

Central Compartment Atopic Disease as a Pathophysiologically Distinct Subtype of Chronic Rhinosinusitis: A Scoping Review
 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.1.1. Participants
2.1.2. Information Sources
2.1.3. Search Strategy
2.2. Study Selection
2.3. Data Extraction and Analysis
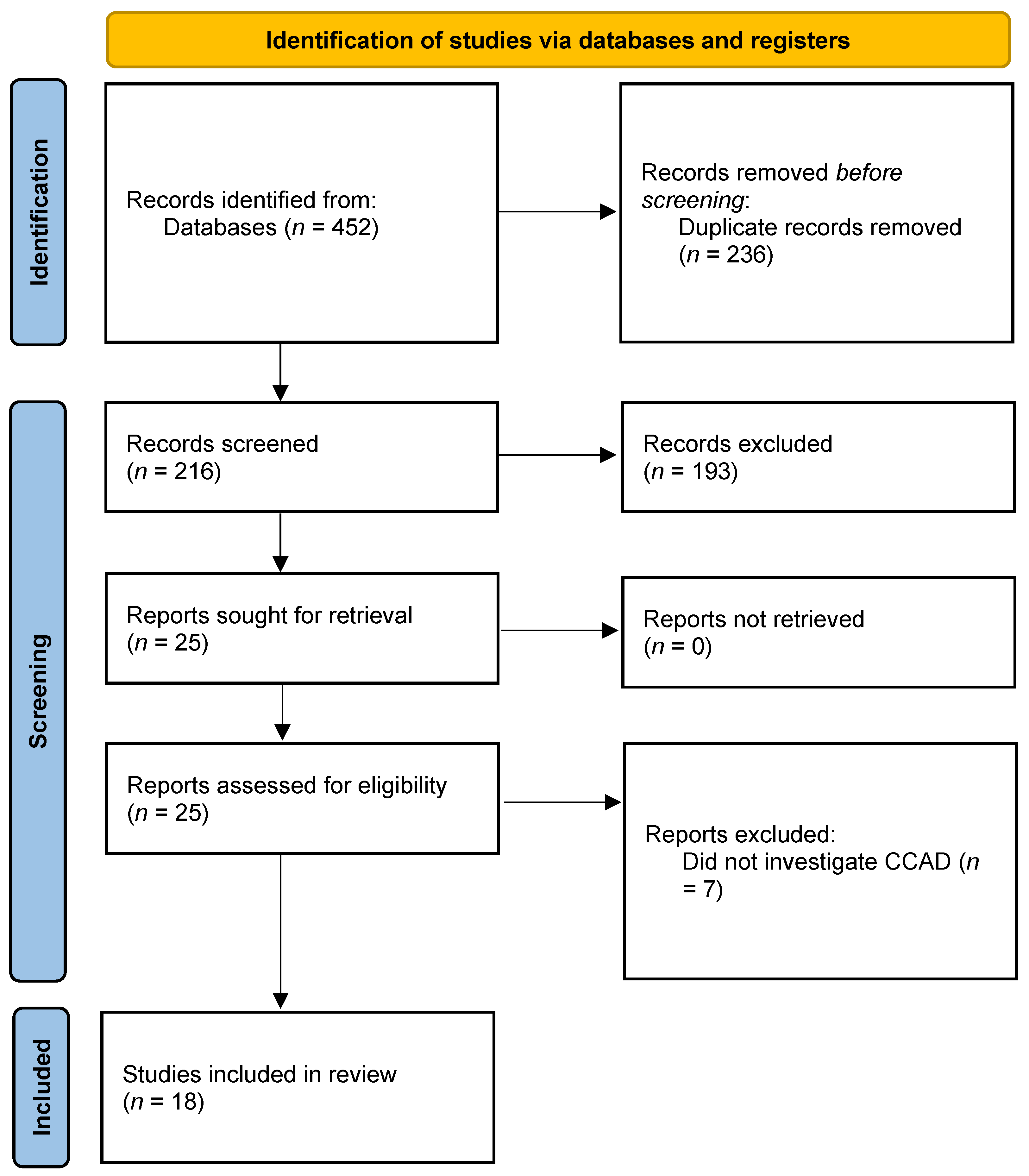
3. Results

{kind=link}
| Study | Aim of Study | Study Design and Level of Evidence | Population | Results |
|---|---|---|---|---|
| White, 2014 [6] | Investigate the association between isolated MT polyps and inhalant allergy | Case series Level 4 | 25 patients with isolated MT polyps |
|
| Brunner, 2017 [8] | Compare clinical characteristics of polypoid change of the MT (PCMT) with paranasal sinus polyposis (PSP) | Case series Level 4 | 593 patients: 23 (3.9%) with PCMT and 44 (7.4%) with PSP |
|
| DelGaudio, 2017 [3] | Describe a newly recognized variant of CRS, termed CCAD | Case series Level 4 | 15 patients with sinonasal symptoms and CC polypoid mucosal changes |
|
| Hamizan, 2017 [7] | Determine the characteristics of MT edema as a marker of inhalant allergy | Cross-sectional Level 4 | 187 patients |
|
| Hamizan, 2018 [12] | Identify radiologic patterns in CRS to predict allergic etiology | Cross-sectional Level 4 | 112 patients with CRS |
|
| DelGaudio, 2019 [2] | Investigate the role of allergy and surgery in CC involvement in AERD | Retrospective Cohort Level 3 | 72 patients with AERD: 59 (80.6%) had CC polyps/polypoid disease, with 53 bilateral and 6 unilateral |
|
| Abdullah, 2020 [14] | Define the clinical and radiological characteristics of the allergic phenotype of CRSwNP | Cross-sectional Level 4 | 38 patients with CRSwNP: 19 with allergy and 19 without allergy |
|
| Marcus, 2020 [4] | Determine the prevalence of allergy and asthma in CCAD compared with other CRSwNP subtypes | Retrospective Cohort Level 3 | 356 patients with CRSwNP: 37.1% with CRSwNP NOS, 24.2% with AERD, 23.6% with AFRS, 11.5% with CCAD, and 3.7% with CRSwNP/CC |
|
| Roland, 2020 [13] | Evaluate CT findings associated with each CRSwNP phenotype | Retrospective Cohort Level 3 | 356 patients: 23% with AFRS 28% with AERD 12% with CCAD 37% with CRSwNP NOS |
|
| Lin, 2021 [17] | Investigate the clinical features and cytokine profiles of CCAD in East Asian patients. | Cross-sectional Level 4 | 95 patients: 16 with CCAD and 51 with other CRS subtypes |
|
| Steehler, 2021 [16] | Evaluate surgical outcomes in CRSwNP subtypes | Retrospective Cohort Level 3 | 132 patients: 38 with CCAD, 20 with AERD, 37 with AFRS, 37 with CRSwNP NOS |
|
