
The Multi-Biomarker Approach for Heart Failure in Patients with Hypertension


 ,
, 

Abstract
:1. Introduction
2. Results and Discussion
2.1. General Characteristics of Patients

{kind=link}
{kind=link}
| Parameter | Mean ± Standard Deviation (SD) | p | |||
|---|---|---|---|---|---|
| Non-HF Group n = 60 | HF Group n = 60 | Non-HF vs. HF | |||
| Age (years) | 61.76 ± 11 | 64.54 ± 11 | 0.57 | ||
| BMI (kg/m2) | 27.38 ± 4 | 28.66 ± 4 | 0.16 | ||
| GFR MDRD (mL/min/1.73 m2) | 89.31 ± 6 | 67.72 ± 24 | 0.0001 | ||
| Systolic BP (mmHg) | 135.82 ± 8 | 122.28 ± 14 | 0.0001 | ||
| Diastolic BP (mmHg) | 82.00 ± 8 | 75.72 ± 8 | 0.0001 | ||
| HR (bpm) | 70.57 ± 4 | 74.34 ± 9 | 0.09 | ||
| Hemoglobin (g/dL) | 14.38 ± 0.96 | 13.87 ± 1 | 0.11 | ||
| Galectin-3 (ng/mL) | 21.27 ± 5 | 18.59 ± 11 | 0.43 | ||
| TNF-α (pg/mL) | 32.63 ± 44 | 30.94 ± 16 | 0.23 | ||
| CT-1 (pg/mL) | 89.13 ± 115 | 229.51 ± 129.7 | <0.0001 | ||
| TGF-β (ng/mL) | 10.67 ± 2.92 | 5.98 ± 2 | <0.0001 | ||
| Syndecan (ng/mL) | 1.39 ± 1.08 | 4.14 ± 3 | <0.0001 | ||
| NT-proBNP (pg/mL) | 150.12 ± 115 | 1889.03 ± 336 | <0.0001 | ||
| CysC (mg/L) | 0.81 ± 0.44 | 1.37 ± 0.83 | <0.0001 | ||
| NGAL (ng/mL) | 50.71 ± 45 | 64.96 ± 36 | 0.007 | ||
| PIIINP (ng/mL) | 2.21 ± 1 | 2.62 ± 0.97 | 0.06 | ||
| IL1R1(ng/mL) | 0.45 ± 0.31 | 0.35 ± 0.19 | 0.05 | ||
| CRP (mg/L) | 2.26 ± 1 | 3.60 ± 4.70 | 0.95 | ||
| LVEDD (mm) | 49.86 ± 5 | 63.22 ± 9 | <0.0001 | ||
| LVESD (mm) | 31.65 ± 5 | 48.10 ± 10 | <0.0001 | ||
| LVEF (%) | 60.92 ± 4 | 36.70 ± 10 | <0.0001 | ||
| LA (mm) | 36.59 ± 5 | 45.14 ± 7 | <0.0001 | ||
| peak E (cm/s) | 70.84 ± 15 | 62.90 ± 23 | 0.19 | ||
| peak A (cm/s) | 68.10 ± 19 | 87.40 ± 13 | 0.01 | ||
| E/A ratio | 1.10 ± 0.38 | 0.66 ± 0.25 | 0.008 | ||
| DT (ms) | 257.88 ± 66 | 343.17 ± 106 | 0.04 | ||
| IVSD (mm) | 9.39 ± 2 | 11.77 ± 2 | <0.0001 | ||
| PWD (mm) | 9.29 ± 1 | 11.33 ± 2 | 0.002 | ||
| RVdD (mm) | 27.31 ± 3 | 28.82 ± 4 | 0.08 | ||
| LVEDV (mL) | 83.44 ± 23 | 213.59 ± 60 | <0.0001 | ||
| LVESV (mL) | 29.06 ± 8 | 135.55 ± 50 | <0.0001 | ||
| TAPSE (mm) | 25.16 ± 3 | 21.67 ± 3 | 0.005 | ||
| Parameter | Number of Patients (%) | p | |||
| Non-HF Group; n = 60 | HF Group; n = 60 | ||||
| Gender (male) | 22 (45) | 43 (86) | <0.0001 | ||
| Smoking | 4 (8) | 2 (4) | 0.65 | ||
| Heart failure acc. to NYHA | I | 35 (72) | 5 (10) | 0.0001 | |
| II | 14 (28) | 21 (42) | |||
| III | 0 | 24 (48) | |||
| IV | 0 | 0 | |||
| Stenocardia acc. to CCS | 0 | 27 (55) | 2 (4) | 0.0001 | |
