
Real-Time Operative Coding for Endoscopic Sinonasal Procedures: Quality Improvement in Practice


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
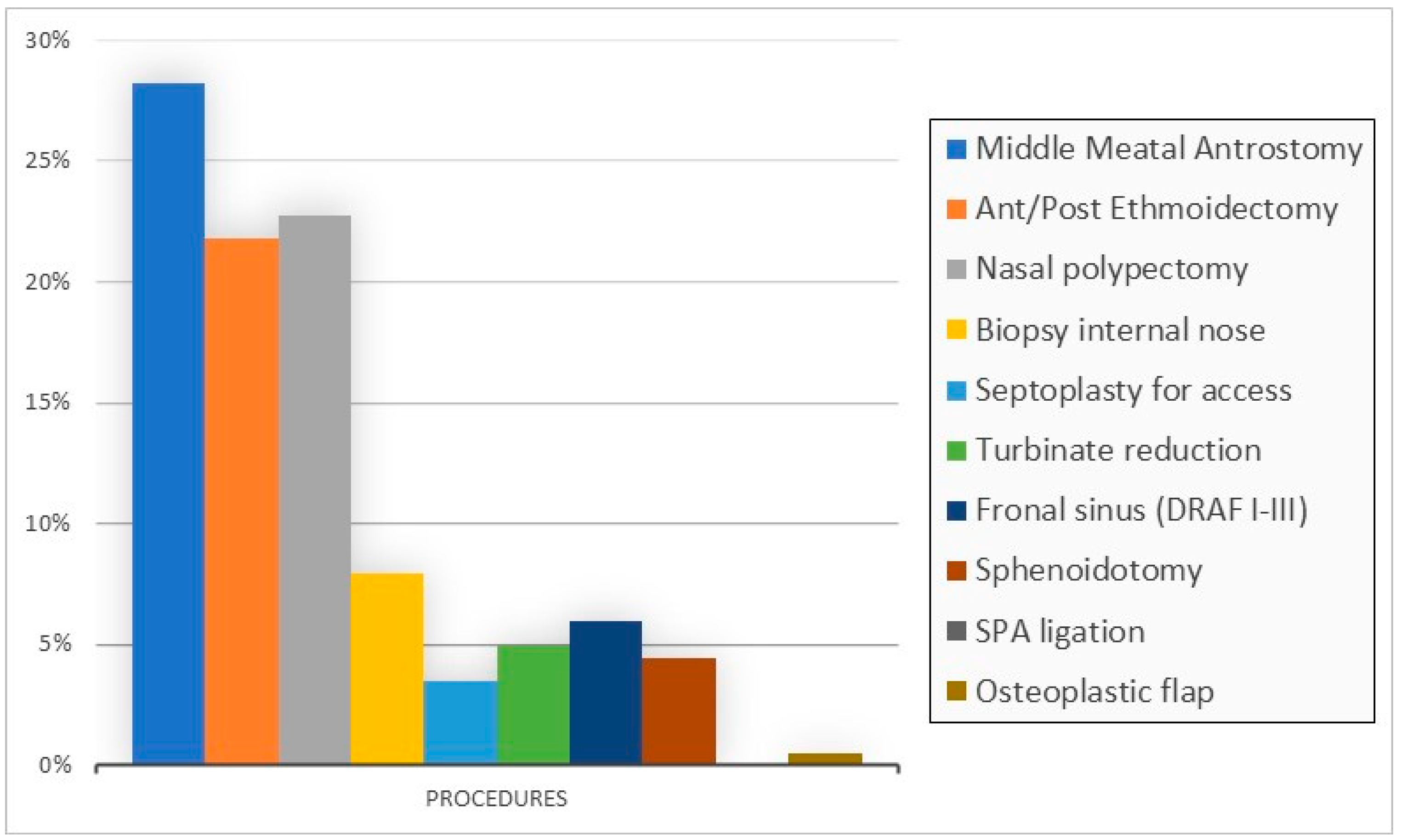
3. Results
3.1. First Cycle (May 2017–August 2017)
3.2. Second Cycle (September and December 2017)
3.3. Both Cycles
4. Discussion
4.1. Understand Inaccuracy in Coding
4.2. Financial Implication
4.3. Strength and Limitation in Our Study
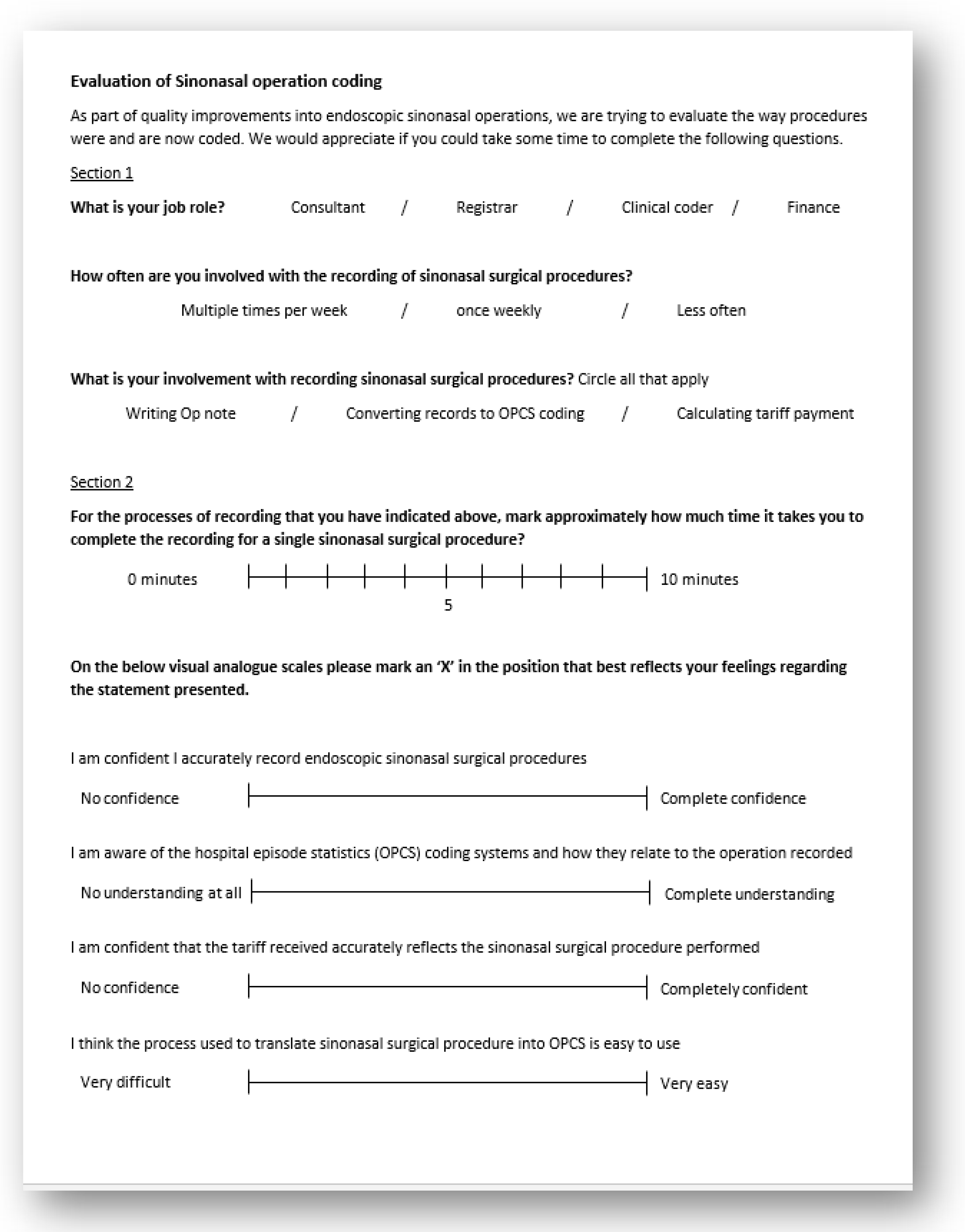
4.4. Feedback on Intraoperative Coding
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nouraei, S.A.R.; Hudovsky, A.; Virk, J.; Chatrath, P.; Sandhu, G.S. An audit of the nature and impact of clinical coding subjectivity variability and error in otolaryngology. Clin. Otolaryngol. 2013, 38, 512–524. [Google Scholar] [CrossRef] [PubMed]
- Mason, A.; Ward, P.; Street, A. England: The Healthcare Resource Group system. In Diagnosis-Related Groups in Europe, Ch 12, 12; Busse, R., Ed.; Open University Press: Berkshire, UK, 2011; pp. 197–220. [Google Scholar]
- NHS Digital. Hospital Episode Statistics. Available online: http://content.digital.nhs.uk/hes (accessed on 24 November 2017).
- World Health Organization. International Classification of Diseases. Available online: http://www.who.int/classifications/icd/en/ (accessed on 24 November 2017).
- NHS Digital. Clinical Classifications. Available online: https://digital.nhs.uk/article/1117/Clinical-Classifications (accessed on 24 November 2017).
