
Tinnitus, Aural Fullness, and Hearing Loss in a Patient with Acoustic Neuroma and Pituitary Macroadenoma



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:- (d)
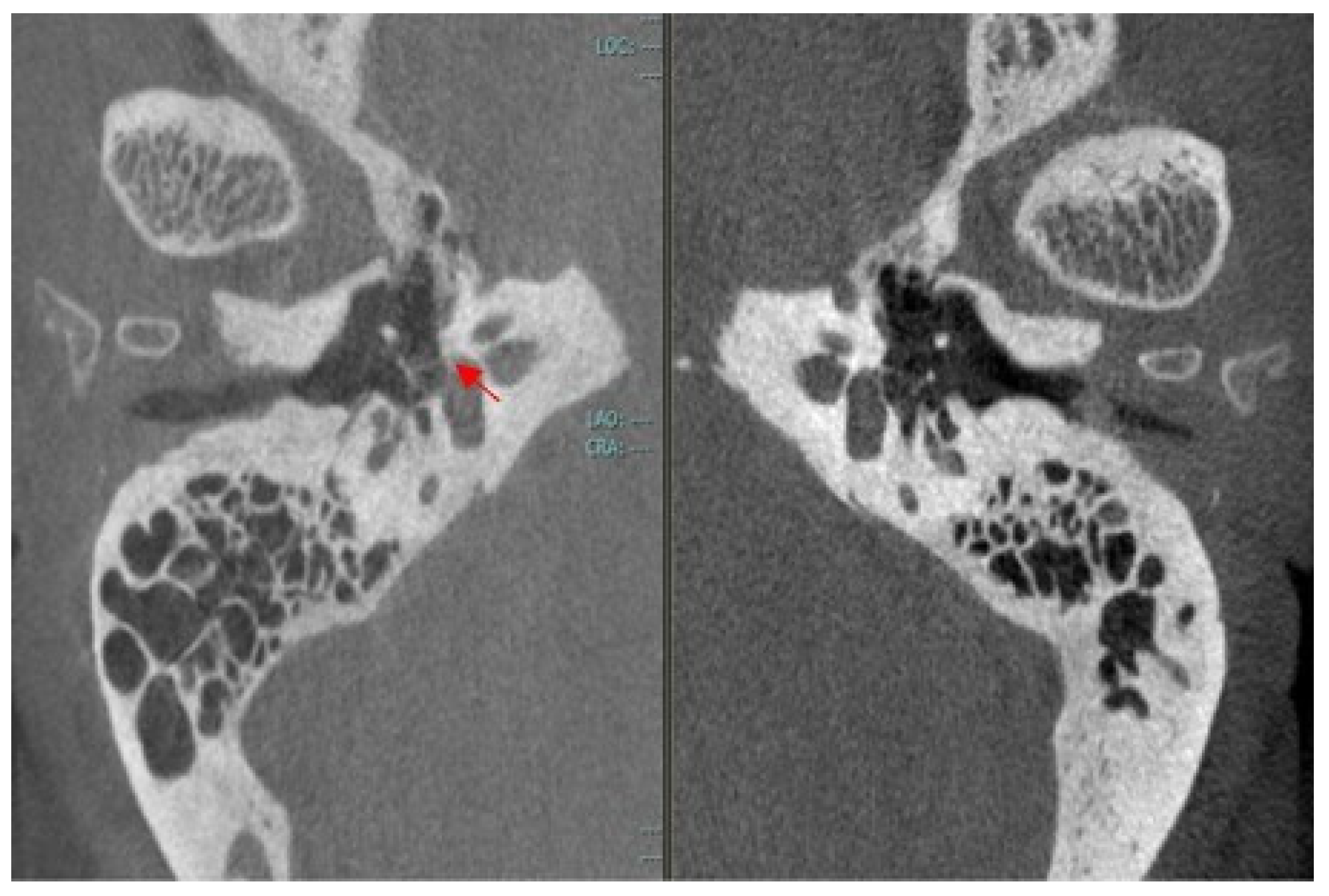
- Outbreak of otosclerosis (3 mm) around the fissula ante fenestram in the right ear (Figure 5).