| I | 5 (10) | 34 (68) | |||
| II | 17 (34) | 13 (26) | |||
| III | 0 | 1 (2) | |||
| Diabetes mellitus or abnormal glucose level | 9 (18) | 19 (38) | 0.03 | ||
| Statins | 21 (43) | 32 (64) | 0.03 | ||
| Insulin | 4 (8) | 3 (6) | 0.97 | ||
| Loop diuretics | 21 (42) | 46 (92) | <0.0001 | ||
| Β-blockers | 17 (77) | 26 (96) | 0.06 | ||
| Spironolactone/eplerenone | 7 (14) | 41 (82) | 0.01 | ||
| Acetylsalicylic acid | 17 (35) | 26 (53) | 0.06 | ||
| ACE inhibitors | 22 (45) | 43 (86) | <0.0001 | ||
| Sartans (ARBs) | 22 (45) | 8 (16) | 0.001 | ||
| Calcium channel blockers | 16 (32) | 4 (8) | 0.005 | ||
| Digoxin | 0 | 12 (24) | 0.0008 | ||
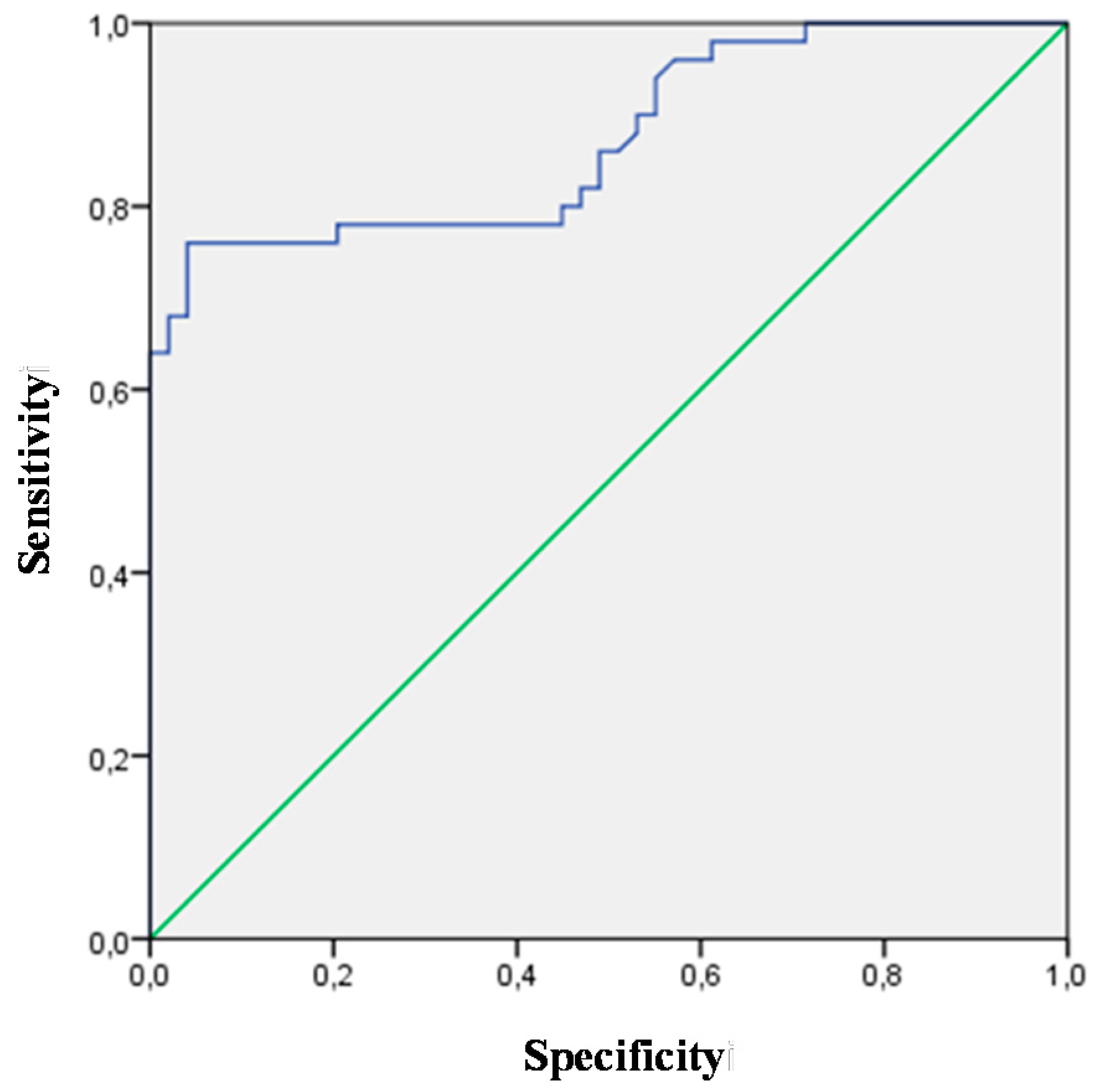
2.2. Assessment of Biomarkers
| Biomarker | AUC | Standard Error—SE | p | 95% CI | |
|---|---|---|---|---|---|
| CT-1 | 0.831 | 0.045 | 0.0001 | 0.743 | 0.918 |
| TGF-β | 0.878 | 0.034 | 0.0001 | 0.811 | 0.944 |
| Syndecan | 0.781 | 0.047 | 0.0001 | 0.689 | 0.873 |
| NT-proBNP | 0.873 | 0.036 | 0.0001 | 0.803 | 0.943 |
| CysC | 0.793 | 0.045 | 0.0001 | 0.705 | 0.881 |
| NGAL | 0.673 | 0.065 | 0.007 | 0.545 | 0.802 |


| Meters | CT-1 ≥152.2 pg/mL | TGF-β ≤7.7 ng/mL | Syndecan ≥2.3 ng/mL | NT-proBNP ≥332.5 pg/mL | CysC ≥1.0 mg/L | NGAL ˃39.9 ng/mL |
|---|---|---|---|---|---|---|
| Sensitivity | 0.77 | 0.72 | 0.64 | 0.76 | 0.62 | 0.58 |
| Specificity | 0.85 | 0.91 | 0.87 | 0.95 | 0.83 | 0.81 |
| PPV | 0.83 | 0.90 | 0.83 | 0.95 | 0.78 | 0.68 |
| NPV | 0.80 | 0.76 | 0.71 | 0.79 | 0.69 | 0.74 |
| OR | 20.50 | 28.92 | 13.06 | 74.41 | 8.54 | 6.34 |
| OR (−95% CI) | 7.05 | 8.76 | 4.62 | 15.68 | 3.28 | 2.34 |
| OR (+95% CI) | 59.52 | 95.52 | 36.93 | 353.01 | 22.23 | 17.16 |
| p | 0.0001 | 0.0001 | 0.0001 | 0.0001 | 0.0001 | 0.0001 |
2.3. Predictive Value of Selected Biomarkers in Univariate and Multivariate Regression Analysis
| Analysis | Variable | Parameter—B | SE | p | OR | 95% CI | c Statistic | |
|---|---|---|---|---|---|---|---|---|
| Univariate analysis | Galectin-3 | −0.039 | 0.027 | 0.145 | 0.961 | 0.912 | 1.014 | 0.549 |
| TNF-α | −0.002 | 0.006 | 0.800 | 0.998 | 0.986 | 1.011 | 0.418 | |
| CT-1 | 0.010 | 0.002 | 0.000 | 1.010 | 1.006 | 1.015 | 0.830 | |
| TGF-β | −0.630 | 0.124 | 0.000 | 0.533 | 0.418 | 0.679 | 0.878 | |
| Syndecan | 0.675 | 0.173 | 0.000 | 1.964 | 1.398 | 2.759 | 0.781 | |
| NT-proBNP | 0.007 | 0.002 | 0.000 | 1.007 | 1.003 | 1.010 | 0.873 | |
| CysC | 2.714 | 0.742 | 0.000 | 15.091 | 3.523 | 64.645 | 0.793 | |
