
Forensic Aspects of a Fatal Intoxication Involving Acetaminophen, Citalopram and Trazodone: A Case Report

 , ,
, ,  and
and
Abstract
:1. Introduction
1.1. Acetaminophen
1.2. Citalopram
1.3. Trazodone
2. Case Report
2.1. Scene of Death Inspection
2.2. Autopsy Findings
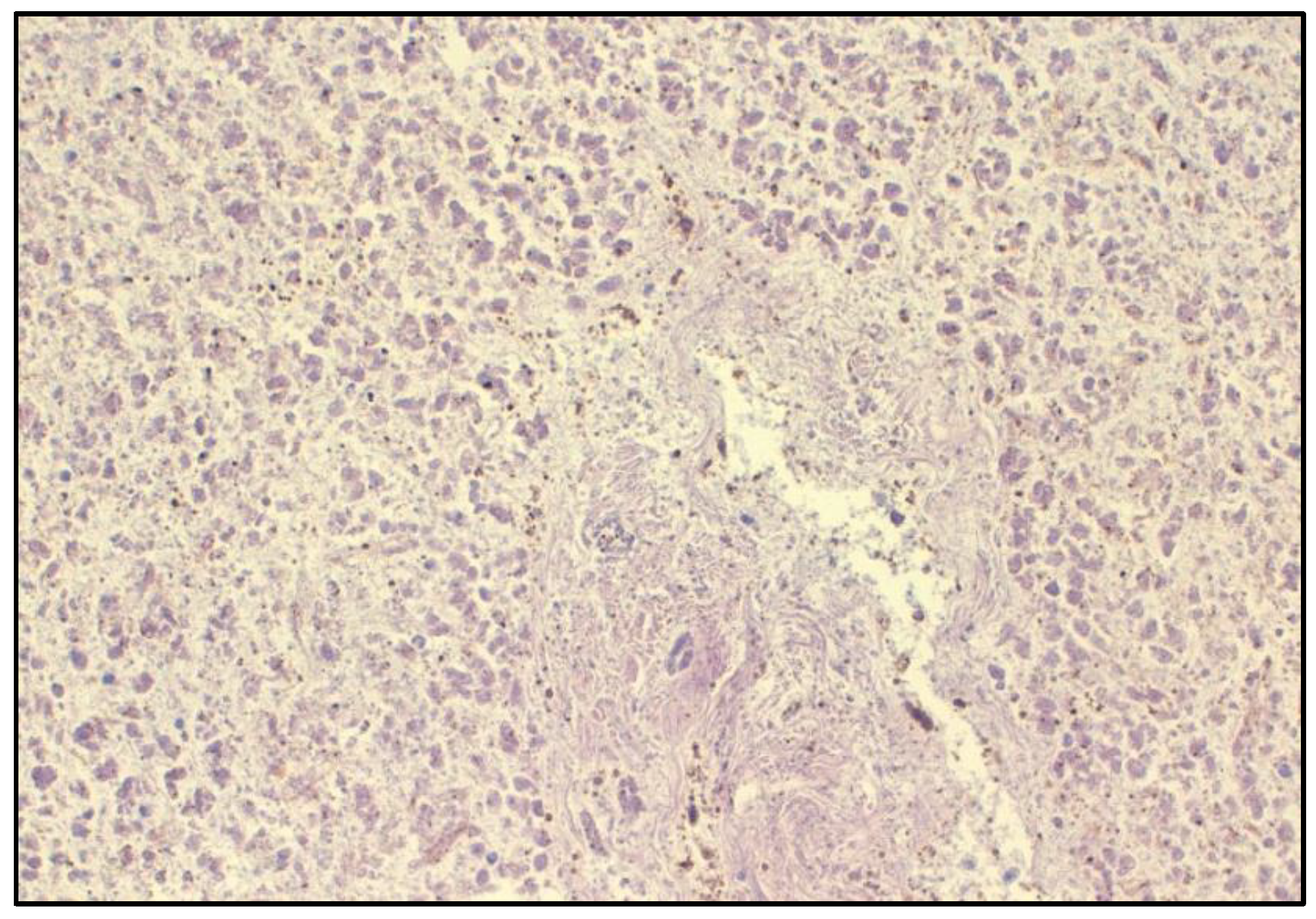
2.3. Histological Findings
3. Materials and Methods
3.1. Samples
3.2. Chemical and Reagents
3.3. Qualitative Analysis
3.4. Quantitative Analysis of Acetaminophen
3.5. Quantitative Analysis of Citalopram and Trazodone
3.6. Instrumentation and Conditions
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gupta, A.; Bah, M. NSAIDs in the Treatment of Postoperative Pain. Curr. Pain Headache Rep. 2016, 20, 62. [Google Scholar] [CrossRef] [PubMed]
- Sheen, C.L.; Dillon, J.F.; Bateman, D.N.; Simpson, K.J.; MacDonald, T.M. Paracetamol-related deaths in Scotland, 1994–2000. Br. J. Clin. Pharmacol. 2002, 54, 430–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tittarelli, R.; Pellegrini, M.; Scarpellini, M.G.; Marinelli, E.; Bruti, V.; di Luca, N.M.; Busardo, F.P.; Zaami, S. Hepatotoxicity of paracetamol and related fatalities. Eur. Rev. Med. Pharmacol. Sci. 2017, 21 (Suppl. 1), 95–101. [Google Scholar] [PubMed]
- Lancaster, E.M.; Hiatt, J.R.; Zarrinpar, A. Acetaminophen hepatotoxicity: An updated review. Arch. Toxicol. 2015, 89, 193–199. [Google Scholar] [CrossRef] [PubMed]
- De-Giorgio, F.; Lodise, M.; Chiarotti, M.; D’Aloja, E.; Carbone, A.; Valerio, L. Possible Fatal Acetaminophen Intoxication with Atypical Clinical Presentation. J. Forensic Sci. 2013, 58, 1397–1400. [Google Scholar] [CrossRef]
- Moyer, A.M.; Fridley, B.L.; Jenkins, G.D.; Batzler, A.J.; Pelleymounter, L.L.; Kalari, K.R.; Ji, Y.; Chai, Y.; Nordgren, K.K.; Weinshilboum, R.M. Acetaminophen-NAPQI hepatotoxicity: A cell line model system genome-wide association study. Toxicol. Sci. 2011, 120, 33–41. [Google Scholar] [CrossRef]
- Bloukh, S.; Wazaify, M.; Matheson, C. Paracetamol: Unconventional uses of a well-known drug. Int. J. Pharm. Pract. 2021, 29, 527–540. [Google Scholar] [CrossRef]
- Doyon, S.; Klein-Schwartz, W.; Lee, S.; Beuhler, M.C. Fatalities involving acetaminophen combination products reported to United States poison centers. Clin. Toxicol. 2013, 51, 941–948. [Google Scholar] [CrossRef]
- Yoon, E.; Babar, A.; Choudhary, M.; Kutner, M.; Pyrsopoulos, N. Acetaminophen-Induced Hepatotoxicity: A Comprehensive Update. J. Clin. Transl. Hepatol. 2016, 4, 131–142. [Google Scholar] [CrossRef] [Green Version]
- Schulz, M.; Schmoldt, A.; Andresen-Streichert, H.; Iwersen-Bergmann, S. Revisited: Therapeutic and toxic blood concentrations of more than 1100 drugs and other xenobiotics. Crit. Care 2020, 24, 195. [Google Scholar] [CrossRef]
