
Effects of COVID-19 Disease on DNA Damage, Oxidative Stress and Immune Responses

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Experimental Design
2.2. Preparation of Samples
2.3. Determination of Biochemical Parameters
2.4. Determination of Oxidative Stress and Immune Parameters
2.5. Determination of DNA Damage
2.6. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Hemograms and Biochemical Parameters
3.3. Oxidative Stress and Immune Parameters
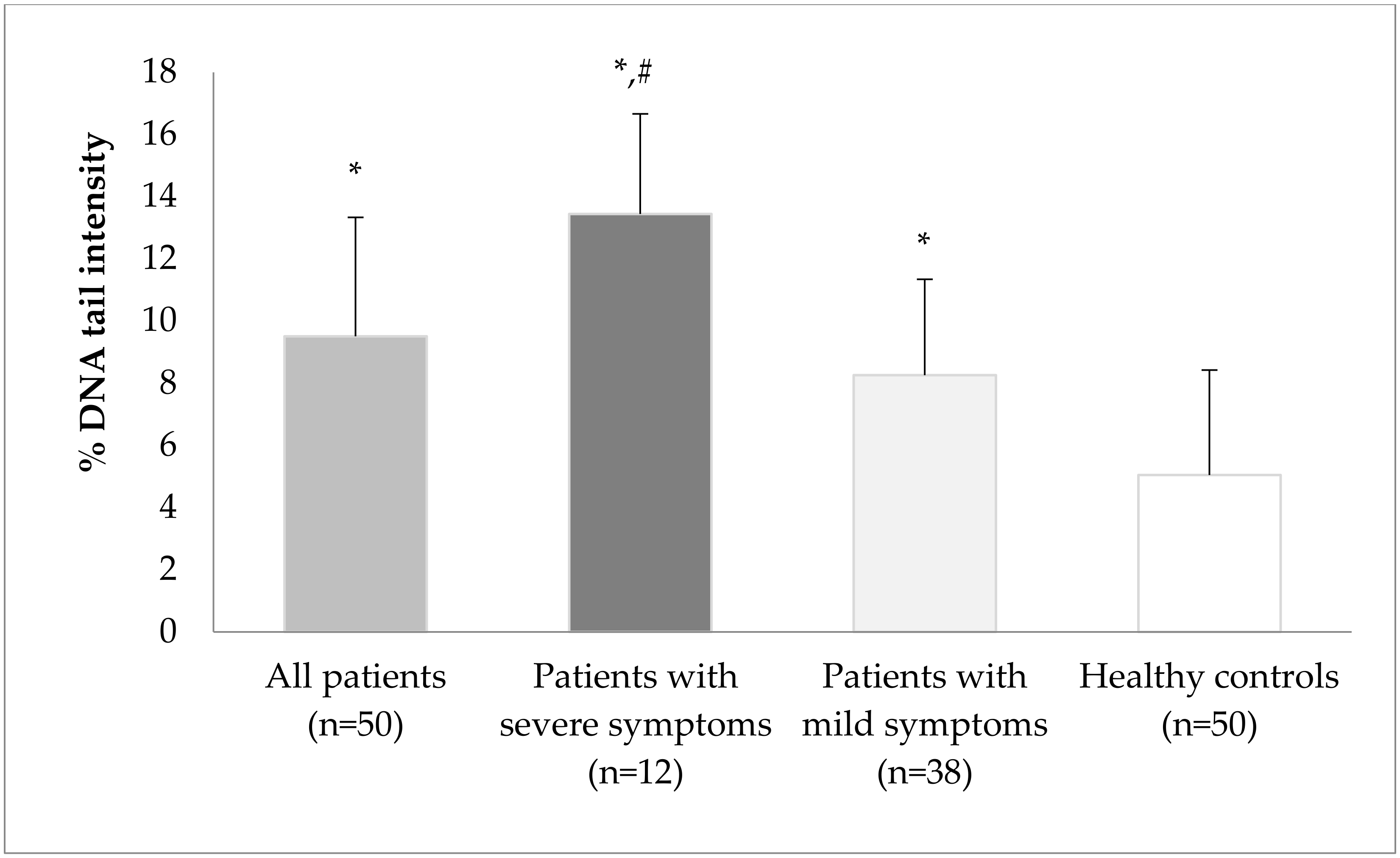
3.4. The Alkaline Single-Cell Gel Electrophoresis Technique (Comet Assay)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tang, D.; Comish, P.; Kang, R. The hallmarks of COVID-19 disease. PLoS Pathog. 2020, 16, e1008536. [Google Scholar] [CrossRef] [PubMed]
- Karimzadeh, S.; Bhopal, R.; Nguyen Tien, H. Review of infective dose, routes of transmission and outcome of COVID-19 caused by the SARS-CoV-2: Comparison with other respiratory viruses. Epidemiol. Infect. 2021, 149, e96. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-Las-Peñas, C.; Palacios-Ceña, D.; Gómez-Mayordomo, V.; Cuadrado, M.L.; Florencio, L.L. Defining Post-COVID Symptoms (Post-Acute COVID, Long COVID, Persistent Post-COVID): An Integrative Classification. Int. J. Environ. Res. Public Health 2021, 18, 2621. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 long-term effects of COVID-19: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 16144. [Google Scholar] [CrossRef] [PubMed]
- Kermali, M.; Khalsa, R.K.; Pillai, K.; Ismail, Z.; Harky, A. The role of biomarkers in diagnosis of COVID-19—A systematic review. Life Sci. 2020, 254, 117788. [Google Scholar] [CrossRef] [PubMed]
- Henry, B.M.; de Oliveira, M.H.S.; Benoit, S.; Plebani, M.; Lippi, G. Hematologic, biochemical and immune biomarker abnormalities associated with severe illness and mortality in coronavirus disease 2019 (COVID-19): A meta-analysis. Clin. Chem. Lab. Med. 2020, 58, 1021–1028. [Google Scholar] [CrossRef] [PubMed]
- Akboga, S.A.; Gokce, A.; Hatipoglu, M.; Beyoglu, M.A.; Inan, K.; Sezen, A.I.; Dal, H.C.; Akkas, Y.; Turan, S.; Kocer, B. The relationship between mortality and inflammatory markers and the systemic immune inflammatory index in patients in the intensive care unit with a pneumothorax as a complication of COVID-19 disease. Ir. J. Med. Sci. 2022, 191, 1931–1936. [Google Scholar] [CrossRef] [PubMed]
- Çakırca, G.; Damar Çakırca, T.; Üstünel, M.; Torun, A.; Koyuncu, İ. Thiol level and total oxidant/antioxidant status in patients with COVID-19 infection. Ir. J. Med. Sci. 2022, 191, 1925–1930. [Google Scholar] [CrossRef]
