A Retrospective Analysis of the Effect of Subretinal Hyper-Reflective Material and Other Morphological Features of Neovascular Age-Related Macular Degeneration on Visual Acuity Outcomes in Eyes Treated with Intravitreal Aflibercept over One Year


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Visual Acuity and Morphological Outcomes
4. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Rosenfeld, P.J.; Brown, D.M.; Heier, J.S.; Boyer, D.S.; Kaiser, P.K.; Chung, C.Y.; Kim, R.Y.; MARINA Study Group. Ranibizumab for neovascular age-related macular degeneration. N. Engl. J. Med. 2006, 355, 1419–1431. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.P.; Bressler, S.B.; Bressler, N.M. Impact of availability of anti-vascular endothelial growth factor therapy on visual impairment and blindness due to neovascular age-related macular degeneration. Arch. Ophthalmol. 2012, 130, 794–795. [Google Scholar] [CrossRef] [PubMed]
- Holz, F.G.; Tadayoni, R.; Beatty, S.; Berger, A.; Cereda, M.G.; Cortez, R.; Hoyng, C.B.; Hykin, P.; Staurenghi, G.; Heldner, S.; et al. Multi-country real-life experience of anti-vascular endothelial growth factor therapy for wet age-related macular degeneration. Br. J. Ophthalmol. 2015, 99, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Bergers, G.; Hanahan, D. Modes of resistance to anti-angiogenic therapy. Nat. Rev. Cancer 2008, 8, 592–603. [Google Scholar] [CrossRef] [PubMed]
- Funk, M.; Karl, D.; Georgopoulos, M.; Benesch, T.; Sacu, S.; Polak, K.; Zlabinger, G.J.; Schmidt-Erfurth, U. Neovascular age-related macular degeneration: Intraocular cytokines and growth factors and the influence of therapy with ranibizumab. Ophthalmology 2009, 116, 2393–2399. [Google Scholar] [CrossRef] [PubMed]
- Gerding, H.; Loukopoulos, V.; Riese, J.; Hefner, L.; Timmermann, M. Results of flexible renibizumab treatment in age-related macular degeneration and search for parameters with impact on outcome. Graefes Arch. Clin. Exp. Ophthalmol. 2011, 249, 653–662. [Google Scholar] [CrossRef] [PubMed]
- Holash, J.; Davis, S.; Papadopoulos, N.; Croll, S.D.; Ho, L.; Russell, M.; Boland, P.; Leidich, R.; Hylton, D.; Burova, E.; et al. VEGF-Trap: A VEGF blocker with potent antitumor effects. Proc. Natl. Acad. Sci. USA 2002, 99, 11393–11398. [Google Scholar] [CrossRef] [PubMed]