| NGAL | −0.010 | 0.006 | 0.123 | 0.990 | 0.978 | 1.003 | 0.673 | |
| PIIINP | 0.374 | 0.206 | 0.069 | 1.454 | 0.971 | 2.177 | 0.590 | |
| IL1R1 | −1.640 | 0.850 | 0.054 | 0.194 | 0.037 | 1.025 | 0.587 | |
| CRP | 0.153 | 0.093 | 0.099 | 1.165 | 0.972 | 1.398 | 0.504 | |
| Comparison of Models—NT-proBNP vs.: | Measure | |
|---|---|---|
| Galectin-3 | NRI (Categorical) (95% CI): −0.3963 (−0.6305–−0.162); p-value: 0.00092 | |
| NRI (Continuous) (95% CI): −1.1735 (−1.524–−0.8229); p-value: 0.00000 | ||
| IDI (95% CI): −0.4621 (−0.5864–−0.3379); p-value: 0.00000 | ||
| TNF-α | NRI (Categorical) (95% CI): −0.6513 (−0.8–−0.5026); p-value: 0.00000 | |
| NRI (Continuous) (95% CI): −1.4765 (−1.7278–−1.2252); p-value: 0.00000 | ||
| IDI (95% CI): −0.4962 (−0.5948–−0.3975); p-value: 0.00000 | ||
| CT-1 | NRI (Categorical) (95% CI): −0.0625 (−0.2909–0.1659); p-value: 0.59176 | |
| NRI (Continuous) (95% CI): −0.7111 (−1.091–−0.3312); p-value: 0.00024 | ||
| IDI (95% CI): −0.2023 (−0.3402–−0.0645); p-value: 0.00401 | ||
| TGF-β | NRI (Categorical) (95% CI): −0.0816 (−0.2969–0.1336); p-value: 0.45731 | |
| NRI (Continuous) (95% CI): −0.2188 (−0.6047–0.1671); p-value: 0.26649 | ||
| IDI (95% CI): −0.031 (−0.17–0.1079); p-value: 0.66165 | ||
| Syndecan | NRI (Categorical) (95% CI): −0.1658 (−0.3694–0.0377); p-value: 0.11034 | |
| NRI (Continuous) (95% CI): −0.7211 (−1.0922–−0.3499); p-value: 0.00014 | ||
| IDI (95% CI): −0.2204 (−0.345–−0.0958); p-value: 0.00053 | ||
| CysC | NRI (Categorical) (95% CI): −0.2479 (−0.4714–−0.0244); p-value: 0.02974 | |
| NRI (Continuous) (95% CI): −0.6811 (−1.0551–−0.3072); p-value: 0.00036 | ||
| IDI (95% CI): −0.2526 (−0.374–−0.1312); p-value: 0.00000 | ||
| NGAL | NRI (Categorical) (95% CI): −0.4502 (−0.6725–−0.2279); p-value: 0.00000 | |
| NRI (Continuous) (95% CI): −1.1261 (−1.4897–−0.7624); p-value: 0.00000 | ||
| IDI (95% CI): −0.4029 (−0.5347–−0.2711); p-value: 0.00000 | ||
| PIIINP | NRI (Categorical) (95% CI): −0.5858 (−0.8364–−0.3352); p-value: 0.00000 | |
| NRI (Continuous) (95% CI): −1.0872 (−1.4282–−0.7462); p-value: 0.00000 | ||
| IDI (95% CI): −0.4543 (−0.5718–−0.3368); p-value: 0.00000 | ||
| IL1R1 | NRI (Categorical) (95% CI): −0.595 (−0.853–−0.337); p-value: 0.00000 | |
| NRI (Continuous) (95% CI): −1.2626 (−1.5716–−0.9535); p-value: 0.00000 | ||
| IDI (95% CI): −0.4404 (−0.5486–−0.3322); p-value: 0.00000 | ||
| CRP | NRI (Categorical) (95% CI): −0.4872 (−0.7025–−0.2718); p-value: 0.00000 | |