- De Martel, C.; Georges, D.; Bray, F.; Ferlay, J.; Clifford, G.M. Global burden of cancer attributable to infections in 2018: A worldwide incidence analysis. Lancet Glob. Health 2020, 8, 180–190. [Google Scholar] [CrossRef]
- Gaglia, M.M.; Munger, K. More than just oncogenes: Mechanisms of tumorigenesis by human viruses. Curr. Opin. Virol. 2018, 32, 48–59. [Google Scholar] [CrossRef]
- Moore, P.S.; Chang, T. Why do viruses cause cancer. Highlights of the first century of human tumour virology. Nat. Rev. Cancer 2010, 10, 878–889. [Google Scholar] [CrossRef]
- Martin, D.; Gutkind, J.S. Human tumor-associated viruses and new insights into the molecular mechanisms of cancer. Oncogene 2008, 27, 31–42. [Google Scholar] [CrossRef]
- Zur Hausen, H. Papillomaviruses and cancer: From basic studies to clinical application. Nat. Rev. Cancer 2002, 2, 342–350. [Google Scholar] [CrossRef] [PubMed]
- El-Serag, H.B. Hepatocellular carcinoma. N. Engl. J. Med. 2011, 365, 1118–1127. [Google Scholar] [CrossRef]
- Bartsch, H.; Nair, J. Oxidative stress and lipid peroxidation-derived DNA-lesions in inflammation driven carcinogenesis. Cancer Detect. Prev. 2004, 28, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Winer, S.; Winer, D.A. The adaptive immune system as a fundamental regulator of adipose tissue inflammation and insulin resistance. Immunol. Cell Biol. 2012, 90, 755–762. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.Y.; Oh, E.; Kim, Y.; Jung, W.W.; Kim, H.S.; Lee, J.; Sul, D. Enhanced oxidative damage to DNA, lipids, and proteins and levels of some antioxidant enzymes, cytokines, and heat shock proteins in patients infected with influenza H1N1 virus. Acta Virol. 2014, 58, 253–260. [Google Scholar] [CrossRef]
- Ng, M.P.; Lee, J.C.; Loke, W.M.; Yeo, L.L.; Quek, A.M.; Lim, E.C.; Halliwell, B.; Seet, R.C. Does influenza A infection increase oxidative damage? Antioxid. Redox Signal. 2014, 21, 1025–1031. [Google Scholar] [CrossRef] [PubMed]
- Van Loon, B.; Markkanen, E.; Hübscher, U. Oxygen as a friend and enemy: How to combat the mutational potential of 8-oxo-guanine. DNA Repair 2010, 9, 604–616. [Google Scholar] [CrossRef] [PubMed]
- Markkanen, E. Not breathing is not an option: How to deal with oxidative DNA damage. DNA Repair 2017, 59, 82–105. [Google Scholar] [CrossRef] [PubMed]
- Pande, P.; Das, R.S.; Sheppard, C.; Know, Y.W.; Basu, A.K. Repair efficiency of (5′S)-8,5′-cyclo-2′-deoxyguanosine and (5′S)-8,5′-cyclo-2′-deoxyadenosine depends on the complementary base. DNA Repair 2012, 11, 926–931. [Google Scholar] [CrossRef]
- Delgado-Roche, L.; Mesta, F. Oxidative stress as key player in severe acute respiratory syndrome coronavirus (SARS-CoV) infection. Arch. Med. Res. 2020, 51, 384–387. [Google Scholar] [CrossRef]