- Heier, J.S.; Brown, D.M.; Chong, V.; Korobelnik, J.F.; Kaiser, P.K.; Nguyen, Q.D.; Kirchhof, B.; Ho, A.; Ogura, Y.; Yancopoulos, G.D.; et al. Intravitreal aflibercept (VEGF trap-eye) in wet age-related macular degeneration. Ophthalmology 2012, 119, 2537–2548. [Google Scholar] [CrossRef] [PubMed]
- Schmidt-Erfurth, U.; Kaiser, P.K.; Korobelnik, J.F.; Brown, D.M.; Chong, V.; Nguyen, Q.D.; Ho, A.C.; Ogura, Y.; Simader, C.; Jaffe, G.J.; et al. Intravitreal aflibercept injection for neovascular age-related macular degeneration. Ninety-six-week results of the VIEW studies. Ophthalmology 2014, 121, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Willoughby, A.S.; Ying, G.S.; Toth, C.A.; Maguire, M.G.; Burns, R.E.; Grunwald, J.E.; Daniel, E.; Jaffe, G.J.; Comparison of Age-Related Macular Degeneration Treatments Trials Research Group. Subretinal hyperreflective material in the comparison of age-related macular degeneration treatments trials. Ophthalmology 2015, 122, 1846–1853. [Google Scholar] [CrossRef] [PubMed]
- Daniel, E.; Toth, C.A.; Grunwald, J.E.; Jaffe, G.J.; Martin, D.F.; Fine, S.L.; Huang, J.; Ying, G.S.; Hagstrom, S.A.; Winter, K.; et al. Comparison of Age-related Macular Degeneration Treatments Trials Research Group. Risk of scar in the comparison of age-related macular degeneration treatments trials. Ophthalmology 2014, 121, 656–666. [Google Scholar] [CrossRef] [PubMed]
- Longmore, M.; Khan, M.; Downes, S.; Chong, V. The incidence of subretinal hyper-reflective material in patients with newly diagnosed neovascular age-related macular degeneration requiring anti-VEGF therapy. In Proceedings of the 15th EURETINA Congress, Nice, France, 17–20 September 2015. [Google Scholar]
- Major, J.C., Jr.; Wykoff, C.C.; Mariani, A.F.; Chen, E.; Croft, D.E.; Brown, D.M. Comparison of spectral-domain and time-domain optical coherence tomography in the detection of neurovascular age-related macular degeneration activity. Retina 2013, 34, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Dugel, P.U. Anti-PDGF therapy offers new approach to AMD treatment. Retina Times 2012, 12 (Suppl. 1). [Google Scholar]
- Jo, N.; Mailhos, C.; Ju, M.; Cheung, E.; Bradley, J.; Nishijima, K.; Robinson, G.S.; Adamis, A.P.; Shima, D.T. Inhibition of platelet-derived growth factor B signaling enhances the efficacy of anti- vascular endothelial growth factor therapy in multiple models of ocular neovascularization. Am. J. Pathol. 2006, 168, 2036–2053. [Google Scholar] [CrossRef] [PubMed]
