
Male Lower Urinary Tract Dysfunction: An Underrepresented Endpoint in Toxicology Research

Abstract
:1. Introduction
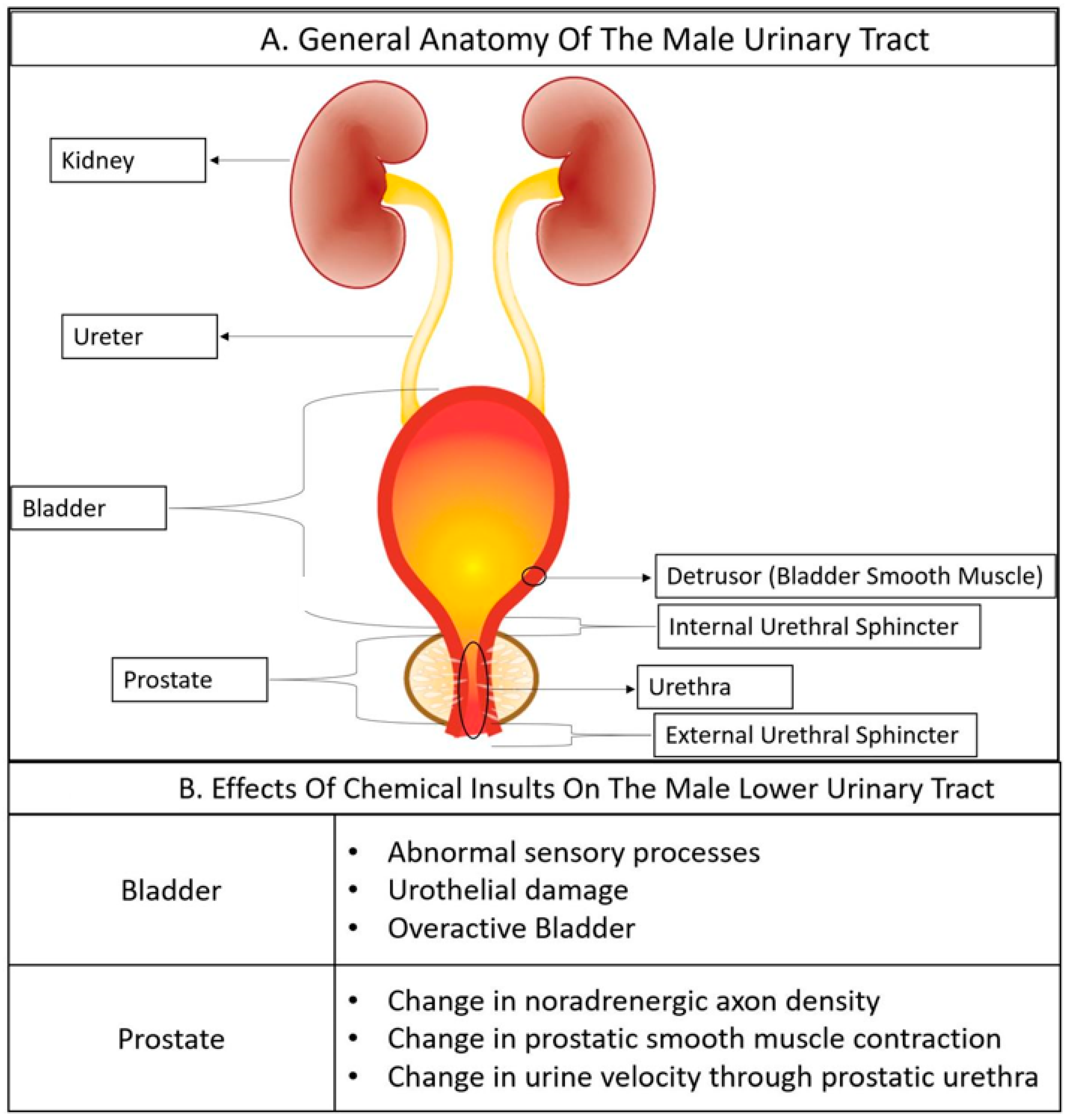
2. Overview of Male Lower Urinary Tract Anatomy and Physiology
2.1. The Bladder
2.2. The Urethra
2.3. The Urethral Sphincter
2.4. The Prostate
3. LUTD Mechanisms
3.1. Benign Prostatic Diseases
3.2. Bladder Mechanisms of Male LUTD
3.3. Urethral Mechanisms of Male LUTD
3.4. The Relationship between LUTD and Comorbidities
4. Mouse Research Models of Male LUTD
4.1. Benign Prostatic Hyperplasia
4.2. Mouse Models of Prostate Inflammation
4.3. Mouse Models of Partial Bladder Outlet Obstruction (pBOO)
4.4. Mouse Models of Overactive Bladder (OAB)
4.5. Mouse Models of Detrusor Sphincter Dyssynergia (DSD)
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jacobsen, S.J.; Jacobson, D.J.; Girman, C.J.; Roberts, R.O.; Rhodes, T.; Guess, H.A.; Lieber, M.M. Natural history of prostatism: Risk factors for acute urinary retention. J. Urol. 1997, 158, 481–487. [Google Scholar] [CrossRef]
- Roehrborn, C.G.; Malice, M.-P.; Cook, T.J.; Girman, C.J. Clinical predictors of spontaneous acute urinary retention in men with luts and clinical bph: A comprehensive analysis of the pooled placebo groups of several large clinical trials. Urology 2001, 58, 210–216. [Google Scholar] [CrossRef]
- Winters, J.C.; Dmochowski, R.R.; Goldman, H.B.; Herndon, C.D.; Kobashi, K.C.; Kraus, S.R.; Lemack, G.E.; Nitti, V.W.; Rovner, E.S.; Wein, A.J.; et al. Urodynamic studies in adults: AUA/SUFU guideline. J. Urol. 2012, 188, 2464–2472. [Google Scholar] [CrossRef]
- Agarwal, A.; Eryuzlu, L.N.; Cartwright, R.; Thorlund, K.; Tammela, T.L.; Guyatt, G.H.; Auvinen, A.; Tikkinen, K.A. What is the most bothersome lower urinary tract symptom? Individual- and population-level perspectives for both men and women. Eur. Urol. 2014, 65, 1211–1217. [Google Scholar] [CrossRef] [Green Version]
- Shah, H.N. Benign prostate hyperplasia and bladder stones: An update. Curr. Bladder Dysfunct. Rep. 2013, 8, 250–260. [Google Scholar] [CrossRef]
- Wei, J.T.; Calhoun, E.; Jacobsen, S.J. Urologic diseases in america project: Benign prostatic hyperplasia. J. Urol. 2005, 173, 1256–1261. [Google Scholar] [CrossRef]
- Launer, B.M.; McVary, K.T.; Ricke, W.A.; Lloyd, G.L. The rising worldwide impact of benign prostatic hyperplasia. BJU Int. 2021, 127, 722–728. [Google Scholar] [CrossRef]
- Kobelt, G.; Borgstrom, F.; Mattiasson, A. Productivity, vitality and utility in a group of healthy professionally active individuals with nocturia. BJU Int. 2003, 91, 190–195. [Google Scholar] [CrossRef] [Green Version]
- Cakir, O.O.; McVary, K.T. LUTS and sleep disorders: Emerging risk factor. Curr. Urol. Rep. 2012, 13, 407–412. [Google Scholar] [CrossRef]
- Ancoli-Israel, S.; Bliwise, D.L.; Norgaard, J.P. The effect of nocturia on sleep. Sleep Med. Rev. 2011, 15, 91–97. [Google Scholar] [CrossRef]
- Johnson, T.V.; Abbasi, A.; Ehrlich, S.S.; Kleris, R.S.; Owen-Smith, A.; Raison, C.L.; Master, V.A. IPSS quality of life question: A possible indicator of depression among patients with lower urinary tract symptoms. Can. J. Urol. 2012, 19, 6100–6104. [Google Scholar]
- Rom, M.; Schatzl, G.; Swietek, N.; Rucklinger, E.; Kratzik, C. Lower urinary tract symptoms and depression. BJU Int. 2012, 110, E918–E921. [Google Scholar] [CrossRef]
- Jepsen, J.V.; Bruskewitz, R.C. Recent developments in the surgical management of benign prostatic hyperplasia. Urology 1998, 51, 23–31. [Google Scholar] [CrossRef]
- Chute, C.G.; Panser, L.A.; Girman, C.J.; Oesterling, J.E.; Guess, H.A.; Jacobsen, S.J.; Lieber, M.M. The prevalence of prostatism: A population-based survey of urinary symptoms. J. Urol. 1993, 150, 85–89. [Google Scholar] [CrossRef]
- Berry, S.J.; Coffey, D.S.; Walsh, P.C.; Ewing, L.L. The development of human benign prostatic hyperplasia with age. J. Urol. 1984, 132, 474–479. [Google Scholar] [CrossRef]
- Hutchison, A.; Farmer, R.; Verhamme, K.; Berges, R.; Navarrete, R.V. The efficacy of drugs for the treatment of LUTS/BPH, a study in 6 European countries. Eur. Urol. 2007, 51, 207–216. [Google Scholar] [CrossRef]
- Kirby, R.S.; Roehrborn, C.; Boyle, P.; Bartsch, G.; Jardin, A.; Cary, M.M.; Sweeney, M.; Grossman, E.B. Efficacy and tolerability of doxazosin and finasteride, alone or in combination, in treatment of symptomatic benign prostatic hyperplasia: The Prospective European doxazosin and combination therapy (PREDICT) trial. Urology 2003, 61, 119–126. [Google Scholar] [CrossRef]
- Roehrborn, C.G. Efficacy of alpha-adrenergic receptor blockers in the treatment of male lower urinary tract symptoms. Rev. Urol. 2009, 11, S1–S8. [Google Scholar]
- Keil Stietz, K.P.; Kennedy, C.L.; Sethi, S.; Valenzuela, A.; Nunez, A.; Wang, K.; Wang, Z.; Wang, P.; Spiegelhoff, A.; Puschner, B.; et al. In utero and lactational pcb exposure drives anatomic changes in the juvenile mouse bladder. Curr. Res. Toxicol. 2021, 2, 1–18. [Google Scholar] [CrossRef]
- Turco, A.E.; Oakes, S.R.; Stietz, K.P.K.; Dunham, C.L.; Joseph, D.B.; Chathurvedula, T.S.; Girardi, N.M.; Schneider, A.J.; Gawdzik, J.; Sheftel, C.M.; et al. A neuroanatomical mechanism linking perinatal TCDD exposure to lower urinary tract dysfunction in adulthood. Dis. Model Mech. 2021, 14, 1–10. [Google Scholar] [CrossRef]
- Turco, A.E.; Thomas, S.; Crawford, L.K.; Tang, W.; Peterson, R.E.; Li, L.; Ricke, W.A.; Vezina, C.M. In utero and lactational 2,3,7,8-tetrachlorodibenzo-p-dioxin (TCDD) exposure exacerbates urinary dysfunction in hormone-treated c57bl/6j mice through a non-malignant mechanism involving proteomic changes in the prostate that differ from those elicited by testosterone and estradiol. Am. J. Clin. Exp. Urol. 2020, 8, 59–72. [Google Scholar] [PubMed]
- Middleton, L.W.; Shen, Z.; Varma, S.; Pollack, A.S.; Gong, X.; Zhu, S.; Zhu, C.; Foley, J.W.; Vennam, S.; Sweeney, R.T.; et al. Genomic analysis of benign prostatic hyperplasia implicates cellular re-landscaping in disease pathogenesis. JCI Insight 2019, 5, e129749. [Google Scholar] [CrossRef] [PubMed]
- Joseph, D.B.; Henry, G.H.; Malewska, A.; Reese, J.C.; Mauck, R.J.; Gahan, J.C.; Hutchinson, R.C.; Mohler, J.L.; Roehrborn, C.G.; Strand, D.W. 5-alpha reductase inhibitors induce a prostate luminal to club cell transition in human benign prostatic hyperplasia. J. Pathol. 2021, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Joseph, D.B.; Henry, G.H.; Malewska, A.; Iqbal, N.S.; Ruetten, H.M.; Turco, A.E.; Abler, L.L.; Sandhu, S.K.; Cadena, M.T.; Malladi, V.S.; et al. Urethral luminal epithelia are castration-insensitive cells of the proximal prostate. Prostate 2020, 80, 872–884. [Google Scholar] [CrossRef] [PubMed]
- Andersson, K.-E.; McCloskey, K.D. Lamina propria: The functional center of the bladder? Neurourol. Urodyn. 2014, 33, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Apodaca, G. The uroepithelium: Not just a passive barrier. Traffic 2004, 5, 117–128. [Google Scholar] [CrossRef] [PubMed]
- Graham, E.; Chai, T.C. Dysfunction of bladder urothelium and bladder urothelial cells in interstitial cystitis. Curr. Urol. Rep. 2006, 7, 440–446. [Google Scholar] [CrossRef]
- Guo, C.; Balsara, Z.R.; Hill, W.G.; Li, X. Stage- and subunit-specific functions of polycomb repressive complex 2 in bladder urothelial formation and regeneration. Development 2017, 144, 400–408. [Google Scholar] [CrossRef] [Green Version]
- Khandelwal, P.; Abraham, S.N.; Apodaca, G. Cell biology and physiology of the uroepithelium. Am. J. Physiol. Ren. Physiol. 2009, 297, F1477–F1501. [Google Scholar] [CrossRef] [Green Version]
- Hurst, R.E. Structure, function, and pathology of proteoglycans and glycosaminoglycans in the urinary tract. World J. Urol. 1994, 12, 3–10. [Google Scholar] [CrossRef]
- Hu, P.; Deng, F.-M.; Liang, F.-X.; Hu, C.-M.; Auerbach, A.B.; Shapiro, E.; Wu, X.-R.; Kachar, B.; Sun, T.-T. Ablation of uroplakin III gene results in small urothelial plaques, urothelial leakage, and vesicoureteral reflux. J. Cell Biol. 2000, 151, 961–972. [Google Scholar] [CrossRef]
- Wu, X.R.; Kong, X.P.; Pellicer, A.; Kreibich, G.; Sun, T.T. Uroplakins in urothelial biology, function, and disease. Kidney Int. 2009, 75, 1153–1165. [Google Scholar] [CrossRef] [Green Version]
- Kątnik-Prastowska, I.; Lis, J.; Matejuk, A. Glycosylation of uroplakins. Implications for bladder physiopathology. Glycoconj. J. 2014, 31, 623–636. [Google Scholar] [CrossRef] [Green Version]