- Pantano, F.; Tittarelli, R.; Mannocchi, G.; Zaami, S.; Ricci, S.; Giorgetti, R.; Terranova, D.; Busardo, F.P.; Marinelli, E. Hepatotoxicity Induced by “the 3Ks”: Kava, Kratom and Khat. Int. J. Mol. Sci. 2016, 17, 580. [Google Scholar] [CrossRef] [PubMed]
- Danan, G.; Teschke, R. RUCAM in Drug and Herb Induced Liver Injury: The Update. Int. J. Mol. Sci. 2016, 17, 14. [Google Scholar] [CrossRef] [PubMed]
- Luchini, D.; Morabito, G.; Centini, F. Case Report of a Fatal Intoxication by Citalopram. Am. J. Forensic Med. Pathol. 2005, 26, 352–354. [Google Scholar] [CrossRef] [PubMed]
- Schult, R.F.; Morris, A.J.; Picard, L.; Wiegand, T.J. Citalopram overdose and severe serotonin syndrome in an intermediate metabolizing patient. Am. J. Emerg. Med. 2019, 37, 1993.e5–1993.e6. [Google Scholar] [CrossRef] [PubMed]
- Gruszecki, A.C.; Kloda, S.; Simmons, G.T.; Daly, T.M.; Hardy, R.W.; Robinson, C.A. Polydrug fatality involving metaxalone. J. Forensic Sci. 2003, 48, 432–434. [Google Scholar] [CrossRef] [PubMed]
- Moore, K.A.; Levine, B.; Fowler, D. A fatality involving metaxalone. Forensic Sci. Int. 2005, 149, 249–251. [Google Scholar] [CrossRef]
- Kraai, E.P.; Seifert, S.A. Citalopram Overdose: A Fatal Case. J. Med. Toxicol. 2015, 11, 232–236. [Google Scholar] [CrossRef] [Green Version]
- Hargrove, V.; Molina, D.K. A Fatality Due to Cyproheptadine and Citalopram. J. Anal. Toxicol. 2009, 33, 564–567. [Google Scholar] [CrossRef] [Green Version]
- Moffat, A.C.; Osselton, D.M.; Widdop, B. Clarke’s Analysis of Drugs and Poisons in Pharmaceuticals, Body Fluids and Postmortem Material, 4th ed.; Pharmaceutical Press: London, UK, 2011. [Google Scholar]
- Khouzam, H.R. A review of trazodone use in psychiatric and medical conditions. Postgrad. Med. 2017, 129, 140–148. [Google Scholar] [CrossRef]
- Bossini, L.; Casolaro, I.; Koukouna, D.; Cecchini, F.; Fagiolini, A. Off-label uses of trazodone: A review. Expert Opin. Pharmacother. 2012, 13, 1707–1717. [Google Scholar] [CrossRef]
- Marek, G.J.; McDougle, C.J.; Price, L.H.; Seiden, L.S. A comparison of trazodone and fluoxetine: Implications for a serotonergic mechanis of antidepressant action. Psychopharmacology 1992, 109, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Martínez, M.A.; Ballesteros, S.; Sánchez de la Torre, C.; Almarza, E. Investigation of a Fatality Due to Trazodone Poisoning: Case Report and Literature Review. J. Anal. Toxicol. 2005, 29, 262–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Meester, A.; Carbutti, G.; Gabriel, L.; Jacques, J. Fatal overdose with trazodone: Case report and literature review. Acta Clin. Belg. 2001, 56, 258–261. [Google Scholar] [CrossRef] [PubMed]