| NRI (Continuous) (95% CI): −0.9704 (−1.3663–−0.5745); p-value: 0.00000 | ||
| IDI (95% CI): −0.4035 (−0.5319–−0.2752); p-value: 0.00000 | ||
Comparison of the Basic Model of NT-proBNP with Models Extended by an Additional Biomarker
| Comparison of Models—NT-proBNP vs. NT-proBNP + Additional Biomarker: | Measure |
|---|---|
| Galectin-3 | NRI (Categorical) (95% CI): −0.0147 (−0.1356–0.1061); p-value: 0.81102 |
| NRI (Continuous) (95% CI): 0.3401 (−0.0229–0.7031); p-value: 0.06627 | |
| IDI (95% CI): 0.0534 (0.0143–0.0924); p-value: 0.00742 | |
| TNF-α | NRI (Categorical) (95% CI): −0.0417 (−0.099–0.0155); p-value: 0.15329 |
| NRI (Continuous) (95% CI): 0.0643 (−0.1991–0.3278); p-value: 0.63213 | |
| IDI (95% CI): 0.0022 (−0.0113–0.0156); p-value: 0.75434 | |
| Cardiotrophin | NRI (Categorical) (95% CI): 0.0444 (−0.0876–0.1764); p-value: 0.5093 |
| NRI (Continuous) (95% CI): 1.175 (0.8603–1.4897); p-value: 0.00000 | |
| IDI (95% CI): 0.1207 (0.0575–0.1839); p-value: 0.00018 | |
| TGF-β | NRI (Categorical) (95% CI): 0.1204 (−0.0246–0.2654); p-value: 0.10364 |
| NRI (Continuous) (95% CI): 1.2343 (0.9371–1.5315); p-value: 0.00000 | |
| IDI (95% CI): 0.2139 (0.1314–0.2965); p-value: 0.00000 | |
| Syndecan | NRI (Categorical) (95% CI): 0.1029 (−0.0302–0.236); p-value: 0.12963 |
| NRI (Continuous) (95% CI): 1.0676 (0.7499–1.3853); p-value: 0.00000 | |
| IDI (95% CI): 0.0979 (0.0417–0.1542); p-value: 0.00064 | |
| Cystatin | NRI (Categorical) (95% CI): −0.02 (−0.1089–0.0689); p-value: 0.6595 |
| NRI (Continuous) (95% CI): 1.0519 (0.7234–1.3803); p-value: 0.00000 | |
| IDI (95% CI): 0.0733 (0.0257–0.1209); p-value: 0.00253 | |
| NGAL | NRI (Categorical) (95% CI): −0.009 (−0.0984–0.0804); p-value: 0.84352 |
| NRI (Continuous) (95% CI): 0.9628 (0.5862–1.3393); p-value: 0.00000 | |
| IDI (95% CI): 0.0407 (−0.0015–0.0828); p-value: 0.05869 | |
| PIIINP | NRI (Categorical) (95% CI): 0.0204 (−0.0888–0.1297); p-value: 0.71427 |
| NRI (Continuous) (95% CI): 0.8242 (0.4631–1.1854); p-value: 0.00000 | |
| IDI (95% CI): 0.0808 (0.0333–0.1283); p-value: 0.00086 | |
| IL1R1 | NRI (Categorical) (95% CI): 0.0186 (−0.0516–0.0888); p-value: 0.60352 |
| NRI (Continuous) (95% CI): −0.0458 (−0.4257–0.3341); p-value: 0.81317 | |
| IDI (95% CI): 0.0097 (−0.0029–0.0222); p-value: 0.13103 | |
| CRP | NRI (Categorical) (95% CI): 0.0086 (−0.0747–0.0919); p-value: 0.8404 |
| NRI (Continuous) (95% CI): 0.2581 (0.0396–0.4765); p-value: 0.02058 | |