- (a)
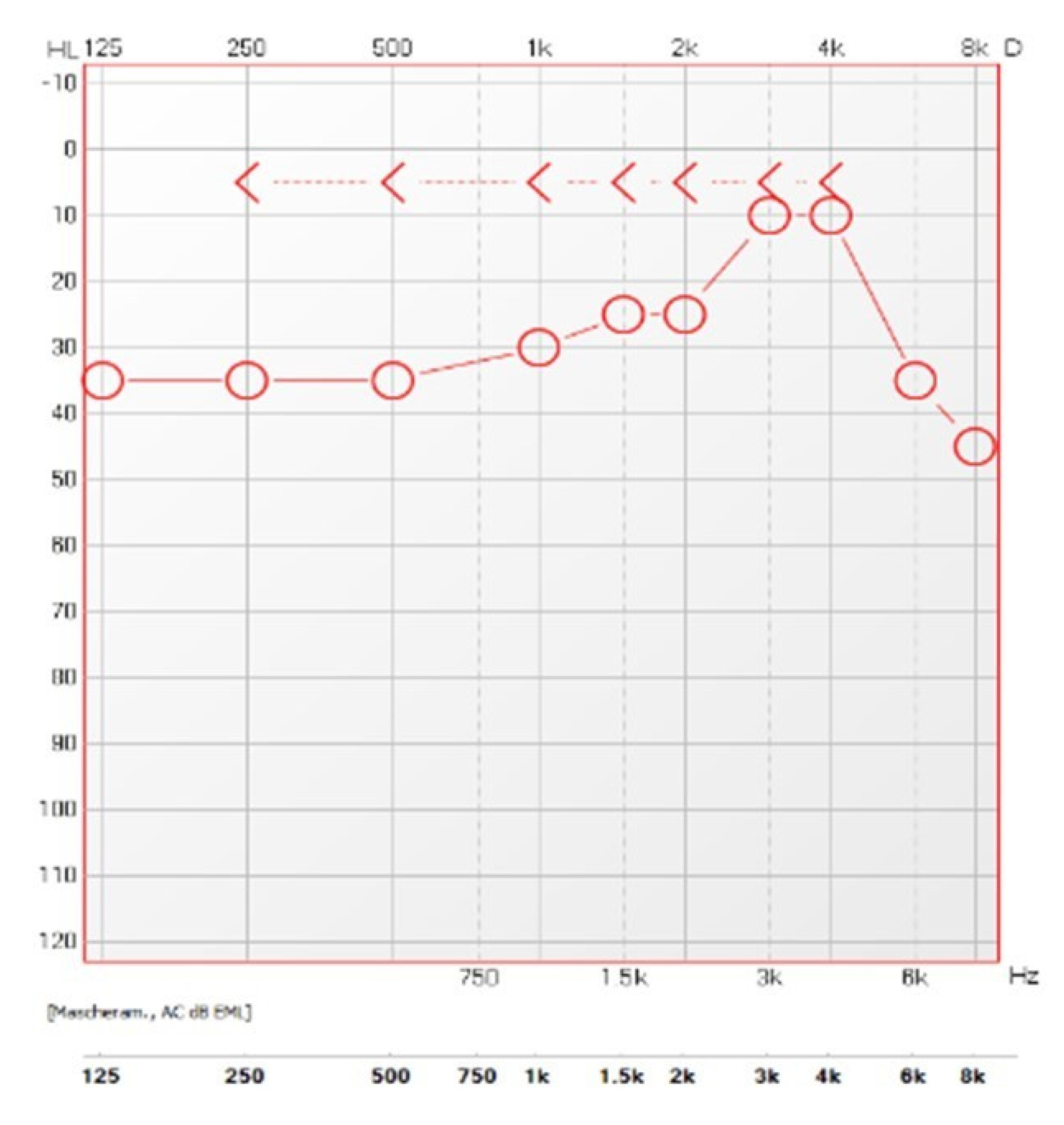
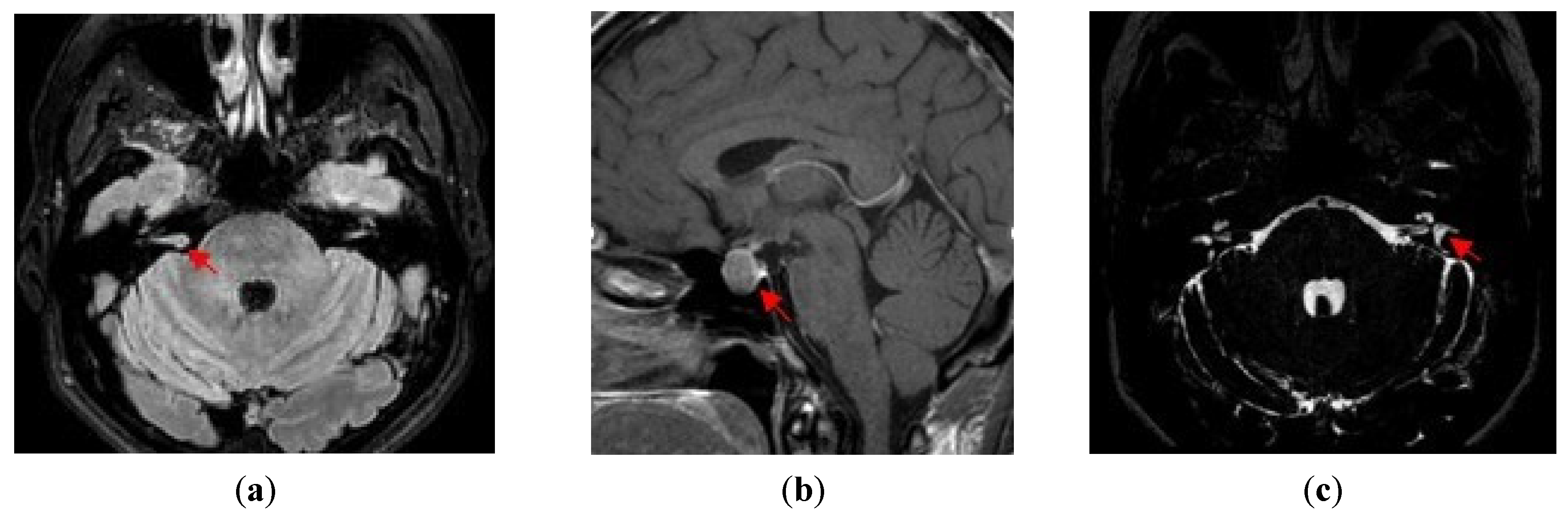
- Acoustic neuroma (right ear): sharply sloping sensorineural hearing loss, high-pitched tinnitus, and MRI findings;
- (b)
- Growth hormone-secreting macroadenoma of the pituitary gland: chronic headache, hyperhidrosis, amenorrhea, insomnia, broadened hands and feet, widened and stubby fingers, and MRI findings;
- (c)
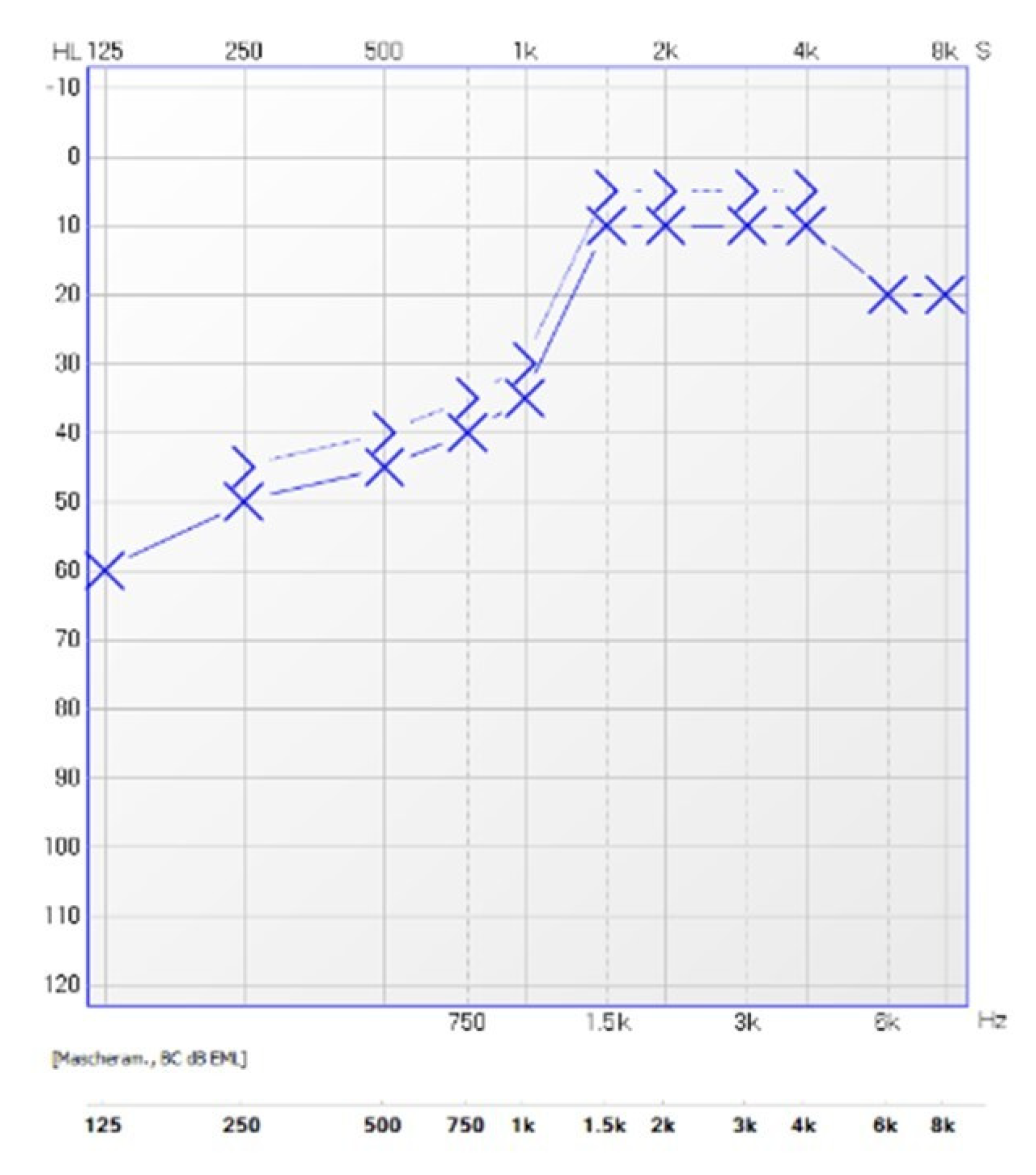