- Karkhanei, B.; Talebi Ghane, E.; Mehri, F. Evaluation of oxidative stress level: Total antioxidant capacity, total oxidant status and glutathione activity in patients with COVID-19. New Microbes New Infect. 2021, 42, 100897. [Google Scholar] [CrossRef] [PubMed]
- Mehri, F.; Rahbar, A.H.; Ghane, E.T.; Souri, B.; Esfahani, M. Changes in oxidative markers in COVID-19 patients. Arch. Med. Res. 2021, 52, 843–849. [Google Scholar] [CrossRef] [PubMed]
- Simmons, S.; Erfinanda, L.; Bartz, C.; Kuebler, W.M. Novel mechanisms regulating endothelial barrier function in the pulmonary microcirculation. J. Physiol. 2019, 597, 997–1021. [Google Scholar] [CrossRef] [PubMed]
- Reshi, M.L.; Su, Y.C.; Hong, J.R. RNA Viruses: ROS-mediated cell death. Int. J. Cell Biol. 2014, 2014, 467452. [Google Scholar] [CrossRef] [PubMed]
- Hendricks, K.; To, E.; Vlahos, R.; Broughton, B.; Peshavariya, H.; Selemidis, S. Influenza A virus causes vascular endothelial cell oxidative stress via NOX2 oxidase. Eur. Respir. J. 2016, 48, PA3967. [Google Scholar]
- Khomich, O.A.; Kochetkov, S.N.; Bartosch, B.; Ivanov, A.V. Redox biology of respiratory viral infections. Viruses 2018, 10, 392. [Google Scholar] [CrossRef]
- Abdi, A.; Jalilian, M.; Sarbarzeh, P.A.; Vlaisavljevic, Z. Diabetes and COVID-19: A systematic review on the current evidences. Diabetes Res. Clin. Pract. 2020, 166, 108347. [Google Scholar] [CrossRef] [PubMed]
- Mihalopoulos, M.; Dogra, N.; Mohamed, N.; Badani, K.; Kyprianou, N. COVID-19 and Kidney Disease: Molecular Determinants and Clinical Implications in Renal Cancer. Eur. Urol. Focus 2020, 6, 1086–1096. [Google Scholar] [CrossRef]
- Bektemur, G.; Bozali, K.; Colak, S.; Aktas, S.; Metin Guler, E. Oxidative stress, DNA damage, and inflammation in COVID-19 patients. North. Clin. Istanb. 2023. (ahead of print). [Google Scholar] [CrossRef]
- Mihaljevic, O.; Zivancevic-Simonovic, S.; Cupurdija, V.; Marinkovic, M.; Tubic Vukajlovic, J.; Markovic, A.; Stanojevic-Pirkovic, M.; Milosevic-Djordjevic, O. DNA damage in peripheral blood lymphocytes of severely ill COVID-19 patients in relation to inflammatory markers and parameters of hemostasis. Mutagenesis 2022, 37, 203–212. [Google Scholar] [CrossRef]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk factors associated with acute respiratory distress syndrome and death in patients with Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef]
- Sanders, O.D.; Rajagopal, L.; Rajagopal, J.A. The oxidatively damaged DNA and amyloid-β oligomer hypothesis of Alzheimer’s disease. Free Radic. Biol. Med. 2022, 179, 403–412. [Google Scholar] [CrossRef]
