
Helium Suicide, a Rapid and Painless Asphyxia: Toxicological Findings

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sampling
2.2. Toxicological Analysis
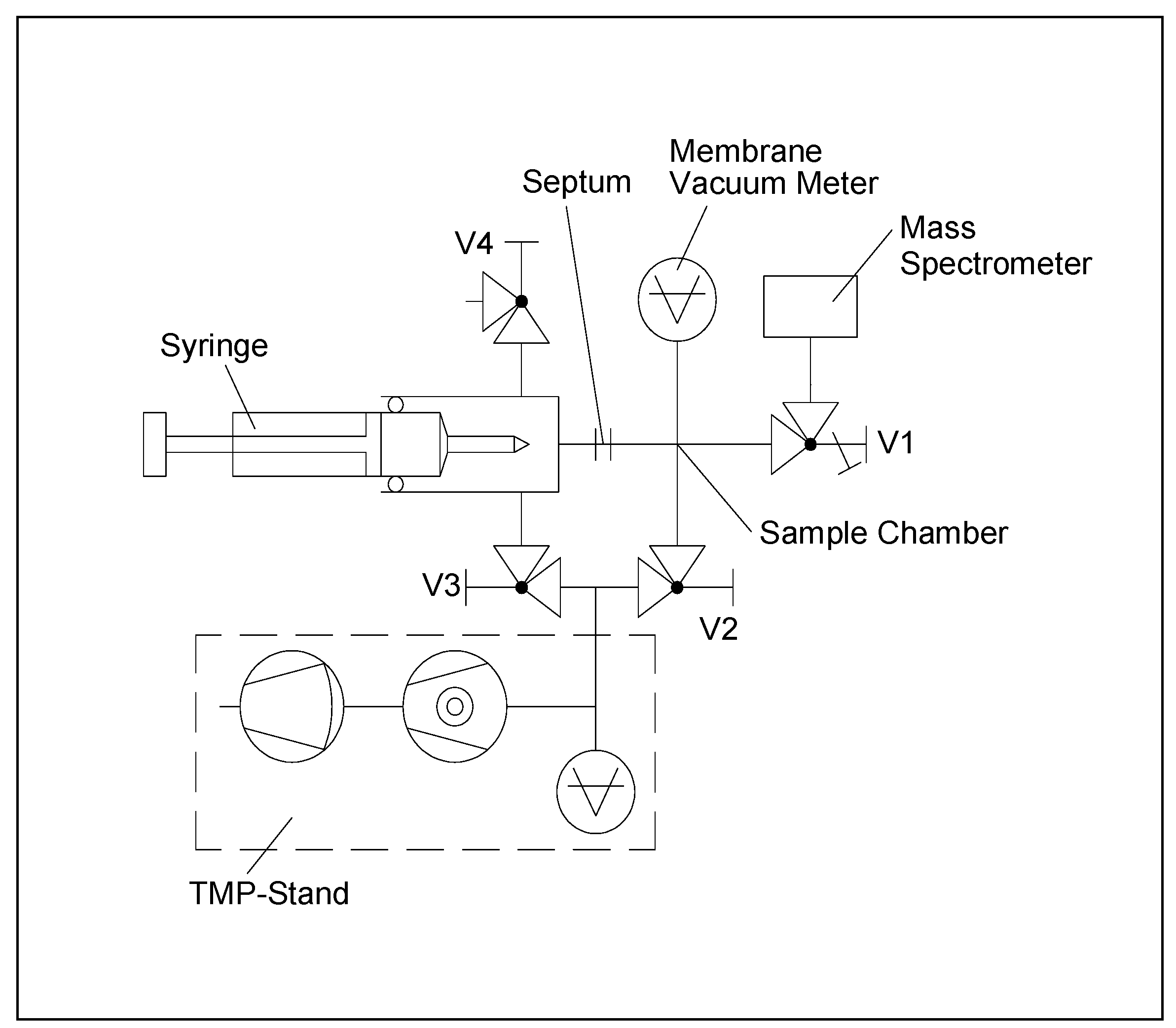
2.3. Gas-Inlet System
3. Results
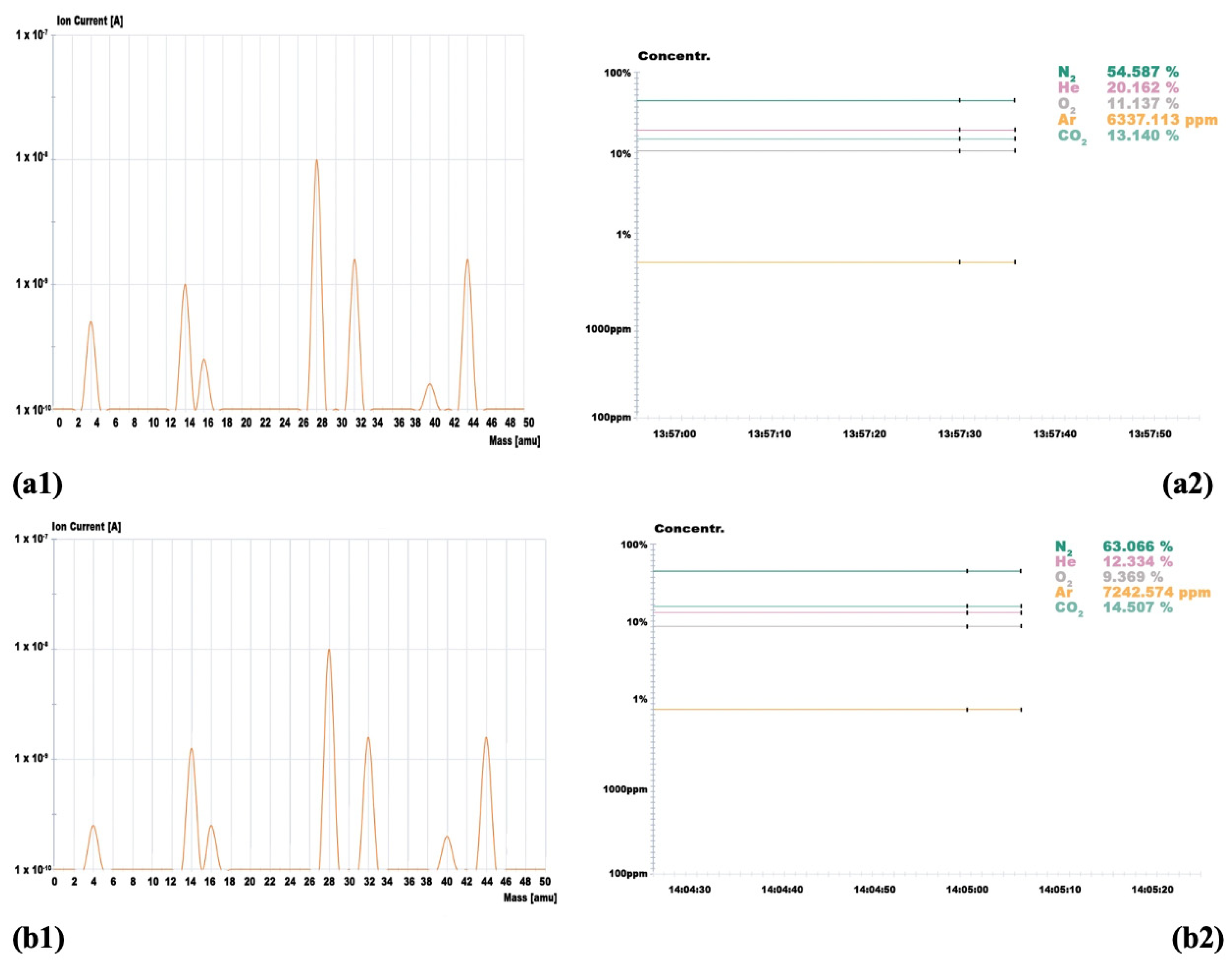
- Trachea: 20.16%
- Right lung: 12.33%
- Stomach: 1.5%
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Avis, S.P.; Archibald, J.T.; Musshoff, F.; Hagemeier, L.; Kirschbaum, K.; Madea, B. Two cases of suicide by asphyxiation due to helium and argon. Forensic Sci. Int. 2012, 223, e27–e30. [Google Scholar]
- Wick, R.; Gilbert, J.D.; Felgate, P.; Byard, R.W. Inhalant deaths in South Australia: A 20-year retrospective autopsy study. Am. J. Forensic Med. Pathol. 2007, 28, 319–322. [Google Scholar] [CrossRef] [PubMed]
- Gentile, G.; Galante, N.; Tambuzzi, S.; Zoja, R. A forensic analysis on 53 cases of complex suicides and one complicated assessed at the Bureau of Legal Medicine of Milan (Italy). Forensic Sci. Int. 2021, 319, 110662. [Google Scholar] [CrossRef] [PubMed]
- Avis, S.P.; Archibald, J.T. Asphyxial suicide by propane inhalation and plastic bag suffocation. J. Forensic Sci. 1994, 39, 253–256. [Google Scholar] [CrossRef]
- Gallagher, K.; Smith, D.M.; Mellen, P. Suicidal Asphyxiation by Using Pure Helium Gas Case Report, Review, and Discussion of the Influence of the Internet. Am. J. Forensic Med. Pathol. 2003, 24, 361–363. [Google Scholar] [CrossRef]
- Austin, A.; Winskog, C.; van den Heuvel, C.; Byard, R.W. Recent trends in suicides utilizing helium. J. Forensic Sci. 2011, 56, 649–651. [Google Scholar] [CrossRef]
- Frost, J. Death by self-inflicted asphyxia with helium—First case reports from Norway and review of the literature. Scand. J. Forensic Sci. 2013, 19, 52–54. [Google Scholar]
- Nowak, K.; Szpot, P.; Zawadzi, M. Suicidal deaths due to helium inhalation. Forensic Toxicol. 2019, 37, 273–287. [Google Scholar] [CrossRef] [Green Version]
- Wiergowski, M.; Kaliszan, M.; Suminska-Ziemann, B.; Gos, T.; Jankowski, Z. Helium detection in the lungs in case of suicide by helium inhalation-case report and literature review. Rom. J. Leg. Med. 2014, 22, 153–156. [Google Scholar]
