
A Review of Dietary Intake of Acrylamide in Humans

 ,
, 
 and
and
Abstract
:1. Introduction
2. Methods
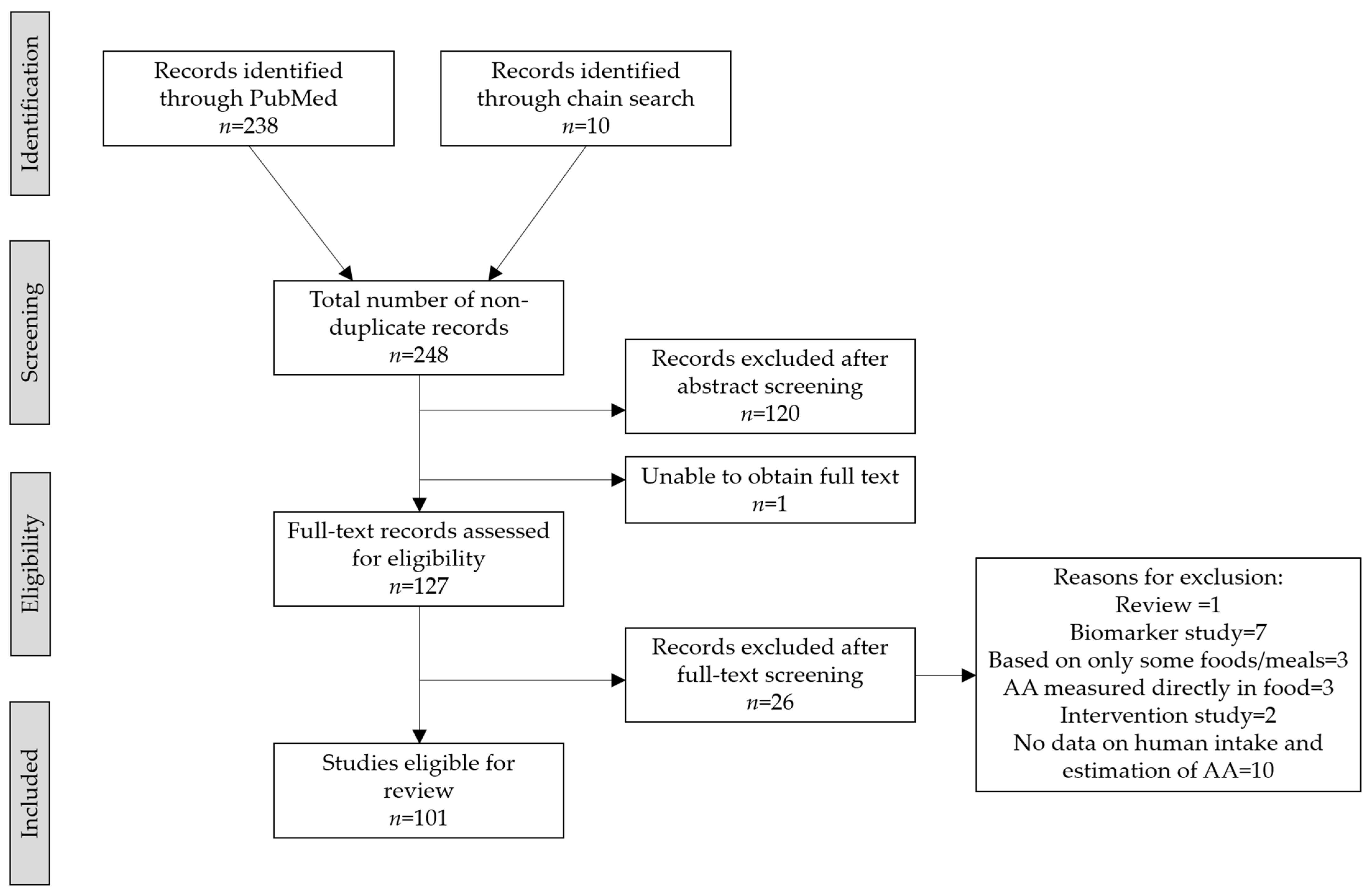
2.1. Search Strategy
2.2. Selection and Data Collection Process
2.3. Synthesis Methods
3. Results
3.1. Demography of Study Populations
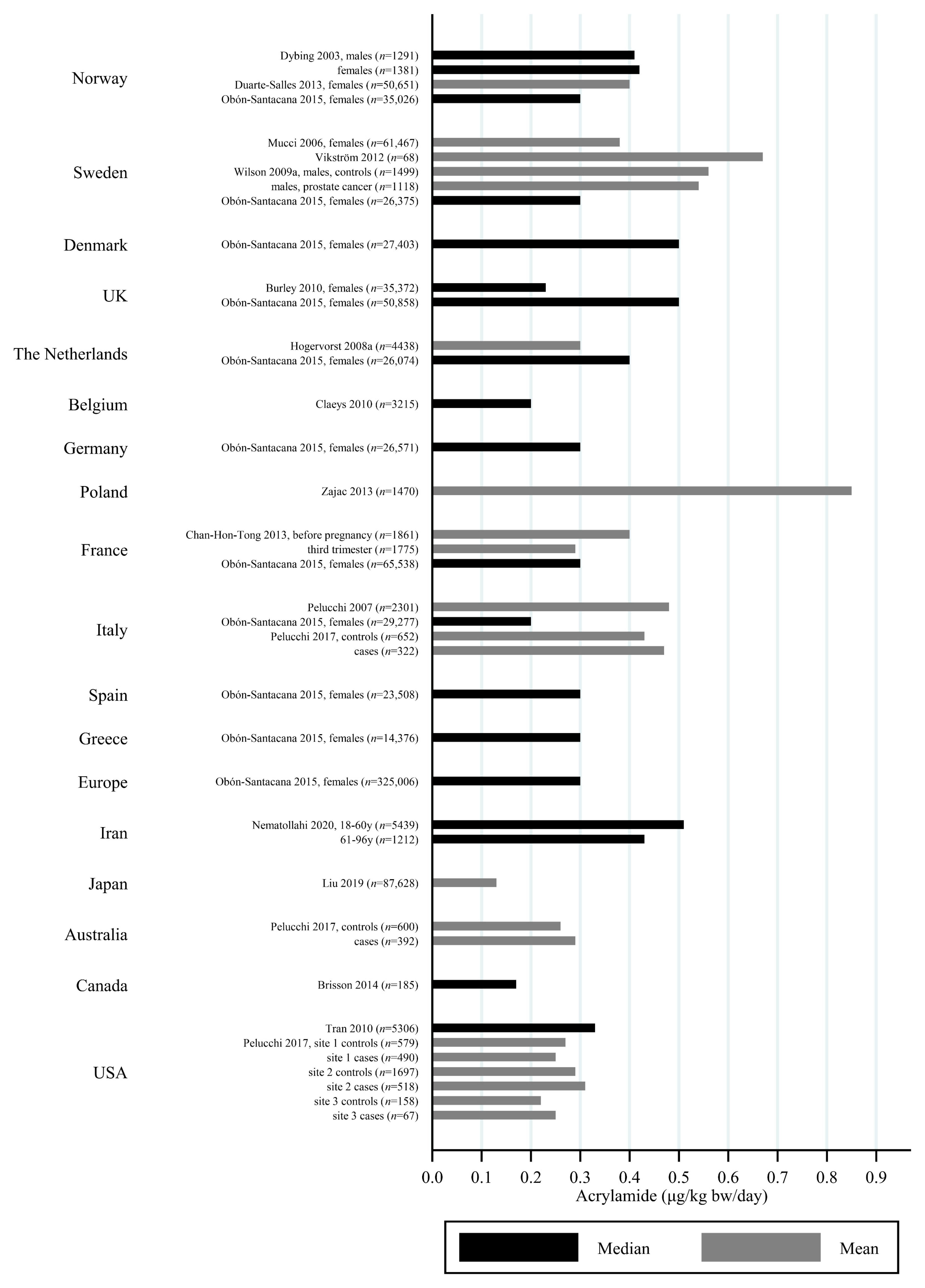
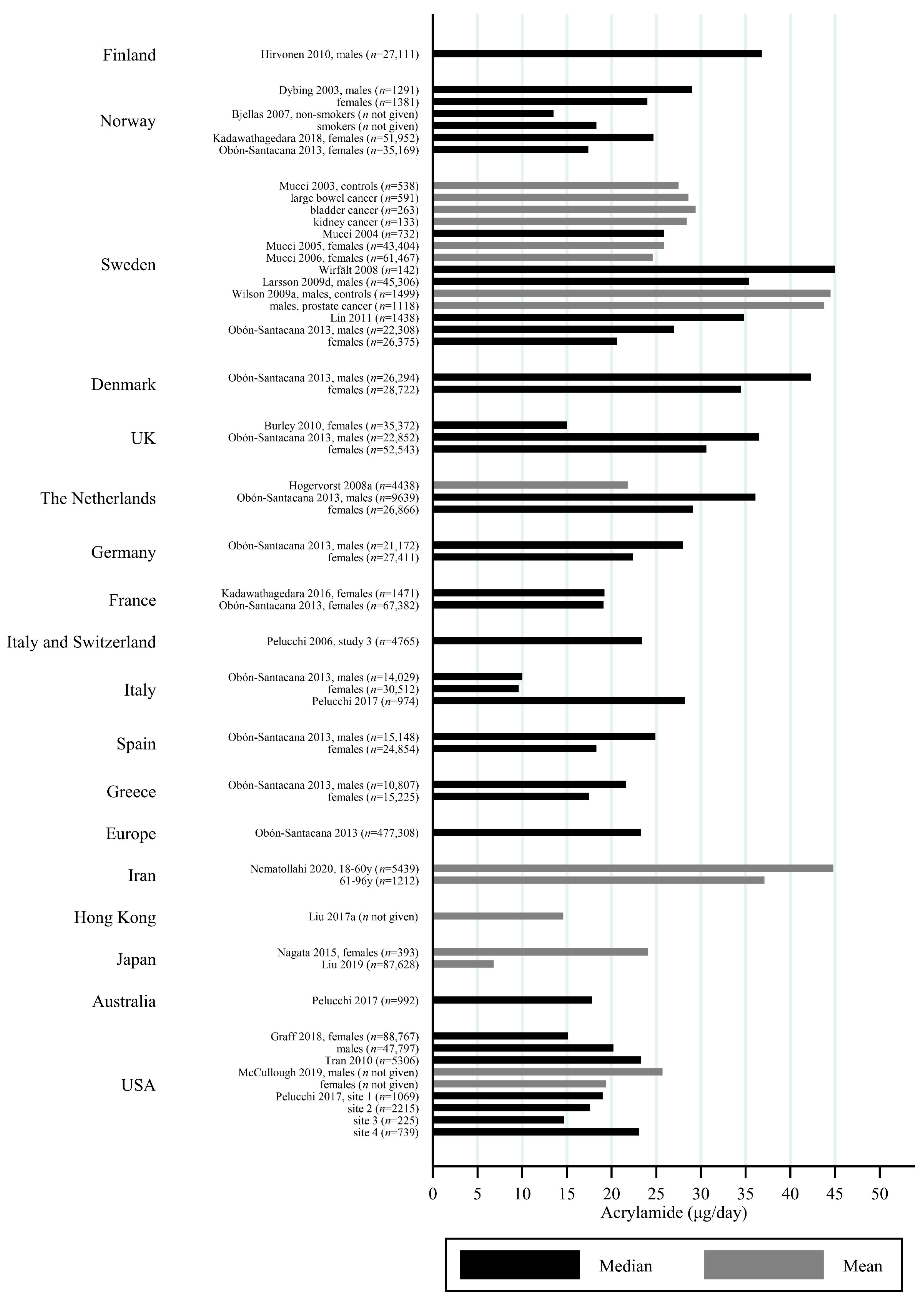
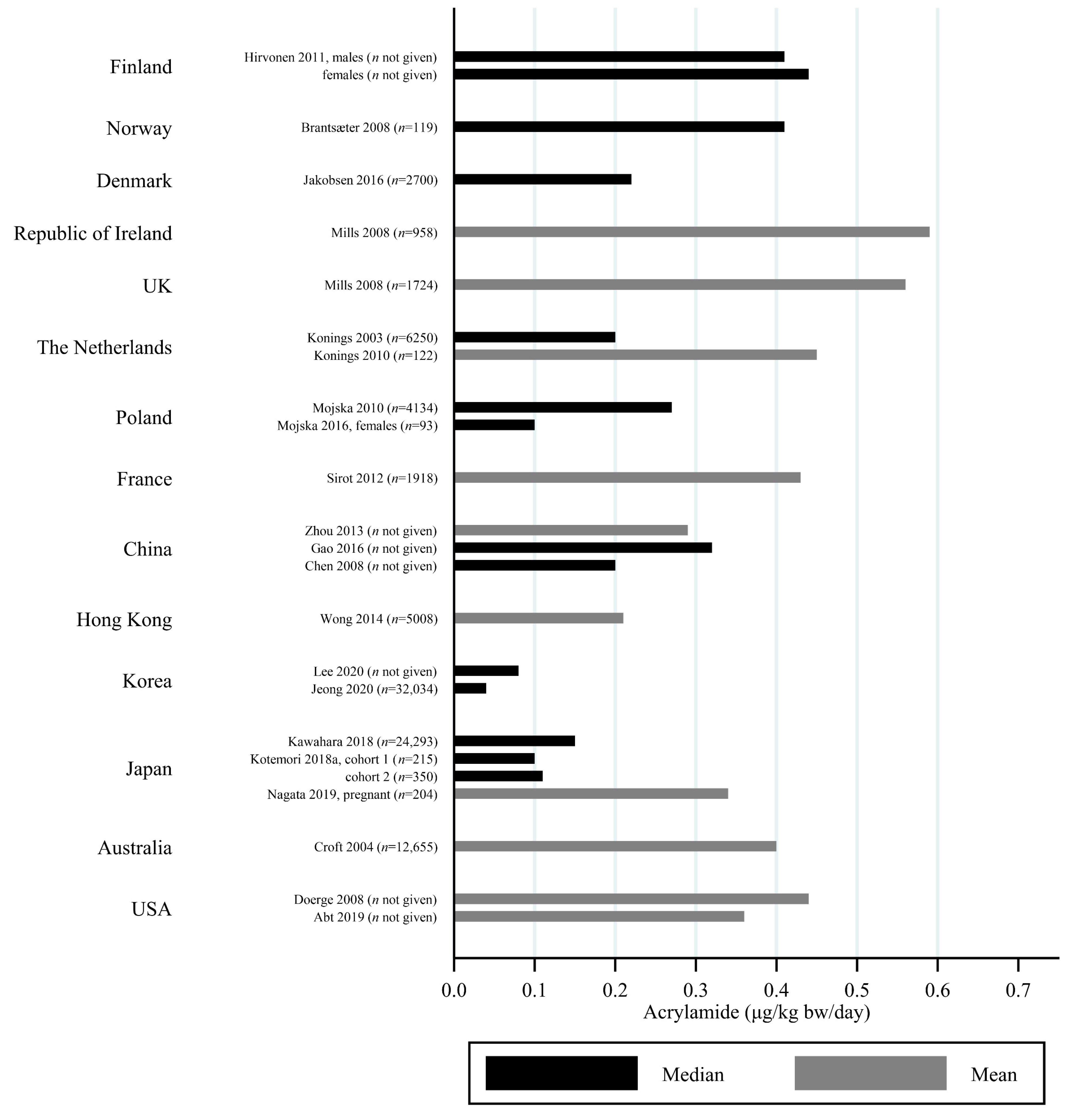
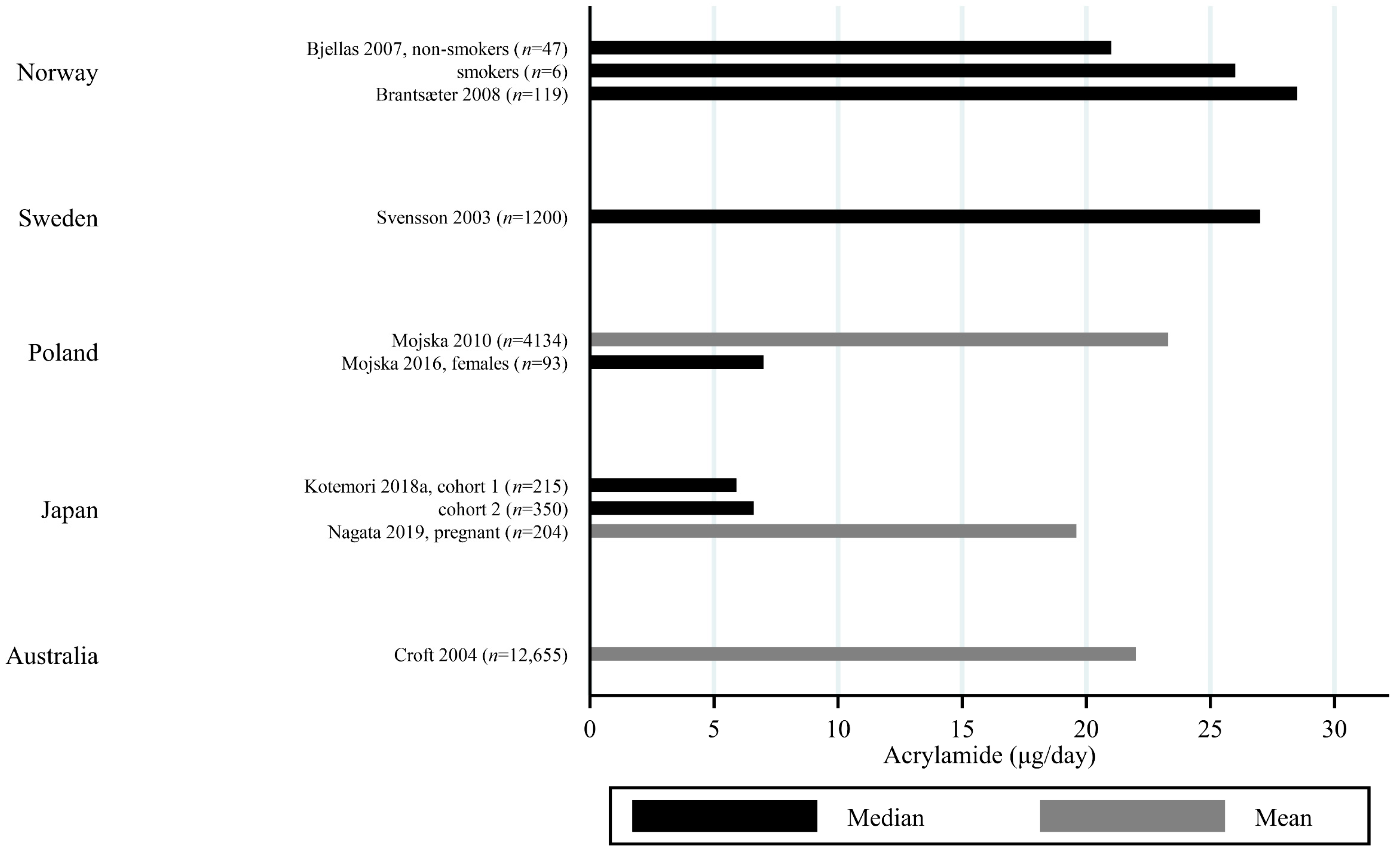
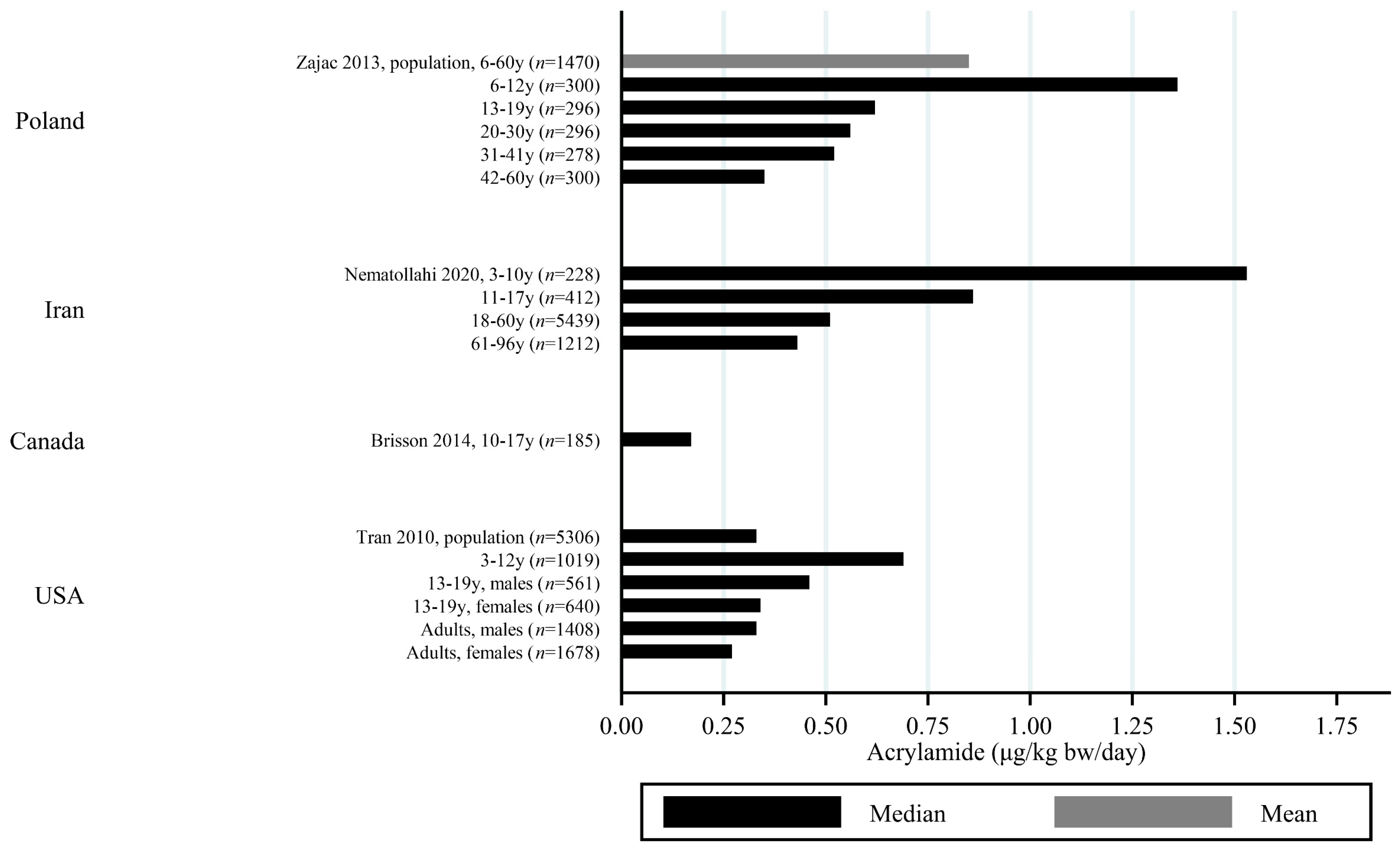
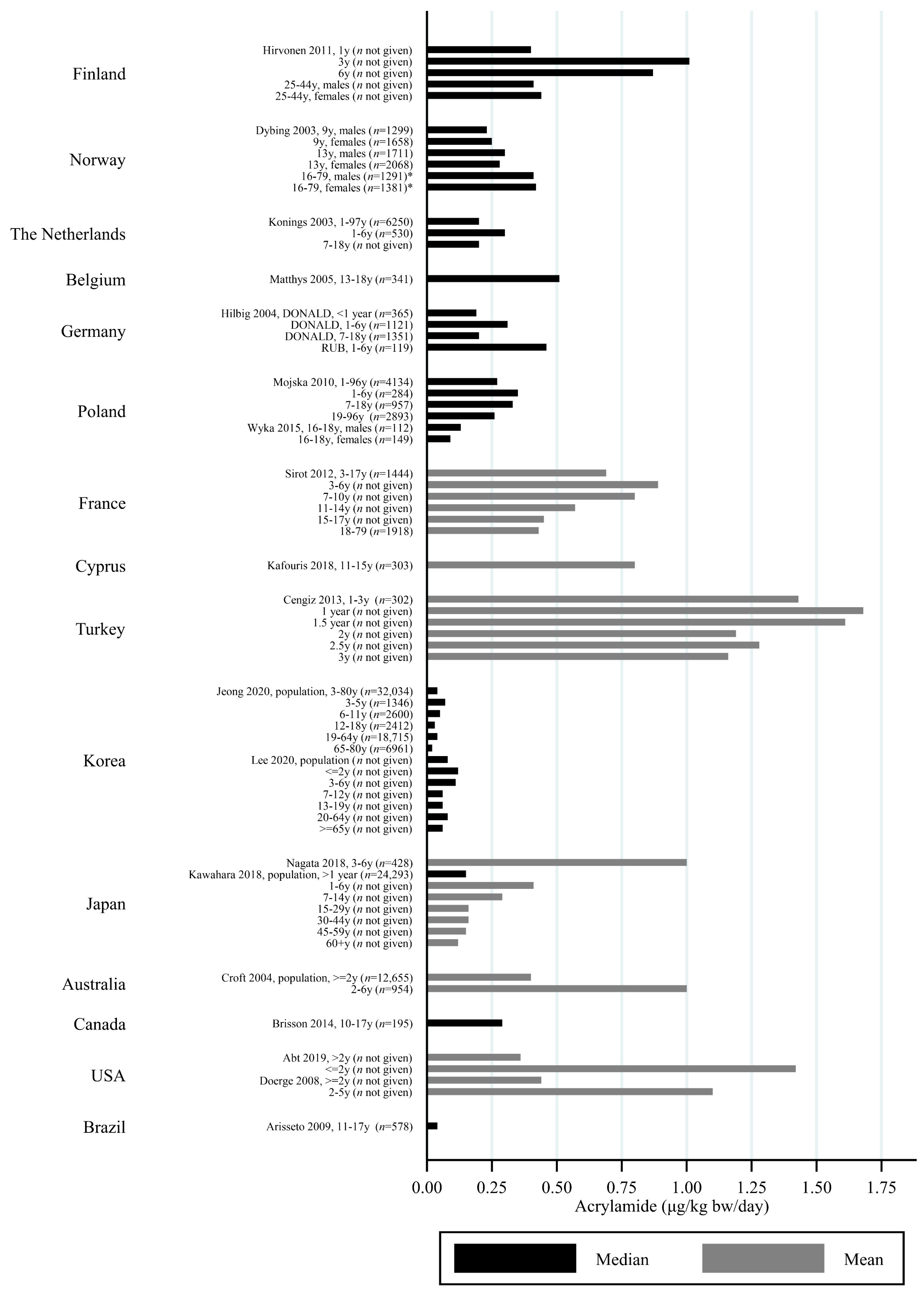
3.2. Estimated AA Intakes across Countries and Age-Groups
3.3. Dietary Assessment Methods
4. Discussion
4.1. Country-Specific Differences in AA Intake and Food Groups Contributing to the Total AA Intake
4.2. Age-Related Differences in AA Intake and Food Groups Contributing to the Total AA Intake
