Inadvertent doping through supplement use by athletes: Assessment and management of the risk in Australia. Int. J. Sport Nutr. Exerc. Metab. 2001, 11, 365–383. [Google Scholar] [CrossRef]
- Geyer, H.; Parr, M.K.; Koehler, K.; Mareck, U.; Schänzer, W.; Thevis, M. Nutritional supplements cross-contaminated and faked with doping substances. J. Mass Spectrom. 2008, 43, 892–902. [Google Scholar] [CrossRef]
- Abel, T.; Knechtle, B.; Perret, C.; Eser, P.; von Arx, P.; Knecht, H. Influence of chronic supplementation of arginine aspartate in endurance athletes on performance and substrate metabolism. Int. J. Sports Med. 2005, 26, 344–349. [Google Scholar] [CrossRef]
- Jeukendrup, A.E.; Randell, R. Fat burners: Nutrition supplements that increase Fat metabolism. Obes. Rev. 2011, 12, 841–851. [Google Scholar] [CrossRef] [PubMed]
- Muwonge, H.; Zavuga, R.; Kabenge, P.A.; Makubuya, T. Nutritional supplement practices of professional Ugandan athletes: A cross-sectional study. J. Int. Soc. Sports Nutr. 2017, 14, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daher, J.; El Khoury, D.; Dwyer, J.J. Education interventions to improve knowledge, beliefs, intentions and practices with respect to dietary supplements and doping substances: A narrative review. Nutrients 2021, 13, 3935. [Google Scholar] [CrossRef] [PubMed]
- Deldicque, L.; Francaux, M. Potential harmful effects of dietary supplements in sports medicine. Curr. Opin. Clin. Nutr. Metab. Care 2016, 19, 439–445. [Google Scholar] [CrossRef]
- Maughan, R.J. Contamination of dietary supplements and positive drug tests in sport. J. Sports Sci. 2005, 23, 883–889. [Google Scholar] [CrossRef]
- Maughan, R.J.; Greenhaff, P.L.; Hespel, P. Dietary supplements for athletes: Emerging trends and recurring themes. J. Sports Sci. 2011, 29, 65–74. [Google Scholar] [CrossRef]
- Johnston, D.I.; Chang, A.; Viray, M.; Chatham-Stephens, K.; He, H.; Taylor, E.; Wong, L.L.; Schier, J.; Martin, C.; Fabricant, D.; et al. Hepatotoxicity associated with the dietary supplement oxyelite pro™—Hawaii 2013. Drug Test. Anal. 2015, 8, 319–327. [Google Scholar] [CrossRef] [Green Version]
- Bakhtiar, M.; Rahman, M.; Kamruzzaman, M.; Sultana, N.; Rahaman, K.S.; Rahman, S.S. Determinants of nutrition knowledge, attitude and practices of Adolescent Sports Trainee: A cross-sectional study in Bangladesh. Heliyon 2021, 7, e06637. [Google Scholar] [CrossRef]
- Kish, L. Survey Sampling; American Political Science Review; John Wiley & Sons, Inc.: New York, NY, USA, 1965; Volume 59, p. 1025. [Google Scholar] [CrossRef]
- Tafeit, E.; Cvirn, G.; Lamprecht, M.; Hohensinn, M.; Moeller, R.; Hamlin, M.; Horejsi, R. Using body mass index ignores the intensive training of elite Special Force personnel. Exp. Biol. Med. 2019, 244, 873–879. [Google Scholar] [CrossRef]
- Shah, N.; Braverman, E. Measuring adiposity in patients: The utility of body mass index (BMI), percent body fat, and leptin. PLoS ONE 2012, 7, e33308. [Google Scholar] [CrossRef] [Green Version]
- Aljaloud, S.O.; Ibrahim, S.A. Use of dietary supplements among professional athletes in Saudi Arabia. J. Nutr. Metab. 2013, 2013, 245349. [Google Scholar] [CrossRef] [PubMed]
- Bianco, A.; Mammina, C.; Paoli, A.; Bellafiore, M.; Battaglia, G.; Caramazza, G.; Palma, A.; Jemni, M. Protein supplementation in strength and conditioning adepts: Knowledge, dietary behavior and practice in Palermo, Italy. J. Int. Soc. Sports Nutr. 2011, 8, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Khoury, D.; Antoine-Jonville, S. Intake of nutritional supplements among people exercising in gyms in Beirut City. J. Nutr. Metab. 2012, 2012, 703490. [Google Scholar] [CrossRef] [PubMed]
- Mohamad Shalan, N.A.; Azharuddin, N.F.; Abdul Rahim, N. Knowledge and awareness of dietary supplements among athletes in Universiti pendidikan sultan idris. J. Sains Sukan Pendidik. Jasm. 2018, 7, 120–129. [Google Scholar] [CrossRef]
- Denham, B.E. Athlete information sources about dietary supplements: A review of Extant Research. Int. J. Sport Nutr. Exerc. Metab. 2017, 27, 325–334. [Google Scholar] [CrossRef]
- Burns, R.D.; Schiller, M.R.; Merrick, M.A.; Wolf, K.N. Intercollegiate student athlete use of nutritional supplements and the role of athletic trainers and Dietitians in nutrition counseling. J. Am. Diet. Assoc. 2004, 104, 246–249. [Google Scholar] [CrossRef]
- Whitehouse, G.; Lawlis, T. Protein supplements and adolescent athletes: A pilot study investigating the risk knowledge, motivations and prevalence of use. Nutr. Diet. 2017, 74, 509–515. [Google Scholar] [CrossRef]
- Jacob, R.; Couture, S.; Lamarche, B.; Provencher, V.; Morissette, É.; Valois, P.; Goulet, C.; Drapeau, V. Determinants of coaches’ intentions to provide different recommendations on sports nutrition to their athletes. J. Int. Soc. Sports Nutr. 2019, 16, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Mohsen, H.; Yazbeck, N.; Al-Jawaldeh, A.; Bou Chahine, N.; Hamieh, H.; Mourad, Y.; Skaiki, F.; Salame, H.; Salameh, P.; Hoteit, M. Knowledge, attitudes, and practices related to dietary supplementation, before and during the COVID-19 pandemic: Findings from a cross-sectional survey in the Lebanese population. Int. J. Environ. Res. Public Health 2021, 18, 8856. [Google Scholar] [CrossRef]