| Warman, 2021 [15] | Compare the inflammatory features of antrochoanal polyps (ACP) to diffuse primary CRSwNP (d-CRS) and its subgroups | Case series Level 4 | 96 patients: 40 (41.6%) with ACP, 36 (37.5%) with d-CRS, and 20 (20.8%) with control (patients undergoing turbinate reduction surgery due to nasal obstructions) |
|
| Edwards, 2022 [22] | Compare allergen sensitivity of local sinonasal tissue to that of skin and serum in patients with CCAD | Case series Level 4 | 15 participants with CCAD |
|
| Kong, 2022 [19] | Identify clinical presentations and cellular endotyping diagnosis of Chinese CCAD using artificial intelligence | Retrospective Cohort Level 3 | 79 Patients: 14 with CCAD, 32 with eosinophilic CRSwNP (ENP), and 26 with non-eosinophilic CRSwNP (NENP) |
|
| Lee, 2022 [23] | Investigate the ability of radiologic studies to predict CCAD in pediatric patients | Retrospective Cohort Level 3 | 82 pediatric patients diagnosed with CRS: 55/82 (67.1%) had aeroallergen sensitization, and 31/164 (18.9%) sides of sinuses had the radiologic CCAD phenotype |
|
| Nie, 2022 [20] | Describe the clinical manifestations of CCAD and compare to CRSwNP/CC involvement and CRSwNP NOS | Case series Level 4 | 116 patients: 39 with CCAD, 38 with CRSwNP/CC, and 39 with CRSwNP NOS |
|
| Shih, 2022 [18] | Determine the clinical presentations, risk factors, and surgical outcomes of CCAD in the Asian population | Case control Level 4 | 442 patients with CRSwNP: 51 with CCAD and 391 with lateral-dominant nasal polyp (LDNP) |
|
| Tripathi, 2022 [21] | Identify allergens associated with CRS endotypes and any relationships between their allergen sensitivity profiles. | Cross sectional Level 4 | 515 patients: 341 with CRS, 174 with AR. Of CRS patients: CRSwNP = 182, CRSsNP = 159. Of CRSwNP: AERD = 15, AFRS = 18, CCAD = 24, CRSwNP NOS = 125 |
|
4. Discussion
4.1. Clinical Characteristics
4.1.1. Patient Characteristics
4.1.2. Nasal Endoscopy
4.1.3. Radiologic Imaging
4.1.4. Allergy Testing
4.1.5. Histology and Molecular Findings
4.2. Management and Treatment Outcomes
4.3. Specific Populations
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Grayson, J.W.; Cavada, M.; Harvey, R.J. Clinically relevant phenotypes in chronic rhinosinusitis. J. Otolaryngol. Head Neck Surg. 2019, 48, 23. [Google Scholar] [CrossRef] [PubMed]
- DelGaudio, J.M.; Levy, J.M.; Wise, S.K. Central compartment involvement in aspirin-exacerbated respiratory disease: The role of allergy and previous sinus surgery. Int. Forum Allergy Rhinol. 2019, 9, 1017–1022. [Google Scholar] [CrossRef] [PubMed]