- Soe, K.K.; Lee, M.Y. Arrhythmias in Severe Trazodone Overdose. Am. J. Case Rep. 2019, 20, 1949–1955. [Google Scholar] [CrossRef]
- Adson, D.E.; Erickson-Birkedahl, S.; Kotlyar, M. An Unusual Presentation of Sertraline and Trazodone Overdose. Ann. Pharmacother. 2001, 35, 1375–1377. [Google Scholar] [CrossRef]
- Saitman, A.; Park, H.-D.; Fitzgerald, R.L. False-Positive Interferences of Common Urine Drug Screen Immunoassays: A Review. J. Anal. Toxicol. 2014, 38, 387–396. [Google Scholar] [CrossRef] [Green Version]
- Peters, F.T.; Drummer, O.H.; Musshoff, F. Validation of new methods. Forensic Sci. Int. 2007, 165, 216–224. [Google Scholar] [CrossRef]
- Ferrari, L.A.; Triszcz, J.M.; Giannuzzi, L. Kinetics of ethanol degradation in forensic blood samples. Forensic Sci. Int. 2006, 161, 144–150. [Google Scholar] [CrossRef]
- O’Neal, C.L.; Poklis, A. Postmortem Production of Ethanol and Factors that Influence Interpretation. Am. J. Forensic Med. Pathol. 1996, 17, 8–20. [Google Scholar] [CrossRef]
- Boumba, V.A. Modeling Postmortem Ethanol Production/Insights into the Origin of Higher Alcohols. Molecules 2022, 27, 700. [Google Scholar] [CrossRef]
- Lin, Z.; Wang, H.; Jones, A.W.; Wang, F.; Zhang, Y.; Rao, Y. Evaluation and review of ways to differentiate sources of ethanol in postmortem blood. Int. J. Leg. Med. 2020, 134, 2081–2093. [Google Scholar] [CrossRef] [PubMed]
- Seetohul, L.N.; De Paoli, G.; Drummond, G.; Maskell, P.D. Nefopam Hydrochloride: A Fatal Overdose. J. Anal. Toxicol. 2015, 39, 486–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, A.W.; Holmgren, A.; Ahlner, J. Toxicology findings in suicides: Concentrations of ethanol and other drugs in femoral blood in victims of hanging and poisoning in relation to age and gender of the deceased. J. Forensic Leg. Med. 2013, 20, 842. [Google Scholar] [CrossRef]
- Fernandes, N.F.; Martin, R.R.; Schenker, S. Trazodone-induced hepatotoxicity: A case report with comments on drug-induced hepatotoxicity. Am. J. Gastroenterol. 2000, 95, 532–535. [Google Scholar] [CrossRef] [PubMed]
- Taziki, S.; Sattari, M.R.; Eghbal, M.A. Mechanisms of trazodone-induced cytotoxicity and the protective effects of melatonin and/or taurine toward freshly isolated rat hepatocytes. J. Biochem. Mol. Toxicol. 2013, 27, 457–462. [Google Scholar] [CrossRef]
- Incalzi, R.A.; Caraci, F.; Cuomo, A.; Fagiolini, A.; Ferini Strambi, L. Trattamento Personalizzato dei Fenotipi di Depressione: Ruolo del Trazodone nella Depressione con Insonnia. Riv. Psichiatr. 2020, 55, 371–379. Available online: https://www.rivistadipsichiatria.it/archivio/3503/articoli/34896/ (accessed on 3 August 2022).
