
The Conometric Connection for the Implant-Supported Fixed Prosthesis: A Narrative Review

 ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Results
2.1. Absence of Cement or Screw
2.2. Marginal Adaptation and Bacterial Sealing
2.3. Retention Force
2.4. Digital Workflow
2.5. Follow-Up Evalutation
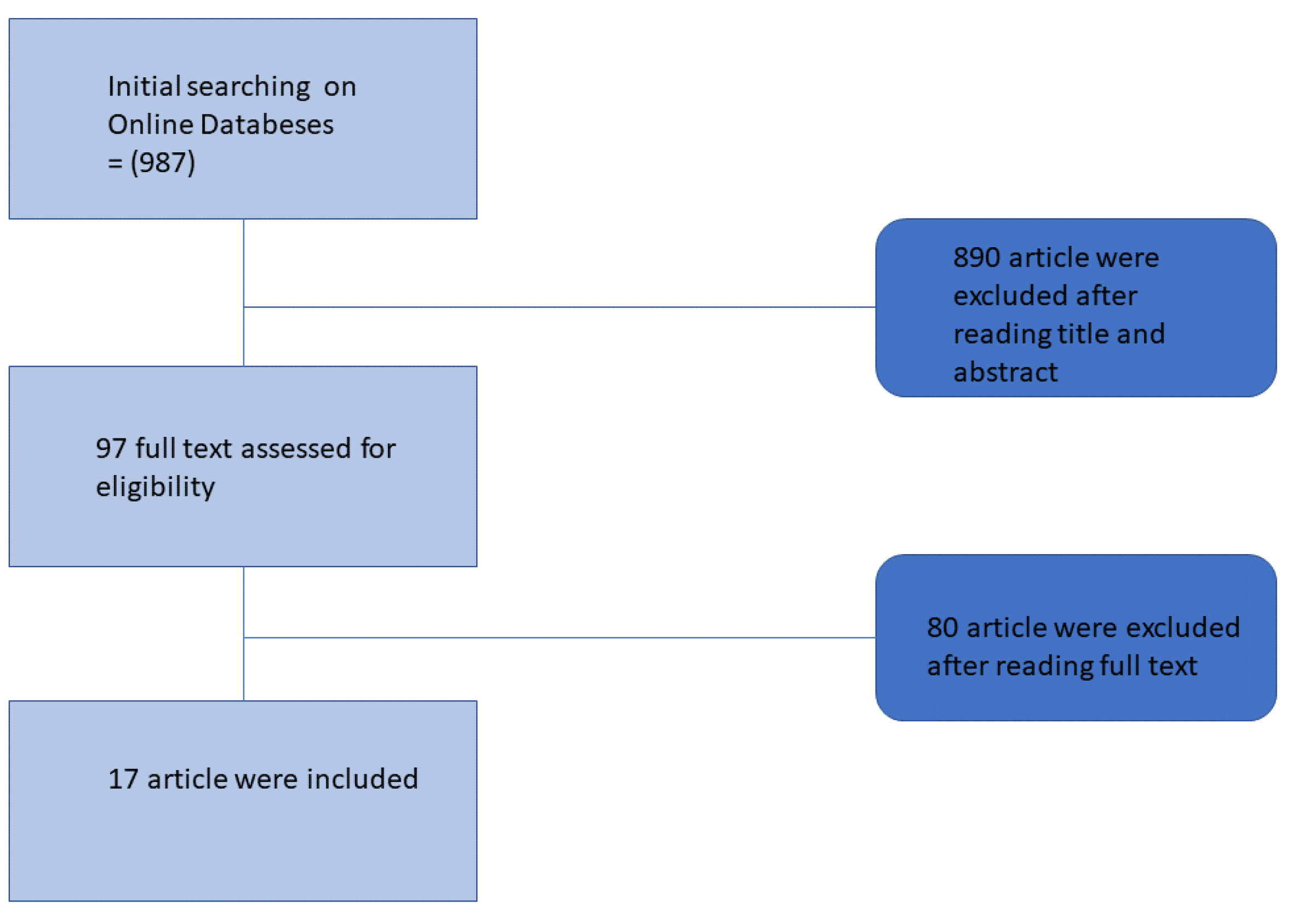
3. Materials and Methods
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pjetursson, B.E.; Thoma, D.; Jung, R.; Zwahlen, M.; Zembic, A. A Systematic Review of the Survival and Complication Rates of Implant-Supported Fixed Dental Prostheses (FDPs) after a Mean Observation Period of at Least 5 Years. Clin. Oral Implants Res. 2012, 23, 22–38. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, S.; Zampetti, P.; Rodriguez, Y.; Baena, R.; Svanosio, D.; Lupi, S.M. Retrospective Analysis of 521 Endosseous Implants Placed under Antibiotic Prophylaxis and Review of Literature. Minerva Stomatol. 2010, 59, 75–88. [Google Scholar] [PubMed]
- Pjetursson, B.E.; Brägger, U.; Lang, N.P.; Zwahlen, M. Comparison of Survival and Complication Rates of Tooth-Supported Fixed Dental Prostheses (FDPs) and Implant-Supported FDPs and Single Crowns (SCs). Clin. Oral Implants Res. 2007, 18, 97–113. [Google Scholar] [CrossRef] [PubMed]
- Butera, A.; Gallo, S.; Pascadopoli, M.; Luraghi, G.; Scribante, A. Ozonized Water Administration in Peri-Implant Mucositis Sites: A Randomized Clinical Trial. Appl. Sci. 2021, 11, 7812. [Google Scholar] [CrossRef]
- Butera, A.; Pascadopoli, M.; Pellegrini, M.; Gallo, S.; Zampetti, P.; Cuggia, G.; Scribante, A. Domiciliary Use of Chlorhexidine vs. Postbiotic Gels in Patients with Peri-Implant Mucositis: A Split-Mouth Randomized Clinical Trial. Appl. Sci. 2022, 12, 2800. [Google Scholar] [CrossRef]
- Gehrke, P.; Hartjen, P.; Smeets, R.; Gosau, M.; Peters, U.; Beikler, T.; Fischer, C.; Stolzer, C.; Geis-Gerstorfer, J.; Weigl, P.; et al. Marginal Adaptation and Microbial Leakage at Conometric Prosthetic Connections for Implant-Supported Single Crowns: An In Vitro Investigation. Int. J. Mol. Sci. 2021, 22, 881. [Google Scholar] [CrossRef] [PubMed]
- Salvi, G.E.; Cosgarea, R.; Sculean, A. Prevalence and Mechanisms of Peri-Implant Diseases. J. Dent. Res. 2017, 96, 31–37. [Google Scholar] [CrossRef]
- Albrektsson, T.; Canullo, L.; Cochran, D.; De Bruyn, H. “Peri-Implantitis”: A Complication of a Foreign Body or a Man-Made “Disease”. Facts and Fiction. Clin. Implant Dent. Relat. Res. 2016, 18, 840–849. [Google Scholar] [CrossRef]
- Urdaneta, R.A.; Marincola, M.; Weed, M.; Chuang, S.K. A Screwless and Cementless Technique for the Restoration of Single-Tooth Implants: A Retrospective Cohort Study. J. Prosthodont. 2008, 17, 562–571. [Google Scholar] [CrossRef]
- Sanz, M.; Chapple, I.L. Clinical Research on Peri-Implant Diseases: Consensus Report of Working Group 4. J. Clin. Periodontol. 2012, 39, 202–206. [Google Scholar] [CrossRef]
- Degidi, M.; Nardi, D.; Sighinolfi, G.; Degidi, D. The Conometric Concept for the Definitive Rehabilitation of a Single Posterior Implant by Using a Conical Indexed Abutment: A Technique. J. Prosthet. Dent. 2020, 123, 576–579. [Google Scholar] [CrossRef]
