
A Tunable Self-Offloading Module for Plantar Pressure Regulation in Diabetic Patients

 , , , , ,
, , , , ,  , and
, and
Abstract
:1. Introduction
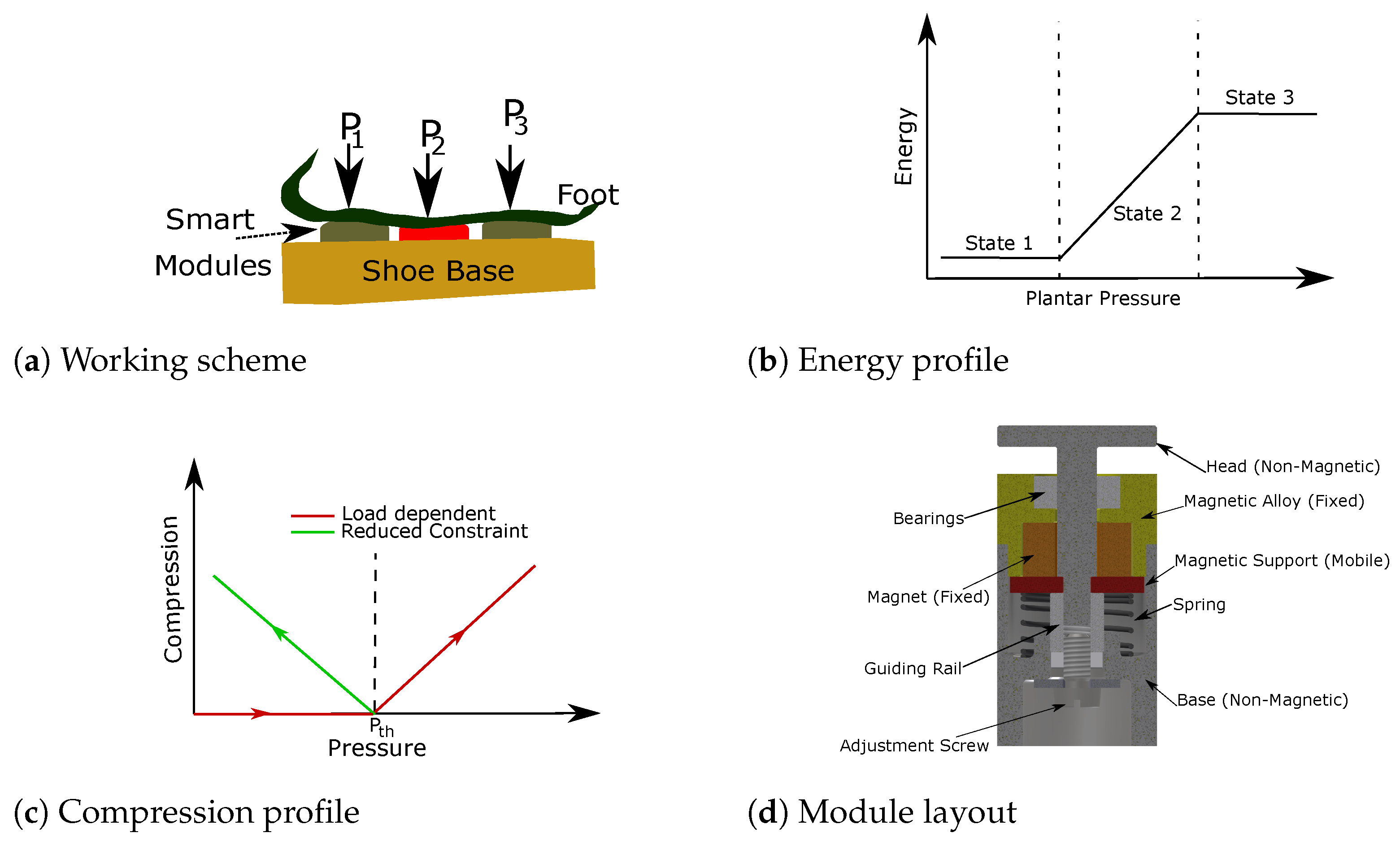
2. System Design and Concept
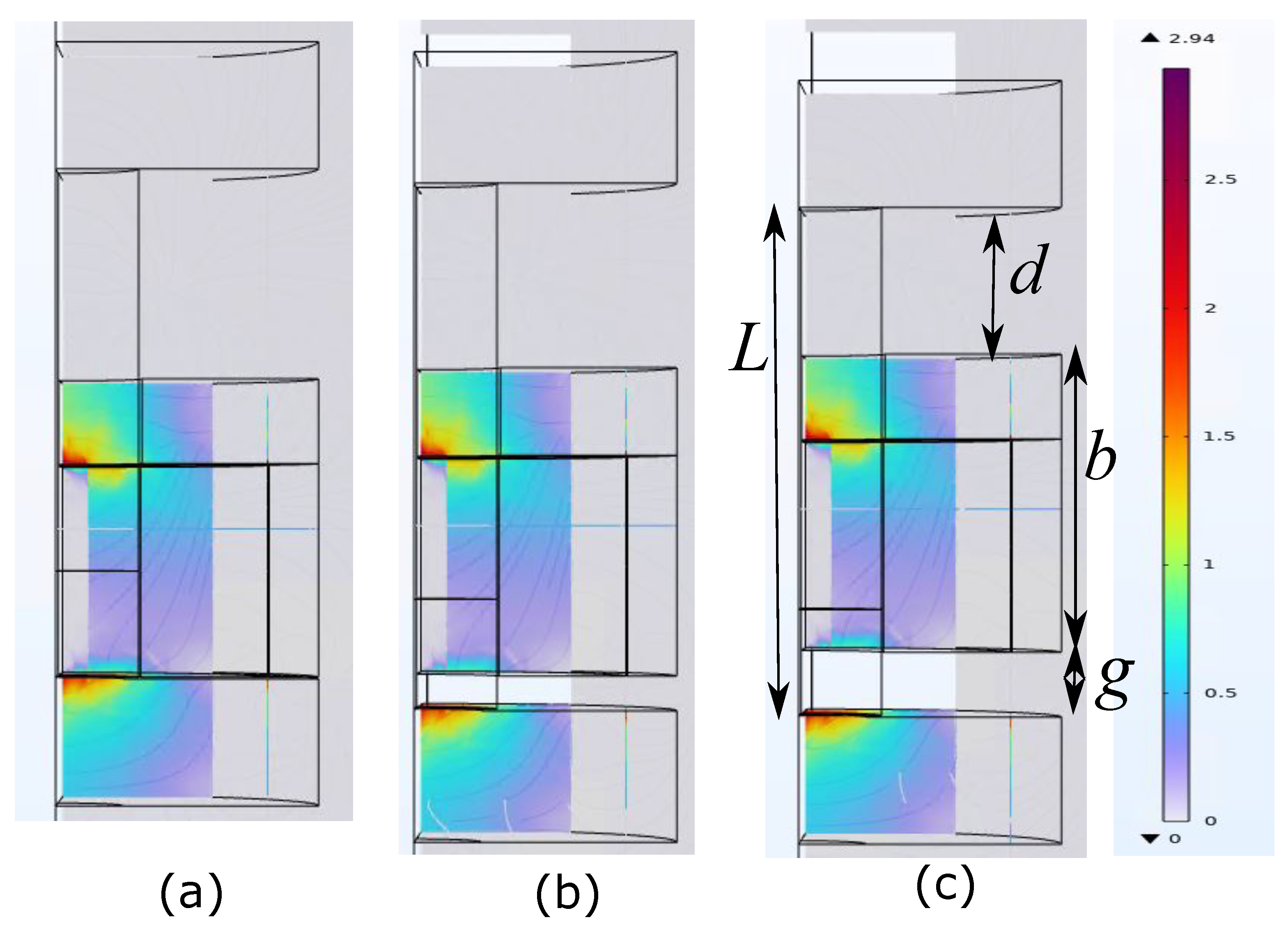
3. Modeling and Simulation
4. Experimental Studies
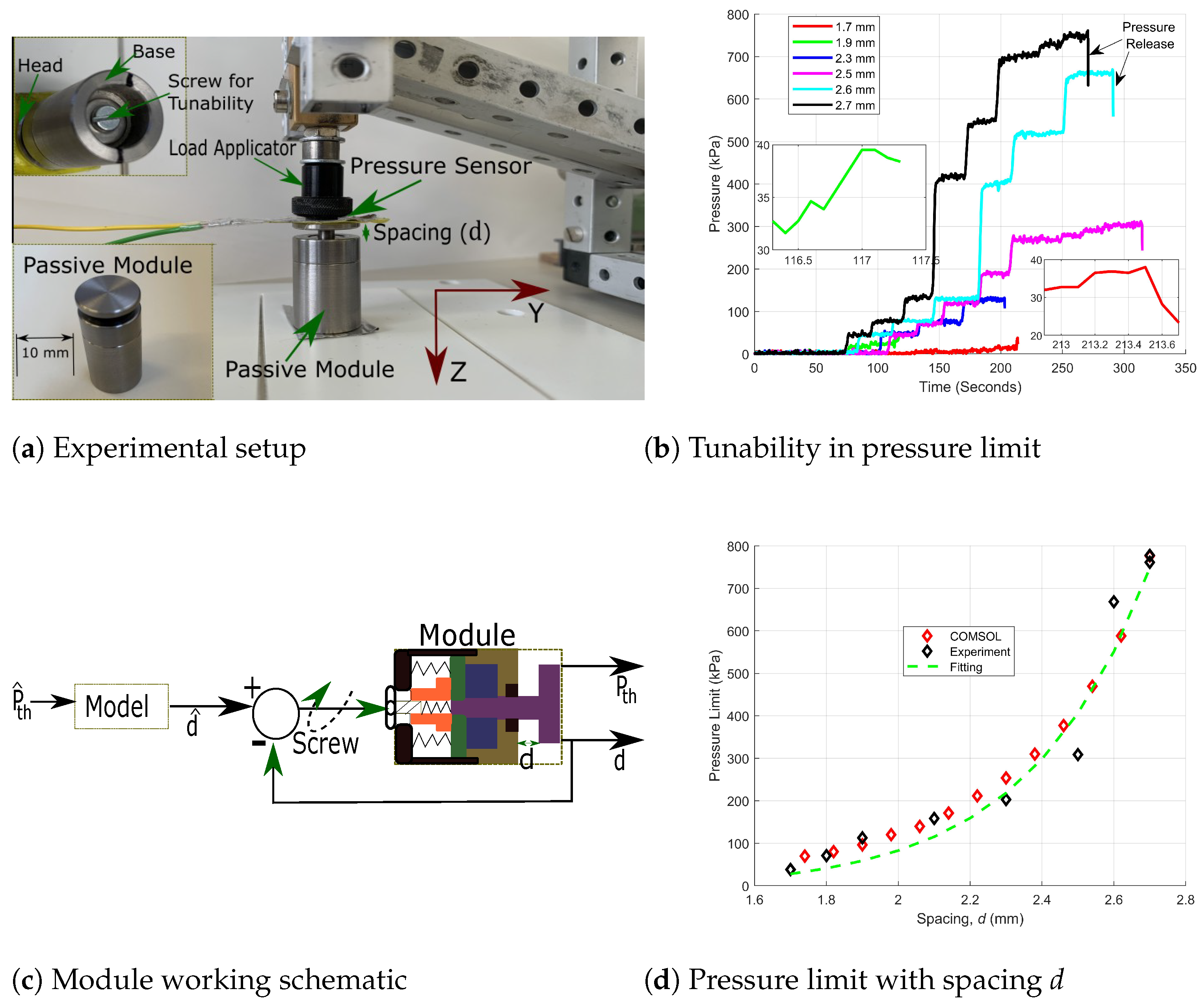
4.1. Tunability and Calibration
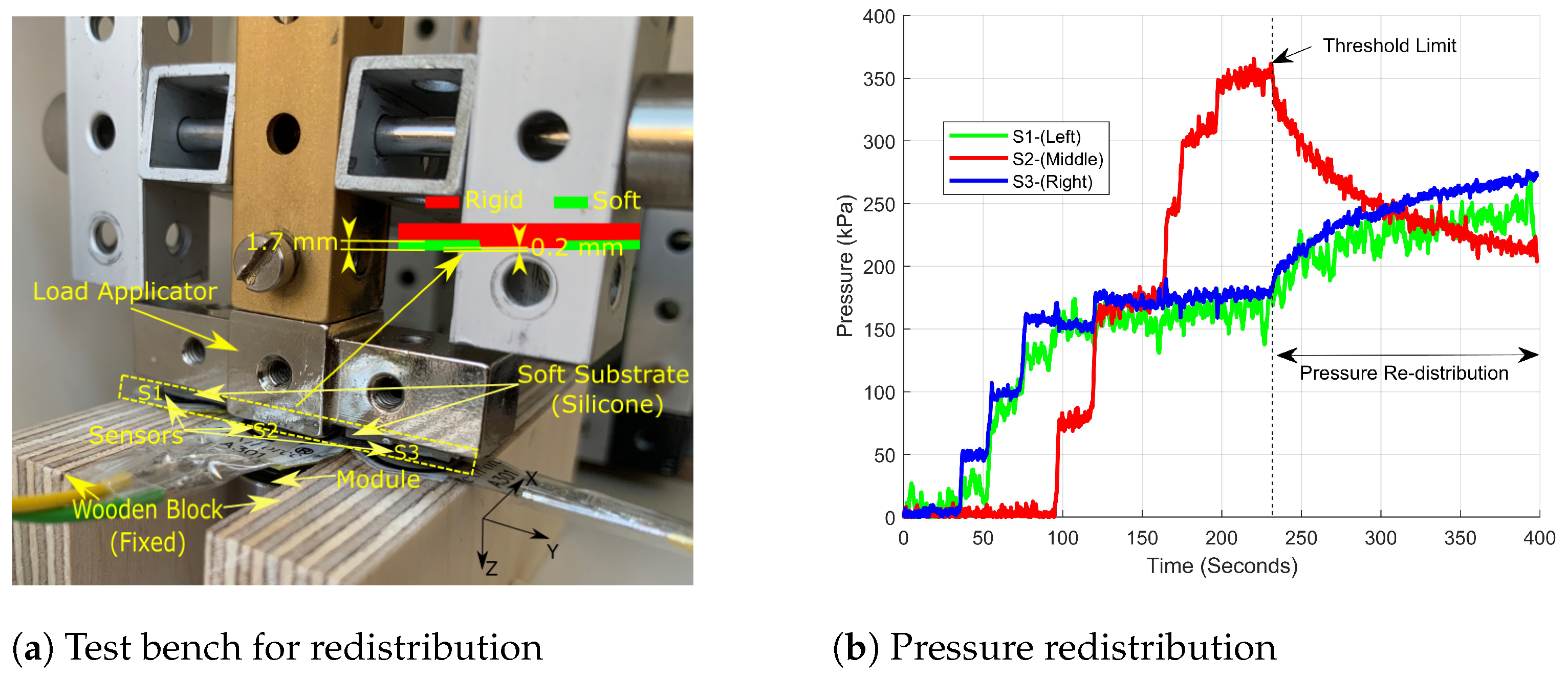
4.2. Pressure Redistribution
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- GBD 2021 Diabetes Collaborators. Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: A systematic analysis for the Global Burden of Disease Study 2021. Lancet 2023, 402, 203–234. [Google Scholar] [CrossRef] [PubMed]
- Mekkes, J.R.; Loots, M.A.M.; Wal, A.C.V.D.; Bos, J.D. Causes, investigation and treatment of leg ulceration. Br. J. Dermatol. 2003, 148, 388–401. [Google Scholar] [CrossRef]
- Jouven, X.; Lemaître, R.N.; Rea, T.D.; Sotoodehnia, N.; Empana, J.P.; Siscovick, D.S. Diabetes, glucose level, and risk of sudden cardiac death. Eur. Heart J. 2005, 26, 2142–2147. [Google Scholar] [PubMed]
- Hou, Y.; Zhou, M.; Xie, J.; Chao, P.; Feng, Q.; Wu, J. High glucose levels promote the proliferation of breast cancer cells through GTPases. Breast Cancer 2017, 9, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, D.G.; Lipsky, B.A. Diabetic foot infections: Stepwise medical and surgical management. Int. Wound J. 2004, 1, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Chamberlain, R.C.; Fleetwood, K.; Wild, S.H.; Colhoun, H.M.; Lindsay, R.S.; Petrie, J.R.; McCrimmon, R.J.; Gibb, F.; Philip, S.; Sattar, N.; et