- Chabaiki, I.J.; Bekadi, A.; Bechikh, M.Y. Sports supplements: Use, knowledge, and risks for Algerian athletes. N. Afr. J. Food Nutr. Res. 2020, 4, 231–239. [Google Scholar] [CrossRef]
- Petróczi, A.; Naughton, D.P.; Mazanov, J.; Holloway, A.; Bingham, J. Limited agreement exists between rationale and practice in athletes’ supplement use for maintenance of Health: A Retrospective Study. Nutr. J. 2007, 6, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vernec, A.; Stear, S.J.; Burke, L.M.; Castell, L.M. A–Z of nutritional supplements: Dietary supplements, sports nutrition foods and ergogenic AIDS for Health and performance: Part 48. Br. J. Sports Med. 2013, 47, 998–1000. [Google Scholar] [CrossRef] [Green Version]
- Mathews, N.M. Prohibited contaminants in dietary supplements. Sports Health Multidiscip. Approach 2018, 10, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.J.; Sherley, M.; McLeod, M. Adverse effects of sports supplements in men. Aust. Prescr. 2018, 41, 10–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bailey, R.L. Current regulatory guidelines and resources to support research of dietary supplements in the United States. Crit. Rev. Food Sci. Nutr. 2018, 60, 298–309. [Google Scholar] [CrossRef] [PubMed]
- FDA. Center for Food Safety and Applied Nutrition. Questions and Answers on Dietary Supplements. 2019. Available online: https://www.fda.gov/food/information-consumers-using-dietary-supplements/questions-and-answers-dietary-supplements (accessed on 19 February 2022).
- Knapik, J.J.; Steelman, R.A.; Hoedebecke, S.S.; Austin, K.G.; Farina, E.K.; Lieberman, H.R. Prevalence of dietary supplement use by athletes: Systematic Review and meta-analysis. Sports Med. 2015, 46, 103–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maughan, R.J. Topic 2: The use and abuse of dietary supplements by athletes. Nutr. Perform. Sport 2015, 46, 137–142. [Google Scholar] [CrossRef]
- Steinberg, L.; Monahan, K.C. Age differences in resistance to peer influence. Dev. Psychol. 2007, 43, 1531–1543. [Google Scholar] [CrossRef] [Green Version]
- Graupensperger, S.A.; Benson, A.J.; Evans, M.B. Everyone else is doing it: The association between Social Identity and susceptibility to peer influence in NCAA athletes. J. Sport Exerc. Psychol. 2018, 40, 117–127. [Google Scholar] [CrossRef]
- Al-Shaar, L.; Vercammen, K.; Lu, C.; Richardson, S.; Tamez, M.; Mattei, J. Health effects and public health concerns of energy drink consumption in the United States: A mini-review. Front. Public Health 2017, 5, 225. [Google Scholar] [CrossRef]
- Itany, M.; Diab, B.; Rachidi, S.; Awada, S.; Al Hajje, A.; Bawab, W.; Salameh, P. Consumption of energy drinks among Lebanese youth: A pilot study on the prevalence and side effects. Int. J. High Risk Behav. Addict. 2014, 3, e18857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wajid, S.; Aljaloud, S.O.; Al-Ghaiheb, A.L.; Khoshhal, K.I.; Konbaz, S.M.; Al Massad, A. Effect of athletes’ attitudes, beliefs, and knowledge on doping and dietary supplementation in Saudi Sports Clubs. J. Musculoskelet. Surg. Res. 2020, 4, 14. [Google Scholar] [CrossRef]
- Williams, M.H. Vitamin Supplementation and Athletic Performance. Int. J. Vitam. Nutr. Res. Suppl. 1989, 30, 163–191. Available online: https://pubmed.ncbi.nlm.nih.gov/2507696/ (accessed on 17 February 2022). [PubMed]
- Wagenmakers, A.J.M. Amino acid supplements to improve athletic performance. Curr. Opin. Clin. Nutr. Metab. Care 1999, 2, 539–544. [Google Scholar] [CrossRef]
- Chang, C.-K.; Chang Chien, K.-M.; Chang, J.-H.; Huang, M.-H.; Liang, Y.-C.; Liu, T.-H. Branched-chain amino acids and arginine improve performance in two consecutive days of simulated handball games in male and female athletes: A randomized trial. PLoS ONE 2015, 10, e0121866. [Google Scholar] [CrossRef] [PubMed]
- Blomstrand, E.; Eliasson, J.; Karlsson, H.K.; Köhnke, R. Branched-chain amino acids activate key enzymes in protein synthesis after physical exercise. J. Nutr. 2006, 136, 269S–273S. [Google Scholar] [CrossRef]
- Maughan, R.J. Creatine supplementation and exercise performance. Int. J. Sport Nutr. 1995, 5, 94–101. [Google Scholar] [CrossRef]
- Williams, M.H. Dietary supplements and sports performance: Introduction and vitamins. J. Int. Soc. Sports Nutr. 2004, 1, 1. [Google Scholar] [CrossRef] [Green Version]
- Peeling, P.; Binnie, M.J.; Goods, P.S.R.; Sim, M.; Burke, L.M. Evidence-based supplements for the enhancement of athletic performance. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 178–187. [Google Scholar] [CrossRef] [Green Version]
- Azakir, B.; Abou Daher, G.; Abou Al Naga, A. Dietary Supplements Consumption among Sportsmen Inlebanon. BAU J. Health Wellbeing 2018, 1, 7. Available online: https://digitalcommons.bau.edu.lb/hwbjournal/vol1/iss3/7 (accessed on 24 February 2022).