- Gandhi, D.; Molotkov, A.; Batourina, E.; Schneider, K.; Dan, H.; Reiley, M.; Laufer, E.; Metzger, D.; Liang, F.; Liao, Y.; et al. Retinoid signaling in progenitors controls specification and regeneration of the urothelium. Develop. Cell 2013, 26, 469–482. [Google Scholar] [CrossRef] [Green Version]
- Sutherland Ronald, S.; Baskin Laurence, S.; Hayward Simon, W.; Cunha Gerald, R. Regeneration of bladder urothelium, smooth muscle, blood vessels and nerves into an acellular tissue matrix. J. Urol. 1996, 156, 571–577. [Google Scholar] [CrossRef]
- Hicks, R.M. The mammalian urinary bladderan accommodating organ. Biol. Rev. 1975, 50, 215–246. [Google Scholar] [CrossRef]
- Joseph, D.B.; Chandrashekar, A.S.; Abler, L.L.; Chu, L.F.; Thomson, J.A.; Mendelsohn, C.; Vezina, C.M. In vivo replacement of damaged bladder urothelium by Wolffian duct epithelial cells. Proc. Natl. Acad. Sci. USA 2018, 115, 8394–8399. [Google Scholar] [CrossRef] [Green Version]
- Cox, P.J. Cyclophosphamide cystitis—Identification of acrolein as the causative agent. Biochem. Pharmacol. 1979, 28, 2045–2049. [Google Scholar] [CrossRef]
- Brock, N.; Stekar, J.; Pohl, J.; Niemeyer, U.; Scheffler, G. Acrolein, the causative factor of urotoxic side-effects of cyclophosphamide, ifosfamide, trofosfamide and sufosfamide. Arzneimittelforschung 1979, 29, 659–661. [Google Scholar]
- Al-Rawithi, S.; El-Yazigi, A.; Ernst, P.; Al-Fiar, F.; Nicholls, P.J. Urinary excretion and pharmacokinetics of acrolein and its parent drug cyclophosphamide in bone marrow transplant patients. Bone Marrow Transplant. 1998, 22, 485–490. [Google Scholar] [CrossRef] [Green Version]
- Andersson, K.E.; Nomiya, M.; Yamaguchi, O. Chronic pelvic ischemia: Contribution to the pathogenesis of lower urinary tract symptoms (LUTS): A new target for pharmacological treatment? Low Urin. Tract Symptoms 2015, 7, 1–8. [Google Scholar] [CrossRef]
- Birder, L.A.; Kanai, A.J.; de Groat, W.C.; Kiss, S.; Nealen, M.L.; Burke, N.E.; Dineley, K.E.; Watkins, S.; Reynolds, I.J.; Caterina, M.J. Vanilloid receptor expression suggests a sensory role for urinary bladder epithelial cells. Proc. Natl. Acad. Sci. USA 2001, 98, 13396–13401. [Google Scholar] [CrossRef] [Green Version]
- Ferguson, D.R.; Kennedy, I.; Burton, T.J. ATP is released from rabbit urinary bladder epithelial cells by hydrostatic pressure changes—Possible sensory mechanism? J. Physiol. 1997, 505, 503–511. [Google Scholar] [CrossRef]
- Wiseman, O.J.; Fowler, C.J.; Landon, D.N. The role of the human bladder lamina propria myofibroblast. BJU Int. 2003, 91, 89–93. [Google Scholar] [CrossRef] [Green Version]
- Aitken, K.J.; Bägli, D.J. The bladder extracellular matrix. Part I: Architecture, development and disease. Nat. Rev. Urol. 2009, 6, 596–611. [Google Scholar] [CrossRef]
- Andersson, K.-E.; Arner, A. Urinary bladder contraction and relaxation: Physiology and pathophysiology. Physiol. Rev. 2004, 84, 935–986. [Google Scholar] [CrossRef] [Green Version]
- Sjuve, R.; Haase, H.; Ekblad, E.; Malmqvist, U.; Morano, I.; Arner, A. Increased expression of non-muscle myosin heavy chain-B in connective tissue cells of hypertrophic rat urinary bladder. Cell Tissue Res. 2001, 304, 271–278. [Google Scholar] [CrossRef]
- Seki, T.; Naito, I.; Oohashi, T.; Sado, Y.; Ninomiya, Y. Differential expression of type IV collagen isoforms, alpha5(IV) and alpha6(IV) chains, in basement membranes surrounding smooth muscle cells. Histochem. Cell Biol. 1998, 110, 359–366. [Google Scholar] [CrossRef]
- Gilpin, S.A.; Gilpin, C.J.; Dixon, J.S.; Gosling, J.A.; Kirby, R.S. The effect of age on the autonomic innervation of the urinary bladder. Br. J. Urol. 1986, 58, 378–381. [Google Scholar] [CrossRef]
- Erdem, N.; Chu, F.M. Management of overactive bladder and urge urinary incontinence in the elderly patient. Am. J. Med. 2006, 119, 29–36. [Google Scholar] [CrossRef]
- Drake, M.J.; Mills, I.W.; Gillespie, J.I. Model of peripheral autonomous modules and a myovesical plexus in normal and overactive bladder function. Lancet 2001, 358, 401–403. [Google Scholar] [CrossRef]
- Häbler, H.J.; Jänig, W.; Koltzenburg, M. Activation of unmyelinated afferent fibres by mechanical stimuli and inflammation of the urinary bladder in the cat. J. Physiol. 1990, 425, 545–562. [Google Scholar] [CrossRef] [Green Version]
- Morrison, J. The activation of bladder wall afferent nerves. Exp. Physiol. 1999, 84, 131–136. [Google Scholar] [CrossRef]
- Tennyson, L.E.; Tai, C.; Chermansky, C.J. Using the native afferent nervous system to sense bladder fullness: State of the art. Curr. Bladder Dysfunct. Rep. 2016, 11, 346–349. [Google Scholar] [CrossRef] [Green Version]
- Marshall, K.L.; Saade, D.; Ghitani, N.; Coombs, A.M.; Szczot, M.; Keller, J.; Ogata, T.; Daou, I.; Stowers, L.T.; Bönnemann, C.G.; et al. PIEZO2 in sensory neurons and urothelial cells coordinates urination. Nature 2020, 588, 290–295. [Google Scholar] [CrossRef]
- Dalghi, M.G.; Ruiz, W.G.; Clayton, D.R.; Montalbetti, N.; Daugherty, S.L.; Beckel, J.M.; Carattino, M.D.; Apodaca, G. Functional roles for PIEZO1 and PIEZO2 in urothelial mechanotransduction and lower urinary tract interoception. JCI Insight 2021, 6, e152984. [Google Scholar] [CrossRef]
- Ford, A.P.; Cockayne, D.A. ATP and P2X purinoceptors in urinary tract disorders. In Handbook of Experimental Pharmacology; Springer: Berlin/Heidelberg, Germany, 2011; pp. 485–526. [Google Scholar]
- Vlaskovska, M.; Kasakov, L.; Rong, W.; Bodin, P.; Bardini, M.; Cockayne, D.A.; Ford, A.P.; Burnstock, G. P2X3 knock-out mice reveal a major sensory role for urothelially released. ATP J. Neurosci. 2001, 21, 5670–5677. [Google Scholar] [CrossRef] [Green Version]
- Ferguson, A.C.; Sutton, B.W.; Boone, T.B.; Ford, A.P.; Munoz, A. Inhibition of urothelial P2X3 receptors prevents desensitization of purinergic detrusor contractions in the rat bladder. BJU Int. 2015, 116, 293–301. [Google Scholar] [CrossRef] [Green Version]
- Heppner, T.J.; Tykocki, N.R.; Hill-Eubanks, D.; Nelson, M.T. Transient contractions of urinary bladder smooth muscle are drivers of afferent nerve activity during filling. J. Gen. Physiol. 2016, 147, 323–335. [Google Scholar] [CrossRef] [Green Version]
- Barrington, F.J.F. The effect of lesions of the hind- and mid-brain on micturition in the cat. Q. J. Exp. Physiol. 1925, 15, 81–102. [Google Scholar] [CrossRef] [Green Version]
- Sasaki, M. Role of Barrington’s nucleus in micturition. J. Comp. Neurol. 2005, 493, 21–26. [Google Scholar] [CrossRef]
- Westlund, K.N.; Coulter, J.D. Descending projections of the locus coeruleus and subcoeruleus/medial parabrachial nuclei in monkey: Axonal transport studies and dopamine-β-hydroxylase immunocytochemistry. Brain Res. Rev. 1980, 2, 235–264. [Google Scholar] [CrossRef]
- Martin, G.F.; Humbertson, A.O., Jr.; Laxson, L.C.; Panneton, W.M.; Tschismadia, I. Spinal projections from the mesencephalic and pontine reticular formation in the north American opossum: A study using axonal transport techniques. J. Comp. Neurol. 1979, 187, 373–399. [Google Scholar] [CrossRef]
- Loewy, A.D.; Saper, C.B.; Baker, R.P. Descending projections from the pontine micturition center. Brain Res. 1979, 172, 533–538. [Google Scholar] [CrossRef]
- Holstege, G.; Kuypers, H.G.J.M.; Boer, R.C. Anatomical evidence for direct brain stem projections to the somatic motoneuronal cell groups and autonomic preganglionic cell groups in cat spinal cord. Brain Res. 1979, 171, 329–333. [Google Scholar] [CrossRef]
- Blok, B.F.M.; Holstege, G. Direct projections from the periaqueductal gray to the pontine micturition center (M-region). An anterograde and retrograde tracing study in the cat. Neurosci. Lett. 1994, 166, 93–96. [Google Scholar] [CrossRef]
- Verstegen, A.M.J.; Vanderhorst, V.; Gray, P.A.; Zeidel, M.L.; Geerling, J.C. Barrington’s nucleus: Neuroanatomic landscape of the mouse “pontine micturition center”. J. Comp. Neurol. 2017, 525, 2287–2309. [Google Scholar] [CrossRef]
- Verstegen, A.M.J.; Klymko, N.; Zhu, L.; Mathai, J.C.; Kobayashi, R.; Venner, A.; Ross, R.A.; VanderHorst, V.G.; Arrigoni, E.; Geerling, J.C.; et al. Non-crh glutamatergic neurons in barrington’s nucleus control micturition via glutamatergic afferents from the midbrain and hypothalamus. Curr. Biol. 2019, 29, 2775–2789.e2777. [Google Scholar] [CrossRef]
- Keller, J.A.; Chen, J.; Simpson, S.; Wang, E.H.-J.; Lilascharoen, V.; George, O.; Lim, B.K.; Stowers, L. Voluntary urination control by brainstem neurons that relax the urethral sphincter. Nat. Neurosci. 2018, 21, 1229–1238. [Google Scholar] [CrossRef]