4.3. DQs Compared to DRs
4.4. Limitations of DQs and DRs for Studies Estimating Total Dietary AA Intake
4.5. DQs and DRs Compared to Other Methods of Estimating Dietary AA Intake
4.6. Limitations to Our Review
4.7. Perspectives
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tareke, E.; Rydberg, P.; Karlsson, P.; Eriksson, S.; Törnqvist, M. Analysis of Acrylamide, a Carcinogen Formed in Heated Foodstuffs. J. Agric. Food Chem. 2002, 50, 4998–5006. [Google Scholar] [CrossRef] [PubMed]
- Mottram, D.S.; Wedzicha, B.L.; Dodson, A.T. Acrylamide is formed in the Maillard reaction. Nat. Cell Biol. 2002, 419, 448–449. [Google Scholar] [CrossRef] [PubMed]
- Stadler, R.H.; Blank, I.; Varga, N.; Robert, F.; Hau, J.; Guy, P.A.; Robert, M.-C.; Riediker, S. Acrylamide from Maillard reaction products. Nat. Cell Biol. 2002, 419, 449–450. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization International Agency for Research on Cancer. Some Industrial Chemicals. In IARC Monograhs on the Evaluation of Carcinogenic Risks to Humans; IARC: Lyon, France, 1994. [Google Scholar]
- EFSA. Scientific Opinion on acrylamide in food. EFSA J. 2015, 13. [Google Scholar] [CrossRef] [Green Version]
- Government of Canada. Sampling Plan for the First Phase of the Acrylamide Monitoring Program 2009 [updated August 2009]. Available online: https://www.canada.ca/en/health-canada/services/food-nutrition/food-safety/chemical-contaminants/food-processing-induced-chemicals/acrylamide/sampling-plan-first-phase-acrylamide-monitoring-program-chemical-contaminants.html (accessed on 27 April 2021).