- Martínez-Sanz, J.; Sospedra, I.; Ortiz, C.; Baladía, E.; Gil-Izquierdo, A.; Ortiz-Moncada, R. Intended or unintended doping? A review of the presence of doping substances in dietary supplements used in sports. Nutrients 2017, 9, 1093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tawfik, S.; El Koofy, N.; Moawad, E.M. Patterns of nutrition and dietary supplements use in young Egyptian athletes: A community-based cross-sectional survey. PLoS ONE 2016, 11, e0161252. [Google Scholar] [CrossRef] [PubMed]
- Darvishi, L.; Askari, G.; Hariri, M.; Bahreynian, M.; Ghiasvand, R.; Ehsani, S.; Mashhadi, N.S.; Rezai, P.; Khorvash, F. The Use of Nutritional Supplements among Male Collegiate Athletes. Int. J. Prev. Med. 2013, 4, S68. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3665030/ (accessed on 16 February 2022). [PubMed]
- Jovanov, P.; Đorđić, V.; Obradović, B.; Barak, O.; Pezo, L.; Marić, A.; Sakač, M. Prevalence, knowledge and attitudes towards using sports supplements among young athletes. J. Int. Soc. Sports Nutr. 2019, 16, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dascombe, B.J.; Karunaratna, M.; Cartoon, J.; Fergie, B.; Goodman, C. Nutritional supplementation habits and perceptions of elite athletes within a state-based Sporting Institute. J. Sci. Med. Sport 2010, 13, 274–280. [Google Scholar] [CrossRef]
- Lun, V.; Erdman, K.A.; Fung, T.S.; Reimer, R.A. Dietary supplementation practices in Canadian high-performance athletes. Int. J. Sport Nutr. Exerc. Metab. 2012, 22, 31–37. [Google Scholar] [CrossRef]
- Braun, H.; Koehler, K.; Geyer, H.; Kleinert, J.; Mester, J.; Schänzer, W. Dietary supplement use among elite young German athletes. Int. J. Sport Nutr. Exerc. Metab. 2009, 19, 97–109. [Google Scholar] [CrossRef]
- Sundgot-Borgen, J.; Berglund, B.; Torstveit, M.K. Nutritional supplements in Norwegian elite athletes-impact of International Ranking and Advisors. Scand. J. Med. Sci. Sports 2003, 13, 138–144. [Google Scholar] [CrossRef]
- Sousa, M.; Fernandes, M.J.; Moreira, P.; Teixeira, V.H. Nutritional supplements usage by Portuguese athletes. Int. J. Vitam. Nutr. Res. 2013, 83, 48–58. [Google Scholar] [CrossRef]
- Baltazar-Martins, G.; de Brito Souza, D.; Aguilar-Navarro, M.; Muñoz-Guerra, J.; del Plata, M.; Del Coso, J. Prevalence and patterns of dietary supplement use in elite Spanish athletes. J. Int. Soc. Sports Nutr. 2019, 16, 30. [Google Scholar] [CrossRef] [Green Version]
- Schroder, H.; Navarro, E.; Mora, J.; Seco, J.; Torregrosa, J.M.; Tramullas, A. The type, amount, frequency and timing of dietary supplement use by elite players in the first Spanish Basketball League. J. Sports Sci. 2002, 20, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Nieper, A. Nutritional supplement practices in UK junior national track and field athletes. Br. J. Sports Med. 2005, 39, 645–649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nabuco, H.C.; Rodrigues, V.B.; Barros, W.M.; Ravagnani, F.C.; Espinosa, M.M.; de Ravagnani, C. Use of dietary supplements among Brazilian athletes. Rev. Nutr. 2017, 30, 163–173. [Google Scholar] [CrossRef] [Green Version]
- Van Janse Rensburg, D.C.; Sparks, I.M.; Fletcher, L.; van Jansen Rensburg, A. A cross-sectional study of 2550 amateur cyclists shows lack of knowledge regarding relevant sports nutrition guidelines. S. Afr. J. Sports Med. 2018, 30, 1–6. [Google Scholar] [CrossRef]
- Barrack, M.T.; Sassone, J.; Dizon, F.; Wu, A.C.; DeLuca, S.; Ackerman, K.E.; Tenforde, A.S. Dietary supplement intake and factors associated with increased use in preadolescent endurance runners. J. Acad. Nutr. Diet. 2022, 122, 573–582. [Google Scholar] [CrossRef]
- Scofield, D.E.; Unruh, S. Dietary supplement use among adolescent athletes in central Nebraska and their sources of information. J. Strength Cond. Res. 2006, 20, 452. [Google Scholar] [CrossRef]
- Froiland, K.; Koszewski, W.; Hingst, J.; Kopecky, L. Nutritional supplement use among college athletes and their sources of information. Int. J. Sport Nutr. Exerc. Metab. 2004, 14, 104–120. [Google Scholar] [CrossRef]
- Ziegler, P.J.; Nelson, J.A.; Jonnalagadda, S.S. Use of dietary supplements by elite figure skaters. Int. J. Sport Nutr. Exerc. Metab. 2003, 13, 266–276. [Google Scholar] [CrossRef]