- Hou, X.H.; Hyun, M.; Taranda, J.; Huang, K.W.; Todd, E.; Feng, D.; Atwater, E.; Croney, D.; Zeidel, M.L.; Osten, P. Central control circuit for context-dependent micturition. Cell 2016, 167, 73–86. [Google Scholar] [CrossRef] [Green Version]
- Griffiths, D.; Holstege, G.; Dalm, E.; Wall, H.D. Control and coordination of bladder and urethral function in the brainstem of the cat. Neurourol. Urodyn. 1990, 9, 63–82. [Google Scholar] [CrossRef]
- Van Batavia, J.P.; Butler, S.; Lewis, E.; Fesi, J.; Canning, D.A.; Vicini, S.; Valentino, R.J.; Zderic, S.A. Corticotropin-releasing hormone from the pontine micturition center plays an inhibitory role in micturition. J. Neurosci. 2021, 41, 7314–7325. [Google Scholar] [CrossRef]
- Siblerud, R.; Mutter, J.; Moore, E.; Naumann, J.; Walach, H. A hypothesis and evidence that mercury may be an etiological factor in Alzheimer’s disease. Int. J. Environ. Res. Public Health 2019, 16, 5152. [Google Scholar] [CrossRef] [Green Version]
- Tchounwou, P.B.; Ayensu, W.K.; Ninashvili, N.; Sutton, D. Review: Environmental exposure to mercury and its toxicopathologic implications for public health. Environ. Toxicol. 2003, 18, 149–175. [Google Scholar] [CrossRef]
- Sindhu, K.K.; Sutherling, W.W. Role of lead in the central nervous system: Effect on electroencephlography, evoked potentials, electroretinography, and nerve conduction. Neurodiagn. J. 2015, 55, 107–121. [Google Scholar] [CrossRef]
- Mason, L.H.; Harp, J.P.; Han, D.Y. Pb neurotoxicity: Neuropsychological effects of lead toxicity. Biomed. Res. Int. 2014, 2014, 840547. [Google Scholar] [CrossRef] [Green Version]
- Naughton, S.X.; Terry, A.V. Neurotoxicity in acute and repeated organophosphate exposure. Toxicology 2018, 408, 101–112. [Google Scholar] [CrossRef]
- Mochizuki, H. Arsenic neurotoxicity in humans. Int. J. Mol. Sci. 2019, 20, 3418. [Google Scholar] [CrossRef] [Green Version]
- Richardson, J.R.; Fitsanakis, V.; Westerink, R.H.S.; Kanthasamy, A.G. Neurotoxicity of pesticides. Acta Neuropathol. 2019, 138, 343–362. [Google Scholar] [CrossRef]
- Sethi, S.; Morgan, R.K.; Feng, W.; Lin, Y.; Li, X.; Luna, C.; Koch, M.; Bansal, R.; Duffel, M.W.; Puschner, B.; et al. Comparative analyses of the 12 most abundant PCB congeners detected in human maternal serum for activity at the thyroid hormone receptor and ryanodine receptor. Environ. Sci. Technol. 2019, 53, 3948–3958. [Google Scholar] [CrossRef] [Green Version]
- Rude, K.M.; Keogh, C.E.; Gareau, M.G. The role of the gut microbiome in mediating neurotoxic outcomes to PCB exposure. Neurotoxicology 2019, 75, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Galgano, S.J.; Sivils, C.; Selph, J.P.; Sanyal, R.; Lockhart, M.E.; Zarzour, J.G. The male urethra: Imaging and surgical approach for common pathologies. Curr. Probl. Diagn. Radiol. 2021, 50, 410–418. [Google Scholar] [CrossRef] [PubMed]
- Georgas, K.M.; Armstrong, J.; Keast, J.R.; Larkins, C.E.; McHugh, K.M.; Southard-Smith, E.M.; Cohn, M.J.; Batourina, E.; Dan, H.; Schneider, K.; et al. An illustrated anatomical ontology of the developing mouse lower urogenital tract. Development 2015, 142, 1893–1908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morales, O.; Romanus, R. Urethrography in the male: The boundaries of the different urethral parts and detail studies of the urethral mucous membrane and its motility. J. Urol. 1955, 73, 162–171. [Google Scholar] [CrossRef]
- Henry, G.H.; Malewska, A.; Joseph, D.B.; Malladi, V.S.; Lee, J.; Torrealba, J.; Mauck, R.J.; Gahan, J.C.; Raj, G.V.; Roehrborn, C.G.; et al. A cellular anatomy of the normal adult human prostate and prostatic urethra. Cell Rep. 2018, 25, 3530–3542.e3535. [Google Scholar] [CrossRef] [Green Version]
- Crowley, L.; Cambuli, F.; Aparicio, L.; Shibata, M.; Robinson, B.D.; Xuan, S.; Li, W.; Hibshoosh, H.; Loda, M.; Rabadan, R. A single-cell atlas of the mouse and human prostate reveals heterogeneity and conservation of epithelial progenitors. Elife 2020, 9, e59465. [Google Scholar] [CrossRef]
- Zhai, J.; Insel, M.; Addison, K.J.; Stern, D.A.; Pederson, W.; Dy, A.; Rojas-Quintero, J.; Owen, C.A.; Sherrill, D.L.; Morgan, W.; et al. Club cell secretory protein deficiency leads to altered lung function. Am. J. Respir. Crit. Care Med. 2019, 199, 302–312. [Google Scholar] [CrossRef]
- Rawlins, E.L.; Okubo, T.; Xue, Y.; Brass, D.M.; Auten, R.L.; Hasegawa, H.; Wang, F.; Hogan, B.L. The role of Scgb1a1+ Clara cells in the long-term maintenance and repair of lung airway, but not alveolar, epithelium. Cell Stem Cell 2009, 4, 525–534. [Google Scholar] [CrossRef] [Green Version]
- Hong, K.U.; Reynolds, S.D.; Giangreco, A.; Hurley, C.M.; Stripp, B.R. Clara cell secretory protein-expressing cells of the airway neuroepithelial body microenvironment include a label-retaining subset and are critical for epithelial renewal after progenitor cell depletion. Am. J. Respir. Cell Mol. Biol. 2001, 24, 671–681. [Google Scholar] [CrossRef] [Green Version]
- Montoro, D.T.; Haber, A.L.; Biton, M.; Vinarsky, V.; Lin, B.; Birket, S.E.; Yuan, F.; Chen, S.; Leung, H.M.; Villoria, J.; et al. A revised airway epithelial hierarchy includes CFTR-expressing ionocytes. Nature 2018, 560, 319–324. [Google Scholar] [CrossRef]
- Deprez, M.; Zaragosi, L.E.; Truchi, M.; Becavin, C.; Ruiz García, S.; Arguel, M.J.; Plaisant, M.; Magnone, V.; Lebrigand, K.; Abelanet, S.; et al. A single-cell atlas of the human healthy airways. Am. J. Respir. Crit. Care Med. 2020, 202, 1636–1645. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.; Ahn, H.K.; Huh, Y. Clinical and functional anatomy of the urethral sphincter. Int. Neurourol. J. 2012, 16, 102–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oelrich, T.M. The urethral sphincter muscle in the male. Am. J. Anat. 1980, 158, 229–246. [Google Scholar] [CrossRef] [Green Version]
- Nyangoh Timoh, K.; Moszkowicz, D.; Creze, M.; Zaitouna, M.; Felber, M.; Lebacle, C.; Diallo, D.; Martinovic, J.; Tewari, A.; Lavoué, V.; et al. The male external urethral sphincter is autonomically innervated. Clin. Anat. 2021, 34, 263–271. [Google Scholar] [CrossRef] [PubMed]
- McNeal, J.E. The zonal anatomy of the prostate. Prostate 1981, 2, 35–49. [Google Scholar] [CrossRef]
- Verze, P.; Cai, T.; Lorenzetti, S. The role of the prostate in male fertility, health and disease. Nat. Rev. Urol. 2016, 13, 379–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Medved, M.; Sammet, S.; Yousuf, A.; Oto, A. MR imaging of the prostate and adjacent anatomic structures before, during, and after ejaculation: Qualitative and quantitative evaluation. Radiology 2014, 271, 452–460. [Google Scholar] [CrossRef] [Green Version]
- Joseph, D.B.; Henry, G.H.; Malewska, A.; Reese, J.C.; Mauck, R.J.; Gahan, J.C.; Hutchinson, R.C.; Malladi, V.S.; Roehrborn, C.G.; Vezina, C.M.; et al. Single-cell analysis of mouse and human prostate reveals novel fibroblasts with specialized distribution and microenvironment interactions. J. Pathol. 2021, 255, 141–154. [Google Scholar] [CrossRef]
- McNeal, J.; Kindrachuk, R.; Freiha, F.; Bostwick, D.; Redwine, E.; Stamey, T. Patterns of progression in prostate cancer. Lancet 1986, 327, 60–63. [Google Scholar] [CrossRef]
- Frick, J.; Aulitzky, W. Physiology of the prostate. Infection 1991, 19, S115–S118. [Google Scholar] [CrossRef]
- Lee, C.H.; Akin-Olugbade, O.; Kirschenbaum, A. Overview of prostate anatomy, histology, and pathology. Endocrinol. Metab. Clin. N. Am. 2011, 40, 565–575. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.; Hu, K.; Nguyen, D.; Wang, Z.A. From genomics to functions: Preclinical mouse models for understanding oncogenic pathways in prostate cancer. Am. J. Cancer Res. 2019, 9, 2079–2102. [Google Scholar]
- Liu, T.T.; Thomas, S.; McLean, D.T.; Roldan-Alzate, A.; Hernando, D.; Ricke, E.A.; Ricke, W.A. Prostate enlargement and altered urinary function are part of the aging process. Aging 2019, 11, 2653–2669. [Google Scholar] [CrossRef]
- Huggins, C. The etiology of benign prostatic hypertrophy. Bull. N. Y. Acad. Med. 1947, 23, 696–704. [Google Scholar] [PubMed]
- Ittmann, M. Anatomy and histology of the human and murine prostate. Cold Spring Harb. Perspect. Med. 2018, 8, a030346. [Google Scholar] [CrossRef] [PubMed]
- Pattabiraman, G.; Bell-Cohn, A.J.; Murphy, S.F.; Mazur, D.J.; Schaeffer, A.J.; Thumbikat, P. Mast cell function in prostate inflammation, fibrosis, and smooth muscle cell dysfunction. Am. J. Physiol. Ren. Physiol. 2021, 321, F466–F479. [Google Scholar] [CrossRef] [PubMed]