- Smedra, A.; Szustowski, S.; Jurczyk, A.P.; Klemm, J.; Szram, S.; Berent, J. Suicidal asphyxiation by using helium-two case reports. Arch. Med. Sad. Kryminol. 2015, 65, 37–46. [Google Scholar]
- Konopka, T.; Strona, M.; Ksiezniak-Baran, D.; Wojton, D. Plastic bag suffocation in material collected by Department of Forensic Medicine in Krakow. Arch. Med. Sad. Kryminol. 2013, 63, 93–98. [Google Scholar]
- Barnung, S.K.; Feddersen, C. Selvmord ved hjaelp af helium og en plastikpose [Suicide by inhaling helium inside a plastic bag]. Ugeskr. Laeger 2004, 166, 3506–3507. [Google Scholar] [PubMed]
- Marzuk, P.M.; Tardiff, K.; Hirsch, C.S.; Leon, A.C.; Stajic, M.; Hartwell, N.; Portera, L. Increase in suicide by asphyxiation in New York City after the publication of Final Exit. N. Engl. J. Med. 1993, 329, 1508–1510. [Google Scholar] [CrossRef]
- Marzuk, P.M.; Tardiff, K.; Leon, A.C. Increase in fatal suicidal poisonings and suffocations in the year Final Exit was published: A national study. Am. J. Psychiatry 1994, 151, 1813–1814. [Google Scholar]
- van den Hondel, K.E.; Punt, P.; Dorn, T.; Ceelen, M.; Aarts, F.; van der Zande, D.; van Kuijk, S.; Duijst, W.; Stumpel, R.; van Mesdag, T.; et al. Suicide by helium inhalation in the Netherlands between 2012 and 2019. Forensic Sci. Int. 2021, 318, 110566. [Google Scholar] [CrossRef]
- Ogden, R.D.; Hassan, S. Suicide by Oxygen Deprivation with Helium: A Preliminary Study of British Columbia Coroner Investigations. Death Stud. 2011, 35, 338–364. [Google Scholar] [CrossRef]
- Humphry, D. Final Exit the Practicalities of Self-Deliverance and Assisted Suicide for the Dying, 3rd ed.; Delta Trade Paperback: New York, NY, USA, 2002. [Google Scholar]
- Humphry, D. Supplement to Final Exit: The Latest How-To and Why of Euthanasia/Hastened Death; Norris Lane Press: Eugene, OR, USA, 2000. [Google Scholar]
- Gilson, T.; Parks, B.O.; Porterfield, C.M. Suicide with inert gases: Addendum to Final Exit. Am. J. Forensic Med. Pathol. 2003, 24, 306–308. [Google Scholar] [CrossRef]
- Berganza, C.J.; Zhang, J.H. The role of helium gas in medicine. Med. Gas Res. 2013, 3, 18. [Google Scholar] [CrossRef] [Green Version]