- Brill, J.B.; Keane, M.W. Supplementation patterns of competitive male and female bodybuilders. Int. J. Sport Nutr. 1994, 4, 398–412. [Google Scholar] [CrossRef]
- Kim, J.; Kang, S.-K.; Jung, H.-S.; Chun, Y.-S.; Trilk, J.; Jung, S.H. Dietary supplementation patterns of Korean olympic athletes participating in the Beijing 2008 Summer Olympic Games. Int. J. Sport Nutr. Exerc. Metab. 2011, 21, 166–174. [Google Scholar] [CrossRef]
- Slater, G.; Tan, B.; Teh, K.C. Dietary supplementation practices of Singaporean athletes. Int. J. Sport Nutr. Exerc. Metab. 2003, 13, 320–332. [Google Scholar] [CrossRef] [PubMed]
- Rashani, N.; Pigera, S.; Fernando, P.; Nirriela, M.; Jayawickreme, S.; De Silva, A. Dietary Supplement Usage, Associated Knowledge and Attitudes of Sri Lankan National-Level Athletes: A Cross Sectional Study. J. Exerc. Nutr. 2021, 4. [Google Scholar] [CrossRef]
- Knapik, J.J.; Trone, D.W.; Austin, K.G.; Steelman, R.A.; Farina, E.K.; Lieberman, H.R. Prevalence, adverse events, and factors associated with dietary supplement and nutritional supplement use by US Navy and Marine Corps personnel. J. Acad. Nutr. Diet. 2016, 116, 1423–1442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baume, N.; Hellemans, L.; Saugy, M. Guide to over-the-Counter Sports Supplements for Athletes: Review Article: Semantic Scholar. 1970. Available online: https://www.semanticscholar.org/paper/Guide-to-over-the-counter-sports-supplements-for-%3A-Baume-Hellemans/648eeb526541aece7d76a7258b89d249448f7a2a (accessed on 17 February 2022).
- Maughan, R.J.; Depiesse, F.; Geyer, H. The use of dietary supplements by athletes. J. Sports Sci. 2007, 25 (Suppl. 1), S103–S113. [Google Scholar] [CrossRef]
- Adami, P.E.; Koutlianos, N.; Baggish, A.; Bermon, S.; Cavarretta, E.; Deligiannis, A.; Furlanello, F.; Kouidi, E.; Marques-Vidal, P.; Niebauer, J.; et al. Cardiovascular effects of doping substances, commonly prescribed medications and ergogenic aids in relation to sports: A position statement of the sport cardiology and exercise nucleus of the European Association of Preventive Cardiology. Eur. J. Prev. Cardiol. 2022, 29, 559–575. [Google Scholar] [CrossRef]
- Montuori, P.; Loperto, I.; Paolo, C.; Castrianni, D.; Nubi, R.; de Rosa, E.; Palladino, R.; Triassi, M. Bodybuilding, dietary supplements and hormones use: Behaviour and determinant analysis in young bodybuilders. BMC Sports Sci. Med. Rehabil. 2021, 13, 147. [Google Scholar] [CrossRef]
- Jawadi, A.H.; Addar, A.M.; Alazzam, A.S.; Alrabieah, F.O.; Al Alsheikh, A.S.; Amer, R.R.; Aldrees, A.A.; Al Turki, M.A.; Osman, A.K.; Badri, M. Prevalence of dietary supplements use among gymnasium users. J. Nutr. Metab. 2017, 2017, 9219361. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall N = 455 | Males N = 333 (73.1%) | Females N = 122 (26.9%) | p-Value | |||||
|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |||
| Age in years | Youths (15–24) | 202 | 44.4 | 140 | 42 | 62 | 50.8 | <0.001 |
| Adults (>24) | 253 | 55.6 | 193 | 58 | 60 | 49.2 | ||
| Marital status | Single | 304 | 66.8 | 223 | 67.0 | 81 | 66.4 | <0.001 |
| Married | 139 | 30.5 | 101 | 30.3 | 38 | 31.1 | ||
| Divorced | 7 | 1.5 | 5 | 1.5 | 2 | 1.6 | ||
| Widowed | 5 | 1.1 | 4 | 1.2 | 1 | 0.8 | ||
| Education level | High school or below | 178 | 39.1 | 147 | 44.3 | 31 | 25.4 | <0.001 |
| Bachelor’s degree | 188 | 41.3 | 129 | 38.7 | 59 | 48.4 | ||
| Master’s or Ph.D. degrees | 89 | 19.6 | 57 | 17.1 | 32 | 26.2 | ||
| Sports categories | Ball games | 198 | 43.5 | 151 | 45.3 | 47 | 38.5 | 0.406 |
| Combat sports | 123 | 27.0 | 91 | 27.4 | 32 | 26.2 | ||
| Endurance sports | 74 | 16.3 | 50 | 15.0 | 24 | 19.7 | ||
| Weightlifting | 60 | 13.2 | 41 | 12.3 | 19 | 15.6 | ||
| Duration being in their sports (years) | 2–5 | 204 | 44.8 | 134 | 40.2 | 70 | 57.3 | <0.001 |
| >5 | 251 | 55.2 | 199 | 59.7 | 52 | 42.6 | ||
| Time spent exercising (hours/week) | 10 or below | 368 | 80.9 | 256 | 76.8 | 112 | 91.7 | <0.001 |
| More than 10 | 87 | 19.1 | 77 | 23.1 | 10 | 8.1 | ||
| Competition level | Amateur | 248 | 54.4 | 169 | 50.7 | 78 | 64.0 | <0.001 |
| International | 54 | 11.8 | 42 | 12.6 | 12 | 9.8 | ||
