
Kinetics of Excretion of the Perfluoroalkyl Surfactant cC6O4 in Humans

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Field Study
- Day 1: A working day with a 6:00 to 14:00 work-shift; the first blood sample was collected at the end of the shift (time 0 h);
- Day 2: A day off; at 8:00 the second blood sample was collected (time 18 h);
- Day 3: A day off; at 8:00 the third blood sample was collected (time 42 h);
- Day 4 and day 5: Two days off; no blood sample was collected;
- Day 6: A working day with a 6:00 to 14:00 work-shift; before the start of the shift the fourth blood sample was collected (time 114 h).
2.2. Analytical Measurements of Serum and Urinary cC6O4
2.3. Elimination Kinetics of Serum cC6O4 and Clearance
2.4. Statistical Analysis
3. Results
3.1. Study Subjects
3.2. Biological Monitoring
3.2.1. cC6O4 Urinary Excretion
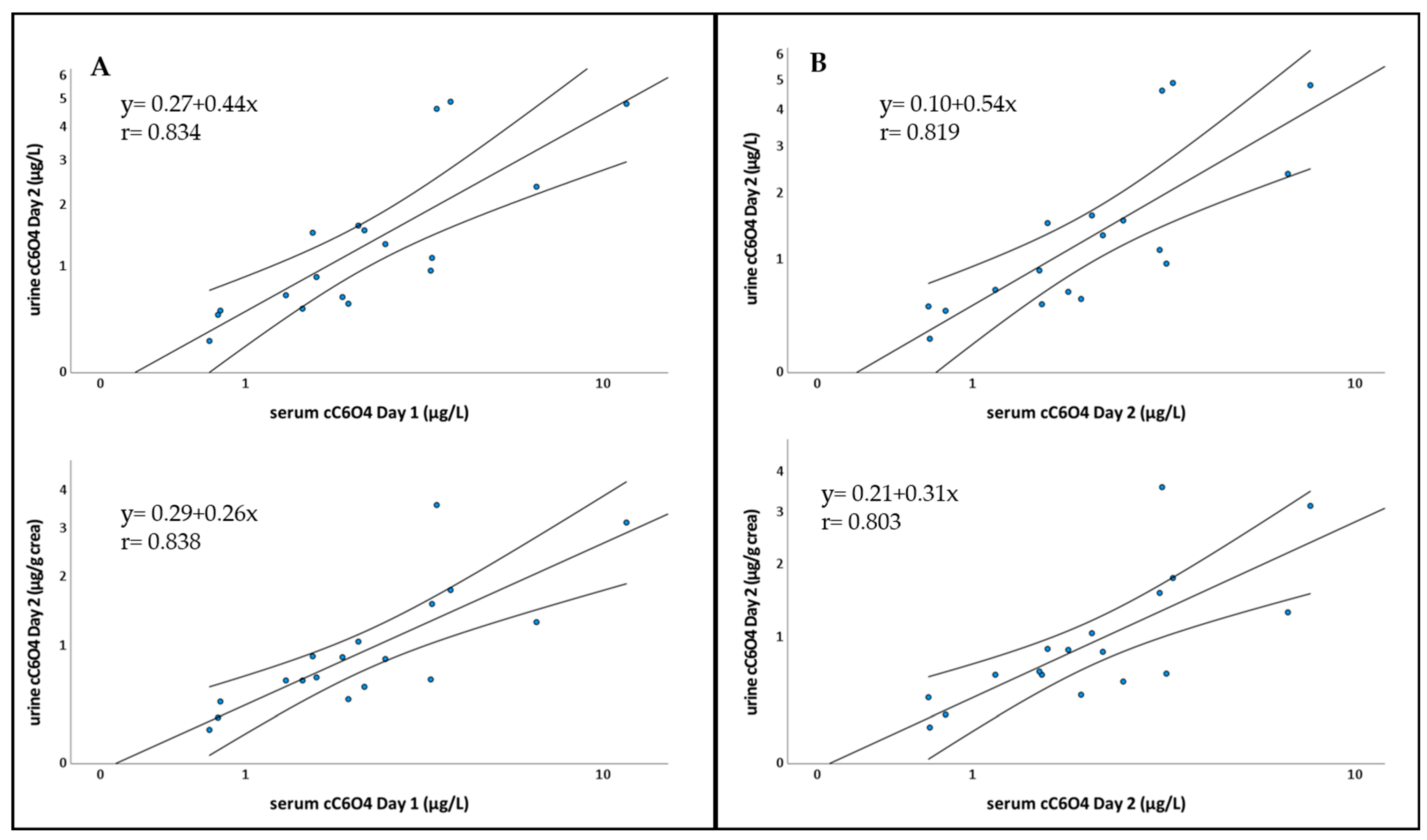
