
Using Urinary Biomarkers to Estimate the Benzene Exposure Levels in Individuals Exposed to Benzene

Abstract
:1. Introduction
2. Materials and Method
2.1. Study Population
2.2. Personal Exposure
2.3. Urine Analysis
2.4. Calculation of Benzene Daily Intake (DI)
2.5. Back Calculated Airborne Benzene Levels
2.6. Statistical Analysis
3. Results
3.1. Summary Statistics
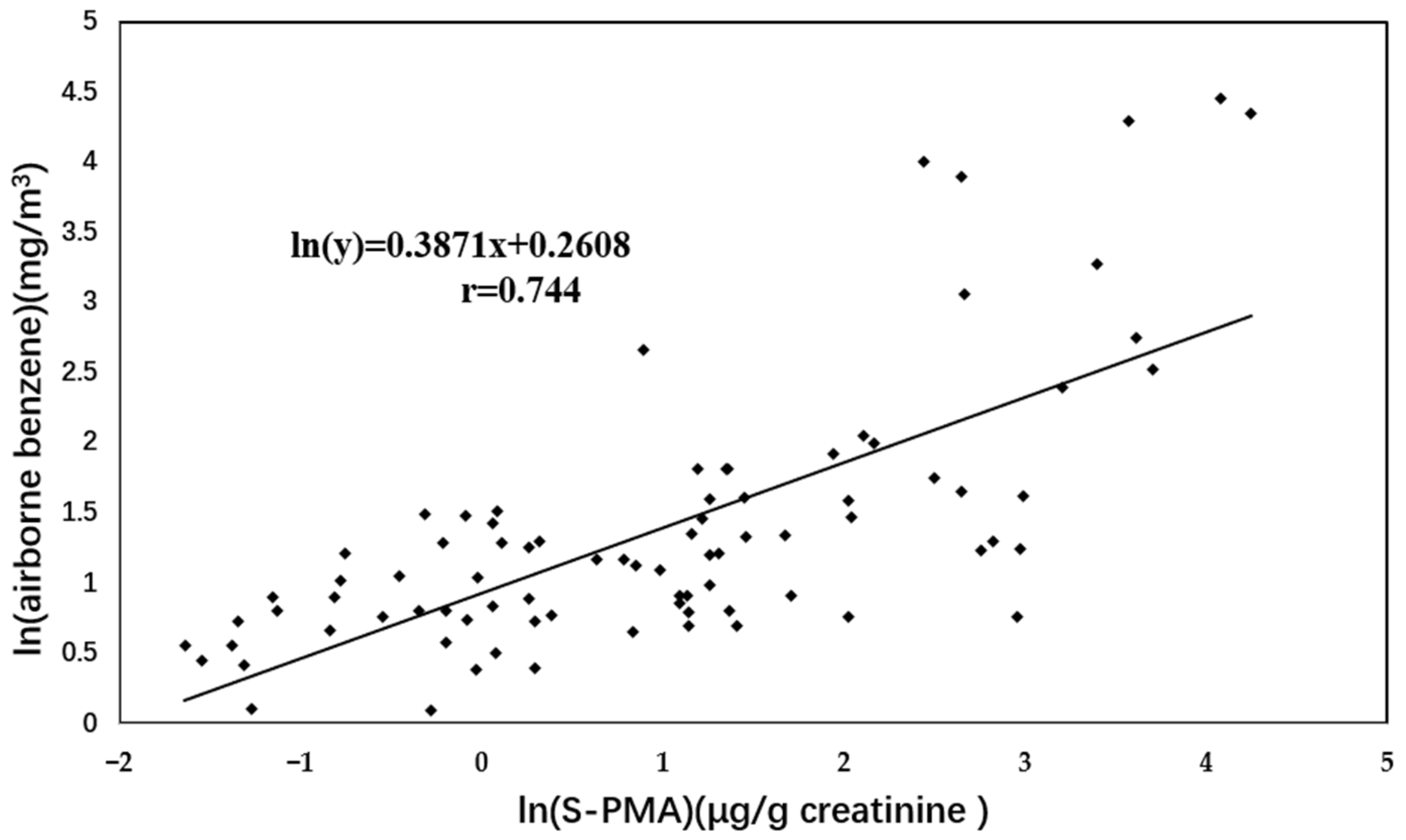
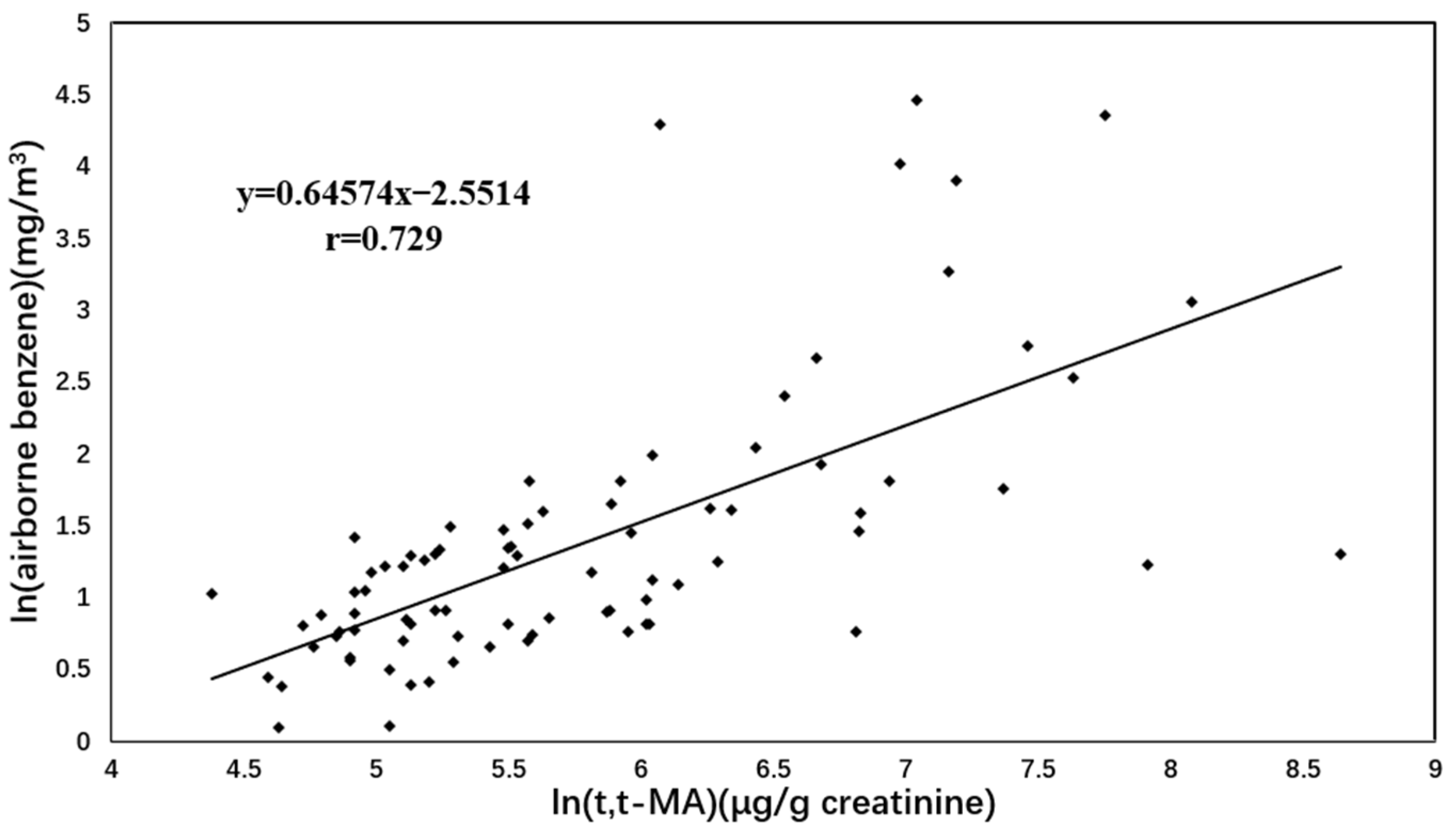
3.2. Comparison between Measured Airborne Benzene Levels and Back Calculated Airborne Benzene Levels
3.3. Comparison of BCABL Based on t, t-MA with Respect to Smoking in EXPOSED Subjects
3.4. Comparison of BCABL Based on t, t-MA with Respect to Dietary Habit in Exposed Subjects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, X.; Zhou, J.; Han, L.; Cheng, X.; Shao, H.; Jia, Q.; Xu, P.; Liu, J.; Ren, J.; Li, J.; et al. The Distribution and Concentration Monitoring of Benzene Industries—Six PLADs, China, 2020. China CDC Wkly. 2021, 3, 897–900. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Guo, X.; Chen, Y.; Zhang, W.; Ren, J.; Gao, A. Association between benzene exposure, serum levels of cytokines and hematological measures in Chinese workers: A cross-sectional study. Ecotoxicol. Environ. Saf. 2021, 207, 111562. [Google Scholar] [CrossRef] [PubMed]
- Khalade, A.; Jaakkola, M.S.; Pukkala, E.; Jaakkola, J.J. Exposure to benzene at work and the risk of leukemia: A systematic review and meta-analysis. Environ. Health A Glob. Access Sci. Source 2010, 9, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, M.T.; Zhang, L.; McHale, C.M.; Skibola, C.F.; Rappaport, S.M. Benzene, the exposome and future investigations of leukemia etiology. Chem. Biol. Interact. 2011, 192, 155–159. [Google Scholar] [CrossRef] [Green Version]
- Shallis, R.M.; Weiss, J.; Deziel, N.C.; Gore, S.D. A clandestine culprit with critical consequences: Benzene and acute myeloid leukemia. Blood Rev. 2021, 47, 100736. [Google Scholar] [CrossRef]
- Smith, M.T. Advances in Understanding Benzene Health Effects and Susceptibility. Annu. Rev. Public Health 2010, 31, 133–148. [Google Scholar] [CrossRef] [Green Version]
- Schnatter, A.R.; Glass, D.; Tang, G.; Irons, R.D.; Rushton, L. Myelodysplastic Syndrome and Benzene Exposure Among Petroleum Workers: An International Pooled Analysis. JNCI J. Natl. Cancer Inst. 2012, 104, 1724–1737. [Google Scholar] [CrossRef] [Green Version]