| First-class player | 81 | 17.8 | 64 | 19.2 | 17 | 14.0 | ||
| Third/fourth-class players | 73 | 16.0 | 58 | 17.4 | 15 | 12.3 | ||
| Weight status | Underweight | 15 | 3.3 | 5 | 1.5 | 10 | 8.2 | <0.001 |
| Normal weight | 286 | 63.0 | 198 | 59.5 | 88 | 72.1 | ||
| Overweight | 113 | 24.8 | 98 | 29.4 | 15 | 12.3 | ||
| Obese | 41 | 9.0 | 32 | 9.6 | 9 | 7.4 | ||
| DSs-Related Knowledge | Overall N = 455 | Males N = 333 | Females N = 122 | |||||
|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | p-Value | ||
| DSs may be replacements for a balanced diet. | No | 303 | 66.6 | 222 | 66.6 | 81 | 66.4 | 0.956 |
| Yes | 152 | 33.4 | 111 | 33.4 | 41 | 33.6 | ||
| DSs’ ingredients interact with those of drugs. | No | 251 | 55.2 | 188 | 56.4 | 63 | 51.6 | 0.560 |
| Yes | 204 | 44.8 | 145 | 43.6 | 59 | 48.4 | ||
| DSs have side effects on health. | No | 209 | 45.9 | 155 | 46.5 | 54 | 44.3 | 0.665 |
| Yes | 246 | 54.1 | 178 | 53.5 | 68 | 55.7 | ||
| DSs build and support muscles. | No | 137 | 30.0 | 102 | 30.6 | 31 | 25.4 | 0.278 |
| Yes | 311 | 70.0 | 231 | 69.4 | 91 | 74.6 | ||
| The FDA is responsible for taking action against adulterated DSs. | No | 407 | 89.4 | 296 | 88.8 | 111 | 90.9 | 0.783 |
| Yes | 48 | 10.6 | 37 | 11.2 | 11 | 9.1 | ||
| DSs should undergo safety tests before marketing. | No | 424 | 93.1 | 304 | 91.3 | 120 | 98.3 | 0.045 |
| Yes | 31 | 6.9 | 29 | 8.7 | 2 | 1.7 | ||
| EDs energize the body. | No | 182 | 40.0 | 137 | 41.1 | 45 | 36.8 | 0.347 |
| Yes | 273 | 60.0 | 196 | 58.9 | 77 | 63.2 | ||
| EDs cause stress and fatigue. | No | 179 | 39.3 | 136 | 40.8 | 43 | 35.2 | 0.272 |
| Yes | 276 | 60.7 | 197 | 59.2 | 79 | 64.8 | ||
| EDs cause insomnia. | No | 179 | 39.3 | 136 | 40.8 | 43 | 35.2 | 0.223 |
| Yes | 276 | 60.7 | 197 | 59.2 | 79 | 64.8 | ||
| EDs may cause hallucinatory experiences. | No | 266 | 58.4 | 206 | 61.8 | 60 | 49.1 | 0.023 |
| Yes | 189 | 41.6 | 127 | 38.2 | 62 | 50.9 | ||
| EDs overconsumption may cause death. | No | 278 | 61.0 | 208 | 62.4 | 70 | 57.3 | 0.228 |
| Yes | 177 | 39.0 | 125 | 37.6 | 52 | 42.7 | ||
| DS-related attitudes. | N | % | N | % | N | % | p-value | |
| Sports supplements improve the body shape of athletes. | No | 210 | 46.2 | 157 | 47.1 | 53 | 43.4 | <0.001 |
| Yes | 245 | 53.8 | 176 | 52.9 | 69 | 56.6 | ||
| Sports supplements ameliorate performance. | No | 262 | 57.6 | 179 | 53.8 | 61 | 50 | <0.001 |
| Yes | 193 | 42.4 | 154 | 46.2 | 61 | 50 | ||
| DSs are necessary, only when food nutrients are not enough to meet dietary needs. | No | 240 | 52.7 | 193 | 58 | 69 | 56.6 | <0.001 |
| Yes | 215 | 47.3 | 140 | 42 | 53 | 43.4 | ||
| I am encouraged to use supplements if my teammates do so. | No | 70 | 15.4 | 54 | 16.2 | 17 | 14 | <0.001 |
| Yes | 385 | 84.6 | 279 | 83.8 | 105 | 86 | ||
| I use EDs because of their rich taste. | No | 271 | 59.5 | 202 | 60.6 | 75 | 61.5 | 0.06 |
| Yes | 184 | 40.5 | 131 | 39.4 | 47 | 38.5 | ||
| I believe that EDs have health-related risks. | No | 250 | 55 | 185 | 55.5 | 68 | 55.7 | 0.07 |
| Yes | 205 | 45 | 148 | 44.5 | 54 | 44.3 | ||
| Sports supplements on the Lebanese market have probably been manipulated. | No | 192 | 42.1 | 157 | 47.1 | 53 | 43.4 | 0.004 |
| Yes | 263 | 57.9 | 176 | 52.9 | 69 | 56.6 | ||
| DS-related practices. | N | % | N | % | N | % | p-value | |
| Use of sports supplements. | No | 222 | 48.8 | 159 | 47.8 | 63 | 48.4 | 0.462 |
| Yes | 233 | 51.2 | 174 | 52.2 | 59 | 51.6 | ||
| Use of vitamin and mineral supplements. | No | 293 | 64.4 | 218 | 65.5 | 75 | 61.5 | 0.408 |
| Yes | 162 | 35.6 | 115 | 34.5 | 47 | 38.5 | ||
| Use of energy drinks (EDs). | No | 338 | 74.3 | 244 | 73.2 | 94 | 77.0 | 0.414 |
| Yes | 114 | 25.7 | 86 | 51.1 | 28 | 23.0 | ||
| Estimated use of EDs (cans/week) (among users; N = 114). | 1–2 | 57 | 50.0 | 39 | 48.1 | 18 | 54.5 | 0.685 |
| 3–4 | 57 | 50.0 | 42 | 51.9 | 15 | 45.5 | ||
| Read the nutrition label of DSs. | No | 314 | 69.0 | 231 | 69.3 | 83 | 68.0 | 0.662 |
| Yes | 141 | 31.0 | 101 | 30.0 | 39 | 32.0 | ||
| Use of DSs based on health specialists’ recommendations. | No | 155 | 34.0 | 118 | 35.4 | 38 | 31.1 | 0.511 |
| Yes | 300 | 66.0 | 215 | 64.6 | 84 | 68.9 | ||
| DSs Use | |||||
|---|---|---|---|---|---|
| Yes | No | p-Value | |||