| IDI (95% CI): 0.0259 (0.0094–0.0423); p-value: 0.00206 |
| Variable | Parameter—B | SE | p | OR | 95% CI | c Statistic | |||
|---|---|---|---|---|---|---|---|---|---|
| NT-proBNP | 0.008 | 0.003 | 0.003 | 1.008 | 1.003 | 1.014 | 0.973 | ||
| TGF-β | −0.611 | 0.186 | 0.001 | 0.543 | 0.377 | 0.781 | |||
| CT-1 | 0.009 | 0.003 | 0.013 | 1.009 | 1.002 | 1.016 | |||
| NT-proBNP | 0.010 | 0.004 | 0.008 | 1.010 | 1.003 | 1.017 | 0.985 | ||
| TGF-β | −0.752 | 0.240 | 0.002 | 0.472 | 0.295 | 0.754 | |||
| CT-1 | 0.007 | 0.003 | 0.040 | 1.007 | 1.000 | 1.014 | |||
| CysC | 2.490 | 1.046 | 0.017 | 12.058 | 1.551 | 93.720 | |||
| Comparison of the 3-Variable Model with the Model Only with NT-proBNP | Comparison of the 4-Variable Model with the Model Only with NT-proBNP | Comparison of the 4-Variable moDel with the 3-Variable Model | |||||||
| NRI (Categorical) (95% CI): 0.1319 (−0.0225–0.2864); p-value: 0.0941 | NRI (Categorical) (95% CI): 0.1333 (−0.031–0.2976); p-value: 0.11173 | NRI (Categorical) (95% CI): 0.0014 (−0.0577–0.0604); p-value: 0.96323 | |||||||
| NRI (Continuous) (95% CI): 1.6083 (1.3833–1.8333); p-value: 0.00000 | NRI (Continuous) (95% CI): 1.6111 (1.3862–1.836); p-value: 0.00000 | NRI (Continuous) (95% CI): 1.3278 (1.0407–1.6148); p-value: 0.00000 | |||||||
| IDI (95% CI): 0.2637 (0.1761–0.3512); p-value: 0.00000 | IDI (95% CI): 0.2982 (0.206–0.3904); p-value: 0.00000 | IDI (95% CI): 0.0345 (−0.0011–0.0701); p-value: 0.0572 | |||||||
2.4. Discussion
2.4.1. Background
2.4.2. BNP/NT-proBNP as the Gold Standard Biomarker in Heart Failure
2.4.3. Short Description of the Results
2.4.4. The Multi-Biomarker Heart Failure Approach
Transforming Growth Factor-Β
Cardiotrophin-1
Cystatin C
2.5. Limitations of the Study
3. Experimental Section
3.1. Study Population
3.2. Biomarker Tests
3.3. Echocardiography
3.4. Statistical Analysis
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Dalzell, J.R.; Cannon, J.A.; Jackson, C.E.; Lang, N.N.; Gardner, R.S. Emerging biomarkers for heart failure: An update. Biomark. Med. 2014, 8, 833–840. [Google Scholar] [CrossRef] [PubMed]
- Kantor, P.F.; Rusconi, P.; Lipshultz, S.; Mital, S.; Wilkinson, J.D.; Burch, M. Current applications and future needs for biomarkers in pediatric cardiomyopathy and heart failure: Summary from the second international conference on pediatric cardiomyopathy. Prog. Pediatr. Cardiol. 2011, 32, 11–14. [Google Scholar] [CrossRef] [PubMed]