- Li, W.; Schnatter, A.R. Benzene risk assessment: Does new evidence on myelodysplastic syndrome justify a new approach? Crit. Rev. Toxicol. 2018, 48, 417–432. [Google Scholar] [CrossRef]
- International Agency for Research on Cancer. Monograph of carcinogenic risks in human. In Overall Evaluations of Carcinogenicity: An Updating of Iarc Monographs; IARC: Lyon, France, 1987; Volume 42, pp. 120–122. [Google Scholar]
- Seow, W.J.; Pesatori, A.; Dimont, E.; Farmer, P.B.; Albetti, B.; Ettinger, A.S.; Bollati, V.; Bolognesi, C.; Roggieri, P.; Panev, T.I.; et al. Urinary Benzene Biomarkers and DNA Methylation in Bulgarian Petrochemical Workers: Study Findings and Comparison of Linear and Beta Regression Models. PLoS ONE 2012, 7, e50471. [Google Scholar] [CrossRef] [Green Version]
- Carrieri, M.; Spatari, G.; Tranfo, G.; Sapienza, D.; Scapellato, M.L.; Bartolucci, G.B.; Manno, M. Biological monitoring of low level exposure to benzene in an oil refinery: Effect of modulating factors. Toxicol. Lett. 2018, 298, 70–75. [Google Scholar] [CrossRef]
- Lan, Q.; Zhang, L.; Li, G.; Vermeulen, R.; Weinberg, R.S.; Dosemeci, M.; Rappaport, S.M.; Shen, M.; Alter, B.P.; Wu, Y.; et al. Hematotoxicity in Workers Exposed to Low Levels of Benzene. Science 2004, 306, 1774–1776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rappaport, S.M.; Waidyanatha, S.; Yeowell-O’Connell, K.; Rothman, N.; Smith, M.T.; Zhang, L.; Qu, Q.; Shore, R.; Li, G.; Yin, S. Protein adducts as biomarkers of human benzene metabolism. Chem. Biol. Interact. 2005, 153, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Vermeulen, R.; Waidyanatha, S.; Johnson, B.A.; Lan, Q.; Rothman, N.; Smith, M.T.; Zhang, L.; Li, G.; Shen, M.; et al. Using urinary biomarkers to elucidate dose-related patterns of human benzene metabolism. Carcinogenesis 2006, 27, 772–781. [Google Scholar] [CrossRef] [PubMed]
- Melikian, A.A.; Qu, Q.; Shore, R.; Li, G.; Li, H.; Jin, X.; Cohen, B.; Chen, L.; Li, Y.; Yin, S.; et al. Personal exposure to different levels of benzene and its relationships to the urinary metabolites S-phenylmercapturic acid and trans,trans-muconic acid. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2002, 778, 211–221. [Google Scholar] [CrossRef]
- Koch, H.M.; Drexler, H.; Angerer, J. An estimation of the daily intake of di(2-ethylhexyl)phthalate (DEHP) and other phthalates in the general population. Int. J. Hyg. Environ. Health 2003, 206, 77–83. [Google Scholar] [CrossRef]