- Albiero, A.M.; Benato, R.; Momic, S.; Degidi, M. Guided-Welded Approach Planning Using a Computer-Aided Designed Prosthetic Shell for Immediately Loaded Complete-Arch Rehabilitations Supported by Conometric Abutments. J. Prosthet. Dent. 2019, 122, 510–515. [Google Scholar] [CrossRef]
- Michalakis, K.X.; Hirayama, H.; Garefis, P.D. Cement-Retained versus Screw-Retained Implant Restorations: A Critical Review. Int. J. Oral Maxillofac. Implants 2003, 18, 719–728. [Google Scholar]
- Jung, R.E.; Pjetursson, B.E.; Glauser, R.; Zembic, A.; Zwahlen, M.; Lang, N.P. A Systematic Review of the 5-Year Survival and Complication Rates of Implant-Supported Single Crowns. Clin. Oral Implants Res. 2008, 19, 119–130. [Google Scholar] [CrossRef]
- Chee, W.; Felton, D.A.; Johnson, P.F.; Sullivan, D.Y. Cemented versus Screw-Retained Implant Prostheses: Which Is Better? Int. J. Oral Maxillofac. Implants 1999, 14, 137–141. [Google Scholar]
- Wilson, T.G., Jr. The Positive Relationship Between Excess Cement and Peri-Implant Disease: A Prospective Clinical Endoscopic Study. J. Periodontol. 2009, 80, 1388–1392. [Google Scholar] [CrossRef]
- Bornstein, M.M.; Lussi, A.; Schmid, B.; Belser, U.C.; Buser, D. Early Loading of Nonsubmerged Titanium Implants with a Sandblasted and Acid-Etched (SLA) Surface: 3-Year Results of a Prospective Study in Partially Edentulous Patients. Int. J. Oral Maxillofac. Implants 2003, 18, 659–666. [Google Scholar]
- Abboud, M.; Koeck, B.; Stark, H.; Wahl, G.; Paillon, R. Immediate Loading of Single-Tooth Implants in the Posterior Region. Int. J. Oral Maxillofac. Implants 2005, 20, 61–68. [Google Scholar] [CrossRef]
- Agar, J.R.; Cameron, S.M.; Hughbanks, J.C.; Parker, M.H. Cement Removal from Restorations Luted to Titanium Abutments with Simulated Subgingival Margins. J. Prosthet. Dent. 1997, 78, 43–47. [Google Scholar] [CrossRef]
- Linkevicius, T.; Vindasiute, E.; Puisys, A.; Peciuliene, V. The Influence of Margin Location on the Amount of Undetected Cement Excess after Delivery of Cement-Retained Implant Restorations. Clin. Oral Implants Res. 2011, 22, 1379–1384. [Google Scholar] [CrossRef]
- White, D.J. Dental Calculus: Recent Insights into Occurrence, Formation, Prevention, Removal and Oral Health Effects of Supragingival and Subgingival Deposits. Eur. J. Oral Sci. 1997, 105, 508–522. [Google Scholar] [CrossRef]
- Tan, B.; Gillam, D.G.; Mordan, N.J.; Galgut, P.N. A Preliminary Investigation into the Ultrastructure of Dental Calculus and Associated Bacteria. J. Clin. Periodontol. 2004, 31, 364–369. [Google Scholar] [CrossRef]
- Schedle, A.; Franz, A.; Rausch-Fan, X.; Andreas, S.; Lucas, T.; Samorapoompichit, P.; Sperr, W.; Boltz-Nitulescu, G. Cytotoxic Effects of Dental Composites, Adhesive Substances, Compomers and Cements. Dent. Mater. 1998, 14, 429–440. [Google Scholar] [CrossRef]