- Thielen, J.L.; Volzing, K.G.; Collier, L.S.; Green, L.E.; Largaespada, D.A.; Marker, P.C. Markers of prostate region-specific epithelial identity define anatomical locations in the mouse prostate that are molecularly similar to human prostate cancers. Differentiation 2007, 75, 49–61. [Google Scholar] [CrossRef]
- Cunha, G.R.; Vezina, C.M.; Isaacson, D.; Ricke, W.A.; Timms, B.G.; Cao, M.; Franco, O.; Baskin, L.S. Development of the human prostate. Differentiation 2018, 103, 24–45. [Google Scholar] [CrossRef] [Green Version]
- Tubaro, A.; Mariani, S.; De Nunzio, C.; Miano, R. Bladder weight and detrusor thickness as parameters of progression of benign prostatic hyperplasia. Curr. Opin. Urol. 2010, 20, 37–42. [Google Scholar] [CrossRef]
- Kita, M.; Yunoki, T.; Takimoto, K.; Miyazato, M.; Kita, K.; de Groat, W.C.; Kakizaki, H.; Yoshimura, N. Effects of bladder outlet obstruction on properties of Ca2+-activated K+ channels in rat bladder. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2010, 298, R1310–R1319. [Google Scholar] [CrossRef] [Green Version]
- Sugaya, K.; de Goat, W.C. Excitatory and inhibitory influence of pathways in the pelvic nerve on bladder activity in rats with bladder outlet obstruction. LUTS Low. Urin. Tract Symptoms 2009, 1, 51–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gosling, J.A.; Kung, L.S.; Dixon, J.S.; Horan, P.; Whitbeck, C.; Levin, R.M. Correlation between the structure and function of the rabbit urinary bladder following partial outlet obstruction. J. Urol. 2000, 163, 1349–1356. [Google Scholar] [CrossRef]
- Kojima, M.; Inui, E.; Ochiai, A.; Naya, Y.; Kamoi, K.; Ukimura, O.; Watanabe, H. Reversible change of bladder hypertrophy due to benign prostatic hyperplasia after surgical relief of obstruction. J. Urol. 1997, 158, 89–93. [Google Scholar] [CrossRef] [PubMed]
- Tubaro, A.; Carter, S.; Hind, A.; Vicentini, C.; Miano, L. A prospective study of the safety and efficacy of suprapubic transvesical prostatectomy in patients with benign prostatic hyperplasia. J. Urol. 2001, 166, 172–176. [Google Scholar] [CrossRef]
- Fibbi, B.; Penna, G.; Morelli, A.; Adorini, L.; Maggi, M. Chronic inflammation in the pathogenesis of benign prostatic hyperplasia. Int. J. Androl. 2010, 33, 475–488. [Google Scholar] [CrossRef]
- Bierhoff, E.; Vogel, J.; Benz, M.; Giefer, T.; Wernert, N.; Pfeifer, U. Stromal nodules in benign prostatic hyperplasia. Eur. Urol. 1996, 29, 345–354. [Google Scholar] [CrossRef]
- Meigs, J.B.; Mohr, B.; Barry, M.J.; Collins, M.M.; McKinlay, J.B. Risk factors for clinical benign prostatic hyperplasia in a community-based population of healthy aging men. J. Clin. Epidemiol. 2001, 54, 935–944. [Google Scholar] [CrossRef]
- Michel, M.C.; Mehlburger, L.; Schumacher, H.; Bressel, H.U.; Goepel, M. Effect of diabetes on lower urinary tract symptoms in patients with benign prostatic hyperplasia. J. Urol. 2000, 163, 1725–1729. [Google Scholar] [CrossRef]
- Verhamme, K.M.; Dieleman, J.P.; Bleumink, G.S.; van der Lei, J.; Sturkenboom, M.C.; Artibani, W.; Begaud, B.; Berges, R.; Borkowski, A.; Chappel, C.R.; et al. Incidence and prevalence of lower urinary tract symptoms suggestive of benign prostatic hyperplasia in primary care—The Triumph project. Eur. Urol. 2002, 42, 323–328. [Google Scholar] [CrossRef]
- McNeal, J. Pathology of benign prostatic hyperplasia. Insight into etiology. Urol. Clin. N. Am. 1990, 17, 477–486. [Google Scholar] [CrossRef]
- Vermeulen, A. Decreased androgen levels and obesity in men. Ann. Med. 1996, 28, 13–15. [Google Scholar] [CrossRef] [PubMed]
- Krieg, M.; Nass, R.; Tunn, S. Effect of aging on endogenous level of 5 alpha-dihydrotestosterone, testosterone, estradiol, and estrone in epithelium and stroma of normal and hyperplastic human prostate. J. Clin. Endocrinol. Metab. 1993, 77, 375–381. [Google Scholar] [PubMed] [Green Version]
- Nicholson, T.M.; Ricke, E.A.; Marker, P.C.; Miano, J.M.; Mayer, R.D.; Timms, B.G.; vom Saal, F.S.; Wood, R.W.; Ricke, W.A. Testosterone and 17β-estradiol induce glandular prostatic growth, bladder outlet obstruction, and voiding dysfunction in male mice. Endocrinology 2012, 153, 5556–5565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belanger, A.; Candas, B.; Dupont, A.; Cusan, L.; Diamond, P.; Gomez, J.L.; Labrie, F. Changes in serum concentrations of conjugated and unconjugated steroids in 40- to 80-year-old men. J. Clin. Endocrinol. Metab. 1994, 79, 1086–1090. [Google Scholar] [PubMed]
- Schatzl, G.; Brossner, C.; Schmid, S.; Kugler, W.; Roehrich, M.; Treu, T.; Szalay, A.; Djavan, B.; Schmidbauer, C.P.; Soregi, S.; et al. Endocrine status in elderly men with lower urinary tract symptoms: Correlation of age, hormonal status, and lower urinary tract function. The prostate study group of the Austrian society of urology. Urology 2000, 55, 397–402. [Google Scholar] [CrossRef]
- Byron, J.K.; Taylor, K.H.; Phillips, G.S.; Stahl, M.S. Urethral sphincter mechanism incompetence in 163 neutered female dogs: Diagnosis, treatment, and relationship of weight and age at neuter to development of disease. J. Vet. Intern. Med. 2017, 31, 442–448. [Google Scholar] [CrossRef] [Green Version]
- Bernoulli, J.; Yatkin, E.; Konkol, Y.; Talvitie, E.M.; Santti, R.; Streng, T. Prostatic inflammation and obstructive voiding in the adult Noble rat: Impact of the testosterone to estradiol ratio in serum. Prostate 2008, 68, 1296–1306. [Google Scholar] [CrossRef]
- Streng, T.; Lehtoranta, M.; Poutanen, M.; Talo, A.; Lammintausta, R.; Santti, R. Developmental, estrogen induced infravesical obstruction is reversible in adult male rodents. J. Urol. 2002, 168, 2263–2268. [Google Scholar] [CrossRef]
- Streng, T.K.; Talo, A.; Andersson, K.E.; Santti, R. A dose-dependent dual effect of oestrogen on voiding in the male mouse? BJU Int. 2005, 96, 1126–1130. [Google Scholar] [CrossRef]
- Walsh, P.C.; Wilson, J.D. The induction of prostatic hypertrophy in the dog with androstanediol. J. Clin. Investig. 1976, 57, 1093–1097. [Google Scholar] [CrossRef] [Green Version]
- Jeyaraj, D.A.; Udayakumar, T.S.; Rajalakshmi, M.; Pal, P.C.; Sharma, R.S. Effects of long-term administration of androgens and estrogen on rhesus monkey prostate: Possible induction of benign prostatic hyperplasia. J. Androl. 2000, 21, 833–841. [Google Scholar] [PubMed]
- Tam, N.N.; Zhang, X.; Xiao, H.; Song, D.; Levin, L.; Meller, J.; Ho, S.M. Increased susceptibility of estrogen-induced bladder outlet obstruction in a novel mouse model. Lab. Investig. 2015, 95, 546–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shenfeld, O.Z.; McCammon, K.A.; Blackmore, P.F.; Ratz, P.H. Rapid effects of estrogen and progesterone on tone and spontaneous rhythmic contractions of the rabbit bladder. Urol. Res. 1999, 27, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Yasay, G.D.; Kau, S.T.; Li, J.H. Mechanoinhibitory effect of estradiol in guinea pig urinary bladder smooth muscles. Pharmacology 1995, 51, 273–280. [Google Scholar] [CrossRef]
- Zhang, J.; Hess, M.W.; Thurnher, M.; Hobisch, A.; Radmayr, C.; Cronauer, M.V.; Hittmair, A.; Culig, Z.; Bartsch, G.; Klocker, H. Human prostatic smooth muscle cells in culture: Estradiol enhances expression of smooth muscle cell-specific markers. Prostate 1997, 30, 117–129. [Google Scholar] [CrossRef]
- Scarano, W.R.; Cordeiro, R.S.; Goes, R.M.; Carvalho, H.F.; Taboga, S.R. Tissue remodeling in Guinea pig lateral prostate at different ages after estradiol treatment. Cell Biol. Int. 2005, 29, 778–784. [Google Scholar] [CrossRef]
- Holterhus, P.M.; Zhao, G.Q.; Aumuller, G. Effects of androgen deprivation and estrogen treatment on the structure and protein expression of the rat coagulating gland. Anat. Rec. 1993, 235, 223–232. [Google Scholar] [CrossRef]
- Tam, C.C.; Wong, Y.C. Ultrastructural study of the effects of 17 beta-oestradiol on the lateral prostate and seminal vesicle of the castrated guinea pig. Acta Anat. 1991, 141, 51–62. [Google Scholar]
- Nicholson, T.M.; Nguyen, J.L.; Leverson, G.E.; Taylor, J.A.; Vom Saal, F.S.; Wood, R.W.; Ricke, W.A. Endocrine disruptor bisphenol A is implicated in urinary voiding dysfunction in male mice. Am. J. Physiol. Ren. Physiol. 2018, 315, F1208–F1216. [Google Scholar] [CrossRef]
- Makowska, K.; Lech, P.; Majewski, M.; Rychlik, A.; Gonkowski, S. Bisphenol A affects vipergic nervous structures in the porcine urinary bladder trigone. Sci. Rep. 2021, 11, 12147. [Google Scholar] [CrossRef]