3.2.2. Pearson’s Correlation and Linear Regression
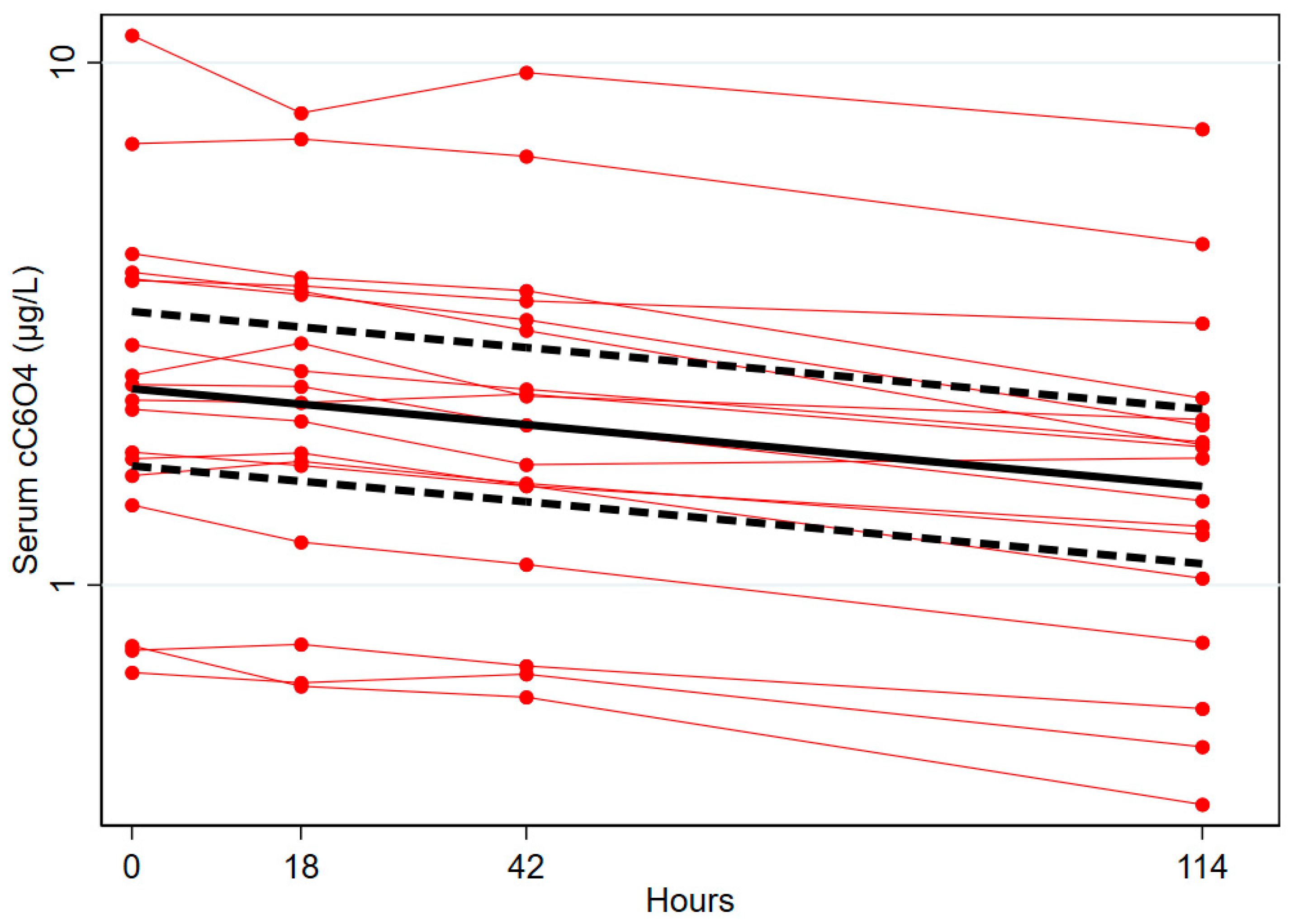
3.3. Kinetics of Elimination of cC6O4, Clearance and Distribution Volume
4. Discussion
- Different doses experienced by study individuals, resulting in a large variability in the concentration of the chemical in the investigated specimens;
- Difficulties in adhering to the study protocol, particularly in collecting all voids, resulting in missing voids or incomplete urine collection. Moreover, this is often associated with an under-reporting of missing samples.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- ECHA, Registration Dossier. Acetic Acid, 2,2-difluoro-2-[[2,2,4,5-tetrafluoro-5-(trifluoromethoxy)-1,3-dioxolan-4-yl]oxy]-, Ammonium Salt (1:1)). According to CLP (Regulation (EC) No 1272/2008. Available online: https://echa.europa.eu/it/registration-dossier/-/registered-dossier/5712 (accessed on 10 October 2022).