| Age | Youths | N (%) | 145 (71.8) | 57 (28.2) | 0.28 |
| Adults | N (%) | 193 (76.2) | 60 (23.8) | ||
| Gender | Male | N (%) | 245 (73.5) | 88 (26.5) | 0.57 |
| Female | N (%) | 93 (76.2) | 29 (23.8) | ||
| Education level | High school or below | N (%) | 120 (67.4) | 58 (32.6) | 0.01 |
| University | N (%) | 218 (78.7) | 59 (21.3) | ||
| Sports categories | Ball games | N (%) | 158 (79.8) | 40 (20.2) | 0.02 |
| Combat sports | N (%) | 90 (73.1) | 33 (26.9) | ||
| Endurance sports | N (%) | 45 (60.8) | 29 (39.2) | ||
| Weightlifting | N (%) | 45 (75) | 15 (25) | ||
| Competition level | Amateur | N (%) | 180 (72.8) | 67 (27.2) | 0.39 |
| International/ first class | N (%) | 106 (78.5) | 29 (21.5) | ||
| Third/fourth class | N (%) | 52 (71.2) | 21 (28.8) | ||
| Duration being in their sports (years) | 2–5 | N (%) | 152 (74.5) | 52 (25.5) | 0.92 |
| >5 | N (%) | 186 (74.1) | 65 (25.9) | ||
| Time spent exercising (h/week) | ≤10 | N (%) | 274 (74.5) | 94 (25.5) | 0.86 |
| >10 | N (%) | 64 (73.6) | 23 (26.4) | ||
| BMI | Underweight | N (%) | 8 (2.4) | 7 (6) | 0.03 |
| Normal | N (%) | 224 (66.3) | 62 (53) | ||
| Overweight | N (%) | 80 (23.7) | 33 (28.2) | ||
| Obese | N (%) | 26 (7.7) | 15 (12.8) | ||
| Binary Logistic Regression Taking the DSs Use among Athletes (No (Reference) vs. Yes) as the Dependent Variable | Odds Ratio (95% Confidence Interval) | p-Valve |
|---|---|---|
| Age (reference: youth) | - | - |
| Adults | 1.29 (0.82–2.05) | 0.27 |
| Gender (reference: male) | - | - |
| Female | 1.09 (0.65–1.85) | 0.74 |
| Education (reference: high school or below) | - | - |
| Holding a university degree | 1.81 (1.17–2.79) | 0.007 |
| Sports categories (reference: ball games) | - | |
| Combat sports | 0.69 (0.41–1.12) | 0.17 |
| Endurance sports | 0.39 (0.21–0.67) | <0.001 |
| Weightlifting | 0.70 (0.35–1.40) | 0.31 |
| BMI (reference: underweight) | - | - |
| Normal | 2.65 (0.87–8.05) | 0.08 |
| Overweight | 1.63 (0.49–5.37) | 0.42 |
| Obese | 1.12 (0.31–4.01) | 0.86 |
| Country | Author(s) (Year) | Sample Size and Subpopulation | Sport Disciplines | Dietary Supplements | Mostly Consumed | Total Prevalence of DSs Use (%) |
|---|---|---|---|---|---|---|
| Middle East/North Africa region (MENA region) | ||||||
| Saudi Arabia | Aljaloud, S. O. and Ibrahim, S. A. (2013) [22] | N = 105 professional male athletes (20 to 30 years old) | Football players from three teams residing in Riyadh: Al Hilal, Al Nasr, and Al-Shabab | Sports supplements, vitamins, minerals, carbohydrates, proteins, fish oils, herbals, and ergogenic aids | Sports supplements | 93.3% |
| Algeria | Chabaiki, I. J. et al. (2020) [31] | N = 200 recreational and professional athletes (males: 95%; mostly 21–30 years old) | Body building, football, martial arts, athletics, cross fit, power lifting, and swimming | Mass gainers, whey protein, BCAA, glutamine, creatine, vitamins, fat burners, and arginine | Mass gainers | 100% |
| Egypt | Tawfik, S. et al. (2016) [54] | N = 358 (13–18 years old; males: 56.4%) | Ball games (football, basketball, and volley ball); endurance (swimming, running, and cycling); weight class (wrestling, boxing, kickboxing, and weightlifting), and antigravity sports | Sports drinks, creatine, vitamins and minerals, and amino acids | Sports drinks and creatine | 48.9% |
| Iran | Darvishi, L. et al. (2013) [55] | N = 192 male collegiate athletes; individual sports (mean age: 21.2 ± 2.2 years); team sports: (mean age: 22.1 ± 2.4 years) | Individual and team sports | Protein powders, amino acid powders, carbohydrates, slimming products, fish oils, ergogenic aids, creatine, caffeine, vitamins and minerals, glucosamine, and chondroitin sulphate | Multivitamins and vitamin C | 45% |
| Asia region | ||||||
| Korea | Kim, J. et al. (2011) [72] | N = 161 athletes; male: 89%; 14–37 years old) | Hockey, handball, basketball, badminton, table tennis, weight lifting, distance running, boxing, archery, taekwondo, judo, wrestling, gymnastics, and swimming | Vitamins, oriental supplements, amino acids, creatine, Korean ginseng, Korean red ginseng, and deer antler | Vitamins and oriental supplements | Males: 79%; Females: 82% |