- Menière’s disease (left ear): low-frequency sensorineural hearing loss, spontaneous episodes of vertigo (each lasting between 20 min and 12 h), fluctuating aural symptoms (hearing, tinnitus and fullness) in the affected ear, and saccular hydrops detected by 3D FLAIR MRI evaluation;
- (d)
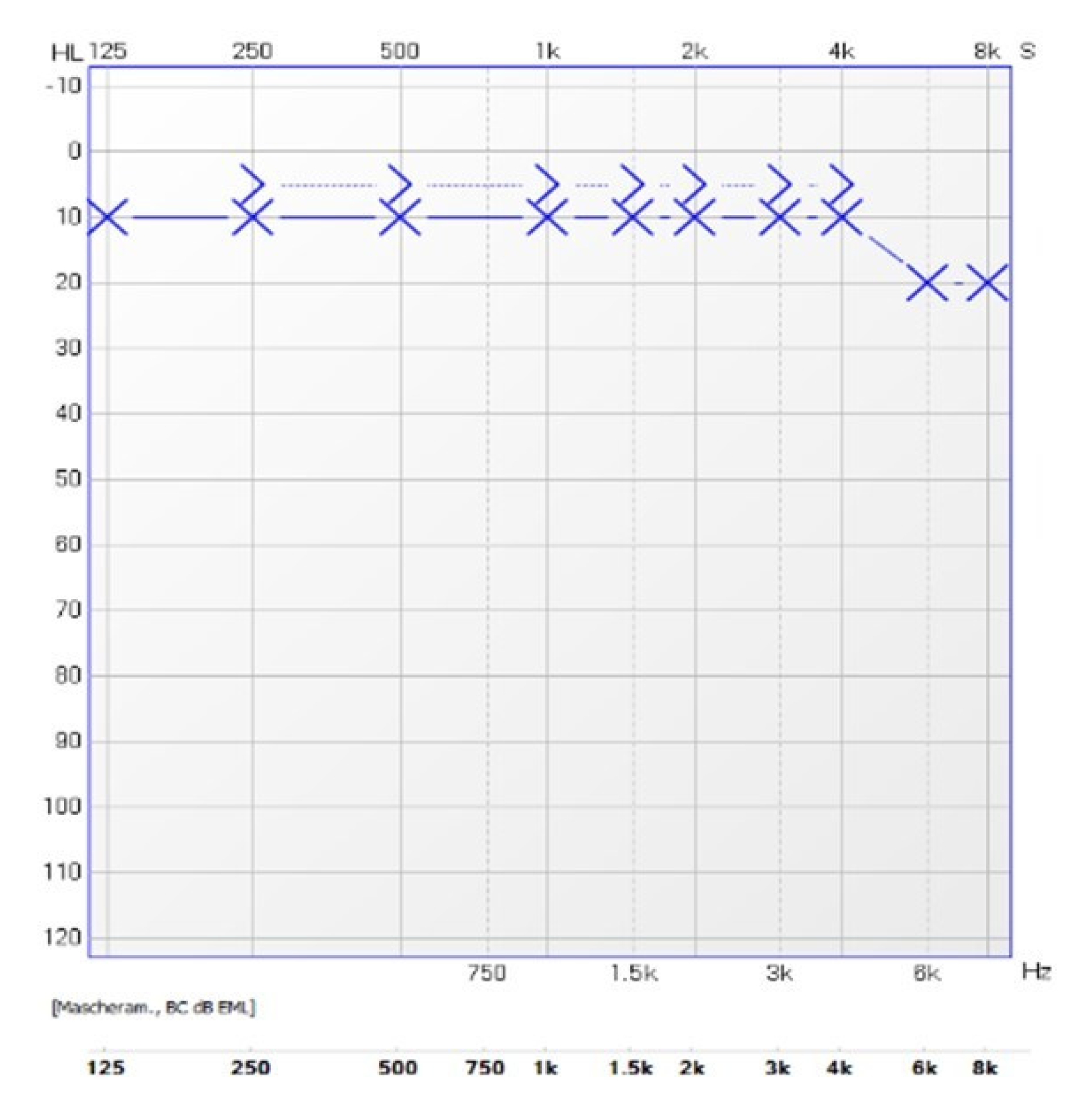
- Otosclerosis (right ear): Schwartze’s sign, low-frequency conductive hearing loss, type As tympanogram, absent acoustic reflexes, and outbreak of otosclerosis detected by CBCT scan.
- (1)
- Definite Menière’s disease:
- Two or more spontaneous episodes of vertigo, each lasting 20 min to 12 h.
- Audiometrically documented low-to-medium frequency sensorineural hearing loss in one ear, defining the affected ear on at least one occasion before, during or after one of the episodes of vertigo.
- Fluctuating aural symptoms (hearing, tinnitus, or fullness) in the affected ear.
- Not better accounted for by another vestibular diagnosis.
- (2)
- Probable Menière’s disease:
- Two or more episodes of vertigo or dizziness, each lasting 20 min to 24 h.
- Fluctuating aural symptoms (hearing, tinnitus, or fullness) in the affected ear.
- Not better accounted for by another vestibular diagnosis.
- At least five episodes fulfilling criteria C and D.
- A current or past history of Migraine without aura or Migraine with aura.
- Vestibular symptoms of moderate or severe intensity, lasting between 5 min and 72 h.