- Hopf, N.B.; Fustinoni, S. Biological monitoring of exposure to industrial chemicals. Part 2, Chemical Agents. In Patty’s Industrial Hygiene; Cohrssen, B., Ed.; Wiley: Hoboken, NJ, USA, 2021. [Google Scholar] [CrossRef]
- Jain, R.B.; Ducatman, A. Serum concentrations of selected perfluoroalkyl substances for US females compared to males as they age. Sci Total Environ. 2022, 842, 156891. [Google Scholar] [CrossRef] [PubMed]
- Girardi, P.; Rosina, A.; Merler, E. Report of the Project: Bio-PFAS: La Concentrazione di Sostanze Perfluorurate nel Sangue dei Dipendenti ed Ex-Dipendenti Delle Ditte RIMAR e Miteni. Trissino. Vicenza. Italia [In Italian]. 2018. Available online: https://pfas.land/2019/03/02/02-marzo-2019-persistenza-dei-pfas-nel-sangue-dei-lavoratori-miteni/ (accessed on 15 December 2022).
- Fustinoni, S.; Consonni, D. Historical Trend of Exposure to Perfluoroalkyl Surfactants PFOA, ADV, and cC6O4 and its Management in Two Perfluoroalkyl Polymers Plants, Italy. Ann. Work Exp. Health 2023, wxac095. [Google Scholar] [CrossRef] [PubMed]
- Decreto Legislativo 81 del 9 Aprile 2008. Available online: http://www.gazzettaufficiale.it/eli/id/2008/04/30/008G0104/sg (accessed on 7 July 2022).
- Frigerio, G.; Cafagna, S.; Polledri, E.; Mercadante, R.; Fustinoni, S. Development and validation of an LC-MS/MS method for the quantitation of 30 legacy and emerging per- and polyfluoroalkyl substances (PFASs) in human plasma, including HFPO-DA, DONA, and cC6O4. Anal. Bioanal. Chem. 2022, 414, 1259–1278. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food and Drug Administration. Bioanalytical Method Validation Guidance for Industry. Available online: https://www.fda.gov/files/drugs/published/Bioanalytical-Method-Validation-Guidance-for-Industry.pdf (accessed on 8 January 2022).
- EMA. ICH Guideline M10 on Bioanalytical Method Validation. 2022. Available online: https://www.ema.europa.eu/en/ich-m10-bioanalytical-method-validation-scientific-guideline#current-version-section (accessed on 8 January 2022).