- U.S. Food and Drug Administration. Survey Data on Acrylamide in Food: Total Diet Study Results 2018 [updated 25 January 2018]. Available online: https://www.fda.gov/food/chemicals/survey-data-acrylamide-food-total-diet-study-results (accessed on 27 April 2021).
- Food Standards Australia New Zealand. 24th Australian Total Diet Study; FSANZ: Canberra, NSW, Australia; Wellington, New Zealand, 2014.
- Cressey, P.; Thomson, B.; Ashworth, M.; Grounds, P.; McGill, E. Acrylamide in New Zealand Food and Updated Exposure Assess-ment; Ministry of Agriculture and Forestry: Wellington, New Zealand, 2012.
- FAO/WHO. Safety Evaluation of Certain Contaminants in Food; Prepared by the Seventy-Second Meeting of the Joint FAO/WHO Expert Committee on Food Additives (JECFA); World Health Organization: Geneva, Switzerland; Food and Agriculture Organization of the United Nations: Rome, Italy, 2006. [Google Scholar]
- Sörgel, F.; Weissenbacher, R.; Kinzig-Schippers, M.; Hofmann, A.; Illauer, M.; Skott, A.; Landersdorfer, C. Acrylamide: Increased Concentrations in Homemade Food and First Evidence of Its Variable Absorption from Food, Variable Metabolism and Placental and Breast Milk Transfer in Humans. Chemotherapy 2002, 48, 267–274. [Google Scholar] [CrossRef] [Green Version]
- Elmore, J.S.; Koutsidis, G.; Dodson, A.T.; Mottram, N.S.; Wedzicha, B.L. The Effect of Cooking on Acrylamide and Its Precursors in Potato, Wheat and Rye. In Chemistry and Biology of Pteridines and Folates; Springer Science and Business Media LLC: Berlin/Heidelberg, Germany, 2006; Volume 561, pp. 255–269. [Google Scholar]
- Stadler, R.H. Acrylamide Formation in Different Foods and Potential Strategies for Reduction; Springer: Boston, MA, USA, 2005. [Google Scholar]
- Ishihara, K.; Matsunaga, A.; Miyoshi, T.; Nakamura, K.; Nakayama, T.; Ito, S.; Koga, H. Formation of Acrylamide in a Processed Food Model System, and Examination of Inhibitory Conditions. J. Food Hyg. Soc. Jpn. 2005, 46, 33–39. [Google Scholar] [CrossRef] [Green Version]
- Pedreschi, F.; Mariotti, M.S.; Granby, K. Current issues in dietary acrylamide: Formation, mitigation and risk assessment. J. Sci. Food Agric. 2013, 94, 9–20. [Google Scholar] [CrossRef]
- Lachenmeier, D.W.; Schwarz, S.; Teipel, J.; Hegmanns, M.; Kuballa, T.; Walch, S.G.; Breitling-Utzmann, C.M. Potential Antagonistic Effects of Acrylamide Mitigation during Coffee Roasting on Furfuryl Alcohol, Furan and 5-Hydroxymethylfurfural. Toxics 2018, 7, 1. [Google Scholar] [CrossRef] [Green Version]
- FAO/WHO. Safety Evaluation of Certain Contaminants in Food; Prepared by the Seventy-Second Meeting of the Joint FAO/WHO Expert Committee on Food Additives (JECFA); World Health Organization: Geneva, Switzerland; Food and Agriculture Organization of the United Nations: Rome, Italy, 2011. [Google Scholar]
- Pelucchi, C.; Bosetti, C.; Galeone, C.; La Vecchia, C. Dietary acrylamide and cancer risk: An updated meta-analysis. Int. J. Cancer 2015, 136, 2912–2922. [Google Scholar] [CrossRef]
- Riboldi, B.P.; Vinhas Álvaro, M.; Moreira, J.D. Risks of dietary acrylamide exposure: A systematic review. Food Chem. 2014, 157, 310–322. [Google Scholar] [CrossRef]
- Virk-Baker, M.K.; Nagy, T.R.; Barnes, S.; Groopman, J. Dietary acrylamide and human cancer: A systematic review of literature. Nutr. Cancer 2014, 66, 774–790. [Google Scholar] [CrossRef] [Green Version]
- Duarte-Salles, T.; Von Stedingk, H.; Granum, B.; Gützkow, K.B.; Rydberg, P.; Törnqvist, M.; Mendez, M.A.; Brunborg, G.; Brantsæter, A.L.; Meltzer, H.M.; et al. Dietary Acrylamide Intake during Pregnancy and Fetal Growth—Results from the Norwegian Mother and Child Cohort Study (MoBa). Environ. Health Perspect. 2013, 121, 374–379. [Google Scholar] [CrossRef]
- Kadawathagedara, M.; Botton, J.; De Lauzon-Guillain, B.; Meltzer, H.M.; Alexander, J.; Brantsaeter, A.L.; Haugen, M.; Papadopoulou, E. Dietary acrylamide intake during pregnancy and postnatal growth and obesity: Results from the Norwegian Mother and Child Cohort Study (MoBa). Environ. Int. 2018, 113, 325–334. [Google Scholar] [CrossRef]
- Kadawathagedara, M.; Tong, A.C.H.; Heude, B.; Forhan, A.; Charles, M.A.; Sirot, V.; Botton, J. The EDEN mother-child cohort study group Dietary acrylamide intake during pregnancy and anthropometry at birth in the French EDEN mother-child cohort study. Environ. Res. 2016, 149, 189–196. [Google Scholar] [CrossRef]
- Chan-Hon-Tong, A.; Charles, M.A.; Forhan, A.; Heude, B.; Sirot, V. Exposure to food contaminants during pregnancy. Sci. Total. Environ. 2013, 458–460, 27–35. [Google Scholar] [CrossRef]
- Nagata, C.; Konishi, K.; Wada, K.; Tamura, T.; Goto, Y.; Koda, S.; Mizuta, F.; Iwasa, S. Maternal Acrylamide Intake during Pregnancy and Sex Hormone Levels in Maternal and Umbilical Cord Blood and Birth Size of Offspring. Nutr. Cancer 2018, 71, 77–82. [Google Scholar] [CrossRef]
- Brantsæter, A.L.; Haugen, M.; De Mul, A.; Bjellaas, T.; Becher, G.; Van Klaveren, J.; Alexander, J.; Meltzer, H.M. Exploration of different methods to assess dietary acrylamide exposure in pregnant women participating in the Norwegian Mother and Child Cohort Study (MoBa). Food Chem. Toxicol. 2008, 46, 2808–2814. [Google Scholar] [CrossRef]
- Kotemori, A.; Ishihara, J.; Nakadate, M.; Sawada, N.; Iwasaki, M.; Sobue, T.; Tsugane, S. Validity of a Self-administered Food Frequency Questionnaire for the Estimation of Acrylamide Intake in the Japanese Population: The JPHC FFQ Validation Study. J. Epidemiol. 2018, 28, 482–487. [Google Scholar] [CrossRef] [Green Version]
- Wirfält, E.; Paulsson, B.; Törnqvist, M.; Axmon, A.; Hagmar, L.; Wirf, E. Associations between estimated acrylamide intakes, and hemoglobin AA adducts in a sample from the Malmö Diet and Cancer cohort. Eur. J. Clin. Nutr. 2007, 62, 314–323. [Google Scholar] [CrossRef]
- Liu, R.; Sobue, T.; Kitamura, T.; Kitamura, Y.; Ishihara, J.; Kotemori, A.; Zha, L.; Ikeda, S.; Sawada, N.; Iwasaki, M.; et al. Dietary Acrylamide Intake and Risk of Esophageal, Gastric, and Colorectal Cancer: The Japan Public Health Center-based Prospective Study. Cancer Epidemiol. Biomark. Prev. 2019, 28, 1461–1468. [Google Scholar] [CrossRef]
- Nematollahi, A.; Kamankesh, M.; Hosseini, H.; Ghasemi, J.; Hosseini-Esfahani, F.; Mohammadi, A.; Khaneghah, A.M. Acrylamide content of collected food products from Tehran’s market: A risk assessment study. Environ. Sci. Pollut. Res. 2020, 27, 30558–30570. [Google Scholar] [CrossRef]