| Singapore | Slater, G., Tan, B. and Teh, K. C. (2003) [73] | N = 160 (males: 53.1%) | Swimming/water polo, combat, hockey, rugby, sailing, racket sports, volleyball, netball, and sepak takraw | Sports drinks, caffeine, vitamin C, multivitamins/ mineral supplements, essence of chicken, birds nest, creatine, ginseng, and weight-gain powders | Sports drinks, caffeine, vitamin C, and multivitamins/ mineral supplements | 77% |
| Sri Lanka | Rashani, SAN et al. (2021) [74] | N = 386 athletes (males: 66.8%; 18–41 years old) | Team (football, volleyball, rugby, hockey, kabaddi, and cricket); individual (wrestling, athletics, weight lifting, and karate); and mixed (wushu and badminton) sports | Multivitamin, electrolyte, protein, calcium, and creatine | Multivitamins | 91.5% |
| Europe | ||||||
| Spain | Baltazar-Martins, G., et al. (2019) [62] | N = 527 elite athletes participating in individual and team sports (males: 65.6%) | Bodybuilding, weightlifting, ball games, endurance sports, and combat sports | Proteins, amino acids/BCAAs, multivitamins, glutamine, creatine, carbohydrate powder, iron mix for recovery, joint support, omega 3, omega 6, magnesium, caffeine, B-alanine, and vitamin C | Proteins and amino acids/BCAAs | 64% |
| Germany | Braun, H. et al. (2009) [59] | N = 164 elite young athletes (males: 47%; 16.6 ± 3.0 years of age) | Endurance, racquet, ball, combat, and other sports | Vitamins, minerals, carbohydrate, protein, and fat supplements; sports drinks; and other ergogenic aids | Minerals, vitamins, sports drinks, energy drinks, and carbohydrates | 80% |
| Serbia, Germany, Japan and Croatia | Jovanov, P. et al. (2019) [56] | N = 348 athletes (males: 60.6%; 15–18 year olds) competing at the international level | Kayaking, rowing, canoeing, basketball, volleyball, swimming, athletics, boxing, soccer, tennis, karate, handball, water polo, dance, golf, weightlifting, archery, and fencing | Protein, carbohydrates, creatine, caffeine, NO reactor, beta alanine, glutamine, amino acids, vitamins and minerals, energy drinks | Protein supplements | 82.2% |
| Norway | Sundgot-Borgen, J., Berglund, B. and Torstveit, M. K. (2003). [60] | N = 1620 elite athletes (males: 69%; mean age: 23.2 ± 4.7 years for males; mean age: 21.4±4.6 years for females) | NA | Vitamins, minerals, omega 3, antioxidants, ginseng, amino acids, creatine, and energy supplements | Energy supplements | 53% |
| Portugal | Sousa, M. et al. (2013) [61] | N = 292 (males: 68%; 12–37 years old) | Volleyball, swimming, triathlon, cycling, judo, athletics, baseball, handball, rugby, gymnastics, basketball, fencing, and boxing | Multivitamins/minerals, sports drinks, magnesium, protein, glutamine, iron, sport gels, vitamin C, creatine, and antioxidants | Multivitamins/minerals, sports drinks, and magnesium | 66% |
| Spain | Schroder, H. et al. (2002) [63] | N = 55 professional athletes (mean age: 25.1 ± 4.0 years) | Basketball | Multivitamins and minerals, sports drinks, miscellaneous supplements, amino acids, proteins, and carbohydrates | Multivitamins and minerals | 58% |
| United Kingdom | Nieper, A. (2005) [64] | N = 32 athletes competing at the 2004 World Junior Championship (males: 62.5%; 18 years old) | Track and field | Ergogenic aids (creatine and caffeine) and recovery nutrients (vitamins/minerals, glucosamine, and glutamine) | Multivitamins and minerals | 62% |
| South and North America | ||||||
| United States | Barrack, M. T. et al. (2022) [67] | N = 2113 pre-adolescent endurance runners (males: 59.4%; mean age: 13.2 ± 0.9 years) | Track and field (running) | Vitamin/mineral supplements (multivitamins, vitamins C,D,E,B-complex, and others); non-vitamin/mineral supplements (amino acids, probiotics, diet pills, creatine, glutamine, herbs or botanicals); and sports foods (protein bars or drinks, electrolyte drinks, and energy bars) | Multivitamins | 26% |
| United States | Ziegler, P. J., Nelson, J. A. and Jonnalagadda, S. S. (2003) [70] | N = 124 athletes (males: 34.3%; mean age for males: 16.9 ± 0.3 years; mean age for females: 15.2 ± 0.2 years) | Figure skating | Multivitamins, minerals, protein powders, amino acid powders, protein bars, energy drinks, energy bars, creatine, herbal supplements, and others | Multivitamins and minerals | 71% |