- Byard, R.W. Changing trends in suicides using helium or nitrogen—A 15-year study. J. Forensic Leg. Med. 2018, 58, 6–8. [Google Scholar] [CrossRef]
- Chang, S.S.; Cheng, Q.; Lee, E.S.; Yip, P.S. Suicide by gassing in Hong Kong 2005–2013: Emerging trends and characteristics of suicide by helium inhalation. J. Affect. Disord. 2016, 192, 162–166. [Google Scholar] [CrossRef]
- Fink, J.B. Opportunities and risks of using heliox in your clinical practice. Respir. Care 2006, 51, 651–660. [Google Scholar]
- Ogden, R.D.; Hamilton, W.K.; Witcher, C. Assisted suicide with oxygen deprivation with helium at a Swiss right-to-die organization. J. Med. Ethics 2010, 36, 174–179. [Google Scholar] [CrossRef]
- Ogden, R.D. Observation of Two Suicides by Helium Inhalation in a Prefilled Environment. Am. J. Forensic Med. Pathol. 2010, 31, 156–161. [Google Scholar] [CrossRef]
- Di Maio, D.J.; Di Maio, V.J.M. Asphyxia. In Forensic Pathology; Elsevier: New York, NY, USA, 1989; pp. 207–251. [Google Scholar]
- Spitz, W.U. Asphyxia. In Spitz and Fisher’s Medicolegal Investigation of Death: Guidelines for the Application of Pathology to Crime Investigation, 3rd ed.; Charles C Thomas: Springfield, IL, USA, 1993; pp. 444–497. [Google Scholar]
- Grassberger, M.; Krauskopf, A. Suicidal asphyxiation with helium: Report of three cases. Wien. Klin. Wochenschr. 2007, 119, 323–325. [Google Scholar] [CrossRef]
- O’Higgins, J.W.; Guillen, J.; Aldrete, J.A. The effect of helium inhalation on asphyxia in dogs. J. Thorac. Cardiovasc. Surg. 1971, 61, 870–874. [Google Scholar] [CrossRef]
- Ogden, R.D. Non-physician assisted suicide: The technological imperative of the deathing counterculture. Death Stud. 2001, 25, 387–401. [Google Scholar] [PubMed]
- Werth, J.L., Jr. Policy and psychosocial considerations associated with non-physician assisted suicide: A commentary on Ogden. Death Stud. 2001, 25, 403–411. [Google Scholar] [PubMed]
- Lubell, K.M.; Swahn, M.H.; Crosby, A.E.; Kegler, S.R. Methods of Suicide Among Persons Aged 10–19 Years—United States, 1992–2001. JAMA J. Am. Med. Assoc. 2004, 292, 427–428. [Google Scholar]