al. Foot Ulcer and Risk of Lower Limb amputation or Death in People With Diabetes: A National Population-Based Retrospective Cohort Study. Diabetes Care 2022, 45, 83–91. [Google Scholar] [CrossRef]
- Chen, L.; Sun, S.; Ran, X. Global mortality of diabetic foot ulcer: A systematic review and meta-analysis of observational studies. Diabetes Obes. Metab. 2023, 25, 36–45. [Google Scholar]
- Wu, H.; Ni, R.; Shi, Y.; Hu, Y.; Shen, Z.; Pang, Q.; Zhu, Y. The Promising Hydrogel Candidates for Preclinically Treating Diabetic Foot Ulcer: A Systematic Review and Meta-Analysis. Adv. Wound Care 2023, 12, 28–37. [Google Scholar] [CrossRef]
- Abid, H.M.U.; Hanif, M.; Mahmood, K.; Aziz, M.; Abbas, G.; Latif, H. Wound-Healing and Antibacterial Activity of the Quercetin-4-Formyl Phenyl Boronic Acid Complex against Bacterial Pathogens of Diabetic Foot Ulcer. ACS Omega 2022, 7, 24415–24422. [Google Scholar] [CrossRef]
- Becerra-Bayona, S.M.; Solarte-David, V.A.; Sossa, C.L.; Mateus, L.C.; Villamil, M.; Pereira, J.; Arango-Rodríguez, M.L. Mesenchymal stem cells derivatives as a novel and potential therapeutic approach to treat diabetic foot ulcers. Endocrinol. Diabetes Metab. Case Rep. 2020, 2020. [Google Scholar] [CrossRef]
- Yuan, Y.; Ding, X.; Jing, Z.; Lu, H.; Yang, K.; Wang, Y.; Xu, H. Modified tibial transverse transport technique for the treatment of ischemic diabetic foot ulcer in patients with type 2 diabetes. J. Orthop. Transl. 2021, 29, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Yang, Y.; Yuan, K.; Yang, S.; Tang, T. Dual-functional hybrid quaternized chitosan/Mg/alginate dressing with antibacterial and angiogenic potential for diabetic wound healing. J. Orthop. Transl. 2021, 30, 6–15. [Google Scholar] [CrossRef] [PubMed]