- DelGaudio, J.M.; Loftus, P.A.; Hamizan, A.W.; Harvey, R.J.; Wise, S.K. Central compartment atopic disease. Am. J. Rhinol. Allergy 2017, 31, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Marcus, S.; Schertzer, J.; Roland, L.T.; Wise, S.K.; Levy, J.M.; DelGaudio, J.M. Central compartment atopic disease: Prevalence of allergy and asthma compared with other subtypes of chronic rhinosinusitis with nasal polyps. Int. Forum Allergy Rhinol. 2020, 10, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Ong, Y.K.; Wang, Y. Precision Medicine in Chronic Rhinosinusitis: Where Does Allergy Fit In? Handb. Exp. Pharmacol. 2022, 268, 151–170. [Google Scholar] [CrossRef]
- White, L.J.; Rotella, M.R.; DelGaudio, J.M. Polypoid changes of the middle turbinate as an indicator of atopic disease. Int. Forum Allergy Rhinol. 2014, 4, 376–380. [Google Scholar] [CrossRef]
- Hamizan, A.W.; Christensen, J.M.; Ebenzer, J.; Oakley, G.; Tattersall, J.; Sacks, R.; Harvey, R.J. Middle turbinate edema as a diagnostic marker of inhalant allergy. Int. Forum Allergy Rhinol. 2017, 7, 37–42. [Google Scholar] [CrossRef]
- Brunner, J.P.; Jawad, B.A.; McCoul, E.D. Polypoid Change of the Middle Turbinate and Paranasal Sinus Polyposis Are Distinct Entities. Otolaryngol. Head Neck Surg. 2017, 157, 519–523. [Google Scholar] [CrossRef]
- DelGaudio, J.M. Central compartment atopic disease: The missing link in the allergy and chronic rhinosinusitis with nasal polyps saga. Int. Forum Allergy Rhinol. 2020, 10, 1191–1192. [Google Scholar] [CrossRef]
- Marcus, S.; Roland, L.T.; DelGaudio, J.M.; Wise, S.K. The relationship between allergy and chronic rhinosinusitis. Laryngoscope Investig. Otolaryngol. 2019, 4, 13–17. [Google Scholar] [CrossRef]
- Chandra, R.K. In Reply: Central compartment atopic disease: The missing link in the allergy and CRSwNP saga. Int. Forum Allergy Rhinol. 2020, 10, 1193–1194. [Google Scholar] [CrossRef] [PubMed]
- Hamizan, A.W.; Loftus, P.A.; Alvarado, R.; Ho, J.; Kalish, L.; Sacks, R.; DelGaudio, J.M.; Harvey, R.J. Allergic phenotype of chronic rhinosinusitis based on radiologic pattern of disease. Laryngoscope 2018, 128, 2015–2021. [Google Scholar] [CrossRef] [PubMed]
- Roland, L.T.; Marcus, S.; Schertzer, J.S.; Wise, S.K.; Levy, J.M.; DelGaudio, J.M. Computed Tomography Findings Can Help Identify Different Chronic Rhinosinusitis with Nasal Polyp Phenotypes. Am. J. Rhinol. Allergy 2020, 34, 679–685. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, B.; Vengathajalam, S.; Md Daud, M.K.; Wan Mohammad, Z.; Hamizan, A.; Husain, S. The Clinical and Radiological Characterizations of the Allergic Phenotype of Chronic Rhinosinusitis with Nasal Polyps. J. Asthma Allergy 2020, 13, 523–531. [Google Scholar] [CrossRef]