- Braunwald, E. Biomarkers in heart failure. N. Engl. J. Med. 2008, 358, 2148–2159. [Google Scholar] [CrossRef] [PubMed]
- Kapoun, A.M.; Liang, F.; O’Young, G.; Damm, D.L.; Quon, D.; White, R.T.; Munson, K.; Lam, A.; Schreiner, G.F.; Protter, A.A. B-type natriuretic peptide exerts broad functional opposition to transforming growth factor-β in primary human cardiac fibroblasts: Fibrosis, myofibroblast conversion, proliferation, and inflammation. Circ. Res. 2004, 94, 453–461. [Google Scholar] [CrossRef] [PubMed]
- Maisel, A.S.; Krishnaswamy, P.; Nowak, R.M.; McCord, J.; Hollander, J.E.; Duc, P.; Omland, T.; Storrow, A.B.; Abraham, W.T.; Wu, A.H.; et al. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. N. Engl. J. Med. 2002, 347, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Troughton, R.W.; Frampton, C.M.; Yandle, T.G.; Espiner, E.A.; Nicholls, M.G.; Richards, A.M. Treatment of heart failure guided by plasma aminoterminal brain natriuretic peptide (N-BNP) concentrations. Lancet 2000, 355, 1126–1130. [Google Scholar] [CrossRef] [PubMed]
- De Lemos, J.A.; McGuire, D.K.; Drazner, M.H. B-type natriuretic peptide in cardiovascular disease. Lancet 2003, 362, 316–322. [Google Scholar] [CrossRef] [PubMed]
- Jungbauer, C.G.; Riedlinger, J.; Block, D.; Stadler, S.; Birner, C.; Buesing, M.; König, W.; Riegger, G.; Maier, L.; Luchner, A. Panel of emerging cardiac biomarkers contributes for prognosis rather than diagnosis in chronic heart failure. Biomark. Med. 2014, 8, 777–789. [Google Scholar] [CrossRef] [PubMed]
- Bielecka-Dabrowa, A.; Michalska-Kasiczak, M.; Gluba, A.; Ahmed, A.; von Healing, S.; Gerdts, E.; Rysz, J.; Banach, M. Biomarkers and echocardiographic predictors of myocardial dysfunction in patients with hypertension. Sci. Rep. 2015, 5. [Google Scholar] [CrossRef] [PubMed]
- Bielecka-Dabrowa, A.; von Haehling, S.; Aronow, W.S.; Ahmed, M.I.; Rysz, J.; Banach, M. Heart failure biomarkers in patients with dilated cardiomyopathy. Int. J. Cardiol. 2013, 168, 2404–2410. [Google Scholar] [CrossRef] [PubMed]
- Petriz, B.A.; Franco, O.L. Effects of hypertension and exercise on cardiac proteome remodelling. Biomed. Res. Int. 2014, 2014, 634132. [Google Scholar] [CrossRef] [PubMed]
- NHS National Institute for Health and Care Excellence: Chronic Heart Failure: Management of Chronic Heart Failure in Adults in Primary and Secondary Care. webcite. Available online: http://www.nice.org.uk/guidance/cg108 (accessed on 8 August 2010).