- Karinen, R.; Andresen, W.; Smith-Kielland, A.; Morland, J. Long-term storage of authentic postmortem forensic blood samples at −20 degrees C: Measured concentrations of benzodiazepines, central stimulants, opioids and certain medicinal drugs before and after storage for 16–18 years. J. Anal. Toxicol. 2014, 38, 686–695. [Google Scholar] [CrossRef] [Green Version]
- Holmgren, P.; Druid, H.; Holmgren, A.; Ahlner, J. Stability of drugs in stored postmortem femoral blood and vitreous humor. J. Forensic Sci. 2004, 49, 820–825. [Google Scholar] [CrossRef]
- Moretti, M.; Freni, F.; Valentini, B.; Vignali, C.; Groppi, A.; Visonà, S.D.; Osculati, A.M.M.; Morini, L. Determination of Antidepressants and Antipsychotics in Dried Blood Spots (DBSs) Collected from Post-Mortem Samples and Evaluation of the Stability over a Three-Month Period. Molecules 2019, 24, 3636. [Google Scholar] [CrossRef] [Green Version]
- Lewis, R.J.; Angier, M.K.; Johnson, R.D.; Rains, B.M.; Nepal, S. Analysis of Citalopram and Desmethylcitalopram in Postmortem Fluids and Tissues Using Liquid Chromatography-Mass Spectrometry; Technical Report for Federal Aviation Administration Oklahoma City OK Civil Aerospace Medical Institute; Civil Aerospace Medical Institute, Federal Aviation Administration: Oklahoma City, OK, USA, 2011; p. 11.
- Martin, A.; Pounder, D.J. Post-mortem toxico-kinetics of trazodone. Forensic Sci. Int. 1992, 56, 201–207. [Google Scholar] [CrossRef]
- McIntyre, I.M.; Mallett, P.; Stabley, R. Postmortem distribution of trazodone concentrations. Forensic Sci. Int. 2015, 251, 195–201. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Blood | Urine | |||
|---|---|---|---|---|
| Compound | LOD (µg/mL) | LLOQ (µg/mL) | LOD (µg/mL) | LLOQ (µg/mL) |
| Acetaminophen | 4.80 | 15.00 | 2.50 | 8.10 |
| Citalopram | 0.34 | 1.10 | 0.10 | 0.32 |
| Trazodone | 0.28 | 0.90 | 0.18 | 0.60 |
| Samples | Acetaminophen (μg/mL) | Citalopram (μg /mL) | Trazodone (μg/mL) |
|---|---|---|---|
| Peripheral Blood | 328 | 2.7 | 21 |
| Urine | 155 | 50 | 109 |
| Substance | Blood-Plasma Concentration (μg/mL) | ||
|---|---|---|---|
| Therapeutic (“Normal”) | Toxic (From) | Comatose-Fatal (From) | |
| Acetaminophen | (5-)10–25 | 100–150 | 200–300 |
| Citalopram | 0.05–0.11 | 0.22 | 5–6 |
| Trazodone | 0.7–1 | 1.2; 3–4 | 12–15 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mannocchi, G.; Tittarelli, R.; Pantano, F.; Vernich, F.; Pallocci, M.; Passalacqua, P.; Treglia, M.; Marsella, L.T. Forensic Aspects of a Fatal Intoxication Involving Acetaminophen, Citalopram and Trazodone: A Case Report. Toxics 2022, 10, 486. https://doi.org/10.3390/toxics10080486
Mannocchi G, Tittarelli R, Pantano F, Vernich F, Pallocci M, Passalacqua P, Treglia M, Marsella LT. Forensic Aspects of a Fatal Intoxication Involving Acetaminophen, Citalopram and Trazodone: A Case Report. Toxics. 2022; 10(8):486. https://doi.org/10.3390/toxics10080486
Chicago/Turabian StyleMannocchi, Giulio, Roberta Tittarelli, Flaminia Pantano, Francesca Vernich, Margherita Pallocci, Pierluigi Passalacqua, Michele Treglia, and Luigi Tonino Marsella. 2022. "Forensic Aspects of a Fatal Intoxication Involving Acetaminophen, Citalopram and Trazodone: A Case Report" Toxics 10, no. 8: 486. https://doi.org/10.3390/toxics10080486
APA StyleMannocchi, G., Tittarelli, R., Pantano, F., Vernich, F., Pallocci, M., Passalacqua, P., Treglia, M., & Marsella, L. T. (2022). Forensic Aspects of a Fatal Intoxication Involving Acetaminophen, Citalopram and Trazodone: A Case Report. Toxics, 10(8), 486. https://doi.org/10.3390/toxics10080486