- At least half of episodes are associated with at least one of the following three migrainous features:
- headache with at least two of the following four characteristics:
- (a)
- unilateral location
- (b)
- pulsating quality
- (c)
- moderate or severe intensity
- (d)
- aggravation by routine physical activity
- photophobia and phonophobia
- visual aura
- Not better accounted for by another ICHD-3 diagnosis or by another vestibular disorder.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Campagnoli, M.; Cerasuolo, M.; Renna, M.; Dell’Era, V.; Valletti, P.A.; Garzaro, M. ENT Referral From Emergency Department During COVID-19: A Single-Center Experience. Ear Nose Throat J. 2023, 102, NP95–NP98. [Google Scholar] [CrossRef] [PubMed]
- Aldè, M.; Barozzi, S.; Berardino, F.D.; Zuccotti, G.; Gonsonni, D.; Ambrosetti, U.; Socci, M.; Bertoli, S.; Battezzati, A.; Foppiani, A.; et al. Prevalence of symptoms in 1512 COVID-19 patients: Have dizziness and vertigo been underestimated thus far? Int. Emerg. Med. 2022, 17, 1343–1353. [Google Scholar] [CrossRef] [PubMed]
- Han, B.I.; Lee, H.W.; Ryu, S.; Kim, J.S. Tinnitus Update. J. Clin. Neurol. 2021, 17, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Aldè, M.; Didier, H.A.; Giannì, A.B.; Sessa, F.; Borromeo, G.; Didier, A.H.; Barozzi, S.; Zanetti, D.; Di Berardino, F. Prevalence of New-Onset Otological Symptoms in Patients with Temporomandibular Disorders. J. Otorhinolaryngol. Hear. Balance Med. 2022, 3, 3. [Google Scholar] [CrossRef]
- Aldè, M.; Di Berardino, F.; Ambrosetti, U.; Barozzi, S.; Piatti, G.; Zanetti, D.; Pignataro, L.; Cantarella, G. Audiological and vestibular symptoms following SARS-CoV-2 infection and COVID-19 vaccination in children aged 5–11 years. Am. J. Otolaryngol. 2023, 44, 103669. [Google Scholar] [CrossRef]
- Greene, J.; Al-Dhahir, M.A. Acoustic, Neuroma; StatPearls Publishing: Treasure Island, FL, USA, 2022; [Updated 4 June 2022]. Available online: https://www.ncbi.nlm.nih.gov/books/NBK470177/ (accessed on 1 March 2023).
- Albera, R.; Luca, D.; Andrea, A.; Ettore, C.; Alfonso, S.; Ralli, M. What factors influence treatment decision making in acoustic neuroma? Our experience on 103 cases. Int. Tinnitus J. 2020, 24, 21–25. [Google Scholar] [CrossRef]
- Mehta, G.U.; Lonser, R.R. Management of hormone-secreting pituitary adenomas. Neuro Oncol. 2017, 19, 762–773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adigun, O.O.; Nguyen, M.; Fox, T.J.; Anastasopoulou, C. Acromegaly; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Paparella, M.M. Pathogenesis of Meniere’s disease and Meniere’s syndrome. Acta Otolaryngol. 1984, 406, 10–25. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Escamez, J.A.; Carey, J.; Chung, W.H.; Goebel, J.A.; Magnusson, M.; Mandalà, M.; Newman-Toker, D.E.; Strupp, M.; Suzuki, M.; Trabalzini, F.; et al. Diagnostic criteria for Menière’s disease. J. Vestib. Res. 2015, 25, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakashima, T.; Pyykkö, I.; Arroll, M.A.; Casselbrant, M.L.; Foster, C.A.; Manzoor, N.F.; Megerian, C.A.; Naganawa, S.; Young, Y.H. Meniere’s Disease. Nat. Views Dis. Prim. 2016, 2, 16028. [Google Scholar] [CrossRef] [PubMed]
- Tabet, P.; Saliba, I. Meniere’s Disease and Vestibular Migraine: Updates and Review of the Literature. J. Clin. Med. Res. 2017, 9, 733–744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnold, M. Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders. Cephalalgia 2018, 38, 1–211. [Google Scholar] [CrossRef]
- Gürkov, R.; Kantner, C.; Strupp, M.; Flatz, W.; Krause, E.; Ertl-Wagner, B. Endolymphatic hydrops in patients with vestibular migraine and auditory symptoms. Eur. Arch. Otorhinolaryngol. 2014, 271, 2661–2667. [Google Scholar] [CrossRef] [PubMed]
- Zafar, N.; Jamal, Z.; Khan, M.A.B. Otosclerosis; StatPearls Publishing: Treasure Island, FL, USA, 2022; [Updated 25 July 2022]. Available online: https://www.ncbi.nlm.nih.gov/books/NBK560671/ (accessed on 1 March 2023).