- Lazo-Porras, M.; Bernabe-Ortiz, A.; Taype-Rondan, A.; Gilman, R.H.; Malaga, G.; Manrique, H.; Neyra, L.; Calderon, J.; Pinto, M.; Armstrong, D.G.; et al. Foot thermometry with mHeath-based supplementation to prevent diabetic foot ulcers: A randomized controlled trial. Wellcome Open Res. 2020, 5, 23. [Google Scholar] [CrossRef]
- Chatwin, K.E.; Abbott, C.A.; Boulton, A.J.M.; Bowling, F.L.; Reeves, N.D. The role of foot pressure measurement in the prediction of diabetic foot ulceration-A comprehensive review. Diabetes/Metabolism Res. Rev. 2020, 36, e3258. [Google Scholar]
- Robinson, C.C.; Balbinot, L.F.; Silva, M.F.; Achaval, M.; Zaro, M.A. Plantar Pressure Distribution Patterns of Individuals with Prediabetes in Comparison with Healthy Individuals and Individuals with Diabetes. J. Diabetes Sci. Technol. 2013, 7, 1113–1121. [Google Scholar]
- Bharara, M.; Najafi, B.; Armstrong, D.G. Methodology for Use of a Neuroprosthetic to Reduce Plantar Pressure: Applications in Patients with Diabetic Foot Disease. J. Diabetes Sci. Technol. 2012, 6, 222–224. [Google Scholar]
- Heck, I.; Lu, W.; Wang, Z.; Zhang, X.; Adak, T.; Cu, T.; Crumley, C.; Zhang, Y.; Wang, X.S. Soft, Wireless Pressure-Sensor-Integrated Smart Bandage for the Management of Diabetic Foot Ulcers. Adv. Mater. Technol. 2022, 8, 2200821. [Google Scholar] [CrossRef]