- Jeong, H.; Hwang, S.; Kwon, H. Survey for acrylamide in processed foods from Korean market and individual exposure estimation using a non-parametric probabilistic model. Food Addit. Contam. Part. A 2020, 37, 916–930. [Google Scholar] [CrossRef]
- Kawahara, J.; Imaizumi, Y.; Kuroda, K.; Aoki, Y.; Suzuki, N. Estimation of long-term dietary exposure to acrylamide of the Japanese people. Food Addit. Contam. Part. A 2018, 35, 1689–1702. [Google Scholar] [CrossRef]
- Cengiz, M.F.; Gündüz, C.P.B. Acrylamide exposure among Turkish toddlers from selected cereal-based baby food samples. Food Chem. Toxicol. 2013, 60, 514–519. [Google Scholar] [CrossRef]
- Svensson, K.; Abramsson, L.; Becker, W.; Glynn, A.; Hellenäs, K.-E.; Lind, Y.; Rosén, J. Dietary intake of acrylamide in Sweden. Food Chem. Toxicol. 2003, 41, 1581–1586. [Google Scholar] [CrossRef]
- Mojska, H.; Gielecińska, I.; Zielińska, A.; Winiarek, J.; Sawicki, W. Estimation of exposure to dietary acrylamide based on mercapturic acids level in urine of Polish women post partum and an assessment of health risk. J. Expo. Sci. Environ. Epidemiol. 2015, 26, 288–295. [Google Scholar] [CrossRef]
- Lujan-Barroso, L.; González, C.A.; Slimani, N.; Obón-Santacana, M.; Ferrari, P.; Freisling, H.; Overvad, K.; Clavel-Chapelon, F.; Boutron-Ruault, M.-C.; Racine, A.; et al. Dietary intake of acrylamide and esophageal cancer risk in the European Prospective Investigation into Cancer and Nutrition cohort. Cancer Causes Control. 2014, 25, 639–646. [Google Scholar] [CrossRef]
- Mucci, L.A.; Sandin, S.; Bälter, K.; Adami, H.-O.; Magnusson, C.; Weiderpass, E. Acrylamide Intake and Breast Cancer Risk in Swedish Women. JAMA 2005, 293, 1322–1327. [Google Scholar] [CrossRef]
- Kotemori, A.; Ishihara, J.; Zha, L.; Liu, R.; Sawada, N.; Iwasaki, M.; Sobue, T.; Tsugane, S. The JPHC Study Group Dietary acrylamide intake and risk of breast cancer: The Japan Public Health Center-based Prospective Study. Cancer Sci. 2017, 109, 843–853. [Google Scholar] [CrossRef] [PubMed]
- Normandin, L.; Bouchard, M.; Ayotte, P.; Blanchet, C.; Becalski, A.; Bonvalot, Y.; Phaneuf, D.; Lapointe, C.; Gagné, M.; Courteau, M. Dietary exposure to acrylamide in adolescents from a Canadian urban center. Food Chem. Toxicol. 2013, 57, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Wilson, K.M.; Bälter, K.; Adami, H.-O.; Grönberg, H.; Vikström, A.C.; Paulsson, B.; Törnqvist, M.; Mucci, L.A. Acrylamide exposure measured by food frequency questionnaire and hemoglobin adduct levels and prostate cancer risk in the Cancer of the Prostate in Sweden Study. Int. J. Cancer 2009, 124, 2384–2390. [Google Scholar] [CrossRef] [Green Version]
- Pelucchi, C.; Rosato, V.; Bracci, P.M.; Li, D.; Neale, R.E.; Lucenteforte, E.; Serraino, D.; Anderson, K.E.; Fontham, E.; Holly, E.A.; et al. Dietary acrylamide and the risk of pancreatic cancer in the International Pancreatic Cancer Case–Control Consortium (PanC4). Ann. Oncol. 2017, 28, 408–414. [Google Scholar] [CrossRef]
- Zając, J.; Bojar, I.; Helbin, J.; Kolarzyk, E.; Potocki, A.; Strzemecka, J.; Owoc, A. Dietary acrylamide exposure in chosen population of South Poland. Ann. Agric. Environ. Med. 2013, 20, 351–355. [Google Scholar]
- Dybing, E. Risk Assessment of Acrylamide in Foods. Toxicol. Sci. 2003, 75, 7–15. [Google Scholar] [CrossRef] [Green Version]
- Hilbig, A.; Freidank, N.; Kersting, M.; Wilhelm, M.; Wittsiepe, J. Estimation of the dietary intake of acrylamide by German infants, children and adolescents as calculated from dietary records and available data on acrylamide levels in food groups. Int. J. Hyg. Environ. Health 2004, 207, 463–471. [Google Scholar] [CrossRef]
- Hirvonen, T.; Jestoi, M.; Tapanainen, H.; Valsta, L.; Virtanen, S.M.; Sinkko, H.; Kronberg-Kippilä, C.; Kontto, J.; Virtamo, J.; Simell, O.; et al. Dietary acrylamide exposure among Finnish adults and children: The potential effect of reduction measures. Food Addit. Contam. Part. A 2011, 28, 1483–1491. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.; Kim, H.J. Dietary Exposure to Acrylamide and Associated Health Risks for the Korean Population. Int. J. Environ. Res. Public Health 2020, 17, 7619. [Google Scholar] [CrossRef]
- Abt, E.; Robin, L.P.; McGrath, S.; Srinivasan, J.; DiNovi, M.; Adachi, Y.; Chirtel, S. Acrylamide levels and dietary exposure from foods in the United States, an update based on 2011-2015 data. Food Addit. Contam. Part. A 2019, 36, 1475–1490. [Google Scholar] [CrossRef]
- Mojska, H.; Gielecińska, I.; Szponar, L.; Ołtarzewski, M. Estimation of the dietary acrylamide exposure of the Polish population. Food Chem. Toxicol. 2010, 48, 2090–2096. [Google Scholar] [CrossRef]
- Tong, P.; Fuentes, D.; Hambridge, T. Australian survey of acrylamide in carbohydrate-based foods. Food Addit. Contam. 2004, 21, 721–736. [Google Scholar] [CrossRef]
- Tran, N.; Barraj, L.; Murphy, M.; Bi, X. Dietary Acrylamide Exposure and Hemoglobin Adducts—National Health and Nutrition Examination Survey (2003–04). Food Chem. Toxicol. 2010, 48, 3098–3108. [Google Scholar] [CrossRef] [PubMed]
- Claeys, W.L.; Baert, K.; Mestdagh, F.; Vercammen, J.; Daenens, P.; De Meulenaer, B.; Maghuin-Rogister, G.; Huyghebaert, A. Assessment of the acrylamide intake of the Belgian population and the effect of mitigation strategies. Food Addit. Contam. Part. A 2010, 27, 1199–1207. [Google Scholar] [CrossRef] [PubMed]
- Vikström, A.C.; Warholm, M.; Paulsson, B.; Axmon, A.; Wirfält, E.; Törnqvist, M. Hemoglobin adducts as a measure of variations in exposure to acrylamide in food and comparison to questionnaire data. Food Chem. Toxicol. 2012, 50, 2531–2539. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, P.; Freisling, H.; Duell, E.J.; Kaaks, R.; Lujan-Barroso, L.; Clavel-Chapelon, F.; Boutron-Ruault, M.-C.; Nailler, L.; Polidoro, S.; Mattiello, A.; et al. Challenges in estimating the validity of dietary acrylamide measurements. Eur. J. Nutr. 2012, 52, 1503–1512. [Google Scholar] [CrossRef]
- Yamamoto, J.; Ishihara, J.; Kotemori, A.; Nakadate, M.; Sobue, T. Validity of Estimated Acrylamide Intake by the Dietary Record Method and Food Frequency Questionnaire in Comparison with a Duplicate Method: A Pilot Study. J. Nutr. Sci. Vitaminol. 2018, 64, 340–346. [Google Scholar] [CrossRef] [Green Version]