- McMurray, J.J.; Adamopoulos, S.; Anker, S.D.; Auricchio, A.; Bohm, M.; Dickstein, K.; Falk, V.; Filippatos, G.; Fonseca, C.; Gomez-Sanchez, M.A.; et al. ESC Committee for Practice Guidelines: ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2012, 33, 1787–1847. [Google Scholar] [CrossRef] [PubMed]
- McCullough, P.A.; Sandberg, K.R. Sorting out the evidence on natriuretic peptides. Rev. Cardiovasc. Med. 2003, 4, 13–19. [Google Scholar]
- Nurko, S. Anemia in chronic kidney disease: Causes, diagnosis, treatment. Clevel. Clin. J. Med. 2006, 73, 289–297. [Google Scholar] [CrossRef]
- James, S.K.; Lindahl, B.; Siegbahn, A.; Stridsberg, M.; Venge, P.; Armstrong, P.; Barnathan, E.S.; Califf, R.; Topol, E.J.; Simoons, M.L.; et al. N-terminal pro-brain natriuretic peptide and other risk markers for the separate prediction of mortality and subsequent myocardial infarction in patients with unstable coronary artery disease. Circulation 2003, 108, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Redfield, M.M.; Rodeheffer, R.J.; Jacobsen, S.J.; Mahoney, D.W.; Bailey, K.K.; Burnett, J.C., Jr. Plasma brain natriuretic peptide concentration: Impact of age and gender. J. Am. Coll. Cardiol. 2002, 40, 976–982. [Google Scholar] [CrossRef] [PubMed]
- Wei, B.Q.; Zhang, J.; Yang, Y.J.; Zhang, Y.H.; Huang, X.H.; Yu, L.T.; Zhou, Q.; Tan, H.Q.; Yang, Y.M.; Wang, G.G.; et al. Influencing factors for the plasma concentration of N-terminal brain natriuretic peptide precursor in patients with heart failure due to various heart diseases. Zhonghua Yi Xue Za Zhi 2011, 91, 2683–2687. [Google Scholar] [PubMed]
- Opie, L.H.; Commerford, P.J.; Gersh, B.J. Controversies in ventricular remodelling. Lancet 2006, 367, 356–367. [Google Scholar] [CrossRef] [PubMed]
- Behnes, M.; Hoffmann, U.; Lang, S.; Weiss, C.; Ahmad-Nejad, P.; Neumaier, M.; Borggrefe, M.; Brueckmann, M. Transforming growth factor β1 (TGF-β1) in atrial fibrillation and acute congestive heart failure. Clin. Res. Cardiol. 2011, 100, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Dobrev, D. Atrial Ca2+ signaling in atrial fibrillation as an antiarrhythmic drug target. Naunyn Schmiedebergs Arch. Pharmacol. 2010, 381, 195–206. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, Y.; Tamura, N.; Chusho, H.; Nakao, K. Brain natriuretic peptide appears to act locally as an antifibrotic factor in the heart. Can. J. Physiol. Pharmacol. 2001, 79, 723–729. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Wang, D.; Lucas, J.; Oparil, S.; Xing, D.; Cao, X.; Novak, L.; Renfrow, M.B.; Chen, Y.F. Atrial natriuretic peptide inhibits transforming growth factor β-induced Smad signaling and myofibroblast transformation in mouse cardiac fibroblasts. Circ. Res. 2008, 102, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Celik, A.; Sahin, S.; Koc, F.; Karayakali, M.; Sahin, M.; Benli, I.; Kadi, H.; Burucu, T.; Ceyhan, K. Cardiotrophin-1 plasma levels are increased in patients with diastolic heart failure. Med. Sci. Monit. 2012, 18, CR25–CR31. [Google Scholar] [CrossRef] [PubMed]
- López, B.; González, A.; Querejeta, R.; Larman, M.; Rábago, G.; Díez, J. Association of cardiotrophin-1 with myocardial fibrosis in hypertensive patients with heart failure. Hypertension 2014, 63, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Ravassa, S.; Beloqui, O.; Varo, N.; Barba, J.; López, B.; Beaumont, J.; Zalba, G.; Díez, J.; González, A. Association of cardiotrophin-1 with left ventricular systolic properties in asymptomatic hypertensive patients. J. Hypertens. 2013, 31, 587–594. [Google Scholar] [PubMed]
- Song, K.; Wang, S.; Huang, B.; Luciano, A.; Srivastava, R.; Mani, A. Plasma cardiotrophin-1 levels are associated with hypertensive heart disease: A meta-analysis. J. Clin. Hypertens. 2014, 16, 686–692. [Google Scholar] [CrossRef]
- Inker, L.A.; Okparavero, A. Cystatin C as a marker of glomerular filtration rate: Prospects and limitations. Curr. Opin. Nephrol. Hypertens. 2011, 20, 631–639. [Google Scholar] [CrossRef] [PubMed]