- Mahmud, S.; Khandakar, A.; Chowdhury, M.E.H.; Moniem, M.A.; Reaz, M.B.I.; Mahbub, Z.B.; Sadasivuni, K.K.; Murugappan, M.; Alhatou, M. Fiber Bragg Gratings based smart insole to measure plantar pressure and temperature. Sens. Actuators A Phys. 2023, 350, 114092. [Google Scholar]
- Nga, D.T.N.; Mattana, G.; Thu, V.T.; Roussel, R.; Piro, B. A simple flexible printed capacitive pressure sensor for chronic wound monitoring. Sens. Actuators A Phys. 2022, 338, 113490. [Google Scholar]
- Ferber, R.; Webber, T.; Kin, B.; Everett, B.; Groenland, M. Validation of Plantar Pressure Measurements for a Novel In-Shoe Plantar Sensory Replacement Unit. J. Diabetes Sci. Technol. 2013, 7, 1167–1175. [Google Scholar] [CrossRef]
- Park, C.; Mishra, R.; Vigana, D.; Macagno, M.; Rossotti, S.; D’Huyvetter, K.; Armstrong, J.G.D.G.; Najafi, B. Smart Offloading Boot System for Remote Patient Monitoring: Toward Adherence Reinforcement and Proper Physical Activity Prescription for Diabetic Foot Ulcer Patientst. J. Diabetes Sci. Technol. 2022, 17, 42–51. [Google Scholar] [PubMed]
- Tiwari, B.; Ntella, S.L.; Jeanmonod, K.; Germano, P.; Koechli, C.; Pataky, Z.; Perriard, Y.C.Y. A Polyester-Nylon Blend Plantar Pressure Sensing Insole for Person with Diabetes. IEEE Sens. Lett. 2024, 8, 1–4. [Google Scholar] [CrossRef]
- Lazzarini, P.A.; Jarl, G.; Gooday, C.; Viswanathan, V.; Caravaggi, C.F.; Armstrong, D.G.; Bus, S.A. Effectiveness of offloading interventions to heal foot ulcers in persons with diabetes: A systematic review. Diabetes Metab. Res. Rev. 2020, 36, e3275. [Google Scholar] [CrossRef] [PubMed]