- Canullo, L.; Peñarrocha, M.; Monje, A.; Catena, A.; Wang, H.-L.; Peñarrocha, D. Association Between Clinical and Microbiologic Cluster Profiles and Peri-Implantitis. Int. J. Oral Maxillofac. Implants 2017, 32, 1054–1064. [Google Scholar] [CrossRef]
- Caricasulo, R.; Malchiodi, L.; Ghensi, P.; Fantozzi, G.; Cucchi, A. The Influence of Implant-Abutment Connection to Peri-Implant Bone Loss: A Systematic Review and Meta-Analysis. Clin. Implant Dent. Relat. Res. 2018, 20, 653–664. [Google Scholar] [CrossRef]
- Gehrke, P.; Burg, S.; Peters, U.; Beikler, T.; Fischer, C.; Rupp, F.; Schweizer, E.; Weigl, P.; Sader, R.; Smeets, R.; et al. Bacterial Translocation and Microgap Formation at a Novel Conical Indexed Implant Abutment System for Single Crowns. Clin. Oral Investig. 2021, 26, 1375–1389. [Google Scholar] [CrossRef]
- Bressan, E.; Stocchero, M.; Jimbo, R.; Rosati, C.; Fanti, E.; Tomasi, C.; Lops, D. Microbial Leakage at Morse Taper Conometric Prosthetic Connection: An in Vitro Investigation. Implant Dent. 2017, 26, 756–761. [Google Scholar] [CrossRef]
- Schriwer, C.; Skjold, A.; Gjerdet, N.R.; Øilo, M. Monolithic Zirconia Dental Crowns. Internal Fit, Margin Quality, Fracture Mode and Load at Fracture. Dent. Mater. 2017, 33, 1012–1020. [Google Scholar] [CrossRef]
- Nardi, D.; Degidi, M.; Sighinolfi, G.; Tebbel, F.; Marchetti, C. Retention Strength of Conical Welding Caps for Fixed Implant-Supported Prostheses. Int. J. Prosthodont. 2017, 30, 553–555. [Google Scholar] [CrossRef]
- Bressan, E.; Lops, D.; Tomasi, C.; Ricci, S.; Stocchero, M.; Carniel, E.L. Experimental and Computational Investigation of Morse Taper Conometric System Reliability for the Definition of Fixed Connections between Dental Implants and Prostheses. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2014, 228, 674–681. [Google Scholar] [CrossRef]
- Antonaya-Martin, J.; Del Rio-Highsmith, J.; Moreno-Hay, I.; Lillo-Rodríguez, J.; Gomez-Polo, M.; Celemin-Viñuela, A. CAD/CAM Conic Crowns for Predictable Retention in Implant-Supported Prostheses. Int. J. Prosthodont. 2016, 29, 230–232. [Google Scholar] [CrossRef]
- Beuer, F.; Edelhoff, D.; Gernet, W.; Naumann, M. Parameters Affecting Retentive Force of Electroformed Double-Crown Systems. Clin. Oral Investig. 2010, 14, 129–135. [Google Scholar] [CrossRef]
- Albiero, A.M.; Benato, R.; Momic, S.; Degidi, M. Implementation of Computer-Guided Implant Planning Using Digital Scanning Technology for Restorations Supported by Conical Abutments: A Dental Technique. J. Prosthet. Dent. 2018, 119, 720–726. [Google Scholar] [CrossRef]
- Zhang, R.-G.; Hannak, W.B.; Roggensack, M.; Freesmeyer, W.B. Retentive Characteristics of Ankylos SynCone Conical Crown System over Long-Term Use in Vitro. Eur. J. Prosthodont. Restor. Dent. 2008, 16, 61–66. [Google Scholar]
- Degidi, M.; Nardi, D.; Piattelli, A. The Conometric Concept: Coupling Connection for Immediately Loaded Titanium-Reinforced Provisional Fixed Partial Dentures—A Case Series. Int. J. Periodontics Restor. Dent. 2016, 36, 347–354. [Google Scholar] [CrossRef]