- Bushman, W.A.; Jerde, T.J. The role of prostate inflammation and fibrosis in lower urinary tract symptoms. Am. J. Physiol. Ren. Physiol. 2016, 311, F817–F821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.; Yang, G.; Bushman, W. Prostatic inflammation induces urinary frequency in adult mice. PLoS ONE 2015, 10, e0116827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lloyd, G.L.; Ricke, W.A.; McVary, K.T. Inflammation, voiding and benign prostatic hyperplasia progression. J. Urol. 2019, 201, 868–870. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, S.A.; Roehrborn, C.G.; McConnell, J.D.; Meehan, A.G.; Surynawanshi, S.; Lee, J.Y.; Rotonda, J.; Kusek, J.W.; Nyberg, L.M., Jr. Long-term treatment with finasteride results in a clinically significant reduction in total prostate volume compared to placebo over the full range of baseline prostate sizes in men enrolled in the MTOPS trial. J. Urol. 2008, 180, 1030–1032. [Google Scholar] [CrossRef] [PubMed]
- St Sauver, J.L.; Jacobson, D.J.; McGree, M.E.; Girman, C.J.; Lieber, M.M.; Jacobsen, S.J. Longitudinal association between prostatitis and development of benign prostatic hyperplasia. Urology 2008, 71, 475–479. [Google Scholar] [CrossRef] [Green Version]
- Penna, G.; Fibbi, B.; Amuchastegui, S.; Cossetti, C.; Aquilano, F.; Laverny, G.; Gacci, M.; Crescioli, C.; Maggi, M.; Adorini, L. Human benign prostatic hyperplasia stromal cells as inducers and targets of chronic immuno-mediated inflammation. J. Immunol. 2009, 182, 4056–4064. [Google Scholar] [CrossRef]
- Doiron, R.C.; Shoskes, D.A.; Nickel, J.C. Male cp/cpps: Where do we stand? World J. Urol. 2019, 37, 1015–1022. [Google Scholar] [CrossRef]
- Roberts, R.O.; Lieber, M.M.; Bostwick, D.G.; Jacobsen, S.J. A review of clinical and pathological prostatitis syndromes. Urology 1997, 49, 809–821. [Google Scholar] [CrossRef]
- Cantiello, F.; Cicione, A.; Salonia, A.; Autorino, R.; Tucci, L.; Madeo, I.; Damiano, R. Periurethral fibrosis secondary to prostatic inflammation causing lower urinary tract symptoms: A prospective cohort study. Urology 2013, 81, 1018–1024. [Google Scholar] [CrossRef]
- Macoska, J. Prostatic fibrosis is associated with lower urinary tract symptoms. J. Urol. 2012, 188, 1375–1381. [Google Scholar] [CrossRef] [Green Version]
- Macoska, J.A.; Uchtmann, K.S.; Leverson, G.E.; McVary, K.T.; Ricke, W.A. Prostate transition zone fibrosis is associated with clinical progression in the MTOPS study. J. Urol. 2019, 202, 1240–1247. [Google Scholar] [CrossRef] [PubMed]
- Ruetten, H.; Wegner, K.A.; Romero, M.F.; Wood, M.W.; Marker, P.C.; Strand, D.; Colopy, S.A.; Vezina, C.M. Prostatic collagen architecture in neutered and intact canines. Prostate 2018, 78, 839–848. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Yang, G.; Mulligan, W.; Gipp, J.; Bushman, W. Ventral prostate fibrosis in the Akita mouse is associated with macrophage and fibrocyte infiltration. J. Diabetes Res. 2014, 2014, 939053. [Google Scholar] [CrossRef] [PubMed]
- Gharaee-Kermani, M.; Rodriguez-Nieves, J.A.; Mehra, R.; Vezina, C.A.; Sarma, A.V.; Macoska, J.A. Obesity-induced diabetes and lower urinary tract fibrosis promote urinary voiding dysfunction in a mouse model. Prostate 2013, 73, 1123–1133. [Google Scholar] [CrossRef] [Green Version]
- Baumgarten, H.G.; Falck, B.; Holstein, A.F.; Owman, C.; Owman, T. Adrenergic innervation of the human testis, epididymis, ductus deferens and prostate: A fluorescence microscopic and fluorimetric study. Z. Zellforsch. Und Mikrosk. Anat. 1968, 90, 81–95. [Google Scholar] [CrossRef]
- Caine, M.; Raz, S.; Zeigler, M. Adrenergic and cholinergic receptors in the human prostate, prostatic capsule and bladder neck. Br. J. Urol. 1975, 47, 193–202. [Google Scholar] [CrossRef]
- Raz, S.; Zeigler, M.; Caine, M. Pharmacological receptors in the prostate. Br. J. Urol. 1973, 45, 663–667. [Google Scholar] [CrossRef]
- Ricke, W.A.; Lee, C.W.; Clapper, T.R.; Schneider, A.J.; Moore, R.W.; Keil, K.P.; Abler, L.L.; Wynder, J.L.; Lopez Alvarado, A.; Beaubrun, I.; et al. In Utero and lactational TCDD exposure increases susceptibility to lower urinary tract dysfunction in adulthood. Toxicol. Sci. 2016, 150, 429–440. [Google Scholar] [CrossRef] [Green Version]
- Turco, A.E.; Oakes, S.R.; Keil Stietz, K.P.; Dunham, C.L.; Joseph, D.B.; Chathurvedula, T.S.; Girardi, N.M.; Schneider, A.J.; Gawdzik, J.; Sheftel, C.M.; et al. A mechanism linking perinatal 2,3,7,8 tetrachlorodibenzo-p-dioxin exposure to lower urinary tract dysfunction in adulthood. Dis. Models Mech. 2021, 14, dmm049068. [Google Scholar] [CrossRef]
- Gupta, A.; Ketchum, N.; Roehrborn, C.G.; Schecter, A.; Aragaki, C.C.; Michalek, J.E. Serum dioxin, testosterone, and subsequent risk of benign prostatic hyperplasia: A prospective cohort study of Air Force veterans. Environ. Health Perspect. 2006, 114, 1649–1654. [Google Scholar] [CrossRef]
- Gupta, A.; Gupta, S.; Pavuk, M.; Roehrborn, C.G. Anthropometric and metabolic factors and risk of benign prostatic hyperplasia: A prospective cohort study of Air Force veterans. Urology 2006, 68, 1198–1205. [Google Scholar] [CrossRef]
- Steers, W.D. Pathophysiology of overactive bladder and urge urinary incontinence. Rev. Urol. 2002, 4, S7. [Google Scholar] [PubMed]
- De Nunzio, C.; Presicce, F.; Lombardo, R.; Carter, S.; Vicentini, C.; Tubaro, A. Detrusor overactivity increases bladder wall thickness in male patients: A urodynamic multicenter cohort study. Neurourol. Urodyn. 2017, 36, 1616–1621. [Google Scholar] [CrossRef] [PubMed]
- Mumtaz, M.M.; Farooqui, M.Y.; Ghanayem, B.I.; Ahmed, A.E. The urotoxic effects of N,N′-dimethylaminopropionitrile. In vivo and in vitro metabolism. Toxicol. Appl. Pharmacol. 1991, 110, 61–69. [Google Scholar] [CrossRef]
- Hara, N.; Saito, H.; Takahashi, K.; Takeda, M. Lower urinary tract symptoms in patients with Niigata Minamata disease: A case-control study 50 years after methyl mercury pollution. Int. J. Urol. 2013, 20, 610–615. [Google Scholar] [CrossRef]
- Eto, K. Pathology of Minamata disease. Toxicol. Pathol. 1997, 25, 614–623. [Google Scholar] [CrossRef] [Green Version]
- Smith, R.A.; Christenson, W.R.; Bartels, M.J.; Arnold, L.L.; St John, M.K.; Cano, M.; Garland, E.M.; Lake, S.G.; Wahle, B.S.; McNett, D.A.; et al. Urinary physiologic and chemical metabolic effects on the urothelial cytotoxicity and potential DNA adducts of o-phenylphenol in male rats. Toxicol. Appl. Pharmacol. 1998, 150, 402–413. [Google Scholar] [CrossRef]
- Abrams, P.; Cardozo, L.; Fall, M.; Griffiths, D.; Rosier, P.; Ulmsten, U.; Van Kerrebroeck, P.; Victor, A.; Wein, A. The standardisation of terminology of lower urinary tract function: Report from the Standardisation Sub-committee of the International Continence Society. Am. J. Obstet. Gynecol. 2002, 187, 116–126. [Google Scholar] [CrossRef] [Green Version]
- Miyazato, M.; Yoshimura, N.; Chancellor, M.B. The other bladder syndrome: Underactive bladder. Rev. Urol. 2013, 15, 11–22. [Google Scholar]
- Kim, S.J.; Kim, J.; Na, Y.G.; Kim, K.H. Irreversible bladder remodeling induced by fibrosis. Int. Neurourol. J. 2021, 25, S3–S7. [Google Scholar] [CrossRef]
- Feng, J.; Gao, J.; Zhou, S.; Liu, Y.; Zhong, Y.; Shu, Y.; Meng, M.S.; Yan, J.; Sun, D.; Fang, Q.; et al. Role of stem cell factor in the regulation of ICC proliferation and detrusor contraction in rats with an underactive bladder. Mol. Med. Rep. 2017, 16, 1516–1522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castro-Diaz, D.; Taracena Lafuente, J.M. Detrusor-sphincter dyssynergia. Int. J. Clin. Pract. Suppl. 2006, 151, 17–21. [Google Scholar] [CrossRef]
- Stoffel, J.T. Detrusor sphincter dyssynergia: A review of physiology, diagnosis, and treatment strategies. Transl. Androl. Urol. 2016, 5, 127–135. [Google Scholar] [PubMed]
- Amarenco, G.; Sheikh Ismaël, S.; Chesnel, C.; Charlanes, A.; Le Breton, F. Diagnosis and clinical evaluation of neurogenic bladder. Eur. J. Phys. Rehabil. Med. 2017, 53, 975–980. [Google Scholar] [CrossRef] [PubMed]
- Ito, H.; Yoshiyasu, T.; Yamaguchi, O.; Yokoyama, O. Male lower urinary tract symptoms: Hypertension as a risk factor for storage symptoms, but not voiding symptoms. Lower Urin. Tract Symptoms 2012, 4, 68–72. [Google Scholar] [CrossRef]
- Wang, X.; Su, Y.; Yang, C.; Hu, Y.; Dong, J.-Y. Benign prostatic hyperplasia and cardiovascular risk: A prospective study among chinese men. World J. Urol. 2021, 40, 177–183. [Google Scholar] [CrossRef]
- Hammarsten, J.; Högstedt, B. Clinical, anthropometric, metabolic and insulin profile of men with fast annual growth rates of benign prostatic hyperplasia. Blood Press. 1999, 8, 29–36. [Google Scholar]