- Lazzarini, P.A.; Jarl, G. Knee-High Devices Are Gold in Closing the Foot Ulcer Gap: A Review of Offloading Treatments to Heal Diabetic Foot Ulcers. Medicina 2021, 57, 941. [Google Scholar] [CrossRef] [PubMed]
- Low, J.H.; Khin, P.M.; Yeow, C.H. A Pressure-Redistributing Insole using Soft Sensors and Actuators. In Proceedings of the 2015 IEEE International Conference on Robotics and Automation (ICRA), Seattle, WA, USA, 26–30 May 2015. [Google Scholar]
- Mo, Y.; Qaiser, Z.; Ou, H.; Johnson, S. A Reconfigurable and Adjustable Compliance System for the Measurement of Interface Orthotic Properties. IEEE Trans. Neural Syst. Rehabil. Eng. 2021, 29, 1886–1894. [Google Scholar] [PubMed]
- Perriard, Y.; Pataky, Z.; Grivon, D.; Civet, Y.R.C. System for Adjusting Pressure Locally on the Skin and Subcutaneous Tissue. U.S. Patent 2017/0348181 A1, 16 March 2021. [Google Scholar]
- Zur, L. Programmable Pressure Management Support Surface. U.S. Patent 10,463,526 B1, 1 October 2021. [Google Scholar]
- Hemler, S.; Ntella, S.L.; Jeanmonod, K.; Köchli, C.; Tiwari, B.; Civet, Y.; Perriard, Y.; Pataky, Z. Intelligent plantar pressure offloading for the prevention of diabetic foot ulcers and amputations. Front. Endocrinol. 2023, 14, 1166513. [Google Scholar]
- Zhang, X.; Wang, H.; Du, C.; Fan, X.; Cui, L.; Chen, H.; Deng, F.; Tong, Q.; He, M.; Yang, M.; et al. Custom-Molded Offloading Footwear Effectively Prevents Recuurence and Amputation, and Lowers Mortality Rates in High-Risk Diabetic Foot Patients: A Multicenter, Prospective Observational Study. Diabetic Metab. Syndr. Obes. Targets Ther. 2022, 15, 103–109. [Google Scholar]