- NHS Digital. SCCI0084—OPCS Classification of Interventions and Procedures. Available online: http://content.digital.nhs.uk/isce/publication/scci0084 (accessed on 24 November 2017).
- Nouraei, S.A.R.; Hudovsky, A.; Virk, J.S.; Saleh, H.A. Impact of developing a multidisciplinary coded dataset standard on administrative data accuracy for septoplasty, septorhinoplasty and nasal trauma surgery. J. Laryngol. Otol. 2017, 131, 341–346. [Google Scholar] [CrossRef]
- Alonso, V.; Santos, J.V.; Pinto, M.; Ferreira, J.; Lema, I.; Lopes, F.; Freitas, A. Problems and Barriers during the Process of Clinical Coding: A Focus Group Study of Coders’ Perceptions. J. Med. Syst. 2020, 44, 44–62. [Google Scholar] [CrossRef]
- Nouraei, S.A.R.; Virk, J.S.; Hudovsky, A.; Wathen, C.; Darzi, A.; Parsons, D. Accuracy of clinician-clinical coder information handover following acute medical admissions: Implication for using administrative datasets in clinical outcomes management. J. Public Health (Bangkok) 2015, 38, 352–362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nouraei, S.A.R.; O’Hanlon, S.; Butler, C.R.; Hadovsky, A.; Donald, E.; Benjamin, E.; Sandhu, G.S. A multidisciplinary audit of clinical coding accuracy in otolaryngology: Financial, managerial and clinical governance considerations under payment-by-results. Clin. Otolaryngol. 2009, 34, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Juniat, V.; Athwal, S.; Khandwala, M. Clinical coding and data quality in oculoplastic procedures. Eye J. 2019, 33, 1733–1740. [Google Scholar] [CrossRef] [PubMed]
- Maclean, D.; Younes, H.B.; Forrest, M.; Towers, H.K. The accuracy of real-time procedure coding by theatre nurses: A comparison with the central national system. Health Inform. J. 2012, 18, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Colville, R.J.; Laing, J.H.; Murison, M.S. Coding plastic surgery operations: An audit of performance using OPCS-4. Br. J. Plast. Surg. 2000, 53, 420–422. [Google Scholar] [CrossRef] [PubMed]
- Naran, S.; Hudovsky, A.; Antscherl, J.; Howells, S.; Nouraei, S.A.R. Audit of accuracy of clinical coding in oral surgery. Br. J. Oral Maxillofac. Surg. 2014, 52, 735–739. [Google Scholar] [CrossRef] [PubMed]
- Barros, P.; Braun, G. Upcoding in a National Health Service: The evidence from Portugal. Health Econ. 2017, 26, 600–618. [Google Scholar] [CrossRef] [PubMed]
- Murphy, J.; May, C.; Di Carlo, S.; Beckingham, I.; Cameron, I.C.; Gomez, D. Coding in surgery: Impact of a specialized coding proforma in hepato-pancreato-biliary surgery. ANZ J. Surg. 2018, 88, 621–625. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, M.; Siciliani, L. Manipulation and auditing of public sector contracts. Eur. J. Political Econ. 2013, 32, 251–267. [Google Scholar] [CrossRef]