- Degidi, M.; Nardi, D.; Sighinolfi, G.; Degidi, D.; Piattelli, A. The Conometric Concept: A two-year follow-up of fixed partial cerec restorations supported by cone-in-cone abutments. J. Prosthodont. 2019, 28, e780–e787. [Google Scholar] [CrossRef]
- Albiero, A.; Benato, R.; Momic, S.; Degidi, M. Computer-Aided Crown Design Using Digital Scanning Technology for Immediate Postextraction Single-Implant Restorations Supported by Conical Indexed Abutments. Int. J. Periodontics Restor. Dent. 2021, 41, 135–140. [Google Scholar] [CrossRef]
- Bressan, E.; Venezze, A.; Magaz, V.; Lops, D.; Ghensi, P. Fixed Conometric Retention with CAD/CAM Conic Coupling Abutments and Prefabricated Syncone Caps: A Case Series. Int. J. Periodontics Restor. Dent. 2018, 38, 277–280. [Google Scholar] [CrossRef]
- Bressan, E.; Lops, D. Conometric Retention for Complete Fixed Prosthesis Supported by Four Implants: 2-Years Prospective Study. Clin. Oral Implants Res. 2014, 25, 546–552. [Google Scholar] [CrossRef]
- Degidi, M.; Nardi, D.; Sighinolfi, G.; Piattelli, A. The Conometric Concept: A 5-Year Follow-up of Fixed Partial Monolithic Zirconia Restorations Supported by Cone-in-Cone Abutments. Int. J. Periodontics Restor. Dent. 2018, 38, 363–371. [Google Scholar] [CrossRef]
- Degidi, M.; Nardi, D.; Sighinolfi, G.; Piattelli, A. The Conometric Concept: Definitive Fixed Lithium Disilicate Restorations Supported by Conical Abutments. J. Prosthodont. 2018, 27, 605–610. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| References | Study Type | Features | Outcomes |
|---|---|---|---|
| Bressan et al. 2014 | Prospective Study | CP supported by 4 implants F.U. 2 yy | No biological or technical adverse events. Good hygiene control. |
| Bressan et Lops. 2014 | In Vitro | Computational investigation of coping-abutment system | Conometric connection could be considered a fixed system if it is adequately activated. Retention and insertion forces are proportional. |
| Bressan et al. 2017 | In Vitro | Microbial leakage at conometric prosthetic connection | Good microbiological seal and a very low rate of leakage are demonstrated. They are good factors for biological health. |
| Bressan et al. 2018 | Case Series | CAD/CAM crown with conometric retention | Good technical and biological response. It is shown that different brands of implant could be used with the association of conometric abutments. |
| Degidi et al. 2016 | Case Series | Conometric connection for immediate loading provisional FPD | The cases show a high rate of success and a good biological response. |
| Degidi et al. 2018 (a) | Observational Study | 5yy F.U. of zirconia FPD supported by conometric abutments | Good prosthetic response and manufacturing due to the space between the coping and the antagonist tooth. 100% rate of implant success. |
| Degidi et al. 2018 (b) | Observational Study | Definitive LS2 FPD supported by conometric abutments | Small prosthetic accidents, but a very good health of the peri-implant tissue. |
| Degidi et al. 2019 | Observational Study | 2 yy F.U. of CAD-CAM FPD supported by conometric abutments | The conometric connection demonstrates a good factor for the support tissue. Possible mis-fit due to the CAD-CAM production could be erased by the cementation of the prosthesis on the coping. |