- Renaudin, X. Reactive oxygen species and DNA damage response in cancer. Int. Rev. Cell Mol. Biol. 2021, 364, 139–161. [Google Scholar] [PubMed]
- Singh, N.P.; McCoy, M.T.; Tice, R.R.; Schneider, E.L. A simple technique for quantitation of low levels of DNA damage in individual cells. Exp. Cell Res. 1988, 175, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Collins, A.R. The comet assay for DNA damage and repair: Principles, applications, and limitations. Mol. Biotechnol. 2004, 26, 249–261. [Google Scholar] [CrossRef]
- Boyum, A. Isolation of lymphocytes, granulocytes and macrophages. Scand. J. Immunol. 1976, 5, 9–15. [Google Scholar] [CrossRef]
- Ntyonga-Pono, M.P. COVID-19 infection and oxidative stress: An under-explored approach for prevention and treatment? Pan Afr. Med. J. 2020, 35, 12. [Google Scholar] [CrossRef]
- Camini, F.C.; da Silva Caetano, C.C.; Almeida, L.T.; de Brito Magalhães, C.L. Implications of oxidative stress on viral pathogenesis. Arch. Virol. 2017, 162, 907–917. [Google Scholar] [CrossRef]
- Gavriatopoulou, M.; Korompoki, E.; Fotiou, D.; Ntanasis-Stathopoulos, I.; Psaltopoulou, T.; Kastritis, E.; Terpos, E.; Dimopoulos, M.A. Organ-specific manifestations of COVID-19 infection. Clin. Exp. Med. 2020, 20, 493–506. [Google Scholar] [CrossRef]
- Huang, L.; Zhao, P.; Tang, D.; Zhu, T.; Han, R.; Zhan, C.; Liu, W.; Zeng, H.; Tao, Q.; Xia, L. Cardiac Involvement in Patients Recovered From COVID-2019 Identified Using Magnetic Resonance Imaging. JACC Cardiovasc. Imaging 2020, 13, 2330–2339. [Google Scholar] [CrossRef]
- Martins-Filho, P.R.; Tavares, C.S.S.; Santos, V.S. Factors associated with mortality in patients with COVID-19. A quantitative evidence synthesis of clinical and laboratory data. Eur. J. Intern. Med. 2020, 76, 97–99. [Google Scholar] [CrossRef]
- Liao, F.L.; Peng, D.H.; Chen, W.; Hu, H.N.; Tang, P.; Liu, Y.Y.; Luo, Y.; Yao, T. Evaluation of serum hepatic enzyme activities in different COVID-19 phenotypes. J. Med. Virol. 2021, 93, 2365–2373. [Google Scholar] [CrossRef] [PubMed]
- Smail, S.W.; Babaei, E.; Amin, K. Hematological, Inflammatory, Coagulation, and Oxidative/Antioxidant Biomarkers as Predictors for Severity and Mortality in COVID-19: A Prospective Cohort-Study. Int. J. Gen. Med. 2023, 16, 565–580. [Google Scholar] [CrossRef] [PubMed]
- Yaghoubi, N.; Youssefi, M.; Jabbari Azad, F.; Farzad, F.; Yavari, Z.; Zahedi Avval, F. Total antioxidant capacity as a marker of severity of COVID-19 infection: Possible prognostic and therapeutic clinical application. J. Med. Virol. 2022, 94, 1558–1565. [Google Scholar] [CrossRef]