- Lüngen, M.; Lauterbach, K.W. Upcoding—Eine Gefahr für den Einsatz von Diagnosis-Related Groups (DRG)? [Upcoding—A risk for the use of diagnosis-related groups]. Dtsch. Med. Wochenschr. 2000, 125, 852–856. (In German) [Google Scholar] [CrossRef] [PubMed]
- Haliasos, N.; Rezajooi, K.; O’Neill, K.S.; Van Dellen, J.; Hudovsky, A.; Nouraei, S. Financial and clinical governance implications of clinical coding accuracy in neurosurgery: A multidisciplinary audit. Br. J. Neurosurg. 2010, 24, 191–195. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
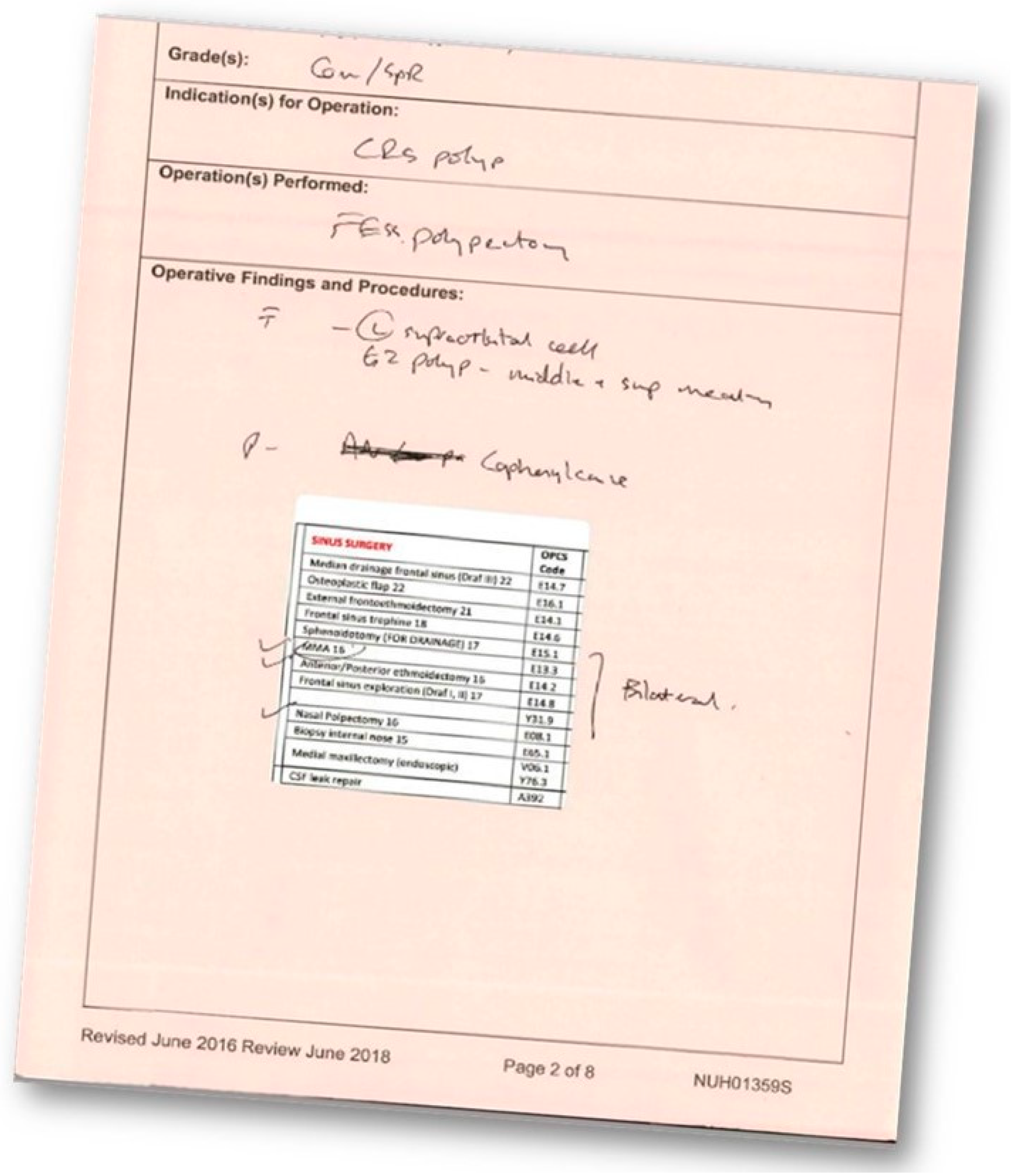
| Elements of Sinus Surgery as Recorded in Operation Notes | OPCS Code | HRG Translations | HRG | Tariff (£) | Combination Scores * |
|---|---|---|---|---|---|
| Median drainage frontal sinus (Draf III) | E14.7 | Median drainage of frontal sinus | CA26 | 2301 | |
| Osteoplastic flap | E16.1 | Frontal sinus osteoplasty | CA26 | 2301 | |
| External frontoethmoidectomy | E14.1 | External frontoethmoidectomy | CA26 | 2301 | |
| Frontal sinus trephine | E14.6 | Trephine of frontal sinus | CA28 | 1493 | 4 |
| Sphenoidotomy (FOR DRAINAGE) | E15.1 | Drainage of sphenoid sinus | CA28 | 1493 | 3 |
| MMA | E13.3 | Intranasal antrostomy | CA29 | 1317 | 2 |
| Anterior/Posterior ethmoidectomy | E14.2 | Intranasal ethmoidectomy | CA29 | 1317 | 2 |
| Frontal sinus exploration (Draf I, II) | E14.8 | Other specified operations on frontal sinus | CA28 | 1493 | 3 |
| Unspecified exploration of organ NOC | Y31.9 | Unspecified exploration of organ NOC | |||
| Nasal Polpectomy | E08.1 | Polypectomy of internal nose | CA14 | 1259 | 2 |
| Biopsy internal nose | E65.1 | Diagnostic endoscopic examination of nasal cavity and biopsy of lesion of nasal cavity | CA24 | 768 | 1 |
| * Combination codes—If procedures include a combination score use the cumulative score to generate a replacement upgrade code. | |||||
| 12 and above | CA26Z | 2301 | |||
| 8 and above | CA27Z | 1626 | |||
| 4 and above | CA28Z | 1493 | |||
| OPCS-S | HRG-S | OPCS-O | HRG-O | Inaccuracy | Explanation | Tarif |
|---|---|---|---|---|---|---|
| E651 | CA24 | E271 | CA83 | Wrong | Convert minor to major | 933 |
| E81, E133, E142, E151 | CA27 | E81, E133, E142 | CA28 | Under | Did not add a step of adenoidectomy | −133 |
| E148, E142, E81, E133 | CA27 | E81, E133, E142, E147 | CA26 | Up | Cumulative score 9 = CA27z not CA26z, E147 Draf III did not happen | 675 |
| E142, E151, E042 | CA28 | E142, E043, | CA29 | Under | Missing step of sphenoidotomy, navigation use was not counted | −176 |