- Byard, R.W. Further observations on plastic bag asphyxia using helium gas. Aust. J. Forensic Sci. 2017, 49, 483–486. [Google Scholar] [CrossRef]
- Borowska-Solonynko, A.; Dabkowska, A. Gas embolism as a potential cause of death by helium poisoning-postmortem computed tomography changes in two cases of suicidal helium inhalation. Leg. Med. 2018, 31, 59–65. [Google Scholar] [CrossRef]
- Malbranque, S.; Mauillon, D.; Turcant, A.; Rouge-maillart, C.; Mangin, P.; Varlet, V. Quantification of fatal helium exposure following self-administration. Int. J. Leg. Med. 2016, 130, 1535–1539. [Google Scholar] [CrossRef]
- Cuypers, E.; Rosier, E.; Loix, S.; Develter, W.; Van Den Bogaert, W.; Wuestenbergs, J.; Van de Voorde, W.; Tytgat, J. Medical Findings and Toxicological Analysis in Infant Death by Balloon Gas Asphyxia: A Case Report. J. Anal. Toxicol. 2017, 41, 347–349. [Google Scholar] [CrossRef] [PubMed]
- Tsujita, A.; Okazaki, H.; Nagasaka, A.; Gohda, A.; Matsumoto, M.; Matsui, T. A new and sensitive method for quantitative determination of helium in human blood by gas chromatography–mass spectrometry using naturally existing neon-21 as internal standard. Forensic Toxicol. 2019, 37, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Schaff, J.E.; Karas, R.P.; Marinetti, L. A Gas Chromatography–Thermal Conductivity Detection Method for Helium Detection in Postmortem Blood and Tissue Specimens. J. Anal. Toxicol. 2012, 36, 112–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oosting, R.; van der Hulst, R.; Poeschier, L.; Verschraagen, M. Toxicological findings in three cases of suicidal asphyxiation with helium. Forensic Sci. Int. 2015, 256, 38–41. [Google Scholar] [CrossRef]
- Tanaka, N.; Takakura, A.; Jamal, M.; Kumihashi, M.; Ito, A.; Ishimoto, S.; Tsutsui, K.; Kimura, S.; Ameno, K.; Kinoshita, H. Stomach gas as a useful matrix for detecting ante-mortem gas exposure. A case of asphyxia by helium inhalation. Rom. J. Leg. Med. 2016, 24, 21–22. [Google Scholar] [CrossRef] [Green Version]
- Varlet, V.; Iwersen-Bergmann, S.; Alexandre, M.; Cordes, O.; Wunder, C.; Holz, F.; Andersen-Streichert, H.; Bevalot, F.; Dumestre-Toulet, V.; Malbranque, S.; et al. Helium poisoning: New procedure for sampling and analysis. Int. J. Leg. Med. 2019, 133, 1809–1818. [Google Scholar] [CrossRef] [PubMed]