- Schönrich, G.; Raftery, M.J.; Samstag, Y. Devilishly radical NETwork in COVID-19: Oxidative stress, neutrophil extracellular traps (NETs), and T cell suppression. Adv. Biol. Regul. 2020, 77, 100741. [Google Scholar] [CrossRef] [PubMed]
- Kumar, D.S.; Hanumanram, G.; Suthakaran, P.K.; Mohanan, J.; Nair, L.D.V.; Rajendran, K. Extracellular Oxidative Stress Markers in COVID-19 Patients with Diabetes as Co-Morbidity. Clin. Pract. 2022, 12, 168–176. [Google Scholar] [CrossRef] [PubMed]
- Smeyne, R.J.; Eells, J.B.; Chatterjee, D.; Byrne, M.; Akula, S.M.; Sriramula, S.; O’Rourke, D.P.; Schmidt, P. COVID-19 Infection Enhances Susceptibility to Oxidative Stress-Induced Parkinsonism. Mov. Disord. 2022, 37, 1394–1404. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 10223, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Monserrat, J.; Gómez-Lahoz, A.; Ortega, M.A.; Sanz, J.; Muñoz, B.; Arévalo-Serrano, J.; Rodríguez, J.M.; Gasalla, J.M.; Gasulla, Ó.; Arranz, A.; et al. Role of Innate and Adaptive Cytokines in the Survival of COVID-19 Patients. Int. J. Mol. Sci. 2022, 23, 10344. [Google Scholar] [CrossRef] [PubMed]
- Tepebaşı, M.Y.; İlhan, İ.; Temel, E.N.; Sancer, O.; Öztürk, Ö. Investigation of inflammation, oxidative stress, and DNA damage in COVID-19 patients. Cell Stress Chaperones 2023, 28, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Pánico, P.; Ostrosky-Wegman, P.; Salazar, A.M. The potential role of COVID-19 in the induction of DNA damage. Mutat. Res. Rev. Mutat. Res. 2022, 789, 108411. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Patients with COVID-19 (n = 50) | Healthy Controls (n = 50) |
|---|---|---|
| Age (years) * | 43.58 ± 16.17 (18–73) | 41.16 ± 14.28 (18–75) |
| Body mass index * | 25.23 ± 3.22 (19.53–31.59) | 25.99 ± 3.62 (18.83–34.09) |
| Gender (n (%)) | ||
| Female | 22 (44%) | 22 (44%) |
| Male | 28 (56%) | 28 (56%) |
| Current cigarette smoker (n (%)) | ||
| Yes | 17 (34%) | 20 (40%) |
| No | 33 (66%) | 30 (60%) |
| Total pack-years of smoking * | 8.23 ± 7.49 (0.20–25.0) | 11.72 ± 19.84 (0.50–30.0) |
| Symptoms (n (%)) | ||
| Fever | 20 (40%) | - |
| Cough | 26 (52%) | - |
| Respiratory distress | 12 (24%) | - |
| Hospitalization (n (%)) # | ||
| Yes (patients with severe symptoms) | 12 (24%) | - |
| No (patients with mild symptoms) | 38 (76%) | - |
| Hemogram | Patients with COVID-19 | Healthy Controls (n = 40) | ||
|---|---|---|---|---|
| All Patients (n = 50) | Patients with Severe Symptoms (n = 12) | Patients with Mild Symptoms (n = 38) | ||
| WBCs (103/µL) | 7.00 ± 2.14 (3.03–11.56) | 6.87 ± 2.32 (3.22–10.8) | 7.04 ± 2.08 (3.03–11.56) | 5.72 ± 1.85 (3.2–9.8) |