| C81, E36 | CA14 | E81, Y762, E36 | CA22 | Up | Convert simple polypectomy to major nasal excision | 129 |
| E148, E042, E133 | CA28 | E147, E162, E133 | CA29 | Up | Cumulative HRG is over, putting osteoplastic flap instead turbinate reduction | 808 |
| E651 | CA24 | E033, E045 | CA15 | Wrong | Wrong coding | −28 |
| E081, E133, E142, E151 | CA27 | E081, E133, E142 | CA28 | Under | Did not add sphenoidotomy | −133 |
| E148, E142 | CA28 | E147, E142, E042 | CA26 | Up | Cumulative score is over | 808 |
| E081, E133, E036, E142 | CA28 | E083, E133, E036, E142 | CA21 | Up | Escalate to major surgery after adding septoplasty | 194 |
| E081, E133, E142 | CA28 | E641, E133, E142, E069 | CA21 | Up | Add codes to steps not done | 194 |
| E651 | CA24 | E271 | CA83 | Wrong | Convert biopsy postnasal to major mouth operation | 689 |
| E081, E133, E142 | CA28 | E081 | CA14 | Under | Cumulative score is underestimate | −234 |
| E082, E133, E142 | CA28 | E081, E133, E142, E162 | CA21 | Up | Frontal recess clearance recorded as osteoplastic flap | 194 |
| E042 | CA24 | E043 | CA15 | Wrong | The operation was partial turbinectomy (histology) not biopsy | −28 |
| E036, E133, E142, E081 | CA28 | E036, E133, E142, E064, E063 | CA21 | Up | Cumulative is overestimate | 194 |
| E651, E042 | CA24 | E081 | CA14 | Up | Biopsy of papillomatosis not polypectomy | 496 |
| Total | £4944.0 (£109.9 excess per patient in sample) | |||||
| % of Accurate Coding | 1st Cycle (no ICS Sticker) n = 45 | 2nd Cycle n = 49 | p-Value * |
|---|---|---|---|
| Intervention firm (using ICS in 35% cases in 2nd cycle) | 50% | 61% ^ | 0.429 |
| Control firm (not using ICS at any point) | 74% | 57% | 0.357 |
| p-value * | 0.140 | 0.801 | |
| Overall | 60% | 59% | 0.936 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mettias, B.; Whittaker, J.D.; Ramakrishnan, Y. Real-Time Operative Coding for Endoscopic Sinonasal Procedures: Quality Improvement in Practice. Sinusitis 2021, 5, 32-44. https://doi.org/10.3390/sinusitis5010004
Mettias B, Whittaker JD, Ramakrishnan Y. Real-Time Operative Coding for Endoscopic Sinonasal Procedures: Quality Improvement in Practice. Sinusitis. 2021; 5(1):32-44. https://doi.org/10.3390/sinusitis5010004
Chicago/Turabian StyleMettias, Bassem, Joshua D. Whittaker, and Yujay Ramakrishnan. 2021. "Real-Time Operative Coding for Endoscopic Sinonasal Procedures: Quality Improvement in Practice" Sinusitis 5, no. 1: 32-44. https://doi.org/10.3390/sinusitis5010004
APA StyleMettias, B., Whittaker, J. D., & Ramakrishnan, Y. (2021). Real-Time Operative Coding for Endoscopic Sinonasal Procedures: Quality Improvement in Practice. Sinusitis, 5(1), 32-44. https://doi.org/10.3390/sinusitis5010004