- ClinicalTrials.gov. Identifier NCT01944839. Available online: https://clinicaltrials.gov/ct2/show/NCT01944839 (accessed on 27 October 2016).
- ClinicalTrials.gov. Identifier NCT01940900. Available online: https://clinicaltrials.gov/ct2/show/NCT01940900 (accessed on 27 October 2016).
- Regeneron Announces Phase 2 Study Of Aflibercept Co-Formulated with Rinucumab (Anti-Pdgfr-Beta) Shows No Benefit Over Aflibercept Alone in Neovascular Age-Related Macular Degeneration. Available online: http://investor.regeneron.com/releasedetail.cfm?releaseid=991601 (accessed on 27 October 2016).
- Schmidt-Erfurth, U.; Waldstein, S.M. A paradigm shift in imaging biomarkers in neovascular age-related macular degeneration. Prog. Retin. Eye Res. 2016, 50, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Ritter, M.; Simader, C.; Bolz, M.; Deák, G.G.; Mayr-Sponer, U.; Sayegh, R.; Kundi, M.; Schmidt-Erfurth, U.M. Intraretinal cysts are the most relevant prognostic biomarker in neovascular age-related macular degeneration independent of the therapeutic strategy. Br. J. Ophthalmol. 2014, 98, 1629–1635. [Google Scholar] [CrossRef] [PubMed]
- Schmidt-Erfurth, U.; Chong, V.; Loewenstein, A.; Larsen, M.; Souied, E.; Schlingemann, R.; Eldem, B.; Monés, J.; Richard, G.; Bandello, F. European Society of Retina Specialists. Guidelines for the management of neovascular age-related macular degeneration by the European Society of Retina Specialists (EURETINA). Br. J. Ophthalmol. 2014, 98, 1144–1167. [Google Scholar] [CrossRef] [PubMed]
- Park, D.H.; Sun, H.J.; Lee, S.J. A comparison of responses to intravitreal bevacizumab, ranibizumab, or aflibercept injections for neovascular age-related macular degeneration. Int. Ophthalmol. 2016. [Google Scholar] [CrossRef] [PubMed]
- Jaffe, G.J.; Martin, D.F.; Toth, C.A.; Daniel, E.; Maguire, M.G.; Ying, G.S.; Grunwald, J.E.; Huang, J.; Comparison of Age-related Macular Degeneration Treatments Trials Research Group. Macular morphology and visual acuity in the comparison of age-related macular degeneration treatment trials. Ophthalmology 2013, 120, 1860–1870. [Google Scholar] [CrossRef] [PubMed]
- Waldstein, S.M.; Wright, J.; Warburton, J.; Margarin, P.; Simader, C.; Schmidt-Erfurth, U. Predictive Value of Retinal Morphology for Visual Acuity Outcomes of Different Ranibizumab Treatment Regimens for Neovascular AMD. Ophthalmology 2016, 123, 60–69. [Google Scholar] [CrossRef] [PubMed]