- Dewalque, L.; Charlier, C.; Pirard, C. Estimated daily intake and cumulative risk assessment of phthalate diesters in a Belgian general population. Toxicol. Lett. 2014, 231, 161–168. [Google Scholar] [CrossRef]
- Schettgen, T.; Ochsmann, E.B.; Alt, A.; Kraus, T.W. A biomarker approach to estimate the daily intake of benzene in non-smoking and smoking individuals in Germany. J. Expo. Sci. Environ. Epidemiol. 2010, 20, 427–433. [Google Scholar] [CrossRef]
- Paci, E.; Pigini, D.; Cialdella, A.M.; Faranda, P.; Tranfo, G. Determination of free and total S-phenylmercapturic acid by HPLC/MS/MS in the biological monitoring of benzene exposure. Biomarkers 2007, 12, 111–122. [Google Scholar] [CrossRef]
- Tranfo, G.; Paci, E.; Sisto, R.; Pigini, D. Validation of an HPLC/MS/MS method with isotopic dilution for quantitative determination of trans,trans-muconic acid in urine samples of workers exposed to low benzene concentrations. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2008, 867, 26–31. [Google Scholar] [CrossRef]
- Wijemanne, N.; Soysa, P.; Wijesundara, S.; Perera, H. Development and Validation of a Simple High Performance Liquid Chromatography/UV Method for Simultaneous Determination of Urinary Uric Acid, Hypoxanthine, and Creatinine in Human Urine. Int. J. Anal. Chem. 2018, 2018, 1647923. [Google Scholar] [CrossRef]
- David, R.M. Exposure to phthalate esters. Environ. Health Perspect. 2000, 108, A440. [Google Scholar] [CrossRef] [PubMed]
- Koch, H.M.; Becker, K.; Wittassek, M.; Seiwert, M.; Angerer, J.; Kolossa-Gehring, M. Di-n-butylphthalate and butylbenzylphthalateurinary metabolite levels and estimated daily intakes: Pilot study for the German Environmental Survey on children. J. Expo. Sci. Environ. Epidemiol. 2007, 17, 378–387. [Google Scholar] [CrossRef] [PubMed]
- Boogaard, P.J.; van Sittert, N.J. Suitability of S-phenyl mercapturic acid and trans-trans-muconic acid as biomarkers for exposure to low concentrations of benzene. Environ. Health Perspect. 1996, 104, 1151–1157. [Google Scholar] [CrossRef]
- Boogaard, P.J.; Van Sittert, N.J. Biological monitoring of exposure to benzene: A comparison between S-phenylmercapturic acid, trans,trans-muconic acid, and phenol. Occup. Environ. Med. 1995, 52, 611–620. [Google Scholar] [CrossRef] [Green Version]