- Carfora, A.; Campobasso, C.P.; Cassandro, P.; Petrella, R.; Borriello, R. Alcohol and drugs use among drivers injured in road accidents in Campania (Italy): A 8-years retrospective analysis. Forensic Sci. Int. 2018, 288, 291–296. [Google Scholar] [CrossRef]
- Carfora, A.; Borriello, R.; Cassandro, P.; Petrella, R.; Campobasso, C.P. Alcohol and drug use in drug-related deaths in campania (Italy): A snapshot study over the years 2008–2018. J. Integr. OMICS 2020, 10, 10–14. [Google Scholar] [CrossRef]
- Madea, B. Asphyiation, Suffocation, and Neck Pressure Deaths; Taylor & Francis Inc.: Boca Raton, FL, USA, 2020; p. 191. [Google Scholar]
- Carfora, A.; Campobasso, C.P.; Cassandro, P.; La Sala, F.; Maiellaro, A.; Perna, A.; Petrella, R.; Borriello, R. Fatal inhalation of volcanic gases in three tourists of a geothermal area. Forensic Sci. Int. 2019, 297, e1–e7. [Google Scholar] [CrossRef]
- Barbera, N.; Montana, A.; Indorato, F.; Arbouche, N.; Romano, G. Domino effect: An unusual case of six fatal hydrogen sulfide poisonings in quick succession. Forensic Sci. Int. 2016, 260, e7–e10. [Google Scholar] [CrossRef]
- Ogden, R.D.; Wooten, R.H. Asphyxial Suicide with Helium and Plastic Bag. Am. J. Forensic Med. Pathol. 2002, 23, 234–237. [Google Scholar] [CrossRef]
- Saukko, P.; Knight, B. (Eds.) Knight’s Forensic Pathology, 3rd ed.; Edwards Arnold Publishers: London, UK, 2004. [Google Scholar]
- Maxeiner, H.; Bockholdt, B. Homicidal and suicidal ligature strangulation: A comparison of the postmortem findigs. Forensic Sci. Int. 2003, 137, 60–66. [Google Scholar] [CrossRef]
- Ely, S.F.; Hirsch, C.S. Asphyxial deaths and petechiae. J. Forensic Sci. 2000, 45, 1274–1277. [Google Scholar] [CrossRef]
- Grellner, W.; Anders, S.; Tsokos, M.; Wilske, J. Suicide with exit bags: Circumstances and special problem situations in assisted suicide. Arch. Kriminol. 2002, 209, 65–75. [Google Scholar]
- Bullock, M.J.; Diniz, D. Suffocation using plastic bags: A retrospective study of suicides in Ontario, Canada. J. Forensic Sci. 2000, 45, 608–613. [Google Scholar] [CrossRef]