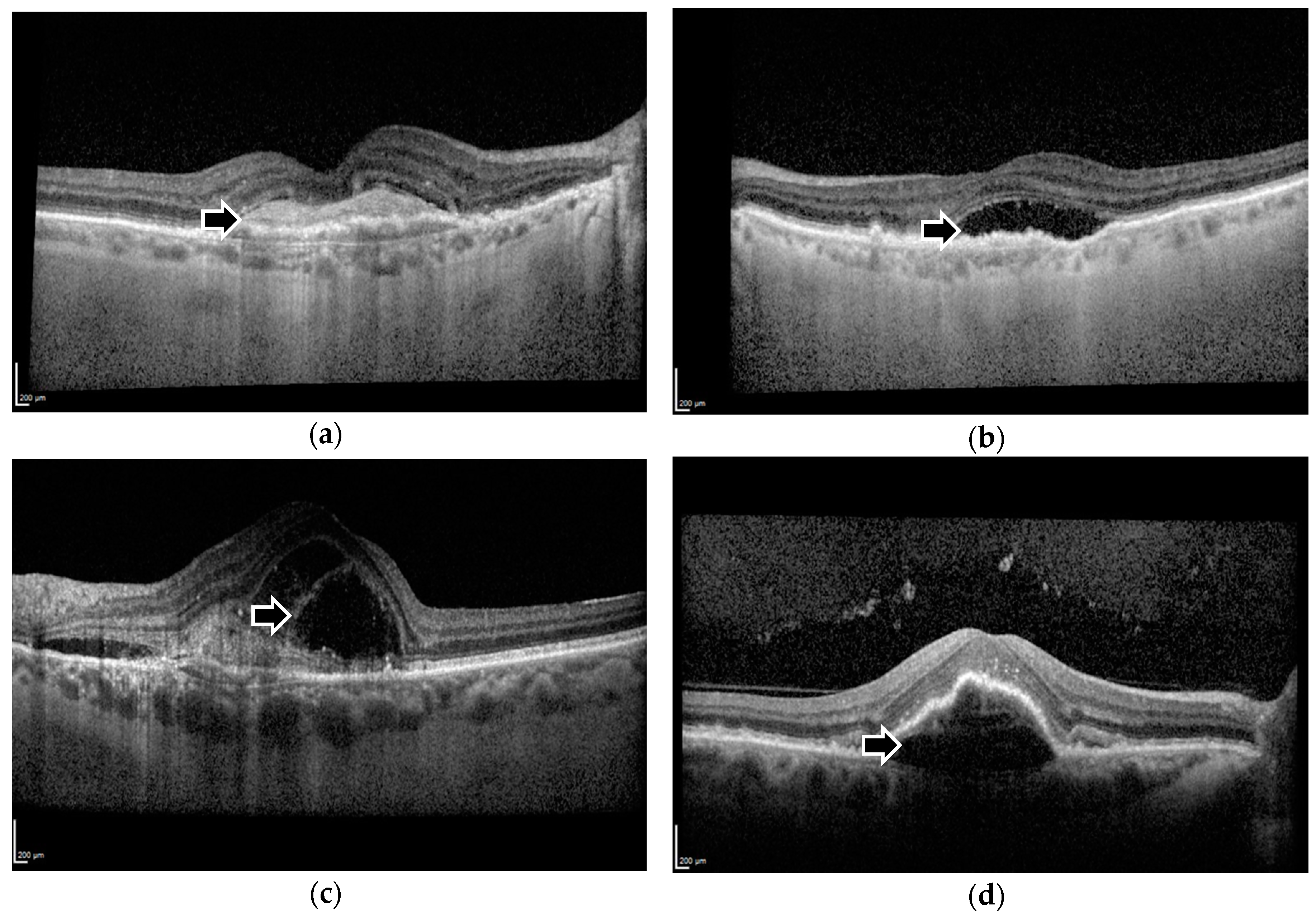{kind=link}
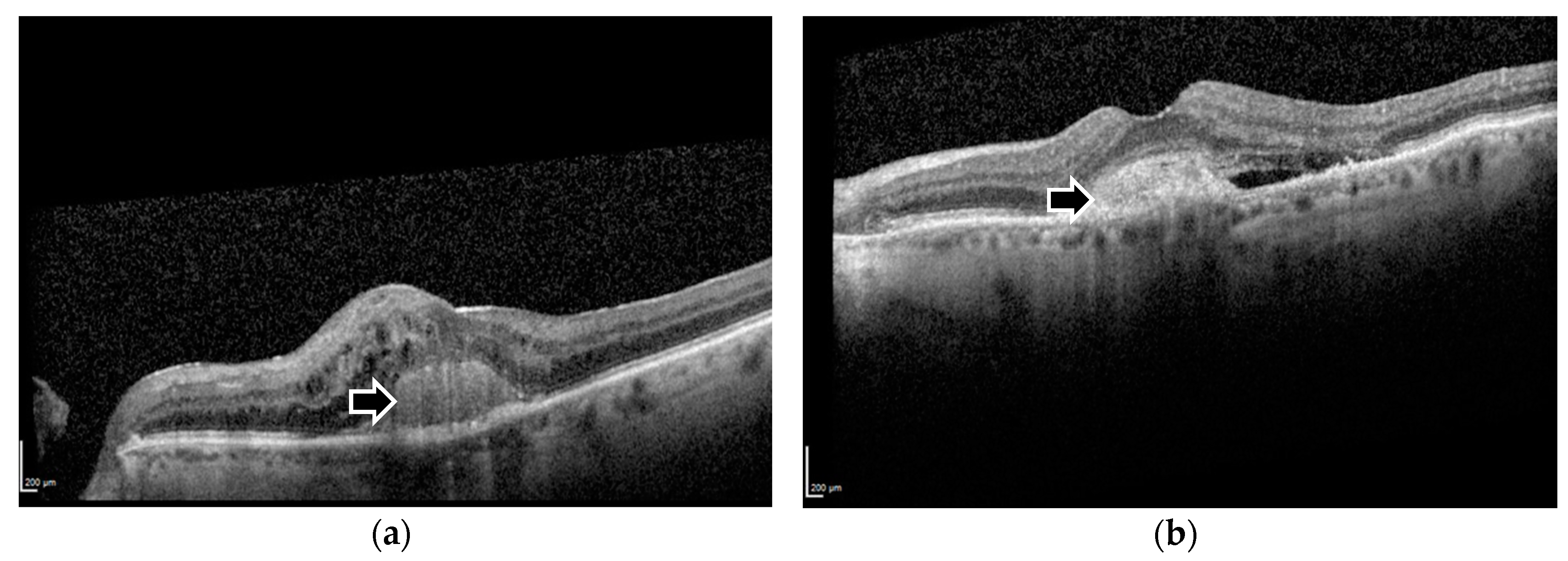{kind=link}
| Characteristics | Number of Eyes (Percentage) | Mean BCVA in Letters (Standard Error of the Mean), and Approximate Snellen Ratio | p-Value | |
|---|---|---|---|---|
| Gender | ||||
| Male | 66 (37.5) | Baseline BCVA | 56.24 (1.917), 20/80 + 1 | 0.901 a |
| One year BCVA | 61.52 (1.903), 20/63 + 2 | 0.212 a | ||
| Change in BCVA | 5.27 (1.291) | 0.054 a | ||
| Female | 110 (62.5) | Baseline BCVA | 56.54 (1.394), 20/80 + 2 | |
| One year BCVA | 58.41 (1.590), 20/80 + 3 | |||
| Change in BCVA | 1.87 (1.183) | |||
| Laterality | ||||
| Left | 88 (50.0) | Baseline BCVA | 56.89 (1.537), 20/80 + 2 | 0.684 |
| One year BCVA | 60.43 (1.795), 20/63 | 0.485 | ||
| Change in BCVA | 3.55 (1.301) | 0.656 | ||
| Right | 88 (50.0) | Baseline BCVA | 55.97 (1.653), 20/80 + 1 | |
| One year BCVA | 58.72 (1.674), 20/63 − 1 | |||
| Change in BCVA | 2.75 (1.222) | |||
| Number of Injections in One Year | ||||
| 7 | 79 (44.9) | Baseline BCVA | 55.67 (1.657), 20/80 + 1 | 0.545 |
| One year BCVA | 59.35 (1.891), 20/63 − 1 | 0.873 | ||
| Change in BCVA | 3.68 (1.221) | 0.583 | ||
| 8 | 97 (55.1) | Baseline BCVA | 57.04 (1.539), 20/80 + 2 | |
| One year BCVA | 59.75 (1.612), 20/63 | |||
| Change in BCVA | 2.71 (1.277) | |||
| SHRM | ||||
| Present at baseline | 51 (29.0) | Baseline BCVA | 50.86 (2.128), 20/100 + 1 | 0.002 |
| One year BCVA | 55.84 (2.425), 20/80 + 1 | 0.064 | ||
| Change in BCVA | 4.98 (1.705) | 0.200 | ||
| Absent at baseline | 125 (71.0) | Baseline BCVA | 58.70 (1.277), 20/63 − 1 | |
| One year BCVA | 61.10 (1.397), 20/63 + 1 | |||
| Change in BCVA | 2.40 (1.040) | |||
| PED—Baseline | ||||
| Present | 58 (33.0) | Baseline BCVA | 56.16 (2.002), 20/80 + 1 | 0.868 |
| One year BCVA | 60.29 (2.239), 20/63 | 0.689 | ||
| Change in BCVA | 4.14 (1.833) | 0.479 | ||
| Absent | 118 (67.0) | Baseline BCVA | 56.56 (1.367), 20/80 + 2 | |
| One year BCVA | 59.22 (1.465), 20/63 − 1 | |||
| Change in BCVA | 2.66 (0.978) | |||
| PED—One Year | One year BCVA | 0.978 | ||
| Present | 44 (25.0) | 59.64 (2.638), 20/63 | ||
| Absent | 132 (75.0) | 59.55 (1.383), 20/63 | ||
| PED—Resolution | Change in BCVA | 0.992 | ||
| Improvement | 23 (13.1) | 3.17 (2.834) | ||
| No improvement | 153 (86.9) | 3.14 (0.935) | ||
| SRF—Baseline | ||||
| Present | 54 (30.7) | Baseline BCVA | 61.24 (1.847), 20/63 + 1 | 0.004 |