- Sabourin, P.J.; Chen, B.; Lucier, G.; Birnbaum, L.S.; Fisher, E.; Henderson, R.F. Effect of dose on the absorption and excretion of [14C]benzene administered orally or by inhalation in rats and mice. Toxicol. Appl. Pharmacol. 1987, 87, 325–336. [Google Scholar] [CrossRef]
- Inoue, O.; Seiji, K.; Nakatsuka, H.; Watanabe, T.; Yin, S.N.; Li, G.L.; Cai, S.X.; Jin, C.; Ikeda, M. Urinary t,t-muconic acid as an indicator of exposure to benzene. Br. J. Ind. Med. 1989, 46, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Vermeulen, R.; Waidyanatha, S.; Johnson, B.A.; Lan, Q.; Smith, M.T.; Zhang, L.; Li, G.; Shen, M.; Yin, S.; et al. Modeling Human Metabolism of Benzene Following Occupational and Environmental Exposures. Cancer Epidemiol. Biomark. Prev. 2006, 15, 2246–2252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weaver, V.M.; Buckley, T.; Groopman, J.D. Lack of specificity of trans,trans-muconic acid as a benzene biomarker after ingestion of sorbic acid-preserved foods. Cancer Epidemiol. Biomark. Prev. 2000, 9, 749–755. [Google Scholar]
- Yu, R.; Weisel, C.P. Measurement of the urinary benzene metabolite trans,trans-muconic acid from benzene exposure in humans. J. Toxicol. Environ. Health Part A 1996, 48, 453–477. [Google Scholar] [CrossRef]
- Schettgen, T.; Musiol, A.; Alt, A.; Kraus, T. Fast determination of urinary S-phenylmercapturic acid (S-PMA) and S-benzylmercapturic acid (S-BMA) by column-switching liquid chromatography–tandem mass spectrometry. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2008, 863, 283–292. [Google Scholar] [CrossRef]
- Waidyanatha, S.; Rothman, N.; Fustinoni, S.; Smith, M.T.; Hayes, R.B.; Bechtold, W.; Dosemeci, M.; Guilan, L.; Yin, S.; Rappaport, S.M. Urinary benzene as a biomarker of exposure among occupationally exposed and unexposed subjects. Carcinogenesis 2001, 22, 279–286. [Google Scholar] [CrossRef]
- Ji, Y.; Gao, F.; Wu, Z.; Li, L.; Li, D.; Zhang, H.; Zhang, Y.; Gao, J.; Bai, Y.; Li, H. A review of atmospheric benzene homologues in China: Characterization, health risk assessment, source identification and countermeasures. J. Environ. Sci. 2020, 95, 225–239. [Google Scholar] [CrossRef] [PubMed]