| RBCs (106/µL) | 4.66 ± 0.81 (2.91–8.40) | 4.59 ± 0.64 (3.33–5.60) | 4.69 ± 0.85 (2.91–8.40) | 4.33 ± 0.40 (3.54–5.21) |
| Hg (g/dL) | 13.52 ± 1.66 (8.3–16.2) | 12.89 ± 2.07 (9.40–16.2) | 13.72 ± 1.46 (8.30–16.0) | 13.89 ± 0.79 (12.5–15.7) |
| MCV (fL) | 87.62 ± 4.96 (75.7–98.2) | 86.05 ± 3.88 (78.4–92.4) | 88.12 ± 5.15 (75.7–98.2) | 89.35 ± 3.51 (82.6–95.2) |
| MCH (pg) | 29.14 ± 2.24 (24.5–33.0) | 28.02 ± 1.93 (24.5–31.4) | 29.49 ± 2.22 (24.5–33.0) | 30.83 ± 1.49 (28.0–34.0) |
| MCHC (g/dL) | 33.23 ± 1.51 (28.6–35.8) | 32.35 ± 1.49 (30.3–35.8) | 33.51 ± 1.41 (28.6–35.6) | 33.37 ± 1.42 (30.2–36.7) |
| HCT (%) | 41.18 ± 4.59 (24.4–49.4) | 40.51 ± 5.55 (29.1–49.4) | 41.39 ± 4.23 (24.4–48.8) | 40.86 ± 2.58 (36.5–47.3) |
| PLT (103/µL) | 261.2 ± 89.9 (99–526) | 301.50 ± 116.60 (138–526) * | 248.47 ± 75.20 (99–432) | 220.86 ± 69.71 (112–372) |
| RDW–SD (fL) | 41.02 ± 3.24 (35.2–57.0) | 40.48 ± 2.22 (37.4–45.5) | 41.20 ± 3.48 (35.2–57.2) | 41.01 ± 2.19 (35.9–46.1) |
| PDW (fL) | 15.93 ± 0.63 (14.3–17.6) | 16.20 ± 0.46 (15.3–16.7) | 15.85 ± 0.65 (14.3–17.6) | 15.84 ± 0.86 (12.4–16.9) |
| MPV (fL) | 9.70 ± 1.28 (6.11–14.4) | 10.01 ± 1.14 (8.5–12.4) | 9.60 ± 1.31 (6.11–14.4) | 9.36 ± 1.01 (7.3–11.3) |
| PCT (103/µL) | 0.22 ± 0.08 (0.02–0.37) | 0.22 ± 0.07 (0.10–0.31) | 0.22 ± 0.08 (0.02–0.37) | 0.26 ± 0.05 (0.13–0.35) |
| NEU (103/µL) | 3.77 ± 1.64 (0.1–8.52) | 3.03 ± 1.09 (1.93–5.45) | 4.01 ± 1.72 (0.10–8.52) | 4.18 ± 1.04 (2.38–6.24) |
| MO (103/µL) | 0.44 ± 0.27 (0.02–1.10) | 0.35 ± 0.26 (0.08–1.10) | 0.47 ± 0.27 (0.02–1.01) | 0.47 ± 0.28 (0.10–1.10) |
| LYM (103/µL) | 1.39 ± 0.78 (0.33–3.56) * | 0.81 ± 0.34 (0.35–1.44) *,# | 1.57 ± 0.79 (0.33–3.56) | 2.65 ± 0.69 (1.01–4.10) |
| EOS (103/µL) | 0.09 ± 0.11 (0.0–0.43) * | 0.02 ± 0.04 (0.0–0.16) *,# | 0.11 ± 0.11 (0.0–0.43) | 0.18 ± 0.10 (0.0–0.40) |
| BASO (103/µL) | 0.02 ± 0.01 (0.0–0.04) | 0.02 ± 0.01 (0.0–0.03) | 0.02 ± 0.01 (0.0–0.04) | 0.03 ± 0.05 (0.01–0.30) |
| Parameter | Patients with COVID-19 | Healthy Controls (n = 50) | ||
|---|---|---|---|---|
| All Patients (n = 50) | Patients with Severe Symptoms (n = 12) | Patients with Mild Symptoms (n = 38) | ||
| CRP (mg/L) | 37.03 ± 58.44 (0.20–250) * | 116.38 ± 71.41 (26.0–250) *,# | 11.97 ± 16.34 (0.20–66.8) * | 2.72 ± 2.01 (0.12–9.2) |
| Ferritin (ng/mL) | 328.8 ± 396.2 (12.54–1893) * | 738.1 ± 581.1 (67.2–1893) *,# | 199.6 ± 174.0 (12.54–598.5) * | 69.47 ± 48.83 (12.01–243.1) |
| d-Dimer (µg/mL) | 578.7 ± 721.8 (85–4360) * | 1356 ± 1117 (265–4360) *,# | 333.1 ± 200.1 (85–983) | 232.7 ± 109.8 (65–456) |
| Fibrinogen (mg/dL) | 369.2 ± 169.1 (38–870) * | 486.2 ± 204.2 (98–870) * | 332.2 ± 137.0 (38–678) | 260.6 ± 82.3 (78–412) |