- D'Avolio, A.; Cantu, M.; Gervasoni, J.; Artusi, C.; Marinova, M.; Nonnato, A.; Cangemi, G.; Persichilli, S. Bioanalytical method validation of quantitative mass spectrometry based assay: Experimental protocols and regulations. Biochim. Clin. 2018, 42, 51–61. [Google Scholar] [CrossRef]
- Kroll, M.H.; Chesler, R.; Hagengruber, C.; Blank, D.W.; Kestner, J.; Rawe, M. Automated determination of urinary creatinine without sample dilution: Theory and practice. Clin. Chem. 1986, 32, 446–452. [Google Scholar] [CrossRef] [PubMed]
- Knuiman, J.T.; Hautvast, J.G.; van der Heijden, L.; Geboers, J.; Joossens, J.V.; Tornqvist, H.; Isaksson, B.; Pietinen, P.; Tuomilehto, J.; Flynn, A.; et al. A multi-centre study on within-person variability in the urinary excretion of sodium, potassium, calcium, magnesium and creatinine in 8 European centres. Hum. Nutr. Clin. Nutr. 1986, 40, 343–348. [Google Scholar] [PubMed]
- Joossens, J.V.; Geboers, J. Monitoring Salt Intake of the Population: Methodological Considerations. In Surveillance of the Dietary Habits of the Population with Regard to Cardiovascular Diseases, EURONUT Report 2; De Backer, G.G., Pedoe, H.T., Ducimetiere, P., Eds.; Department of Human Nutrition, Agricultural University: Wageningen, The Netherlands, 1984; pp. 61–73. [Google Scholar]
- Chang, S.C.; Das, K.; Ehresman, D.J.; Ellefson, M.E.; Gorman, G.S.; Hart, J.A.; Noker, P.E.; Tan, Y.M.; Lieder, P.H.; Lau, C.; et al. Comparative pharmacokinetics of perfluorobutyrate in rats. mice. monkeys. and humans and relevance to human exposure via drinking water. Toxicol. Sci. 2008, 104, 40–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, D.S. The Chemours Company. 2021, March 17. Letter to EPA, Office of Pollution Prevention and Toxics Regarding Propanoic Acid, 2,3,3,3-tetrafluoro-2-(1,1,2,2,3,3,3-heptafluoropropoxy)-CAS RN 13252-13-6 (also Known as HFPO-DA). Available online: https://heronet.epa.gov/heronet/index.cfm/reference/details/reference_id/8631852 (accessed on 6 June 2022).
- U.S. Environmental Protection Agency. Human Health Toxicity Values for Hexafluoropropylene Oxide (HFPO) Dimer Acid and Its Ammonium Salt (CASRN 13252-13-6 and CASRN 62037-80-3), EPA Document Number: 822R-21-010. Available online: https://www.epa.gov/system/files/documents/2021-10/genx-chemicals-toxicity-assessment_tech-edited_oct-21-508.pdf (accessed on 2 October 2021).
- Olsen, G.W.; Burris, J.M.; Ehresman, D.J.; Froehlich, J.W.; Seacat, A.M.; Butenhoff, J.L.; Zobel, L.R. Half-life of serum elimination of perfluorooctanesulfonate.perfluorohexanesulfonate. and perfluorooctanoate in retired fluorochemical production workers. Environ. Health Perspect. 2007, 115, 1298–1305. [Google Scholar] [CrossRef] [PubMed]
- Bruno, S.; Bersani, M.; Astore, S.; Chiabotto, G.; Barge, A.; Binello, A.; Spyrakis, F. Lack of interaction of the fluorosurfactant C6O4 with human renal transporters: In vitro/in silico analysis. Toxicology 2022, 476, 153257. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameter (Unit) | Statistics | Data | |
|---|---|---|---|