- Teras, L.R.; Diver, W.R.; Deubler, E.L.; Krewski, D.; Flowers, C.R.; Switchenko, J.M.; Gapstur, S.M. Residential ambient benzene exposure in the United States and subsequent risk of hematologic malignancies. Int. J. Cancer 2019, 145, 2647–2660. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.-C.; Chen, W.-J.; Chiung, Y.-M.; Shih, T.-S.; Liao, P.-C. Association between GST Genetic Polymorphism and Dose-Related Production of Urinary Benzene Metabolite Markers, trans, trans-Muconic Acid and S-Phenylmercapturic Acid. Cancer Epidemiol. Biomark. Prev. 2008, 17, 1460–1469. [Google Scholar] [CrossRef] [Green Version]
- Jalai, A.; Ramezani, Z.; Ebrahim, K. Urinary Trans, Trans -Muconic Acid is Not a Reliable Biomarker for Low-level Environmental and Occupational Benzene Exposures. Saf. Health Work 2017, 8, 220–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruppert, T.; Scherer, G.; Tricker, A.R.; Adlkofer, F. trans,trans -Muconic acid as a biomarker of non-occupational environmental exposure to benzene. Int. Arch. Occup. Environ. Health 1997, 69, 247–251. [Google Scholar] [CrossRef]
- Fustinoni, S.; Consonni, D.; Campo, L.; Buratti, M.; Colombi, A.; Pesatori, A.C.; Bonzini, M.; Bertazzi, P.A.; Foà, V.; Garte, S.; et al. Monitoring Low Benzene Exposure: Comparative Evaluation of Urinary Biomarkers, Influence of Cigarette Smoking, and Genetic Polymorphisms. Cancer Epidemiol. Biomark. Prev. 2005, 14, 2237–2244. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Controls (n = 49) | Exposure (n = 84) | p-Value | |
|---|---|---|---|
| Age (years) | 32.5 ± 6.33 | 34.2 ± 10.0 | 0.87 a |
| Weight (kg) | 66.1 ± 9.56 | 64.8 ± 9.77 | 0.34 a |
| Working duration (years) | 2.12 ± 1.11 | 1.89 ± 1.32 | 0.12 a |
| Gender [n (%)] | 0.61 b | ||
| Male | 25 (51) | 39 (46) | |
| Female | 24 (49) | 45 (54) | |
| Current smokers [n (%)] | 0.03 b | ||
| Yes | 4 (8) | 19 (23) | |
| No | 45 (92) | 65 (77) | |
| Measured airborne benzene (mg/m3) | <0.001 a | ||
| Median | <0.024 | 3.27 | |
| Range | <0.024 | 1.10–86.2 |
| Exposed | Control | |||||
|---|---|---|---|---|---|---|
| Variable | Total (n = 84) | Smokers (n = 19) | Non-Smokers (n = 65) | Total (n = 49) | Smokers (n = 4) | Non-Smokers (n = 45) |
| S-PMA (μg/g creatinine) | ||||||
| Median | 17.0 | 15.3 | 20.2 | 0.38 | 1.31 | 0.36 |
| Range | 0.72–1908.7 | 1.26–150.8 | 0.72–1908.7 | 0.02–2.34 | 0.62–2.34 | 0.02–1.62 |
| p-value | <0.001 a | 0.176 b | 0.001 b | |||
| t, t-MA (μg/g creatinine) | ||||||
| Median | 371.4 | 264.8 | 404.0 | 68.4 | 117.2 | 63.9 |
| Range | 102.1–8331.2 | 102.1–2773.8 | 107.4–8331.2 | 26.1–252.4 | 41.1–186.6 | 26.1–252.4 |
| p-value | <0.001 a | 0.100 b | 0.004 b | |||