- Brisson, B.; Ayotte, P.; Normandin, L.; Gaudreau, E.; Bienvenu, J.-F.; Fennell, T.R.; Blanchet, C.; Phaneuf, D.; Lapointe, C.; Bonvalot, Y.; et al. Relation between dietary acrylamide exposure and biomarkers of internal dose in Canadian teenagers. J. Expo. Sci. Environ. Epidemiol. 2013, 24, 215–221. [Google Scholar] [CrossRef] [Green Version]
- Wong, W.W.; Chung, S.W.; Lam, C.-H.; Ho, Y.; Xiao, Y. Dietary exposure of Hong Kong adults to acrylamide: Results of the first Hong Kong Total Diet Study. Food Addit. Contam. Part. A 2014, 31, 799–805. [Google Scholar] [CrossRef]
- Arisseto, A.P.T.; de Figueiredo, M.C.; Govaert, Y.; van Loco, J.; Fraselle, S.; Degroodt, J.-M.; Rosseto Caroba, D.C. Contribution of selected foods to acrylamide intake by a population of Brazilian adolescents. Food Sci. Technol. 2009, 42, 207–211. [Google Scholar]
- Brantsæter, A.L.; Knutsen, H.K.; Lillegaard, I.T.L.; Amlund, H.; Eriksen, G.S.; Fæste, C.K.; Kvalem, H.E.; Miles, C.O.; Oskam, I.; Ruus, A.; et al. Risk Assessment of Dietary Exposure to Acrylamide in the Norwegian Population. Eur. J. Nutr. Food Saf. 2018, 8, 162–166. [Google Scholar] [CrossRef] [Green Version]
- Petersen, A.; Fromberg, A.; Andersen, J.H.; Sloth, J.J.; Granby, K.; Duedahl-Olesen, L.; Rasmussen, P.H.; Fagt, S.; Cederberg, T.L.; Christensenet, T.; et al. Chemical Contaminants. Food Monitoring 2004–2011; National Food Institute, Technical University of Denmark, Division of Food Chemistry: Kongens Lyngby, Denmark, 2013. [Google Scholar]
- Mucci, L.A.; Adami, H.-O.; Wolk, A. Prospective study of dietary acrylamide and risk of colorectal cancer among women. Int. J. Cancer 2005, 118, 169–173. [Google Scholar] [CrossRef]
- Mucci, L.A.; Lindblad, P.; Steineck, G.; Adami, H.-O. Dietary acrylamide and risk of renal cell cancer. Int. J. Cancer 2004, 109, 774–776. [Google Scholar] [CrossRef]
- Hogervorst, J.G.; Schouten, L.; Konings, E.J.; Goldbohm, R.A.; Brandt, P.V.D. A Prospective Study of Dietary Acrylamide Intake and the Risk of Endometrial, Ovarian, and Breast Cancer. Cancer Epidemiol. Biomark. Prev. 2007, 16, 2304–2313. [Google Scholar] [CrossRef] [Green Version]
- Mancini, F.R.; Sirot, V.; Busani, L.; Volatier, J.-L.; Hulin, M. Use and impact of usual intake models on dietary exposure estimate and risk assessment of chemical substances: A practical example for cadmium, acrylamide and sulphites. Food Addit. Contam. Part. A 2015, 32, 1065–1074. [Google Scholar] [CrossRef]
- Pelucchi, C.; Galeone, C.; Talamini, R.; Negri, E.; Polesel, J.; Serraino, D.; La Vecchia, C. Dietary acrylamide and pancreatic cancer risk in an Italian case–control study. Ann. Oncol. 2011, 22, 1910–1915. [Google Scholar] [CrossRef]
- Nagata, C.; Konishi, K.; Tamura, T.; Wada, K.; Tsuji, M.; Hayashi, M.; Takeda, N.; Yasuda, K. Associations of Acrylamide Intake with Circulating Levels of Sex Hormones and Prolactin in Premenopausal Japanese Women. Cancer Epidemiol. Biomark. Prev. 2015, 24, 249–254. [Google Scholar] [CrossRef] [Green Version]
- Gao, J.; Zhao, Y.; Zhu, F.; Ma, Y.; Li, X.; Miao, H.; Wu, Y. Dietary exposure of acrylamide from the fifth Chinese Total Diet Study. Food Chem. Toxicol. 2016, 87, 97–102. [Google Scholar] [CrossRef]
- Pedersen, A.N.; Christensen, T.; Matthiessen, J.; Knudsen, V.K.; Rosenlund-Sørensen, M.; Biltoft-Jensen, A.; Hinsch, H.J.; Ygil, K.H.; Kørup, K.; Saxholt, E.; et al. Dietary Habits in Denmark 2011–2013; DTU Fødevareinstituttet: Søborg, Denmark, 2015. [Google Scholar]
- Acrylamide Intake with Urinary Sex Hormone Levels among Preschool Japanese Children. Am. J. Epidemiol. 2017, 187, 75–81. [CrossRef] [Green Version]
- Fohgelberg, P.; Rosén, J.; Hellenäs, K.-E.; Abramsson-Zetterberg, L. The acrylamide intake via some common baby food for children in Sweden during their first year of life—an improved method for analysis of acrylamide. Food Chem. Toxicol. 2005, 43, 951–959. [Google Scholar] [CrossRef]
- Petrarca, M.H.; Rosa, M.A.; Queiroz, S.C.N.; Godoy, H.T. Simultaneous determination of acrylamide and 4-hydroxy-2,5-dimethyl-3(2 H )-furanone in baby food by liquid chromatography–tandem mass spectrometry. J. Chromatogr. A 2017, 1522, 62–69. [Google Scholar] [CrossRef]
- Elias, A.; Roasto, M.; Reinik, M.; Nelis, K.; Nurk, E.; Elias, T. Acrylamide in commercial foods and intake by infants in Estonia. Food Addit. Contam. Part. A 2017, 34, 1875–1884. [Google Scholar] [CrossRef]
- Sirot, V.; Rivière, G.; Leconte, S.; Vin, K.; Traore, T.; Jean, J.; Carne, G.; Gorecki, S.; Veyrand, B.; Marchand, P.; et al. French infant total diet study: Dietary exposure to heat-induced compounds (acrylamide, furan and polycyclic aromatic hydrocarbons) and associated health risks. Food Chem. Toxicol. 2019, 130, 308–316. [Google Scholar] [CrossRef]
- Sirot, V.; Hommet, F.; Tard, A.; Leblanc, J.-C. Dietary acrylamide exposure of the French population: Results of the second French Total Diet Study. Food Chem. Toxicol. 2012, 50, 889–894. [Google Scholar] [CrossRef]
- Previdelli, A.N.; Gómez, G.; Kovalskys, I.; Fisberg, M.; Cortés, L.Y.; Pareja, R.G.; Liria, M.R.; García, M.C.Y.; Herrera-Cuenca, M.; Rigotti, A.; et al. Prevalence and determinants of misreporting of energy intake among Latin American populations: Results from ELANS study. Nutr. Res. 2019, 68, 9–18. [Google Scholar] [CrossRef]
- Tam, K.W.; Veerman, J.L. Prevalence and characteristics of energy intake under-reporting among Australian adults in 1995 and 2011 to 2012. Nutr. Diet. 2019, 76, 546–559. [Google Scholar] [CrossRef]
- Freisling, H.; Moskal, A.; Ferrari, P.; Nicolas, G.; Knaze, V.; Clavel-Chapelon, F.; Boutron-Ruault, M.-C.; Nailler, L.; Teucher, B.; Grote, V.A.; et al. Dietary acrylamide intake of adults in the European Prospective Investigation into Cancer and Nutrition differs greatly according to geographical region. Eur. J. Nutr. 2012, 52, 1369–1380. [Google Scholar] [CrossRef]
- Hirvonen, T.P.; Kontto, J.; Jestoi, M.; Valsta, L.M.; Peltonen, K.; Pietinen, P.; Virtanen, S.M.; Sinkko, H.; Kronbergkippila, C.; Albanes, D.; et al. Dietary acrylamide intake and the risk of cancer among Finnish male smokers. Cancer Causes Control. 2010, 21, 2223–2229. [Google Scholar] [CrossRef] [Green Version]
- Bjellaas, T.; Stølen, L.H.; Haugen, M.; Paulsen, J.E.; Alexander, J.; Lundanes, E.; Becher, G. Urinary acrylamide metabolites as biomarkers for short-term dietary exposure to acrylamide. Food Chem. Toxicol. 2007, 45, 1020–1026. [Google Scholar] [CrossRef]