- Batson, L.; Rizzolo, D. Otosclerosis: An update on diagnosis and treatment. JAAPA 2017, 30, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Koenen, L.; Gupta, G. Schwartze Sign; StatPearls Publishing: Treasure Island, FL, USA, 2022; [Updated 5 September 2022]. Available online: https://www.ncbi.nlm.nih.gov/books/NBK532921/ (accessed on 1 March 2023).
- Amit, A.; Achawal, S.; Dorward, N. Pituitary macro adenoma and vestibular schwannoma: A case report of dual intracranial pathologies. Br. J. Neurosurg. 2008, 22, 695–696. [Google Scholar] [CrossRef] [PubMed]
- Niu, Y.; Ma, L.; Mao, Q.; Wu, L.; Chen, J. Pituitary adenoma and vestibular schwannoma: Case report and review of the literature. J. Postgrad. Med. 2010, 56, 281–283. [Google Scholar] [CrossRef] [PubMed]
- Carlson, M.L.; Patel, N.S.; Glasgow, A.E.; Habermann, E.B.; Grossardt, B.R.; Link, M.J. Vestibular schwannoma and pituitary adenoma in the same patient: Coincidence or novel clinical association? J. Neuro Ooncol. 2016, 128, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Klockars, T.; Kentala, E. Case report: Meniere’s disease and otosclerosis—Different outcomes of the same disease? Auris Nasus Larynx 2007, 34, 101–104. [Google Scholar] [CrossRef] [PubMed]
- Horner, K.C.; Guieu, R.; Magnan, J.; Chays, A.; Cazals, Y. Prolactinoma in some Ménière’s patients—Is stress involved? Neuropsychopharmacology 2002, 26, 135–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dispenza, F.; De Stefano, A.; Flanagan, S.; Romano, G.; Sanna, M. Decision making for solitary vestibular schwannoma and contralateral Meniere’s disease. Audiol. Neurootol. 2008, 13, 53–57. [Google Scholar] [CrossRef] [PubMed]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aldè, M.; Pignataro, L.; Zanetti, D. Tinnitus, Aural Fullness, and Hearing Loss in a Patient with Acoustic Neuroma and Pituitary Macroadenoma. J. Otorhinolaryngol. Hear. Balance Med. 2023, 4, 2. https://doi.org/10.3390/ohbm4010002
Aldè M, Pignataro L, Zanetti D. Tinnitus, Aural Fullness, and Hearing Loss in a Patient with Acoustic Neuroma and Pituitary Macroadenoma. Journal of Otorhinolaryngology, Hearing and Balance Medicine. 2023; 4(1):2. https://doi.org/10.3390/ohbm4010002
Chicago/Turabian StyleAldè, Mirko, Lorenzo Pignataro, and Diego Zanetti. 2023. "Tinnitus, Aural Fullness, and Hearing Loss in a Patient with Acoustic Neuroma and Pituitary Macroadenoma" Journal of Otorhinolaryngology, Hearing and Balance Medicine 4, no. 1: 2. https://doi.org/10.3390/ohbm4010002
APA StyleAldè, M., Pignataro, L., & Zanetti, D. (2023). Tinnitus, Aural Fullness, and Hearing Loss in a Patient with Acoustic Neuroma and Pituitary Macroadenoma. Journal of Otorhinolaryngology, Hearing and Balance Medicine, 4(1), 2. https://doi.org/10.3390/ohbm4010002