| United States | Scofield, D. E. and Unruh, S. (2006) [68] | N = 139 adolescent athletes (males: 71%; mean age 15.8 ± 1.19 years) | Football, volleyball, basketball, wrestling, track and field, soccer, baseball, softball, power lifting, tennis, golf, cross country, swimming, and multisport | Creatine, MRP and protein, vitamins and minerals, diet energy | MRP protein | 22.3% |
| United States | Brill, J. B. and Keane, M. W. (1994) [71] | N = 309 (males: 68%; 13 to 70 years old) | Bodybuilding | Vitamins, protein powder, amino acids, minerals, weight-gain formulas, carbohydrate formulas, anabolic supplements, energy boosters, fat burners, human GH releasers, liver supplements, and sterols | Vitamins, minerals, amino acids, and protein powders | 98% |
| United States | Froiland, K. et al. (2004) [69] | N = 370 athletes (females: 55.8%) | Baseball, softball, volleyball, tennis, football, wrestling, bowling, yell squad and dance team, basketball, soccer, gymnastics, golf, track and field, swimming and diving, and rifle | Protein supplements, weight gainers, vitamin supplements, mineral supplements, herbals, and other supplements | Energy drinks | 61% |
| Canada | Lun, V. et al. (2012) [58] | N = 440 athletes (men: 37%; mean age: 9.99 ± 5.20 years) | Soccer, ice hockey, Taekwondo, speed skating, volleyball, figure skating, athletics, alpine skiing, luge, and basketball | Sports supplements, multivitamins, minerals, carbohydrate sports bars, protein powder, meal-replacement products, vitamin c, ginseng, protein bar, sports gel, iron, essential fatty acids, calcium, echinacea, L-glutamine, and energy drinks | Sports drinks, multivitamins and minerals, carbohydrate sports bars, protein powder, and meal-replacement products | 87% |
| Brazil | Nabuco, H. C. et al. (2017) [65] | N = 182 athletes (14 to 59 years old; males: 83%) | Endurance (triathlon, cycling, and swimming); bodybuilding; intermittent (volleyball, soccer, futsal, beach volleyball, tennis, and American football); combat (Taekwondo, karate, judo, kung Fu, Jiu Jitsu, MMA, boxing, and Mauy Thai); and other (athletics and shooting) sports | NA | NA | 45% |
| South and East Africa | ||||||
| Uganda | Muwonge. H, et al. (2017) [12] | N = 359 athletes (males: 74.7%; 15–35 years old) | Football, volleyball, rugby, netball, basketball, boxing, athletics, and cycling | Carbohydrate supplements, energy drinks, vitamin and mineral supplements, fish oils, protein supplements, herbal supplements, and ergogenic aids | Carbohydrate supplements, energy drinks, vitamin and mineral supplements, fish oils, and protein supplements | 13.4% |
| South Africa | Janse van Rensburg, D. C. et al. (2018) [66] | N = 2550 amateur athletes (25 to 45 years old; 75% males) | Cycling | NA | NA | 59% |
| Australia and Oceania | ||||||
| Australia | Dascombe, B. J. et al. (2010) [57] | N = 72 (21.9 ± 3.9 years old; males: 50%) | Kayaking, field hockey, rowing, water polo, swimming, athletics, and netball | Vitamins, minerals, glucosamine, iron, caffeine, creatine, mixed proteins CHO, proteins, and others | Minerals and vitamins | 87.5% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sadek, Z.; Mohsen, H.; Yazbek, S.; Nabulsi, Z.A.A.; Rifai Sarraj, A.; Hoteit, M. Dietary Supplements Use among Athletes in Lebanon: Knowledge, Attitudes, Practices, and Correlates. Foods 2022, 11, 1521. https://doi.org/10.3390/foods11101521
Sadek Z, Mohsen H, Yazbek S, Nabulsi ZAA, Rifai Sarraj A, Hoteit M. Dietary Supplements Use among Athletes in Lebanon: Knowledge, Attitudes, Practices, and Correlates. Foods. 2022; 11(10):1521. https://doi.org/10.3390/foods11101521
Chicago/Turabian StyleSadek, Zahra, Hala Mohsen, Saja Yazbek, Zein Al Abidin Nabulsi, Ahmad Rifai Sarraj, and Maha Hoteit. 2022. "Dietary Supplements Use among Athletes in Lebanon: Knowledge, Attitudes, Practices, and Correlates" Foods 11, no. 10: 1521. https://doi.org/10.3390/foods11101521
APA StyleSadek, Z., Mohsen, H., Yazbek, S., Nabulsi, Z. A. A., Rifai Sarraj, A., & Hoteit, M. (2022). Dietary Supplements Use among Athletes in Lebanon: Knowledge, Attitudes, Practices, and Correlates. Foods, 11(10), 1521. https://doi.org/10.3390/foods11101521