- Wyka, J.; Tajner-Czopek, A.; Broniecka, A.; Piotrowska, E.; Bronkowska, M.; Biernat, J. Estimation of dietary exposure to acrylamide of Polish teenagers from an urban environment. Food Chem. Toxicol. 2015, 75, 151–155. [Google Scholar] [CrossRef]
- Dybing, E.; Farmer, P.; Andersen, M.; Fennell, T.; Lalljie, S.; Müller, D.; Olin, S.; Petersen, B.; Schlatter, J.; Scholz, G.; et al. Human exposure and internal dose assessments of acrylamide in food. Food Chem. Toxicol. 2005, 43, 365–410. [Google Scholar] [CrossRef]
- Pelucchi, C.; Galeone, C.; Maso, L.D.; Talamini, R.; Montella, M.; Ramazzotti, V.; Negri, E.; Franceschi, S.; La Vecchia, C. Dietary acrylamide and renal cell cancer. Int. J. Cancer 2006, 120, 1376–1377. [Google Scholar] [CrossRef]
- Pelucchi, C.; Galeone, C.; Levi, F.; Negri, E.; Franceschi, S.; Talamini, R.; Bosetti, C.; Giacosa, A.; La Vecchia, C. Dietary acrylamide and human cancer. Int. J. Cancer 2006, 118, 467–471. [Google Scholar] [CrossRef] [PubMed]
- Pelucchi, C.; Galeone, C.; Negri, E.; Bosetti, C.; Serraino, D.; Montella, M.; Talamini, R.; La Vecchia, C. Dietary acrylamide and the risk of endometrial cancer: An Italian case-control study. Nutr. Cancer 2016, 68, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Obón-Santacana, M.; Kaaks, R.; Slimani, N.; Lujan-Barroso, L.; Freisling, H.; Ferrari, P.; Dossus, L.; Chabbert-Buffet, N.; Baglietto, L.; Fortner, R.; et al. Dietary intake of acrylamide and endometrial cancer risk in the European Prospective Investigation into Cancer and Nutrition cohort. Br. J. Cancer 2014, 111, 987–997. [Google Scholar] [CrossRef] [PubMed]
- Obón-Santacana, M.; Lujan-Barroso, L.; Freisling, H.; Cadeau, C.; Fagherazzi, G.; Boutron-Ruault, M.-C.; Kaaks, R.; Fortner, R.; Boeing, H.; Quirós, J.R.; et al. Dietary and lifestyle determinants of acrylamide and glycidamide hemoglobin adducts in non-smoking postmenopausal women from the EPIC cohort. Eur. J. Nutr. 2016, 56, 1157–1168. [Google Scholar] [CrossRef] [Green Version]
- Obón-Santacana, M.; Peeters, P.H.; Freisling, H.; Dossus, L.; Clavel-Chapelon, F.; Baglietto, L.; Schock, H.; Fortner, R.; Boeing, H.; Tjonneland, A.; et al. Dietary Intake of Acrylamide and Epithelial Ovarian Cancer Risk in the European Prospective Investigation into Cancer and Nutrition (EPIC) Cohort. Cancer Epidemiol. Biomark. Prev. 2015, 24, 291–297. [Google Scholar] [CrossRef] [Green Version]
- Obón-Santacana, M.; Slimani, N.; Lujan-Barroso, L.; Travier, N.; Hallmans, G.; Freisling, H.; Ferrari, P.; Boutron-Ruault, M.C.; Racine, A.; Clavel, F.; et al. Dietary intake of acrylamide and pancreatic cancer risk in the European Prospective Investigation into Cancer and Nutrition (EPIC) cohort. Ann. Oncol. 2013, 24, 2645–2651. [Google Scholar] [CrossRef]
- Kafouris, D.; Stavroulakis, G.; Christofidou, M.; Iakovou, X.; Christou, E.; Paikousis, L.; Christodoulidou, M.; Ioannou-Kakouri, E.; Yiannopoulos, S. Determination of acrylamide in food using a UPLC–MS/MS method: Results of the official control and dietary exposure assessment in Cyprus. Food Addit. Contam. Part. A 2018, 35, 1928–1939. [Google Scholar] [CrossRef]
- Castle, L.; Eriksson, S. Analytical methods used to measure acrylamide concentrations in foods. J. AOAC Int. 2005, 88, 274–284. [Google Scholar] [CrossRef]
- Schouten, M.A.; Tappi, S.; Romani, S. Acrylamide in coffee: Formation and possible mitigation strategies–A review. Crit. Rev. Food Sci. Nutr. 2020, 60, 3807–3821. [Google Scholar] [CrossRef]
- Sanny, M.; Jinap, S.; Bakker, E.; van Boekel, M.; Luning, P. Possible causes of variation in acrylamide concentration in French fries prepared in food service establishments: An observational study. Food Chem. 2012, 132, 134–143. [Google Scholar] [CrossRef]
- Mills, C.; Tlustos, C.; Evans, R.; Matthews, W. Dietary Acrylamide Exposure Estimates for the United Kingdom and Ireland: Comparison between Semiprobabilistic and Probabilistic Exposure Models. J. Agric. Food Chem. 2008, 56, 6039–6045. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Acrylamide in Drinking-Water. Background Document for Development of WHO Guidelines for Drinking-Water Quality; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- Pabst, K.; Mathar, W.; Palavinskas, R.; Meisel, H.; Blüthgen, A.; Klaffke, H. Acrylamide–occurrence in mixed concentrate feed for dairy cows and carry-over into milk. Food Addit. Contam. 2005, 22, 210–213. [Google Scholar] [CrossRef]
- Kito, K.; Ishihara, J.; Yamamoto, J.; Hosoda, T.; Kotemori, A.; Takachi, R.; Nakamura, K.; Tanaka, J.; Yamaji, T.; Shimazu, T.; et al. Variations in the estimated intake of acrylamide from food in the Japanese population. Nutr. J. 2020, 19, 17. [Google Scholar] [CrossRef] [Green Version]
- Konings, E.J.M.; Hogervorst, J.G.F.; Van Rooij, L.; Schouten, L.; Sizoo, E.A.; Van Egmond, H.P.; Goldbohm, R.A.; Brandt, P.V.D. Validation of a database on acrylamide for use in epidemiological studies. Eur. J. Clin. Nutr. 2010, 64, 534–540. [Google Scholar] [CrossRef] [Green Version]
- Vikström, A.C.; Wilson, K.M.; Paulsson, B.; Athanassiadis, I.; Grönberg, H.; Adami, H.-O.; Adolfsson, J.; Mucci, L.A.; Bälter, K.; Törnqvist, M. Alcohol influence on acrylamide to glycidamide metabolism assessed with hemoglobin-adducts and questionnaire data. Food Chem. Toxicol. 2010, 48, 820–824. [Google Scholar] [CrossRef]
- Li, J.; Zuo, J.; Qiao, X.; Zhang, Y.; Xu, Z. Effect of garlic powder on acrylamide formation in a low-moisture model system and bread baking. J. Sci. Food Agric. 2016, 96, 893–899. [Google Scholar] [CrossRef]
- Taubert, D.; Glöckner, R.; Müller, D.; Schömig, E. The garlic ingredient diallyl sulfide inhibits cytochrome P450 2E1 dependent bioactivation of acrylamide to glycidamide. Toxicol. Lett. 2006, 164, 1–5. [Google Scholar] [CrossRef]
- Bjellaas, T.; Olesen, P.T.; Frandsen, H.; Haugen, M.; Stølen, L.H.; Paulsen, J.E.; Alexander, J.; Lundanes, E.; Becher, G. Comparison of Estimated Dietary Intake of Acrylamide with Hemoglobin Adducts of Acrylamide and Glycidamide. Toxicol. Sci. 2007, 98, 110–117. [Google Scholar] [CrossRef]
- Törnqvist, M. Acrylamide in Food: The Discovery and Its Implications. Chem. Biol. Pteridines Folates 2006, 561, 1–19. [Google Scholar] [CrossRef]
- Pedersen, M.; Vryonidis, E.; Joensen, A.; Halldorsson, T.I.; Olsen, S.F.; Törnqvist, M. Hemoglobin adducts of acrylamide in human blood—What has been done and what is next? in preparation.