- Abler, L.L.; Vezina, C.M. Links between lower urinary tract symptoms, intermittent hypoxia and diabetes: Causes or cures? Respir. Physiol. Neurobiol. 2018, 256, 87–96. [Google Scholar] [CrossRef]
- Lejay, A.; Fang, F.; John, R.; Van, J.A.D.; Barr, M.; Thaveau, F.; Chakfe, N.; Geny, B.; Scholey, J.W. Ischemia reperfusion injury, ischemic conditioning and diabetes mellitus. J. Mol. Cell. Cardiol. 2016, 91, 11–22. [Google Scholar] [CrossRef]
- Vinik, A.I.; Maser, R.E.; Mitchell, B.D.; Freeman, R. Diabetic autonomic neuropathy. Diabetes Care 2003, 26, 1553–1579. [Google Scholar] [CrossRef] [Green Version]
- Morgan, B.J. Vascular consequences of intermittent hypoxia. In Hypoxia and the Circulation; Springer: Berlin/Heidelberg, Germany, 2007; pp. 69–84. [Google Scholar]
- Andersson, K.E.; Boedtkjer, D.B.; Forman, A. The link between vascular dysfunction, bladder ischemia, and aging bladder dysfunction. Ther. Adv. Urol. 2017, 9, 11–27. [Google Scholar] [CrossRef] [PubMed]
- Lind, L.; Lind, P.M. Can persistent organic pollutants and plastic-associated chemicals cause cardiovascular disease? J. Int. Med. 2012, 271, 537–553. [Google Scholar] [CrossRef] [Green Version]
- Meneguzzi, A.; Fava, C.; Castelli, M.; Minuz, P. Exposure to perfluoroalkyl chemicals and cardiovascular disease: Experimental and epidemiological evidence. Front. Endocrinol. 2021, 12, 850. [Google Scholar] [CrossRef] [PubMed]
- Velmurugan, G.; Ramprasath, T.; Gilles, M.; Swaminathan, K.; Ramasamy, S. Gut microbiota, endocrine-disrupting chemicals, and the diabetes epidemic. Trends Endocrinol. Metab. 2017, 28, 612–625. [Google Scholar] [CrossRef] [PubMed]
- Muller, W.J.; Lee, F.S.; Dickson, C.; Peters, G.; Pattengale, P.; Leder, P. The int-2 gene product acts as an epithelial growth factor in transgenic mice. EMBO J. 1990, 9, 907–913. [Google Scholar] [CrossRef]
- Konno-Takahashi, N.; Takeuchi, T.; Nishimatsu, H.; Kamijo, T.; Tomita, K.; Schalken, J.A.; Teshima, S.; Kitamura, T. Engineered FGF-2 expression induces glandular epithelial hyperplasia in the murine prostatic dorsal lobe. Eur. Urol. 2004, 46, 126–132. [Google Scholar] [CrossRef]
- Tutrone, R.F., Jr.; Ball, R.A.; Ornitz, D.M.; Leder, P.; Richie, J.P. Benign prostatic hyperplasia in a transgenic mouse: A new hormonally sensitive investigatory model. J. Urol. 1993, 149, 633–639. [Google Scholar] [CrossRef]
- Wennbo, H.; Kindblom, J.; Isaksson, O.G.; Törnell, J. Transgenic mice overexpressing the prolactin gene develop dramatic enlargement of the prostate gland. Endocrinology 1997, 138, 4410–4415. [Google Scholar] [CrossRef]
- Pigat, N.; Reyes-Gomez, E.; Boutillon, F.; Palea, S.; Barry Delongchamps, N.; Koch, E.; Goffin, V. Combined sabal and urtica extracts (WS((R)) 1541) exert anti-proliferative and anti-inflammatory effects in a mouse model of benign prostate hyperplasia. Front. Pharmacol. 2019, 10, 311. [Google Scholar] [CrossRef]
- Bernichtein, S.; Pigat, N.; Camparo, P.; Latil, A.; Viltard, M.; Friedlander, G.; Goffin, V. Anti-inflammatory properties of lipidosterolic extract of serenoa repens (Permixon(R)) in a mouse model of prostate hyperplasia. Prostate 2015, 75, 706–722. [Google Scholar] [CrossRef]
- Dillner, K.; Kindblom, J.; Flores-Morales, A.; Pang, S.T.; Tornell, J.; Wennbo, H.; Norstedt, G. Molecular characterization of prostate hyperplasia in prolactin-transgenic mice by using cDNA representational difference analysis. Prostate 2002, 52, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Vital, P.; Castro, P.; Tsang, S.; Ittmann, M. The senescence-associated secretory phenotype promotes benign prostatic hyperplasia. Am. J. Pathol. 2014, 184, 721–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- George, J.W.; Patterson, A.L.; Tanwar, P.S.; Kajdacsy-Balla, A.; Prins, G.S.; Teixeira, J.M. Specific deletion of LKB1/Stk11 in the Mullerian duct mesenchyme drives hyperplasia of the periurethral stroma and tumorigenesis in male mice. Proc. Natl. Acad. Sci. USA 2017, 114, 3445–3450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wegner, K.A.; Mueller, B.R.; Unterberger, C.J.; Avila, E.J.; Ruetten, H.; Turco, A.E.; Oakes, S.R.; Girardi, N.M.; Halberg, R.B.; Swanson, S.M.; et al. Prostate epithelial-specific expression of activated PI3K drives stromal collagen production and accumulation. J. Pathol. 2020, 250, 231–242. [Google Scholar] [CrossRef]
- Turkbey, B.; Huang, R.; Vourganti, S.; Trivedi, H.; Bernardo, M.; Yan, P.; Benjamin, C.; Pinto, P.A.; Choyke, P.L. Age-related changes in prostate zonal volumes as measured by high-resolution magnetic resonance imaging (MRI): A cross-sectional study in over 500 patients. BJU Int. 2012, 110, 1642–1647. [Google Scholar] [CrossRef] [Green Version]
- Nickel, J.C.; Roehrborn, C.G.; O’Leary, M.P.; Bostwick, D.G.; Somerville, M.C.; Rittmaster, R.S. The relationship between prostate inflammation and lower urinary tract symptoms: Examination of baseline data from the REDUCE trial. Eur. Urol. 2008, 54, 1379–1384. [Google Scholar] [CrossRef] [Green Version]
- Nickel, J.C. Prostatitis. Can. Urol. Assoc. J. 2011, 5, 306–315. [Google Scholar] [CrossRef]
- Aiello, S.E.; Moses, M.A.; Allen, D.G. The Merck Veterinary Manual, 11th ed.; Merck & Co. Inc.: Kenilworth, NJ, USA, 2016; p. 3325. [Google Scholar]
- Krieger, J.N.; Riley, D.E. Bacteria in the chronic prostatitis-chronic pelvic pain syndrome: Molecular approaches to critical research questions. J. Urol. 2002, 167, 2574–2583. [Google Scholar] [CrossRef]
- Elkahwaji, J.E.; Ott, C.J.; Janda, L.M.; Hopkins, W.J. Mouse model for acute bacterial prostatitis in genetically distinct inbred strains. Urology 2005, 66, 883–887. [Google Scholar] [CrossRef]
- Rudick, C.N.; Berry, R.E.; Johnson, J.R.; Johnston, B.; Klumpp, D.J.; Schaeffer, A.J.; Thumbikat, P. Uropathogenic Escherichia coli induces chronic pelvic pain. Infect. Immun. 2011, 79, 628–635. [Google Scholar] [CrossRef] [Green Version]
- Nowicki, B.; Singhal, J.; Fang, L.; Nowicki, S.; Yallampalli, C. Inverse relationship between severity of experimental pyelonephritis and nitric oxide production in C3H/HeJ mice. Infect. Immun. 1999, 67, 2421–2427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruetten, H.; Sandhu, J.; Mueller, B.; Wang, P.; Zhang, H.L.; Wegner, K.A.; Cadena, M.; Sandhu, S.; Abler, L.L.; Zhu, J.; et al. A uropathogenic E. coli UTI89 model of prostatic inflammation and collagen accumulation for use in studying aberrant collagen production in the prostate. Am. J. Physiol. Ren. Physiol. 2021, 320, F31–F46. [Google Scholar] [CrossRef] [PubMed]
- Bell-Cohn, A.; Mazur, D.J.; Hall, C.C.; Schaeffer, A.J.; Thumbikat, P. Uropathogenic Escherichia coli-induced fibrosis, leading to lower urinary tract symptoms, is associated with type-2 cytokine signaling. Am. J. Physiol. Ren. Physiol. 2019, 316, F682–F692. [Google Scholar] [CrossRef]
- Wang, H.H.; Wang, L.; Jerde, T.J.; Chan, B.D.; Savran, C.A.; Burcham, G.N.; Crist, S.; Ratliff, T.L. Characterization of autoimmune inflammation induced prostate stem cell expansion. Prostate 2015, 75, 1620–1631. [Google Scholar] [CrossRef] [PubMed]
- Motrich, R.D.; Maccioni, M.; Molina, R.; Tissera, A.; Olmedo, J.; Riera, C.M.; Rivero, V.E. Presence of INFgamma-secreting lymphocytes specific to prostate antigens in a group of chronic prostatitis patients. Clin. Immunol. 2005, 116, 149–157. [Google Scholar] [CrossRef]
- Habermacher, G.M.; Chason, J.T.; Schaeffer, A.J. Prostatitis/chronic pelvic pain syndrome. Annu. Rev. Med. 2006, 57, 195–206. [Google Scholar] [CrossRef]
- Lees, J.R.; Charbonneau, B.; Hayball, J.D.; Diener, K.; Brown, M.; Matusik, R.; Cohen, M.B.; Ratliff, T.L. T-cell recognition of a prostate specific antigen is not sufficient to induce prostate tissue destruction. Prostate 2006, 66, 578–590. [Google Scholar] [CrossRef]
- Lees, J.R.; Charbonneau, B.; Swanson, A.K.; Jensen, R.; Zhang, J.; Matusik, R.; Ratliff, T.L. Deletion is neither sufficient nor necessary for the induction of peripheral tolerance in mature CD8+ T cells. Immunology 2006, 117, 248–261. [Google Scholar] [CrossRef]
- Done, J.D.; Rudick, C.N.; Quick, M.L.; Schaeffer, A.J.; Thumbikat, P. Role of mast cells in male chronic pelvic pain. J. Urol. 2012, 187, 1473–1482. [Google Scholar] [CrossRef] [Green Version]
- Rudick, C.N.; Schaeffer, A.J.; Thumbikat, P. Experimental autoimmune prostatitis induces chronic pelvic pain. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2008, 294, R1268–R1275. [Google Scholar] [CrossRef] [Green Version]
- Lang, M.D.; Nickel, J.C.; Olson, M.E.; Howard, S.R.; Ceri, H. Rat model of experimentally induced abacterial prostatitis. Prostate 2000, 45, 201–206. [Google Scholar] [CrossRef]