- Roser, M.C.; Canavan, P.K.; Najafi, B.; Watchman, M.C.; Vaishnav, K.; Armstrong, D.G. Novel In-Shoe Exoskeleton for Offloading of Forefoot Pressure for Individuals With Diabetic Foot Pathology. J. Diabetes Sci. Technol. 2017, 11, 874–882. [Google Scholar]
- Shaulian, H.; Gefen, A.; Biton, H.; Wolf, A. Graded stiffness offloading insoles better redistribute heel plantar pressure to protect the diabetic neuropathic foot. Gait Posture 2023, 101, 28–34. [Google Scholar] [CrossRef]
- Chatzistergos, P.E.; Gatt, A.; Formosa, C.; Farrugia, K.; Chockalingam, N. Optimised cushioning in diabetic footwear can significantly enhance their capacity to reduce plantar pressure. Gait Posture 2020, 79, 244–250. [Google Scholar] [CrossRef]
- Maharana, P.; Sonawane, J.; Belehalli, P.; Ananthasuresh, G.K. Self-offloading therapeutic footwear using compliant snap-through arches. Wearable Technol. 2022, 3, e7. [Google Scholar]
- Chatzistergos, P.E.; Chockalingam, N. A novel concept for low-cost non-electronic detection of overloading in the foot during activities of daily living. R. Soc. Open Sci. 2020, 8, 202035. [Google Scholar] [CrossRef]
- Wang, L.; Jones, D.; Chapman, G.J.; Siddle, H.J.; Russell, D.A.; Alazmani, A.; Culmer, P. A Review of Wearable Sensor Systems to Monitor Plantar Loading in the Assessment of Diabetic Foot Ulcers. IEEE Trans. Biomed. Eng. 2020, 67, 1989–2004. [Google Scholar] [CrossRef]