| Group (n) | Measured Airborne Benzene (mg/m3) | SPMA-Based Calculation | t, t-MA-Based Calculation | ||
|---|---|---|---|---|---|
| DI (μg/day) | BCABL (mg/m3) | DI (μg/day) | BCABL (mg/m3) | ||
| Controls (49) | <0.024 | 157.3 (9.62–1259.8) | 0.03 (0.002–0.25) | 1330.6 (405.1–4536.5) | 0.80 (0.24–2.72) |
| Exposed (84) | 3.27 (1.10–86.2) | 6919.1 (211.0–530,199.6) | 1.39 c (0.04–106.0) | 6123.8 (1447.0–131,036.1) | 3.67 c (0.87–78.6) |
| Subgroup (n) | Airborne Benzene (mg/m3) | BCABL (mg/m3) | p-Value |
|---|---|---|---|
| Smokers (19) | 2.49 (1.47–15.6) | 3.20 (1.40–34.5) | 0.091 a |
| ≤3.27 mg/m3 (12) | 2.04 (1.47–3.08) | 2.58 (1.39–7.58) | 0.200 a |
| >3.27 mg/m3 (7) | 3.85 (3.63–15.6) | 5.03 (2.96–34.5) | 0.710 a |
| Non-Smokers (65) | 3.36 (1.10–86.2) | 3.85 (0.87–78.6) | 0.483 a |
| ≤3.27 mg/m3 (30) | 2.24 (1.10–3.22) | 2.34 (0.87–19.8) | 0.525 a |
| >3.27 mg/m3 (35) | 5.03 (3.32–86.2) | 6.52 (1.01–78.6) | 0.883 a |
| Subgroup (n) | Airborne Benzene (mg/m3) | BCABL (mg/m3) | p-Value |
|---|---|---|---|
| Eat preserved food (30) | 3.57 (1.73–73.3) | 3.39 (0.98–78.6) | 0.836 a |
| ≤3.27 mg/m3 (11) | 2.24 (1.73–2.98) | 2.62 (0.98–11.1) | 0.401 a |
| >3.27 mg/m3 (19) | 4.46 (3.32–73.3) | 4.08 (1.01–78.6) | 0.246 a |
| Not eat preserved food (54) | 2.84 (1.10–86.2) | 3.87 (0.87–57.0) | 0.073 a |
| ≤3.27 mg/m3 (31) | 2.13 (1.10–3.22) | 2.51 (0.87–19.8) | 0.120 a |
| >3.27 mg/m3 (23) | 4.99 (3.43–86.2) | 8.62 (2.68–57.0) | 0.089 a |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cui, S.; Pang, B.; Yan, H.; Wu, B.; Li, M.; Xing, C.; Li, J. Using Urinary Biomarkers to Estimate the Benzene Exposure Levels in Individuals Exposed to Benzene. Toxics 2022, 10, 636. https://doi.org/10.3390/toxics10110636
Cui S, Pang B, Yan H, Wu B, Li M, Xing C, Li J. Using Urinary Biomarkers to Estimate the Benzene Exposure Levels in Individuals Exposed to Benzene. Toxics. 2022; 10(11):636. https://doi.org/10.3390/toxics10110636
Chicago/Turabian StyleCui, Shiwei, Bo Pang, Huifang Yan, Bo Wu, Ming Li, Caihong Xing, and Juan Li. 2022. "Using Urinary Biomarkers to Estimate the Benzene Exposure Levels in Individuals Exposed to Benzene" Toxics 10, no. 11: 636. https://doi.org/10.3390/toxics10110636
APA StyleCui, S., Pang, B., Yan, H., Wu, B., Li, M., Xing, C., & Li, J. (2022). Using Urinary Biomarkers to Estimate the Benzene Exposure Levels in Individuals Exposed to Benzene. Toxics, 10(11), 636. https://doi.org/10.3390/toxics10110636