- Kütting, B.; Schettgen, T.; Beckmann, M.W.; Angerer, J.; Drexler, H. Influence of Diet on Exposure to Acrylamide—Reflections on the Validity of a Questionnaire. Ann. Nutr. Metab. 2005, 49, 173–177. [Google Scholar] [CrossRef] [Green Version]
- Kütting, B.; Uter, W.; Drexler, H. The association between self-reported acrylamide intake and hemoglobin adducts as biomarkers of exposure. Cancer Causes Control. 2007, 19, 273–281. [Google Scholar] [CrossRef]
- Wilson, K.M.; Vesper, H.W.; Tocco, P.; Sampson, L.; Rosén, J.; Hellenäs, K.-E.; Törnqvist, M.; Willett, W.C. Validation of a food frequency questionnaire measurement of dietary acrylamide intake using hemoglobin adducts of acrylamide and glycidamide. Cancer Causes Control. 2009, 20, 269–278. [Google Scholar] [CrossRef] [Green Version]
- Duke, T.J.; Ruestow, P.S.; Marsh, G.M. The influence of demographic, physical, behavioral, and dietary factors on hemoglobin adduct levels of acrylamide and glycidamide in the general U.S. population. Crit. Rev. Food Sci. Nutr. 2017, 58, 700–710. [Google Scholar] [CrossRef]
- Li, D.; Wang, P.; Liu, Y.; Hu, X.; Chen, F. Metabolism of Acrylamide: Interindividual and Interspecies Differences as Well as the Application as Biomarkers. Curr. Drug Metab. 2016, 17, 317–326. [Google Scholar] [CrossRef]
- Von Stedingk, H.; Vikström, A.C.; Rydberg, P.; Pedersen, M.; Nielsen, J.K.S.; Segerbäck, D.; Knudsen, L.E.; Törnqvist, M. Analysis of Hemoglobin Adducts from Acrylamide, Glycidamide, and Ethylene Oxide in Paired Mother/Cord Blood Samples from Denmark. Chem. Res. Toxicol. 2011, 24, 1957–1965. [Google Scholar] [CrossRef]
- Liu, Z.-M.; Tse, L.A.; Chen, B.; Wu, S.; Chan, D.; Kowk, T.; Woo, J.; Xiang, Y.-T.; Wong, S.Y.-S. Dietary acrylamide exposure was associated with mild cognition decline among non-smoking Chinese elderly men. Sci. Rep. 2017, 7, 6395. [Google Scholar] [CrossRef] [Green Version]
- Liu, Z.-M.; Tse, L.A.; Ho, S.C.; Wu, S.; Chen, B.; Chan, D.; Wong, S.Y.-S. Dietary acrylamide exposure was associated with increased cancer mortality in Chinese elderly men and women: A 11-year prospective study of Mr. and Ms. OS Hong Kong. J. Cancer Res. Clin. Oncol. 2017, 143, 2317–2326. [Google Scholar] [CrossRef] [PubMed]
- McCullough, M.L.; Hodge, R.A.; Um, C.Y.; Gapstur, S.M. Dietary Acrylamide Is Not Associated with Renal Cell Cancer Risk in the CPS-II Nutrition Cohort. Cancer Epidemiol. Biomark. Prev. 2019, 28, 616–619. [Google Scholar] [CrossRef] [PubMed]
- Mucci, L.A.; Dickman, P.; Steineck, G.; Adami, H.-O.; Augustsson, K. Dietary acrylamide and cancer of the large bowel, kidney, and bladder: Absence of an association in a population-based study in Sweden. Br. J. Cancer 2003, 88, 84–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hogervorst, J.G.; Schouten, L.; Konings, E.J.; Goldbohm, R.A.; Brandt, P.V.D. Dietary acrylamide intake and the risk of renal cell, bladder, and prostate cancer. Am. J. Clin. Nutr. 2008, 87, 1428–1438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hogervorst, J.G.; Fortner, R.; Mucci, L.A.; Tworoger, S.; Eliassen, A.H.; Hankinson, S.E.; Wilson, K.M. Associations between Dietary Acrylamide Intake and Plasma Sex Hormone Levels. Cancer Epidemiol. Biomark. Prev. 2013, 22, 2024–2036. [Google Scholar] [CrossRef] [Green Version]
- Wilson, K.M.; Mucci, L.A.; Rosner, B.A.; Willett, W.C. A Prospective Study on Dietary Acrylamide Intake and the Risk for Breast, Endometrial, and Ovarian Cancers. Cancer Epidemiol. Biomark. Prev. 2010, 19, 2503–2515. [Google Scholar] [CrossRef] [Green Version]
- Larsson, S.C.; Åkesson, A.; Bergkvist, L.; Wolk, A. Dietary acrylamide intake and risk of colorectal cancer in a prospective cohort of men. Eur. J. Cancer 2009, 45, 513–516. [Google Scholar] [CrossRef]
- Calleman, C.; Wu, Y.; He, F.; Tian, G.; Bergmark, E.; Zhang, S.; Deng, H.; Wang, Y.; Crofton, K.; Fennell, T.; et al. Relationships between Biomarkers of Exposure and Neurological Effects in a Group of Workers Exposed to Acrylamide. Toxicol. Appl. Pharmacol. 1994, 126, 361–371. [Google Scholar] [CrossRef]
- Hagmar, L.; Törnqvist, M.; Nordander, C.; Rosén, I.; Bruze, M.; Kautiainen, A.; Magnusson, A.-L.; Malmberg, B.; Aprea, P.; Granath, F.; et al. Health effects of occupational exposure to acrylamide using hemoglobin adducts as biomarkers of internal dose. Scand. J. Work. Environ. Health 2001, 27, 219–226. [Google Scholar] [CrossRef] [Green Version]
- Pennisi, M.; Malaguarnera, G.; Puglisi, V.; Vinciguerra, L.; Vacante, M.; Malaguarnera, M. Neurotoxicity of Acrylamide in Exposed Workers. Int. J. Environ. Res. Public Health 2013, 10, 3843–3854. [Google Scholar] [CrossRef] [Green Version]
- Lindeman, B.; Johansson, Y.; Andreassen, M.; Husøy, T.; Dirven, H.; Hofer, T.; Knutsen, H.K.; Caspersen, I.H.; Vejrup, K.; Paulsen, R.E.; et al. Does the food processing contaminant acrylamide cause developmental neurotoxicity? A review and identification of knowledge gaps. Reprod. Toxicol. 2021, 101, 93–114. [Google Scholar] [CrossRef]
- Schettgen, T.; Hornig, M.; Beckmann, M.W.; Weiss, T.; Drexler, H.; Angerer, J. Trans-placental exposure of neonates to acrylamide? A pilot study. Int. Arch. Occup. Environ. Health 2004, 77, 213–216. [Google Scholar] [CrossRef]
- Pedersen, M.; Von Stedingk, H.; Botsivali, M.; Agramunt, S.; Alexander, J.; Brunborg, G.; Chatzi, L.; Fleming, S.J.; Fthenou, E.; Granum, B.; et al. Birth Weight, Head Circumference, and Prenatal Exposure to Acrylamide from Maternal Diet: The European Prospective Mother–Child Study (NewGeneris). Environ. Health Perspect. 2012, 120, 1739–1745. [Google Scholar] [CrossRef]
- Matoso, V.; Bargi-Souza, P.; Ivanski, F.; Romano, M.A.; Romano, R.M. Acrylamide: A review about its toxic effects in the light of Developmental Origin of Health and Disease (DOHaD) concept. Food Chem. 2019, 283, 422–430. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Facet 1 | Facet 2 | Facet 3 |
|---|---|---|
| Acrylamide | Humans | Diet record |
| Acrylamides | Women | Nutrition assessment |
| Men | Surveys and questionnaires | |
| Children | Dietary exposure | |
| Adolescents | Diet | |
| Adults | Feeding Behavior | |
| “Acrylamide Intake” * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Timmermann, C.A.G.; Mølck, S.S.; Kadawathagedara, M.; Bjerregaard, A.A.; Törnqvist, M.; Brantsæter, A.L.; Pedersen, M. A Review of Dietary Intake of Acrylamide in Humans. Toxics 2021, 9, 155. https://doi.org/10.3390/toxics9070155
Timmermann CAG, Mølck SS, Kadawathagedara M, Bjerregaard AA, Törnqvist M, Brantsæter AL, Pedersen M. A Review of Dietary Intake of Acrylamide in Humans. Toxics. 2021; 9(7):155. https://doi.org/10.3390/toxics9070155
Chicago/Turabian StyleTimmermann, Clara Amalie Gade, Signe Sonne Mølck, Manik Kadawathagedara, Anne Ahrendt Bjerregaard, Margareta Törnqvist, Anne Lise Brantsæter, and Marie Pedersen. 2021. "A Review of Dietary Intake of Acrylamide in Humans" Toxics 9, no. 7: 155. https://doi.org/10.3390/toxics9070155
APA StyleTimmermann, C. A. G., Mølck, S. S., Kadawathagedara, M., Bjerregaard, A. A., Törnqvist, M., Brantsæter, A. L., & Pedersen, M. (2021). A Review of Dietary Intake of Acrylamide in Humans. Toxics, 9(7), 155. https://doi.org/10.3390/toxics9070155