- Shipak, M.G.; Sarnak, M.J.; Katz, R.; Fried, L.; Seliger, S.; Newman, A.; Siscovick, D.; Stehman-Breen, C. Cystatin C and mortality in elderly persons with heart failure. J. Am. Coll. Cardiol. 2005, 45, 268–271. [Google Scholar] [CrossRef] [PubMed]
- Gao, C.; Zhong, L.; Gao, Y.; Li, X.; Zhang, M.; Wei, S. Cystatin C levels are associated with the prognosis of systolic heart failure patients. Arch. Cardiovasc. Dis. 2011, 104, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Zhu, H.; Li, P.; Xin, Q.; Liu, J.; Zhang, W.; Xing, Y.H.; Xue, H. Serum cystatin C concentration as an independent marker for hypertensive left ventricular hypertrophy. J. Geriatr. Cardiol. 2013, 10, 286–290. [Google Scholar] [PubMed]
- Manzano-Fernández, S.; Boronat-Garcia, M.; Albaladejo-Otón, M.D.; Pastor, P.; Garrido, I.P.; Pastor-Pérez, F.J.; Martínez-Hernández, P.; Valdés, M.; Pascual-Figal, D.A. Complementary prognostic value of cystatin C, N-terminal pro-B-type natriuretic peptide and cardiac troponin T in patients with acute heart failure. Am. J. Cardiol. 2009, 103, 1753–1759. [Google Scholar] [CrossRef] [PubMed]
- Moran, A.; Katz, R.; Smith, N.L.; Fried, L.F.; Sarnak, M.J.; Seliger, S.L.; Psaty, B.; Siscovick, D.S.; Gottdiener, J.S.; Shlipak, M.G. Cystatin C concentration as a predictor of systolic and diastolic heart failure. J. Card. Fail. 2008, 14, 19–26. [Google Scholar] [CrossRef] [PubMed]
- The Criteria Committee of the New York Heart Association. Nomenclature and Criteria for Diagnosis of Diseases of the Heart and Great Vessels, 9th ed.; Little, Brown & Co.: Boston, MA, USA, 1994; pp. 253–256. [Google Scholar]
- Campeau, L. Grading of angina pectoris. Circulation 1976, 54, 522–523. [Google Scholar] [PubMed]
- Modification of Diet in Renal Disease Study Group. A more accurate accurate method to estimate glomerular filtration rate from serum creatinine: A new prediction equation. Ann. Intern. Med. 1999, 130, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flachskampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.H.; Roman, M.J.; Seward, J.; Shanewise, J.; et al. Recommendations for chamber quantification. Eur. J. Echocardiogr. 2006, 7, 79–108. [Google Scholar] [CrossRef] [PubMed]
- Cook, N.R. Statistical evaluation of prognostic versus diagnostic models: Beyond the ROC curve. Clin. Chem. 2008, 54, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Kundu, S.; Aulchenko, Y.S.; van Duijn, C.M.; Janssens, A.C.J.W. PredictABEL: An R package for the assessment of risk prediction models. Eur. J. Epidemiol. 2011, 26, 261–264. [Google Scholar] [CrossRef] [PubMed]
- Pencina, M.J.; D’Agostino, R.B., Sr.; D’Agostino, R.B., Jr.; Vasan, R.S. Evaluating the added predictive ability of a new marker: From area under the ROC curve to reclassification and beyond. Stat. Med. 2008, 27, 157–172. [Google Scholar] [CrossRef] [PubMed]
- Pencina, M.J.; D’Agostino, R.B., Sr.; Steyerberg, E.W. Extensions of net reclassification improvement calculations to measure usefulness of new biomarkers. Stat. Med. 2011, 30, 11–21. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bielecka-Dabrowa, A.; Gluba-Brzózka, A.; Michalska-Kasiczak, M.; Misztal, M.; Rysz, J.; Banach, M. The Multi-Biomarker Approach for Heart Failure in Patients with Hypertension. Int. J. Mol. Sci. 2015, 16, 10715-10733. https://doi.org/10.3390/ijms160510715
Bielecka-Dabrowa A, Gluba-Brzózka A, Michalska-Kasiczak M, Misztal M, Rysz J, Banach M. The Multi-Biomarker Approach for Heart Failure in Patients with Hypertension. International Journal of Molecular Sciences. 2015; 16(5):10715-10733. https://doi.org/10.3390/ijms160510715
Chicago/Turabian StyleBielecka-Dabrowa, Agata, Anna Gluba-Brzózka, Marta Michalska-Kasiczak, Małgorzata Misztal, Jacek Rysz, and Maciej Banach. 2015. "The Multi-Biomarker Approach for Heart Failure in Patients with Hypertension" International Journal of Molecular Sciences 16, no. 5: 10715-10733. https://doi.org/10.3390/ijms160510715
APA StyleBielecka-Dabrowa, A., Gluba-Brzózka, A., Michalska-Kasiczak, M., Misztal, M., Rysz, J., & Banach, M. (2015). The Multi-Biomarker Approach for Heart Failure in Patients with Hypertension. International Journal of Molecular Sciences, 16(5), 10715-10733. https://doi.org/10.3390/ijms160510715