| One year BCVA | 66.80 (2.065), 20/50 + 2 | 0.0001 | ||
| Change in BCVA | 5.56 (1.312) | 0.047 | ||
| Absent | 122 (69.3) | Baseline BCVA | 54.30 (1.364), 20/80 − 1 | |
| One year BCVA | 56.38 (1.425), 20/80 + 1 | |||
| Change in BCVA | 2.08 (1.136) | |||
| SRF—One year | One year BCVA | 0.394 | ||
| Present | 8 (4.5) | 63.50 (4.396), 20/50 − 1 | ||
| Absent | 168 (95.5) | 59.39 (1.267), 20/63 − 1 | ||
| SRF—Resolution | Change in BCVA | 0.073 | ||
| Improvement | 48 (27.3) | 5.50 (1.411) | ||
| No improvement | 128 (72.7) | 2.27 (1.097) | ||
| IRF—Baseline | ||||
| Present | 73 (41.5) | Baseline BCVA | 50.55 (1.703), 20/100 + 1 | 0.0001 |
| One year BCVA | 54.97 (1.917), 20/80 | 0.002 | ||
| Change in BCVA | 4.42 (1.238) | 0.215 | ||
| Absent | 103 (58.5) | Baseline BCVA | 60.59 (1.363), 20/63 + 1 | |
| One year BCVA | 62.83 (1.521), 20/63 + 3 | |||
| Change in BCVA | 2.24 (1.240) | |||
| IRF—One Year | One year BCVA | 0.318 | ||
| Present | 5 (2.8) | 53.20 (5.687), 20/80 − 2 | ||
| Absent | 171 (97.2) | 59.76 (1.249), 20/63 | ||
| IRF—Resolution | Change in BCVA | 0.205 | ||
| Improvement | 70 (39.8) | 4.50 (1.288) | ||
| No improvement | 106 (60.2) | 2.25 (1.206) | ||
| Total Eyes (n = 176) | SHRM | No SHRM | PED | No PED | SRF | No SRF | IRF | No IRF | |
|---|---|---|---|---|---|---|---|---|---|
| Normal a | 43 | 11 | 32 | 11 | 32 | 25 | 18 | 15 | 28 |
| Impaired b | 26 | 7 | 19 | 11 | 15 | 7 | 19 | 5 | 21 |
| Low c | 107 | 33 | 74 | 36 | 71 | 22 | 85 | 53 | 54 |
| p-Value d | p = 0.789 | p = 0.348 | p ≤ 0.001 | p = 0.011 | |||||
| Model Summary | |||||||
| R | R2 | Adjusted R2 | Std. Error of the Estimate | ||||
| 0.351 a | 0.123 | 0.097 | 11.223 | ||||
| ANOVA b | |||||||
| Sum of Squares | df | Mean Square | F | Sig. | |||
| Regression | 3001.567 | 5 | 600.313 | 4.766 | <0.001 a | ||
| Residual | 21,412.592 | 170 | 125.956 | ||||
| Total | 24,414.159 | 175 | |||||
| Coefficients b | |||||||
| Unstandardised Coefficients | Standardised Coefficients | ||||||
| B | Std. Error | Beta | t | Sig. | |||
| (Constant) | 14.810 | 4.260 | 3.476 | 0.001 | |||
| Baseline visual acuity | −0.249 | 0.064 | −0.315 | −3.888 | <0.001 | ||
| SHRM grading | 0.707 | 1.961 | 0.027 | 0.360 | 0.719 | ||
| PED at baseline | 1.730 | 1.845 | 0.069 | 0.938 | 0.350 | ||
| SRF at baseline | 5.264 | 1.889 | 0.206 | 2.787 | 0.006 | ||