| Personal characteristics | Male subjects | n (%) | 18 (100) |
| Age, year | mean ± SD | 44 ± 5 | |
| Weight, kg | mean ± SD | 79 ± 6 | |
| Height, cm | mean ± SD | 175 ± 6 | |
| BMI, kg/m2 | mean ± SD | 26.1 ± 2.3 | |
| Current tobacco smoker | n (%) | 4 (22) | |
| e-cig smoker | n (%) | 1 (5) | |
| Use of drugs | n (%) | 14 (78) | |
| Available samples | Blood samples | n | 72 |
| Blood sample/subject | n | 4 | |
| Urine samples | n | 254 | |
| Urine sample/subject (day 1–day 3) | n, mean ± SD | 14 ± 4 | |
| Lost urine samples | n | 14 | |
| Urinary creatinine | Creat (g/day) | mean ± SD | 1.465 ± 0.401 |
| Expected Crea (g/day) | mean ± SD | 1.905 ± 0.144 | |
| Crea ratio (%) | mean ± SD | 77 ± 21 | |
| Subjects with crea ratio < 60% | n (%) | 4 (22) |
| ID Subject | cC6O4 Serum µg/L | cC6O4 Urine µg/L | cC6O4 Urine µg/g Crea | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Day 1 | Day 2 | Day 3 | Day 6 | Day 1 | Day 2 | Day 3 | Day 6 | Day 1 | Day 2 | Day 3 | Day 6 | |
| 1 | 0.68 | 0.65 | 0.68 | 0.49 | 0.20 | 0.23 | 0.19 | 0.30 | 0.22 | 0.22 | ||
| 2 | 0.77 | 0.64 | 0.61 | 0.38 | 0.71 | 0.50 | 0.49 | 0.48 | 0.44 | 0.43 | ||
| 3 | 1.62 | 1.72 | 1.57 | 1.25 | 0.51 | 0.52 | 0.42 | 0.65 | 0.63 | 0.50 | ||
| 4 | 0.75 | 0.77 | 0.70 | 0.58 | 0.61 | 0.46 | 0.38 | 0.32 | 0.31 | 0.26 | ||
| 5 | 2.17 | 2.06 | 1.70 | 1.75 | 0.63 | 0.64 | 0.66 | 1.10 | 0.87 | 0.71 | ||
| 6 | 2.89 | 2.57 | 2.37 | 1.88 | 1.76 | 1.32 | 1.47 | 1.95 | 1.11 | 0.85 | 0.37 | 0.46 |
| 7 | 2.52 | 2.91 | 2.30 | 2.08 | 1.60 | 1.54 | 1.76 | 0.68 | 0.56 | 0.57 | 0.55 | 0.23 |
| 8 | 2.42 | 2.40 | 2.03 | 1.45 | 1.45 | 1.62 | 1.71 | 1.43 | 1.25 | 1.05 | 1.02 | 0.78 |
| 9 | 2.26 | 2.24 | 2.32 | 1.84 | 0.45 | 0.57 | 0.70 | 0.59 | 0.60 | 0.46 | 0.23 | 0.33 |
| 10 | 1.75 | 1.79 | 1.55 | 1.03 | 1.06 | 1.50 | 0.64 | 0.39 | 0.87 | 0.88 | 1.55 | 0.44 |
| 11 | 11.29 | 8.01 | 9.57 | 7.46 | 4.20 | 4.82 | 4.02 | 3.48 | 3.73 | 3.14 | 1.89 | 1.63 |
| 12 | 1.80 | 1.69 | 1.55 | 1.30 | 0.64 | 0.87 | 0.60 | 0.50 | 0.63 | 0.66 | 0.43 | 0.35 |
| 13 | 3.97 | 3.65 | 3.07 | 1.86 | 3.89 | 4.63 | 6.08 | 3.76 | 5.12 | 3.59 | 2.59 | 1.18 |
| 14 | 1.42 | 1.21 | 1.09 | 0.78 | 0.70 | 0.66 | 0.68 | 0.58 | 0.59 | 0.63 | 0.32 | 0.44 |
| 15 | 3.83 | 3.74 | 3.50 | 3.17 | 0.78 | 0.95 | 1.09 | 0.65 | 0.49 | 0.64 | 0.93 | 0.47 |
| 16 | 3.86 | 3.60 | 3.22 | 2.03 | 2.40 | 1.12 | 1.45 | 2.09 | 1.60 | 1.56 | 1.49 | 0.97 |
| 18 | 4.31 | 3.88 | 3.66 | 2.28 | 5.92 | 4.90 | 2.48 | 3.12 | 2.11 | 1.78 | 1.49 | 1.27 |
| 19 | 7.00 | 7.15 | 6.62 | 4.50 | 2.45 | 2.38 | 1.71 | 2.94 | 2.19 | 1.30 | 1.48 | 1.65 |
| Mean | 3.07 | 2.82 | 2.67 | 2.01 | 1.66 | 1.62 | 1.47 | 1.70 | 1.32 | 1.09 | 0.91 | 0.78 |
| SD | 2.58 | 2.03 | 2.24 | 1.69 | 1.57 | 1.55 | 1.48 | 1.26 | 1.28 | 0.93 | 0.69 | 0.50 |
| Min | 0.68 | 0.64 | 0.61 | 0.38 | 0.20 | 0.23 | 0.19 | 0.39 | 0.30 | 0.22 | 0.22 | 0.23 |
| p25 | 1.62 | 1.69 | 1.55 | 1.03 | 0.63 | 0.57 | 0.60 | 0.59 | 0.56 | 0.57 | 0.37 | 0.44 |
| Median | 2.34 | 2.32 | 2.17 | 1.80 | 0.92 | 1.04 | 0.90 | 1.43 | 0.76 | 0.76 | 0.63 | 0.47 |
| p75 | 3.86 | 3.65 | 3.22 | 2.08 | 2.40 | 1.62 | 1.71 | 2.94 | 1.60 | 1.30 | 1.49 | 1.18 |