- Warman, M.; Kamar Matias, A.; Yosepovich, A.; Halperin, D.; Cohen, O. Inflammatory Profile of Antrochoanal Polyps in the Caucasian Population—A Histologic Study. Am. J. Rhinol. Allergy 2021, 35, 664–673. [Google Scholar] [CrossRef]
- Steehler, A.J.; Vuncannon, J.R.; Wise, S.K.; DelGaudio, J.M. Central compartment atopic disease: Outcomes compared with other subtypes of chronic rhinosinusitis with nasal polyps. Int. Forum Allergy Rhinol. 2021, 11, 1549–1556. [Google Scholar] [CrossRef]
- Lin, Y.T.; Lin, C.F.; Liao, C.K.; Chiang, B.L.; Yeh, T.H. Clinical characteristics and cytokine profiles of central-compartment-type chronic rhinosinusitis. Int. Forum Allergy Rhinol. 2021, 11, 1064–1073. [Google Scholar] [CrossRef]
- Shih, L.C.; Hsieh, B.H.; Ma, J.H.; Huang, S.S.; Tsou, Y.A.; Lin, C.D.; Huang, K.H.; Tai, C.J. A comparison of central compartment atopic disease and lateral dominant nasal polyps. Int. Forum Allergy Rhinol. 2022, 12, 1387–1396. [Google Scholar] [CrossRef]
- Kong, W.; Wu, Q.; Chen, Y.; Ren, Y.; Wang, W.; Zheng, R.; Deng, H.; Yuan, T.; Qiu, H.; Wang, X.; et al. Chinese Central Compartment Atopic Disease: The Clinical Characteristics and Cellular Endotypes Based on Whole-Slide Imaging. J. Asthma Allergy 2022, 15, 341–352. [Google Scholar] [CrossRef]
- Nie, Z.; Xu, Z.; Fan, Y.; Guo, Y.; Chen, C.; Liu, W.; Li, Y.; Lai, Y.; Shi, J.; Chen, F. Clinical characteristics of central compartment atopic disease in Southern China. Int. Forum Allergy Rhinol. 2022, 13, 205–215. [Google Scholar] [CrossRef]
- Tripathi, S.H.; Ungerer, H.N.; Rullan-Oliver, B.; Patel, T.; Sweis, A.M.; Maina, I.W.; Kohanski, M.A.; Palmer, J.N.; Adappa, N.D.; Bosso, J.V. Similarities between allergen sensitivity patterns of central compartment atopic disease and allergic rhinitis. Int. Forum Allergy Rhinol. 2022, 12, 1299–1302. [Google Scholar] [CrossRef]
- Edwards, T.S.; DelGaudio, J.M.; Levy, J.M.; Wise, S.K. A Prospective Analysis of Systemic and Local Aeroallergen Sensitivity in Central Compartment Atopic Disease. Otolaryngol. Head. Neck Surg. 2022, 167, 885–890. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Kim, T.H.; Lee, S.H.; Kang, C.H.; Je, B.K.; Oh, S. Predictive Value of Radiologic Central Compartment Atopic Disease for Identifying Allergy and Asthma in Pediatric Patients. Ear Nose Throat J. 2022, 101, 593–599. [Google Scholar] [CrossRef] [PubMed]
- Helman, S.N.; Barrow, E.; Edwards, T.; DelGaudio, J.M.; Levy, J.M.; Wise, S.K. The Role of Allergic Rhinitis in Chronic Rhinosinusitis. Immunol. Allergy Clin. N. Am. 2020, 40, 201–214. [Google Scholar] [CrossRef] [PubMed]
- Marcus, S.; DelGaudio, J.M.; Roland, L.T.; Wise, S.K. Chronic Rhinosinusitis: Does Allergy Play a Role? Med. Sci. 2019, 7, 30. [Google Scholar] [CrossRef]