- Jones, L.S.; Wyatt, J.P.; Busuttil, A. Plastic bag asphyxia in southeast Scotland. Am. J. Forensic Med. Pathol. 2000, 21, 401–405. [Google Scholar] [CrossRef]
- Schön, C.A.; Ketterer, T. Asphyxial Suicide by Inhalation of Helium Inside a Plastic Bag. Am. J. Forensic Med. Pathol. 2007, 26, 364–367. [Google Scholar] [CrossRef]
- Campobasso, C.P.; Laviola, D.; Grattagliano, I.; Strada, L.; Dell’Erba, A.S. Undetected patricide: Inaccuracy of cause of death determination without an autopsy. J. For. Leg. Med. 2015, 34, 67–72. [Google Scholar] [CrossRef]
- Auwaerter, V.; Grosse Perdekamp, M.; Kempf, J.; Schmith, U.; Weinmann, W.; Pollak, S. Toxicological analysis after asphyxia suicide with helium and a plastic bag. Forensic Sci. Int. 2007, 170, 139–141. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Trachea | Right Bronchus | Stomach | |
|---|---|---|---|
| Qualitative Analysis | Positive | Positive | Positive |
| Helium (He) | 20.16% | 12.33% | 1.5% |
| Oxygen (O2) | 11.14% | 9.37% | — |
| Nitrogen (N2) | 54.59% | 63.06% | — |
| Carbon Dioxide (CO2) | 13.14% | 14.50% | — |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carfora, A.; Petrella, R.; Ambrosio, G.; Mascolo, P.; Liguori, B.; Juhnke, C.; Campobasso, C.P.; Keller, T. Helium Suicide, a Rapid and Painless Asphyxia: Toxicological Findings. Toxics 2022, 10, 424. https://doi.org/10.3390/toxics10080424
Carfora A, Petrella R, Ambrosio G, Mascolo P, Liguori B, Juhnke C, Campobasso CP, Keller T. Helium Suicide, a Rapid and Painless Asphyxia: Toxicological Findings. Toxics. 2022; 10(8):424. https://doi.org/10.3390/toxics10080424
Chicago/Turabian StyleCarfora, Anna, Raffaella Petrella, Giusy Ambrosio, Pasquale Mascolo, Bruno Liguori, Christian Juhnke, Carlo Pietro Campobasso, and Thomas Keller. 2022. "Helium Suicide, a Rapid and Painless Asphyxia: Toxicological Findings" Toxics 10, no. 8: 424. https://doi.org/10.3390/toxics10080424
APA StyleCarfora, A., Petrella, R., Ambrosio, G., Mascolo, P., Liguori, B., Juhnke, C., Campobasso, C. P., & Keller, T. (2022). Helium Suicide, a Rapid and Painless Asphyxia: Toxicological Findings. Toxics, 10(8), 424. https://doi.org/10.3390/toxics10080424