- Fernando, M.E.; Crowther, R.G.; Lazzarini, P.A.; Sangla, K.S.; Wearing, S.; Buttner, P.; Golledge, J. Plantar pressures are higher in cases with diabetic foot ulcers compared to controls despite a longer stance phase duration. BMC Endocr. Disord. 2016, 16, 51. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Recoil Permeability | 1.05 |
| Effective Remanent Flux Density (Norm) | 2.15 |
| Young Modulus (GPa) | 350 |
| Poisson’s Ratio | 0.35 |
| i (for ) | Value |
|---|---|
| 1 | 0.33 |
| 2 | 4.35 |
| 3 | 43.48 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tiwari, B.; Jeanmonod, K.; Germano, P.; Koechli, C.; Ntella, S.L.; Pataky, Z.; Civet, Y.; Perriard, Y. A Tunable Self-Offloading Module for Plantar Pressure Regulation in Diabetic Patients. Appl. Syst. Innov. 2024, 7, 9. https://doi.org/10.3390/asi7010009
Tiwari B, Jeanmonod K, Germano P, Koechli C, Ntella SL, Pataky Z, Civet Y, Perriard Y. A Tunable Self-Offloading Module for Plantar Pressure Regulation in Diabetic Patients. Applied System Innovation. 2024; 7(1):9. https://doi.org/10.3390/asi7010009
Chicago/Turabian StyleTiwari, Bhawnath, Kenny Jeanmonod, Paolo Germano, Christian Koechli, Sofia Lydia Ntella, Zoltan Pataky, Yoan Civet, and Yves Perriard. 2024. "A Tunable Self-Offloading Module for Plantar Pressure Regulation in Diabetic Patients" Applied System Innovation 7, no. 1: 9. https://doi.org/10.3390/asi7010009
APA StyleTiwari, B., Jeanmonod, K., Germano, P., Koechli, C., Ntella, S. L., Pataky, Z., Civet, Y., & Perriard, Y. (2024). A Tunable Self-Offloading Module for Plantar Pressure Regulation in Diabetic Patients. Applied System Innovation, 7(1), 9. https://doi.org/10.3390/asi7010009