- Hamizan, A.W.; Rimmer, J.; Alvarado, R.; Sewell, W.A.; Kalish, L.; Sacks, R.; Harvey, R.J. Positive allergen reaction in allergic and nonallergic rhinitis: A systematic review. Int. Forum Allergy Rhinol. 2017, 7, 868–877. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, N.; Bo, M.; Holtappels, G.; Zheng, M.; Lou, H.; Wang, H.; Zhang, L.; Bachert, C. Diversity of T(H) cytokine profiles in patients with chronic rhinosinusitis: A multicenter study in Europe, Asia, and Oceania. J. Allergy Clin. Immunol. 2016, 138, 1344–1353. [Google Scholar] [CrossRef]

| Abbreviation | Full Name |
|---|---|
| AFRS | Allergic fungal rhinosinusitis |
| AR | Allergic rhinitis |
| ACP | Antrochoanal polyps |
| AERD | Aspirin-exacerbated respiratory disease |
| CC | Central compartment |
| CCAD | Central compartment atopic disease |
| CRS | Chronic rhinosinusitis |
| CRSwNP | Chronic rhinosinusitis with nasal polyps |
| CRSsNP | Chronic rhinosinusitis without nasal polyps |
| d-CRS | Diffuse primary chronic rhinosinusitis with nasal polyps |
| ENP | Eosinophilic chronic rhinosinusitis with nasal polyps |
| IgE | Immunoglobulin-E |
| LDNP | Lateral-dominant nasal polyp |
| LK | Lund–Kennedy |
| LM | Lund–Mackay |
| MT | Middle turbinate |
| NENP | Non-eosinophilic chronic rhinosinusitis with nasal polyps |
| PSP | Paranasal sinus polyposis |
| PCMT | Polypoid change of the middle turbinate |
| SNS | Superior nasal septum |
| ST | Superior turbinate |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Davies, C.; Wu, F.; Huang, E.Y.; Takashima, M.; Rowan, N.R.; Ahmed, O.G. Central Compartment Atopic Disease as a Pathophysiologically Distinct Subtype of Chronic Rhinosinusitis: A Scoping Review. Sinusitis 2023, 7, 12-26. https://doi.org/10.3390/sinusitis7020003
Davies C, Wu F, Huang EY, Takashima M, Rowan NR, Ahmed OG. Central Compartment Atopic Disease as a Pathophysiologically Distinct Subtype of Chronic Rhinosinusitis: A Scoping Review. Sinusitis. 2023; 7(2):12-26. https://doi.org/10.3390/sinusitis7020003
Chicago/Turabian StyleDavies, Camron, Franklin Wu, Emily Y. Huang, Masayoshi Takashima, Nicholas R. Rowan, and Omar G. Ahmed. 2023. "Central Compartment Atopic Disease as a Pathophysiologically Distinct Subtype of Chronic Rhinosinusitis: A Scoping Review" Sinusitis 7, no. 2: 12-26. https://doi.org/10.3390/sinusitis7020003
APA StyleDavies, C., Wu, F., Huang, E. Y., Takashima, M., Rowan, N. R., & Ahmed, O. G. (2023). Central Compartment Atopic Disease as a Pathophysiologically Distinct Subtype of Chronic Rhinosinusitis: A Scoping Review. Sinusitis, 7(2), 12-26. https://doi.org/10.3390/sinusitis7020003