- Funahashi, Y.; O’Malley, K.J.; Kawamorita, N.; Tyagi, P.; DeFranco, D.B.; Takahashi, R.; Gotoh, M.; Wang, Z.; Yoshimura, N. Upregulation of androgen-responsive genes and transforming growth factor-β1 cascade genes in a rat model of non-bacterial prostatic inflammation. Prostate 2014, 74, 337–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mizoguchi, S.; Mori, K.; Wang, Z.; Liu, T.; Funahashi, Y.; Sato, F.; DeFranco, D.B.; Yoshimura, N.; Mimata, H. Effects of estrogen receptor β stimulation in a rat model of non-bacterial prostatic inflammation. Prostate 2017, 77, 803–811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Funahashi, Y.; Wang, Z.; O’Malley, K.J.; Tyagi, P.; DeFranco, D.B.; Gingrich, J.R.; Takahashi, R.; Majima, T.; Gotoh, M.; Yoshimura, N. Influence of E. coli-induced prostatic inflammation on expression of androgen-responsive genes and transforming growth factor beta 1 cascade genes in rats. Prostate 2015, 75, 381–389. [Google Scholar] [CrossRef] [Green Version]
- Torkko, K.C.; Wilson, R.S.; Smith, E.E.; Kusek, J.W.; van Bokhoven, A.; Lucia, M.S. Prostate biopsy markers of inflammation are associated with risk of clinical progression of benign prostatic hyperplasia: Finding for the MTOPS study. J. Urol. 2015, 194, 454–461. [Google Scholar] [CrossRef]
- Pontari, M.A.; Ruggieri, M.R. Mechanisms in prostatitis/chronic pelvic pain syndrome. J. Urol. 2004, 172, 839–845. [Google Scholar] [CrossRef] [Green Version]
- Nadler, R.B.; Koch, A.E.; Calhoun, E.A.; Campbell, P.L.; Pruden, D.L.; Bennett, C.L.; Yarnold, P.R.; Schaeffer, A.J. IL-1beta and TNF-alpha in prostatic secretions are indicators in the evaluation of men with chronic prostatitis. J. Urol. 2000, 164, 214–218. [Google Scholar] [CrossRef]
- Huang, T.R.; Li, W.; Peng, B. Correlation of inflammatory mediators in prostatic secretion with chronic prostatitis and chronic pelvic pain syndrome. Andrologia 2018, 50, e12860. [Google Scholar] [CrossRef]
- Ricote, M.; García-Tuñón, I.; Bethencourt, F.R.; Fraile, B.; Paniagua, R.; Royuela, M. Interleukin-1 (IL-1alpha and IL-1beta) and its receptors (IL-1RI, IL-1RII, and IL-1Ra) in prostate carcinoma. Cancer 2004, 100, 1388–1396. [Google Scholar] [CrossRef]
- Ashok, A.; Keener, R.; Rubenstein, M.; Stookey, S.; Bajpai, S.; Hicks, J.; Alme, A.K.; Drake, C.G.; Zheng, Q.; Trabzonlu, L.; et al. Consequences of interleukin 1β-triggered chronic inflammation in the mouse prostate gland: Altered architecture associated with prolonged CD4(+) infiltration mimics human proliferative inflammatory atrophy. Prostate 2019, 79, 732–745. [Google Scholar] [CrossRef]
- Hao, L.; Thomas, S.; Greer, T.; Vezina, C.M.; Bajpai, S.; Ashok, A.; De Marzo, A.M.; Bieberich, C.J.; Li, L.; Ricke, W.A. Quantitative proteomic analysis of a genetically induced prostate inflammation mouse model via custom 4-plex DiLeu isobaric labeling. Am. J. Physiol. Ren. Physiol. 2019, 316, F1236–F1243. [Google Scholar] [CrossRef]
- Hao, L.; Shi, Y.; Thomas, S.; Vezina, C.M.; Bajpai, S.; Ashok, A.; Bieberich, C.J.; Ricke, W.A.; Li, L. Comprehensive urinary metabolomic characterization of a genetically induced mouse model of prostatic inflammation. Int. J. Mass Spectrom. 2018, 434, 185–192. [Google Scholar] [CrossRef] [PubMed]
- O’Malley, K.J.; Eisermann, K.; Pascal, L.E.; Parwani, A.V.; Majima, T.; Graham, L.; Hrebinko, K.; Acquafondata, M.; Stewart, N.A.; Nelson, J.B.; et al. Proteomic analysis of patient tissue reveals PSA protein in the stroma of benign prostatic hyperplasia. Prostate 2014, 74, 892–900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pascal, L.E.; Mizoguchi, S.; Chen, W.; Rigatti, L.H.; Igarashi, T.; Dhir, R.; Tyagi, P.; Wu, Z.; Yang, Z.; de Groat, W.C.; et al. Prostate-specific deletion of cdh1 induces murine prostatic inflammation and bladder overactivity. Endocrinology 2021, 162, bqaa212. [Google Scholar] [CrossRef]
- Eljamal, K.; Kajioka, S.; Maki, T.; Ushijima, M.; Kawagoe, K.; Lee, K.; Sasaguri, T. New mouse model of underactive bladder developed by placement of a metal ring around the bladder neck. Lower Urin. Tract Symptoms 2021, 13, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Austin, J.C.; Chacko, S.K.; DiSanto, M.; Canning, D.A.; Zderic, S.A. A male murine model of partial bladder outlet obstruction reveals changes in detrusor morphology, contractility and Myosin isoform expression. J. Urol. 2004, 172, 1524–1528. [Google Scholar] [CrossRef]
- Taylor, J.A.; Zhu, Q.; Irwin, B.; Maghaydah, Y.; Tsimikas, J.; Pilbeam, C.; Leng, L.; Bucala, R.; Kuchel, G.A. Null mutation in macrophage migration inhibitory factor prevents muscle cell loss and fibrosis in partial bladder outlet obstruction. Am. J. Physiol. Ren. Physiol. 2006, 291, F1343–F1353. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Drzewiecki, B.A.; Merryman, W.D.; Pope, J.C. Murine bladder wall biomechanics following partial bladder obstruction. J. Biomechem. 2013, 46, 2752–2755. [Google Scholar] [CrossRef]
- Vasquez, E.; Cristofaro, V.; Lukianov, S.; Burkhard, F.C.; Gheinani, A.H.; Monastyrskaya, K.; Bielenberg, D.R.; Sullivan, M.P.; Adam, R.M. Deletion of neuropilin 2 enhances detrusor contractility following bladder outlet obstruction. JCI Insight 2017, 2, e90617. [Google Scholar] [CrossRef] [Green Version]
- Streng, T.; Li, X.; Lehtoranta, M.; Makela, S.; Poutanen, M.; Talo, A.; Tekmal, R.R.; Santti, R. Infravesical obstruction in aromatase over expressing transgenic male mice with increased ratio of serum estrogen-to-androgen concentration. J. Urol. 2002, 168, 298–302. [Google Scholar] [CrossRef]
- Wegner, K.A.; Ruetten, H.; Girardi, N.M.; O’Driscoll, C.A.; Sandhu, J.K.; Turco, A.E.; Abler, L.L.; Wang, P.; Wang, Z.; Bjorling, D.E.; et al. Genetic background but not prostatic epithelial beta-catenin influences susceptibility of male mice to testosterone and estradiol-induced urinary dysfunction. Am. J. Clin. Exp. Urol. 2021, 9, 121–131. [Google Scholar]
- Konkol, Y.; Vuorikoski, H.; Streng, T.; Tuomela, J.; Bernoulli, J. Characterization a model of prostatic diseases and obstructive voiding induced by sex hormone imbalance in the Wistar and Noble rats. Transl. Androl. Urol. 2019, 8, S45–S57. [Google Scholar] [CrossRef] [PubMed]
- Gopal, M.; Sammel, M.D.; Arya, L.A.; Freeman, E.W.; Lin, H.; Gracia, C. Association of change in estradiol to lower urinary tract symptoms during the menopausal transition. Obstet. Gynecol. 2008, 112, 1045–1052. [Google Scholar] [CrossRef] [Green Version]
- Nicholson, T.M.; Moses, M.A.; Uchtmann, K.S.; Keil, K.P.; Bjorling, D.E.; Vezina, C.M.; Wood, R.W.; Ricke, W.A. Estrogen receptor-alpha is a key mediator and therapeutic target for bladder complications of benign prostatic hyperplasia. J. Urol. 2015, 193, 722–729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buhl, A.E.; Yuan, Y.D.; Cornette, J.C.; Frielink, R.D.; Knight, K.A.; Ruppel, P.L.; Kimball, F.A. Steroid-induced urogenital tract changes and urine retention in laboratory rodents. J. Urol. 1985, 134, 1262–1267. [Google Scholar] [CrossRef]
- Collins, D.E.; Mulka, K.R.; Hoenerhoff, M.J.; Taichman, R.S.; Villano, J.S. Clinical assessment of urinary tract damage during sustained-release estrogen supplementation in mice. Comp. Med. 2017, 67, 11–21. [Google Scholar] [PubMed]
- Van Steenbrugge, G.J.; Groen, M.; de Jong, F.H.; Schroeder, F.H. The use of steroid-containing silastic implants in male nude mice: Plasma hormone levels and the effect of implantation on the weights of the ventral prostate and seminal vesicles. Prostate 1984, 5, 639–647. [Google Scholar] [CrossRef]
- Nomiya, M.; Yamaguchi, O.; Andersson, K.-E.; Sagawa, K.; Aikawa, K.; Shishido, K.; Yanagida, T.; Kushida, N.; Yazaki, J.; Takahashi, N. The effect of atherosclerosis-induced chronic bladder ischemia on bladder function in the rat. Neurourol. Urodyn. 2012, 31, 195–200. [Google Scholar] [CrossRef]
- Yoshida, A.; Kageyama, A.; Fujino, T.; Nozawa, Y.; Yamada, S. Loss of muscarinic and purinergic receptors in urinary bladder of rats with hydrochloric acid-induced cystitis. Urology 2010, 76, 1017-e7. [Google Scholar] [CrossRef]
- Kakizaki, H.; de Groat William, C. Role of spinal nitric oxide in the facilitation of the micturition reflex by bladder irritation. J. Urol. 1996, 155, 355–360. [Google Scholar] [CrossRef]
- Mitsui, T.; Kakizaki, H.; Matsuura, S.; Ameda, K.; Yoshioka, M.; Koyanagi, T. Afferent fibers of the hypogastric nerves are involved in the facilitating effects of chemical bladder irritation in rats. J. Neurophysiol. 2001, 86, 2276–2284. [Google Scholar] [CrossRef] [PubMed]