| Max | 11.29 | 8.01 | 9.57 | 7.46 | 5.92 | 4.90 | 6.08 | 3.76 | 5.12 | 3.59 | 2.59 | 1.65 |
| cC6O4 in Serum Day 1 µg | cC6O4 in Serum Day 2 µg | cC6O4 in Urine Day 2 µg | Urinary Excretion (vs. Serum Day 1) % | Urinary Excretion (vs. Serum Day 2) % | |
|---|---|---|---|---|---|
| Mean | 9.50 | 8.73 | 1.62 | 18.9 | 20.1 |
| SD | 7.95 | 6.36 | 1.42 | 10.1 | 11.0 |
| Min | 1.92 | 1.70 | 0.34 | 4.8 | 4.9 |
| p25 | 5.51 | 5.38 | 0.74 | 12.5 | 12.8 |
| Median | 7.25 | 7.76 | 1.05 | 17.5 | 17.9 |
| p75 | 10.92 | 10.42 | 1.85 | 24.1 | 25.7 |
| Max | 34.08 | 24.18 | 5.37 | 46.4 | 50.5 |
| Statistics | Cl mL/min | Clw mL/min × kg | Serum Volume L | Vd, L | Vdw L/kg |
|---|---|---|---|---|---|
| Mean | 0.41 | 0.0052 | 3.1 | 6.6 | 0.084 |
| SD | 0.21 | 0.0026 | 0.4 | 3.4 | 0.042 |
| Min | 0.13 | 0.0015 | 2.6 | 2.1 | 0.023 |
| p25 | 0.29 | 0.0037 | 2.9 | 4.6 | 0.06 |
| Median | 0.38 | 0.0051 | 3.0 | 6.1 | 0.081 |
| p75 | 0.53 | 0.0064 | 3.1 | 8.6 | 0.103 |
| Max | 1.02 | 0.0128 | 4.0 | 16.3 | 0.204 |
| Chemical | Study | Study Subjects/Company/Country | N Subjects | N Samples, N/Subject | Years of Study | C0 Serum µg/L | t1/2 |
|---|---|---|---|---|---|---|---|
| PFOA | [5] | Fluorochemical workers after the ban of PFOA; Solvay, Italy | 93 (15 F) | 568, 2 to 9/subject | 2013–2021 | Median 750 | GM 3.16 (95% CI 2.98–3.37) years |
| PFOA | [17] | Retired fluorochemical workers; 3M, US | 26 (2 F) | 4 to 8/subject | 1998–2004 | Mean 691 | GM 3.5 (95% CI 3.0–4.1) years |
| PFOA | [4] | Retired fluorochemical workers; Miteni, Italy | 35 M | 81 2/subject | 2000–2018 | GM 1.489 | Mean 3.35 (95% CI 2.89–3.99) years |
| Perfluorobutyrate (PFBA) | [14] | Fluorochemical workers removed from the workplace for >7 days; 3M, US | 9 (2 F) | 2/subject | 2007 | 2–71 | 72 (95% CI 43–101) h |
| GenX | [15,16] | Fluorochemical workers off-work weekend (no exposure for 3–4 days); Chemours, NL | 18 | 2/subject | Before 2021 | Not reported | Mean ± SD 81 ± 55 h |
| cC6O4 | Present study | Fluorochemical workers removed from the workplace for 5 days; Solvay, Italy | 18 M | 72 4/subject | 2021–2022 | Median 2.34 | GM 184 (95% CI 162–213) h |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fustinoni, S.; Mercadante, R.; Lainati, G.; Cafagna, S.; Consonni, D. Kinetics of Excretion of the Perfluoroalkyl Surfactant cC6O4 in Humans. Toxics 2023, 11, 284. https://doi.org/10.3390/toxics11030284
Fustinoni S, Mercadante R, Lainati G, Cafagna S, Consonni D. Kinetics of Excretion of the Perfluoroalkyl Surfactant cC6O4 in Humans. Toxics. 2023; 11(3):284. https://doi.org/10.3390/toxics11030284
Chicago/Turabian StyleFustinoni, Silvia, Rosa Mercadante, Giorgia Lainati, Simone Cafagna, and Dario Consonni. 2023. "Kinetics of Excretion of the Perfluoroalkyl Surfactant cC6O4 in Humans" Toxics 11, no. 3: 284. https://doi.org/10.3390/toxics11030284
APA StyleFustinoni, S., Mercadante, R., Lainati, G., Cafagna, S., & Consonni, D. (2023). Kinetics of Excretion of the Perfluoroalkyl Surfactant cC6O4 in Humans. Toxics, 11(3), 284. https://doi.org/10.3390/toxics11030284