| Degidi et al. 2020 | Dental Technique | Use of a conometric connection for a single crown in posterior area | Good technical and biological feedback; according to the study, the clinician must pay attention at the insertion phase and must correct any interference. |
| Antonaya-Martis et al. 2016 | In Vitro | Evaluation of retention using different conical degree | Retention force is inversely proportional to the conicity. |
| Nardi et al. 2017 | In Vitro | Evaluation of retention strength of conical welding caps for fixed implant prosthesis | Impulse activation increases retention force up to 87%. |
| Zhang et al. 2008 | In Vitro | Retentive characteristics of conical crown system over long-term cycle of in vitro use | An adequate retention force was carried out. |
| Gherke et al. 2021 | In Vitro | Bacterial migration in conical indexed abutment | No bacterial translocation could be individuated. SEM observation demonstrated small microleakage at the interface abutment-coping. |
| Gherke, Hartjen et al. 2021 | In Vitro | Marginal adaptation and leakage at conometric connection for a single crown | No bacterial colonization of the space abutment-coping could be observed. |
| Albiero et al. 2018 | Dental Technique | Implementation using digital scanner with conometric connection | Angulation well predictable in CAD phase. Welding caps are time-saving. |
| Albiero et al. 2019 | Case Report | Guided-welded and CAD-CAM shell for CP supported by conometric abutments | Prosthetic Guided Treatment. CAD phases are very complex. Good hygiene procedure due to the easy removal procedures of the prosthesis. |
| Albiero et al. 2021 | Case Report | CAD/CAM crown using full digital process. Immediate post-extraction single implant | Prosthetic margin apically and extreme aesthetics with total health of the around tissue. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lupi, S.M.; Todaro, C.; De Martis, D.; Blasi, P.; Rodriguez y Baena, R.; Storelli, S. The Conometric Connection for the Implant-Supported Fixed Prosthesis: A Narrative Review. Prosthesis 2022, 4, 458-467. https://doi.org/10.3390/prosthesis4030037
Lupi SM, Todaro C, De Martis D, Blasi P, Rodriguez y Baena R, Storelli S. The Conometric Connection for the Implant-Supported Fixed Prosthesis: A Narrative Review. Prosthesis. 2022; 4(3):458-467. https://doi.org/10.3390/prosthesis4030037
Chicago/Turabian StyleLupi, Saturnino Marco, Claudia Todaro, Dario De Martis, Paola Blasi, Ruggero Rodriguez y Baena, and Stefano Storelli. 2022. "The Conometric Connection for the Implant-Supported Fixed Prosthesis: A Narrative Review" Prosthesis 4, no. 3: 458-467. https://doi.org/10.3390/prosthesis4030037
APA StyleLupi, S. M., Todaro, C., De Martis, D., Blasi, P., Rodriguez y Baena, R., & Storelli, S. (2022). The Conometric Connection for the Implant-Supported Fixed Prosthesis: A Narrative Review. Prosthesis, 4(3), 458-467. https://doi.org/10.3390/prosthesis4030037