- Tai, C.; Shen, B.; Chen, M.; Wang, J.; Liu, H.; Roppolo, J.R.; de Groat, W.C. Suppression of bladder overactivity by activation of somatic afferent nerves in the foot. BJU Int. 2011, 107, 303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choudhary, M.; van Asselt, E.; van Mastrigt, R.; Clavica, F. Neurophysiological modeling of bladder afferent activity in the rat overactive bladder model. J. Physiol. Sci. 2015, 65, 329–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.; Liao, L. Improvement in detrusor-sphincter dyssynergia by bladder-wall injection of replication-defective herpes simplex virus vector-mediated gene delivery of kynurenine aminotransferase II in spinal cord injury rats. Spinal Cord 2017, 55, 155–161. [Google Scholar] [CrossRef]
- Saito, T.; Gotoh, D.; Wada, N.; Tyagi, P.; Minagawa, T.; Ogawa, T.; Ishizuka, O.; Yoshimura, N. Time-dependent progression of neurogenic lower urinary tract dysfunction after spinal cord injury in the mouse model. Am. J. Physiol. Ren. Physiol. 2021, 321, F26–F32. [Google Scholar] [CrossRef]


{kind=link}
| Acronym | Term | Definition |
|---|---|---|
| BPE | Benign Prostatic Enlargement | Non-malignant enlargement of the prostate, defined by imaging or digital rectal exam, and usually caused by BPH. |
| BPH | Benign Prostatic Hyperplasia | Histologically defined benign growth within the prostate. In humans, the growth pattern is nodular and can be primarily epithelial, stromal or mixed patterns of hyperplasia. BPH is often responsible for BPE. |
| BPO | Benign Prostatic Obstruction | BOO secondary to BPE. |
| BOO | Bladder Outlet Obstruction | Blockage of urine passage from an obstruction at the base of the bladder or bladder neck. |
| Clinical Prostatitis | A spectrum of conditions characterized by differing degrees of inflammation, bacterial and abacterial, of the prostate, genitourinary tract or pelvis and may not include the prostate. | |
| DO | Detrusor Overactivity | A urodynamic observation characterized by involuntary detrusor contractions during the filling phase that may be spontaneous or provoked. |
| DSD | Detrsor Spincter Dyssynergia | A disorder where the detrusor muscle contracts while the urethral and/or periurethral sphincter is involuntarily contracted and closed, resulting in bladder outlet obstruction. |
| Histological Prostatitis | Prostate inflammation detected in a biopsy specimen. | |
| LUTD | Lower Urinary Tract Dysfunction | A detrimental deviation from normal voiding function. Examples include decreased flow rate, increased voiding frequency, increased or decreased sensation associated with filling, an inability to completely void urine, and an inability to store urine until voluntary release. |
| LUTS | Lower Urinary Tract Symptoms | Patient described symptoms, scored using the international prostate symptom score, the American Urological Association Symptom index, or other indices that may (or may not) include bother. |
| OAB | Overactive Bladder | Urgency to urinate with or without urge incontinence, and usually associated with increased voiding frequency. |
| OVD | Obstruction Voiding Disorder | Lower urinary tract dysfunction deriving from an obstruction in the lower urinary tract. |
| pBOO | Partial Bladder Outlet Obstruction | Partial blockage of urine passage from an obstruction at the base of the bladder or bladder neck. |
| Prostatitism | Male LUTD deriving from a prostatic mechanism | |
| Prostatomegaly | Prostate enlargement from malignant or non-malignant mechanisms. |
| Method in Men | Method in Male Mice | Method Description | Strengths and Limitations |
|---|---|---|---|
| Cell and tissue-based calcium flux assays | Cell and tissue-based calcium flux assays | Calcium indicator dyes or genetically encoded calcium sensors are used to measure intracellular calcium concentrations in response to pharmacological agents and electrical field stimuli. | This method has been applied in vitro with human and mouse tissues and cells, and in vivo with mice, penetration can be limited for calcium indicator dyes and genetically encoded sensors are generally limited to mouse tissues. |
| Cystometry | Cystometry | A catheter is placed in the bladder and the bladder is filled with water or saline while measuring pressures associated with bladder filling and emptying. The catheter can also be used to collect post-void residual urine in the bladder. | Effective at measuring bladder pressure, but catheter is placed retropublicly in mice and transurethrally in humans which can contribute to intraspecies variability. Baseline pattern can vary by strain in mice. |
| Cystoscopy | Not available | A cystoscope is inserted into the urethra to visualize the lower urinary tract. | Effective in identifying prostatic enlargement, urethral and bladder inflammation, and some urological cancers, but this method is not available for mice. |
| Histology and immunohistoche-mistry | Histology and immunohistochemistry | Tissues sections are evaluated for BPH, inflammation and collagen accumulation (definitive diagnosis of BPH, histological prostatitis, fibrosis) and can be used to assess LUTD mechanisms. | Effective for assessing anatomical and cellular changes in lower urinary tract tissues and definitive diagnosis for some urological diseases but is invasive and therefore control tissues are difficult to obtain for healthy men for experimental comparisons; definitive identification of cell types requires complex multiplex protocols. |
| Isometric contractility | Isometric Contractility | Bladder, prostate, or urethral tissue is mounted in saline bath, pharmacological agents or electrical field stimuli are applied and force displacement is measured. | Quantitative and can reveal specific receptor mediated mechanisms of muscle function but is invasive and destructive to tissue (cannot be easily multiplexed with other methods. |
| Magnetic resonance imaging | Magnetic resonance imaging | Quantifies bladder wall thickness, detrusor and bladder volume, bladder neck angle, urethral length and diameter and prostate volume. | Can identify mechanisms of LUTD (bladder decompensation, BPE), but time consuming and expensive. |
| Symptom score | Not applicable | Standardized surveys such as the American Urological Association Symptom Index, the International Prostate Symptom Score, LURN, the National Institutes of Health-chronic prostatitis symptom index (NIH-CPSI) and others are used to quantify urinary symptoms and quality of life | Rapid, inexpensive and can be given repeatedly to monitor disease progression or responsiveness to therapy; limited to humans and not applicable for mice. |
| Ultrasound | Ultrasound | Quantifies bladder volume and wall thickness, urethral lumen diameter and in mice, velocity of urine as it passes through the urethra. | Fast but high-resolution imaging (for mice) requires expensive equipment. |
| Uroflowmetry | Uroflowmetry | Performed by measuring voided urine flow and volume. | Non-invasive, but requires specialized equipment, and operator experience and cannot distinguish between anatomical (bladder, prostate, or urethra) mechanisms of LUTD. |
| Voiding diary | Void spot assay | Men use a journal to record urinary void frequency, timing, and use a capture container to record volume; for mice, a filter paper is placed at the bottom of the cage and later illuminated to quantify void spot number, size, and pattern. | Inexpensive, noninvasive, but can vary by day and individual and cannot distinguish mechanism (bladder, urethra, prostate) of voiding dysfunction. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peterson, N.T.; Vezina, C.M. Male Lower Urinary Tract Dysfunction: An Underrepresented Endpoint in Toxicology Research. Toxics 2022, 10, 89. https://doi.org/10.3390/toxics10020089
Peterson NT, Vezina CM. Male Lower Urinary Tract Dysfunction: An Underrepresented Endpoint in Toxicology Research. Toxics. 2022; 10(2):89. https://doi.org/10.3390/toxics10020089
Chicago/Turabian StylePeterson, Nelson T., and Chad M. Vezina. 2022. "Male Lower Urinary Tract Dysfunction: An Underrepresented Endpoint in Toxicology Research" Toxics 10, no. 2: 89. https://doi.org/10.3390/toxics10020089
APA StylePeterson, N. T., & Vezina, C. M. (2022). Male Lower Urinary Tract Dysfunction: An Underrepresented Endpoint in Toxicology Research. Toxics, 10(2), 89. https://doi.org/10.3390/toxics10020089