| AST (U/dL) | 27.64 ± 14.50 (13–84) | 38.17 ± 20.79 (19–84) * | 24.32 ± 9.70 (13–60) | 21.84 ± 5.58 (10–36) |
| ALT (U/dL) | 23.20 ± 12.26 (9–92) | 23.17 ± 8.15 (13–39) | 23.21 ± 13.30 (9–92) | 18.40 ± 4.31 (11–30) |
| Parameter | Patients with COVID-19 | Healthy Controls (n = 50) | ||
|---|---|---|---|---|
| All Patients (n = 50) | Patients with Severe Symptoms (n = 12) | Patients with Mild Symptoms (n = 38) | ||
| MDA (nmol/L) | 6.27 ± 7.76 (0.02–32.68) * | 13.88 ± 9.87 (2.21–32.68) *,# | 3.87 ± 4.94 (0.02–25.67) * | 1.78 ± 1.05 (0.28–5.94) |
| GSH (ng/mL) | 1.30 ± 1.33 (0.01–5.37) | 1.55 ± 1.64 (0.01–5.09) | 1.22 ± 1.20 (0.04–5.37) | 1.29 ± 1.19 (0.01–5.36) |
| GPx (µU/mL) | 48.66 ± 62.80 (0.27–277.56) * | 103.00 ± 82.14 (5.71–277.56) *,# | 31.50 ± 42.80 (0.27–217.20) * | 10.75 ± 9.18 (0.24–38.15) |
| SOD (ng/mL) | 10.44 ± 13.66 (0.01–54.43) * | 22.11 ± 16.98 (3.31–54.43) *,# | 6.76 ± 9.89 (0.01–50.88) * | 2.60 ± 1.64 (0.01–7.62) |
| CAT (KU/L) | 69.77 ± 75.14 (5.69–265.71) * | 133.96 ± 84.53 (18.37–265.71) *,# | 49.61 ± 58.98 (5.69–255.65) * | 19.65 ± 10.22 (7.65–65.88) |
| IL-17 (ng/L) | 52.29 ± 66.84 (4.08–316.09) * | 113.96 ± 88.40 (16.01–316.09) *,# | 32.82 ± 42.79 (4.08–241.36) * | 14.81 ± 13.66 (4.57–99.62) |
| IL-23 (ng/L) | 40.34 ± 53.78 (0.43–210.14) * | 89.62 ± 62.97 (11.96–178.81) *,# | 24.77 ± 39.29 (0.43–210.14) * | 10.57 ± 4.69 (3.69–28.12) |
| IL-27 (ng/L) | 136.8 ± 156.6 (20.37–526.22) * | 292.73 ± 181.20 (32.63–512.52) *,# | 87.52 ± 108.50 (20.37–526–22) * | 35.19 ± 17.33 (10.04–90.93) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Basaran, M.M.; Hazar, M.; Aydın, M.; Uzuğ, G.; Özdoğan, İ.; Pala, E.; Aydın Dilsiz, S.; Basaran, N. Effects of COVID-19 Disease on DNA Damage, Oxidative Stress and Immune Responses. Toxics 2023, 11, 386. https://doi.org/10.3390/toxics11040386
Basaran MM, Hazar M, Aydın M, Uzuğ G, Özdoğan İ, Pala E, Aydın Dilsiz S, Basaran N. Effects of COVID-19 Disease on DNA Damage, Oxidative Stress and Immune Responses. Toxics. 2023; 11(4):386. https://doi.org/10.3390/toxics11040386
Chicago/Turabian StyleBasaran, M. Mert, Merve Hazar, Mehtap Aydın, Gülsüm Uzuğ, İlkima Özdoğan, Emin Pala, Sevtap Aydın Dilsiz, and Nursen Basaran. 2023. "Effects of COVID-19 Disease on DNA Damage, Oxidative Stress and Immune Responses" Toxics 11, no. 4: 386. https://doi.org/10.3390/toxics11040386
APA StyleBasaran, M. M., Hazar, M., Aydın, M., Uzuğ, G., Özdoğan, İ., Pala, E., Aydın Dilsiz, S., & Basaran, N. (2023). Effects of COVID-19 Disease on DNA Damage, Oxidative Stress and Immune Responses. Toxics, 11(4), 386. https://doi.org/10.3390/toxics11040386