| IRF at baseline | 0.040 | 1.846 | 0.002 | 0.022 | 0.983 | ||
| Model Summary | ||||||
| R | R2 | Adjusted R2 | Std. Error of the Estimate | |||
| 0.334 a | 0.112 | 0.086 | 11.295 | |||
| ANOVA b | ||||||
| Sum of Squares | df | Mean Square | F | Sig. | ||
| Regression | 2726.419 | 5 | 545.284 | 4.274 | 0.001 a | |
| Residual | 21,687.741 | 170 | 127.575 | |||
| Total | 24,414.159 | 175 | ||||
| Coefficients b | ||||||
| Unstandardised Coefficients | Standardised Coefficients | |||||
| B | Std. Error | Beta | t | Sig. | ||
| (Constant) | 15.899 | 4.122 | 3.857 | <0.001 | ||
| Baseline visual acuity | −0.251 | 0.064 | −0.318 | −3.912 | <0.001 | |
| PED improvement or no improvement | 0.890 | 2.549 | 0.025 | 0.349 | 0.727 | |
| SRF improvement or no improvement | 4.945 | 1.980 | 0.187 | 2.497 | 0.013 | |
| IRF improvement or no improvement | −0.372 | 1.855 | −0.015 | −0.200 | 0.841 | |
| SHRM grading | 0.399 | 1.957 | 0.015 | 0.204 | 0.839 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leung, K.F.C.; Downes, S.M.; Chong, V. A Retrospective Analysis of the Effect of Subretinal Hyper-Reflective Material and Other Morphological Features of Neovascular Age-Related Macular Degeneration on Visual Acuity Outcomes in Eyes Treated with Intravitreal Aflibercept over One Year. Vision 2018, 2, 5. https://doi.org/10.3390/vision2010005
Leung KFC, Downes SM, Chong V. A Retrospective Analysis of the Effect of Subretinal Hyper-Reflective Material and Other Morphological Features of Neovascular Age-Related Macular Degeneration on Visual Acuity Outcomes in Eyes Treated with Intravitreal Aflibercept over One Year. Vision. 2018; 2(1):5. https://doi.org/10.3390/vision2010005
Chicago/Turabian StyleLeung, King Fai Calvin, Susan M. Downes, and Victor Chong. 2018. "A Retrospective Analysis of the Effect of Subretinal Hyper-Reflective Material and Other Morphological Features of Neovascular Age-Related Macular Degeneration on Visual Acuity Outcomes in Eyes Treated with Intravitreal Aflibercept over One Year" Vision 2, no. 1: 5. https://doi.org/10.3390/vision2010005
APA StyleLeung, K. F. C., Downes, S. M., & Chong, V. (2018). A Retrospective Analysis of the Effect of Subretinal Hyper-Reflective Material and Other Morphological Features of Neovascular Age-Related Macular Degeneration on Visual Acuity Outcomes in Eyes Treated with Intravitreal Aflibercept over One Year. Vision, 2(1), 5. https://doi.org/10.3390/vision2010005